Abstract
Cervical disc degenerative disease (CDDD) is a common spinal pathology that is often treated with anterior cervical discectomy and fusion (ACDF), cervical disc arthroplasty (CDA), and/or hybrid cervical surgery (HCS). The purpose of this first-time systematic review is to examine the biomechanical outcomes associated with three types of non-contiguous cervical surgeries—ACDF, CDA, and HCS—to provide a greater understanding of non-contiguous cervical surgical biomechanics. A systematic review was performed using PubMed, Cumulated Index to Nursing and Allied Health Literature (CINAHL), MEDLINE, and Web of Science from database inception until June 6th, 2023. The inclusion criteria was any article that reported biomechanical or kinematic outcomes, outcomes for any of the three non-contiguous cervical surgeries, and human-derived and/or human cadaver subjects. A total of 5 biomechanical articles were included from a total of 523 articles. Non-contiguous two-level HCS experienced less drastic range-of-motion (ROM) changes throughout the cervical spine and decreased intervertebral disc pressure (IDP) compared to non-contiguous two-level ACDF. Non-contiguous two-level CDA resulted in more cervical ROM and less non-operative segment facet contact force compared to non-contiguous two level ACDF. There was less cephalad and caudal non-operative segment ROM in non-contiguous two-level ACDF compared to contiguous three-level ACDF.
1. Introduction
Cervical disc degenerative disease (CDDD) is a common spinal pathology that impacts many patients worldwide and has received extensive attention in the literature [1,2,3,4,5]. Estimates of the prevalence of CDDD in the literature range from 37% to 96%, depending on patient age [6]. Numerous cervical surgical procedures exist for the treatment of CDDD, including anterior cervical discectomy and fusion (ACDF), cervical disc arthroplasty (CDA), and a combination of both of those procedures called hybrid cervical surgery (HCS) [1,2,3,4,5,7,8,9,10,11,12,13]. Patients can develop CDDD in a multi-level contiguous manner, in which adjacent levels of the cervical spine are affected, or in a non-contiguous manner, in which there is “skip-level” CDDD or level(s) of diseased cervical segments between level(s) of healthy cervical segments [1,3,4,5,14,15].
Much of the current literature has focused on cervical surgeries for multi-level contiguous CDDD and related pathologies with a recent systematic review exploring the relative efficacy of ACDF, CDA, and HCS for multi-level contiguous CDDD [15] Furthermore, there has also been a desire to understand the biomechanics of these three cervical surgeries for contiguous CDDD in the form of individual articles and systematic reviews [1,5,12,13,14]. However, there is far less evidence regarding clinical and biomechanical outcomes for non-contiguous ACDF, CDA, and HCS to treat non-contiguous CDDD at this time, presenting a challenge to patients and surgeons alike [16,17,18,19].
To date, no systematic review in the literature examines the biomechanical properties and outcomes of these three cervical surgeries when performed in a non-contiguous manner, despite the publication of multiple individual biomechanical studies in the past five years using previously described methods of cadaveric or finite element analysis [7,8,9,10]. The purpose of this systematic review is to examine the biomechanical outcomes associated with three types of non-contiguous cervical surgeries—ACDF, CDA, and HCS—to provide a benchmark for comparison to contiguous cervical surgeries to guide surgeon decision-making and to advance the current understanding of ideal treatment for non-contiguous cervical pathologies.
2. Materials and Methods
2.1. Information Sources and Search Strategy
This study is a systematic review that was conducted for articles reporting on biomechanical outcomes for non-contiguous ACDF, CDA, or HCS in PubMed, Cumulated Index to Nursing and Allied Health Literature (CINAHL), MEDLINE, and Web of Science from database inception until 6 June 2023. Search terms used in each database were “(non-contiguous OR skip-level OR noncontiguous) AND cervical” and articles were included in the initial search if any of these terms appeared in the article. This study was performed in accordance with the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [20]. This systematic review was not registered prior to completion.
2.2. Inclusion and Exclusion Criteria
Inclusion criteria was any article that reported biomechanical or kinematic outcomes, any article that included outcomes for any of the three non-contiguous cervical surgeries (ACDF, CDA, and HCS), any level of evidence, full-text articles, English articles, and human-derived and/or human cadaver subjects. Exclusion criteria included any article that did not report biomechanical outcomes, articles that reported on outcomes unrelated to the three included non-contiguous cervical surgeries, articles without full text, animal models, and articles not in English.
2.3. Study Definitions
For the purposes of this study, “initial non-operative cervical spine” refers to a cadaver spine prior to any cervical surgery procedure, as seen in the study by Finn et al. (2011), or a finite element model (FEM) prior to any operative procedures, as seen in the other four included articles [7,8,9,10,11]. For the purposes of this study, “cephalad non-operative segment”, “intermediate non-operative segment”, and “caudal non-operative segment” refer to the cervical segment levels that did not receive surgical intervention and are above, between, and below the operative levels, respectively.
2.4. Article Selection Process
The articles found on initial search in the four databases were upload into Rayyan, a software commonly utilized in the literature for the systematic review process [21]. Duplicate articles were removed manually and then articles were screened by title and abstract by two authors. Any discrepancies were solved by a third author. Articles were then screened by full text by two authors with any discrepancies resolved by a third author. Articles that fully met the inclusion criteria were selected for study inclusion.
2.5. Data Extraction
Data extraction was primarily performed by a single author. Data extracted included authors, year of publication, type of material used for analysis (cadaver or finite element), type of study, cervical levels involved, type of non-contiguous cervical surgery (ACDF, CDA, and HCS), variant of HCS (fusion–arthroplasty or arthroplasty–fusion) and biomechanical outcomes relating to cervical ROM, intervertebral disc pressure (IDP), and cervical facet contact pressure in terms of relative magnitude and location.
2.6. Bias and Quality Assessment
The Methodological Index for Non-Randomized Studies (MINORS) scale was utilized for this systematic review for quality and bias assessment of the included articles [22]. The MINORS scale can be utilized for observational studies that are comparative or non-comparative in nature [22]. Comparative observational studies are assessed via a 0–24-point scale with 12 criteria judged on a 0–2 point scale. Non-comparative observational studies are assessed via a 0–16 point scale with eight criteria judged on a 0–2 scale [22]. Categories in the MINORS scale include clearly stated aim, inclusion criteria, prospective collection of data, appropriate end points for the study aim, unbiased assessment of the study end point, appropriate follow-up period, loss to follow-up, prospective calculation of study size, adequate control group, contemporary groups, baseline equivalence of groups, and adequate statistical analysis [22].
2.7. Certainty Assessment
The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach was used in this systematic review to assess the certainty of evidence for the biomechanical outcome categories [23] The certainty of evidence was rated as high, moderate, low, or very low for each included analysis based on the study design, heterogeneity (treatment differences, sample variability, design differences), risk of bias, indirectness, and publication bias. The “high” category suggests that additional research is unlikely to impact the overall effect estimate. The “moderate” category suggests that additional research is likely to significantly alter the confidence in the effect estimate. The “low” category suggests that additional research is highly likely to significantly change the effect estimate. The “very low” category suggests that any effect estimate of the current study is ultimately uncertain due to the low quality of the articles [23]. Grading was performed by a single author.
2.8. Statistical Analysis
Statistical Package for the Social Sciences (SPSS) version 29.0 (IBM Corp, Armonk, NY, USA) was used for the statistical analysis of this systematic review. Descriptive statistics and frequency weighted means were used to report outcomes from the included articles. A meta-analysis was not performed for this systematic review due to the small number of articles and relative heterogeneity between articles. Instead, a narrative approach was undertaken without numerical synthesis to allow for a better presentation of the data.
3. Results
3.1. Study Selection and Characteristics
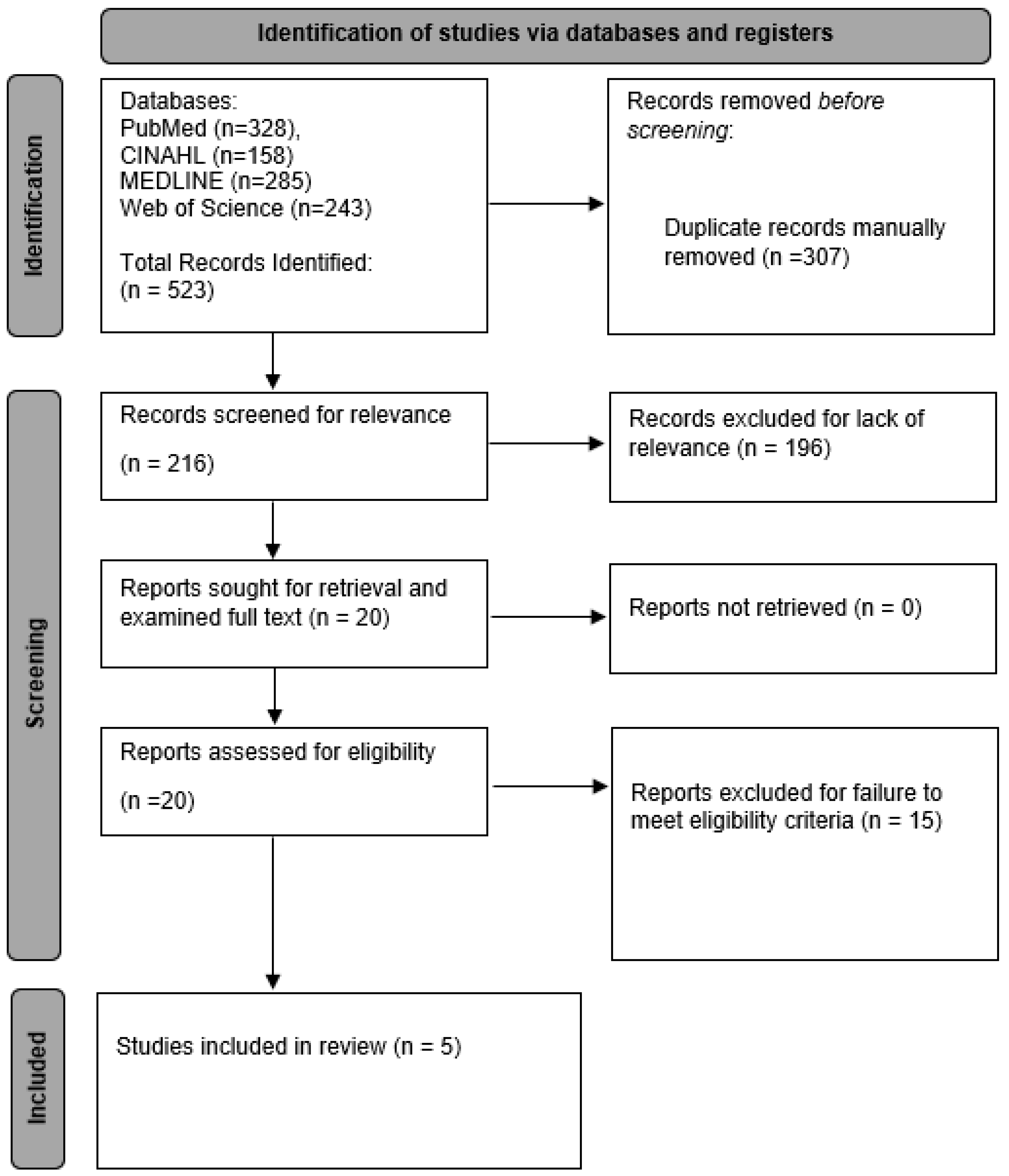
A total of 5 articles on the biomechanics of non-contiguous cervical fusion surgeries were included in this systematic review from a total of 523 articles found on initial search [7,8,9,10,11]. See Figure 1 for more information on the article selection process for this study. All five articles were graded via the MINORS scale and can be seen in Table 1. The certainty of the included data was “very low” for all outcomes via the GRADE scale due to a low sample size increasing the risk of bias and the fact that all of the included articles were non-randomized studies. For specifics on individual articles, Finn et al. (2011) compared two-level non-contiguous ACDF to three-level contiguous ACDF. Sun et al. (2020) compared two-level non-contiguous ACDF to two-level non-contiguous CDA [7] Sun et al. (2023) compared two types of non-contiguous hybrid cervical construction surgeries, with the fusion–arthroplasty variant receiving upper segment (C3–C4) ACDF and lower segment (C5–C6) CDA and the arthroplasty-fusion variant receiving upper segment (C3–C4) CDA and lower segment (C5–C6) ACDF [8]. Wu, Meng, Wang, and colleagues (2019) compared non-contiguous CDA and non-contiguous ACDF at C3–C4 and C5–C6, respectively [10]. Wu, Meng, Liu and colleagues (2019) compared two variants of hybrid cervical surgery at C3–C4 and C5–C6 (fusion–arthroplasty, and arthroplasty–fusion) to one another as well as a fusion–fusion control group [9].
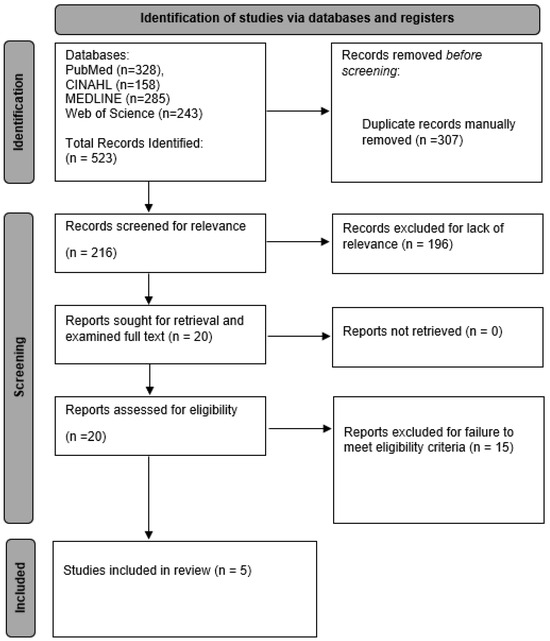
Figure 1.
PRISMA diagram that depicts this systematic review from initial search findings to final article inclusion. This PRISMA diagram is in accordance with the 2020 PRISMA reporting guidelines.

Table 1.
MINORS bias and quality grading for the five included articles. The MINORS scale is assessed on a 0–24-point scale with 12 criteria worth 0–2 points for comparative studies. Abbreviations: MINORS, Methodological Index for Non-Randomized Studies.
3.2. Methodology of Included Articles
Finn et al. (2011) utilized seven fresh and frozen human cadaver cervical spines with levels C3–T1 from patients younger than 65 years old [11]. After measuring the initial ROM of the cadaver cervical spines, an ACDF procedure was conducted in each of the seven cervical spines at C4–C5 and C6–C7 in a non-contiguous fashion [11]. After non-contiguous ACDF testing, the two plates from the prior two ACDF procedures were removed, and an additional ACDF procedure at C5–C6 was performed with the addition of a three-level plate at C4–C7 for contiguous ACDF measurements [11]. Sun et al. (2020) utilized eight finite element models (FEMs) constructed from computed tomography (CT) images of four males and four females (total of eight patients) with mild cervical degenerative disc disease (C2–C7) [7]. Non-contiguous ACDF (CoRoent Contour) and non-contiguous CDA (Prodisc-C) were performed at C3–C4 and C5–C6 with ROM testing in flexion, extension, bilateral side bend, and bilateral axial rotation [7]. Sun et al. (2023) utilized twelve FEMs constructed from CT images of six males and six females (total of twelve patients) with mild cervical spondylopathy [8]. For the hybrid cervical surgery in Sun et al. (2023), the ACDF used NuVasive Helix ACP and CoRoent Contour, whereas the CDA used Prodisc-C [8]. Wu, Meng, Wang, and colleagues (2019) used a single finite element model (FEM) from a healthy male (28 years old) without cervical disease [10]. Wu, Meng, Liu, and colleagues (2019) utilized a FEM from a healthy cervical spine (C2–C7) from a healthy 28-year-old male without cervical disease [9]. All studies using FEMs validated their ROM measurements to ensure they were similar to previously published studies [7,8,9,10]. Furthermore, four of the five included studies with FEMs used C3–C4 and C5–C6 as the two operative levels with the rationale that these levels are the more frequently involved levels in clinical practice. One study, using cadavers, used C4–C5 and C6–C7 as the two operative levels for non-contiguous surgery [11]. Refer to Table 2 for more information on study characteristics.
Table 2.
Information on the study characteristics and methodology of the five included articles. Abbreviations: ACDF; anterior cervical discectomy and fusion; CDA, cervical disc arthroplasty; HCS, hybrid cervical surgery; FEM, finite element model. Data include author, year of publication, method, model demographics, number of models, devices used, surgical levels, and comparison groups. Dashes indicate data not recorded in an individual study.
3.3. Non-Contiguous Hybrid Cervical Surgery Motion
The article by Sun et al. (2023) compared two types of hybrid cervical surgeries [8]. The CDA portion of the non-contiguous hybrid surgeries had significantly more lateral side bend ROM as compared to the initial non-operative cervical spine, regardless of if the CDA was the cephalad or caudal procedure in the hybrid cervical surgery [8]. Furthermore, the fusion–arthroplasty group with CDA at the caudal operative segment had significantly increased caudal non-operative segment ROM in extension (p = 0.015), whereas the arthroplasty–fusion group with CDA at the cephalad operative segment had significantly increased ROM at the cephalad non-operative segment during lateral side bend (p = 0.039) [8]. Overall, Sun et al. (2023) concluded that the differences in ROM at each of the operative segments were related to the biomechanical characteristics of the operative implants (ACDF or CDA) [8]. However, it is important to note that both combinations of HCS had no significant difference in total cervical ROM, indicating similar effects of both surgeries on overall cervical ROM [8]. According to the article by Wu, Meng, Liu, and colleagues (2019), the fusion–fusion (non-contiguous ACDF) comparison group for cervical surgery required far higher force to produce the same ROM in all directions compared to the fusion–arthroplasty and arthroplasty–fusion variants of HCS [9]. Whereas the cephalad, intermediate, and caudal non-operative segment had increased ROM compared to the initial non-operative cervical spine in the fusion–fusion control model, the intermediate non-operative segment had greater ROM than the other two segments [9]. This is in contrast to the two variants of HCS, which experienced more even changes in ROM in the non-operative level, regardless of variant type. Wu, Meng, Liu, and colleagues (2019) concluded that hybrid surgery variants (fusion–arthroplasty or arthroplasty–fusion) had less of an effect on the intermediate non-operative segment compared to the fusion–fusion control model [9].
3.4. Non-Contiguous Hybrid Cervical Surgery Intervertebral Disc Pressure
The fusion–arthroplasty variant of HCS had significantly higher IDP at the cephalad, intermediate, and caudal non-operative segments compared to the initial non-operative cervical spine in all ROM directions [8]. The arthroplasty–fusion variant of HCS had significantly higher IDP at the intermediate and caudal non-operative segments, but not at the cephalad segment, compared to the initial non-operative spine [8]. Both variants of hybrid surgery had relatively lower levels of IDP as compared to non-contiguous ACDF. Depending on the non-operative segment level, the non-contiguous ACDF model increased IDP from 62.9% to 72.5%, whereas the non-contiguous HCS variants increased IDP from 15.0% to 57.1% in the fusion–arthroplasty variant and 10.5% to 59.5% in the arthroplasty variant [9].
3.5. Non-Contiguous Hybrid Cervical Surgery Facet Contact Force
The cephalad and intermediate non-operative segments for both variants of HCS had significantly higher facet contact forces compared to the initial non-operative spine [8]. The fusion–arthroplasty variant of HCS had significantly higher facet contact forces at the cephalad non-operative segment (C2–C3) compared to the arthroplasty–fusion variant (p = 0.007), whereas the arthroplasty–fusion variant had significantly higher facet contact forces at the caudal non-operative segment (C6–C7) compared to the fusion–arthroplasty variant (p < 0.001) [8]. Interestingly, the variant type of HCS influenced the location and magnitude of maximum facet contact force. In the fusion–arthroplasty variant, there was a large increase in the maximum facet contact force (35.7%) in the cephalad non-operative segment treated via ACDF compared to the relatively small increase (2.5%) in the caudal non-operative segment treated via CDA [9]. This pattern repeated in the arthroplasty fusion variant, with the cephalad non-operative segment treated via CDA experiencing smaller increases in facet contact force (14.6%) and the caudal non-operative segment treated via ACDF experiencing larger increases in facet contact force (33.4%) compared to the initial non-operative cervical spine [9]. However, the increase in facet contact force was relatively similar for the intermediate non-operative segment in both variants of HCS [9].
3.6. Non-Contiguous Cervical Disc Arthroplasty Motion
In the study by Sun et al. (2020), the intermediate non-operative cervical segment (C4–C5) and the caudal non-operative cervical segment (C6–C7) had significantly more flexion ROM compared to the initial non-operative cervical spine [7]. The intermediate non-operative segment of the CDA procedure had significantly more lateral side-bend ROM, whereas the cephalad non-operative segment (C2–C3) had significantly less lateral side bend ROM compared to the initial non-operative cervical spine [7]. The cephalad, intermediate, and caudal non-operative segments for the non-contiguous CDA procedure had significantly less flexion, extension, lateral side bend, and axial rotation ROM compared to the non-contiguous ACDF procedure [7]. However, the cephalad operative level (C3–C4) and caudal operative level (C5–C6) had significantly higher ROM in all ROM directions for the non-contiguous CDA procedure compared to the non-contiguous ACDF procedure [7]. Therefore, the non-contiguous CDA procedure resulted in a higher magnitude of ROM in all levels, both operative and non-operative, compared to the non-contiguous ACDF procedure [7]. In the study by Wu, Meng, Wang, and colleagues (2019), the non-contiguous CDA resulted in changes of ROM of −28.8% to 0.5% when examining all cervical ROM directions for the cephalad non-operative segment [10]. Furthermore, the intermediate non-operative segment had changes of −5.5% to 0.3% and the caudal non-operative segment had changes of −0.5% to −9.9% when examining all cervical ROM directions [10].
3.7. Non-Contiguous Cervical Disc Arthroplasty Intervertebral Disc Pressure
There was no significant difference in the intervertebral disc pressure (IDP) at all levels between the non-contiguous CDA procedure and the initial non-operative cervical spine [7]. The IDP for the cephalad, intermediate, and caudal non-operative segment for non-contiguous CDA increased by 2.6% to 9.5%, 3.8% to 10.5%, and 4.0% to 8.3%, respectively, compared to the initial non-operative cervical spine [10].
3.8. Non-Contiguous Cervical Disc Arthroplasty Facet Contact Force
The facet joint contact force at the cephalad non-operative segment was significantly less for the CDA procedure compared to the initial non-operative cervical spine during extension ROM [7]. Furthermore, the cephalad, intermediate, and caudal non-operative segments had significantly less facet joint contact force in the non-contiguous CDA procedure compared to the non-contiguous ACDF procedure [7]. The maximum facet contact force in extension during non-contiguous CDA decreased by 13.0% at the cephalad non-operative segment, increased by 6.4% at the intermediate non-operative segment, and increased by 7.6% at the caudal non-operative segment compared to the initial non-operative cervical spine [10].
3.9. Non-Contiguous Anterior Cervical Discectomy and Fusion Motion
In the study by Finn et al. (2011), the flexion and extension ROM of the intermediate segment (C5–C6) for the non-contiguous ACDF procedure (C4–C5 and C6–C7) was significantly increased compared to the non-operative cervical spines at the beginning of the study (p = 0.022) [11]. However, though cervical side bending and rotation motion were approaching significance, there was no statistically significant difference between the intermittent segment in non-contiguous ACDF compared to the non-operative cervical spine [11]. The segment below C6–C7 had significantly increased ROM in all directions, whereas the segment above C4–C5 only had significantly increased rotation ROM [11]. The magnitude of ROM consisted of about a 35% increase and was similar in all non-operative cervical spine levels (C3–C4, C5–C6, and C7–T1) [11]. Moreover, this increase in ROM for non-contiguous ACDF (35% increase) was less than that seen at the cephalad and caudal non-operative cervical spine levels (C3–C4 and C7–T1) in the contiguous ACDF procedure (72% increase) [11]. This difference in magnitude was significant or nearing significance, with a higher magnitude in the contiguous ACDF compared to the non-contiguous ACDF [11]. When comparing plating systems for two-level non-contiguous ACDF and three-level contiguous ACDF, there was no difference in the ROM for the cephalad and caudal non-operative cervical segment between the two procedures [11]. Furthermore, the caudal non-operative cervical segment of the contiguous ACDF procedure had significant increased rotation ROM compared to the same segment in the non-contiguous ACDF procedure (p = 0.0409), whereas there was no significant difference seen at the cephalad non-operative cervical segment for both procedures (p = 0.43) [11]. In the study by Sun et al. (2020), the cephalad non-operative segment (C2–C3) and the caudal non-operative segment (C6–C7) for ACDF had significantly less flexion, extension, and axial rotation ROM compared to the initial non-operative cervical spine [7]. However, the intermediate non-operative segment (C4–C5) and the caudal non-operative segment (C6–C7) had significantly more lateral side bend ROM in the ACDF procedure compared to the initial non-operative cervical spine (p < 0.001 and p = 0.002, respectively) [7]. In the study by Wu, Meng, Wang, and colleagues (2019), the non-contiguous ACDF caused increases in ROM of the cephalad non-operative segment (C2–C3) from 29.0 to 77.7%, with the most ROM observed during axial rotation, compared to the initial non-operative cervical spine [10]. Furthermore, non-contiguous ACDF resulted in an increase in the intermediate segment (C4–C5) of 39.4% to 89.2% and 35.2% to 74.3% in the caudal segment (C6–C7) compared to the initial non-operative cervical spine [10].
3.10. Non-Contiguous Anterior Cervical Discectomy and Fusion Intervertebral Disc Pressure
The non-contiguous ACDF procedure had significantly higher IDP at the cephalad and caudal non-operative segments compared to the initial non-operative cervical spine. Furthermore, the non-contiguous ACDF procedure had significantly higher IDP at the cephalad, intermediate, and caudal non-operative segments compared to the non-contiguous CDA procedure in flexion, extension, lateral side bend, and axial rotation [7]. Non-contiguous ACDF increased IDP in the cephalad non-operative segment by 52.2% to 66.7% depending on cervical ROM direction compared to the initial non-operative cervical spine, whereas IDP increased in the intermediate non-operative segment by 61.5% to 71.0% depending on cervical ROM [10]. For the caudal non-operative segment, the IDP increased by 69.2% to 80.0% depending on cervical ROM compared to the initial non-operative cervical spine [10].
3.11. Non-Contiguous Anterior Cervical Discectomy and Fusion Facet Contact Force
In extension ROM, the facet joint contact force of the non-contiguous ACDF procedure was significantly more than the initial non-operative cervical spine and the non-contiguous CDA procedure [7]. The maximum facet contact force in cervical extension increased by 36.5% in the cephalad non-operative segment, 54.2% in the intermediate non-operative segment, and 37.4% in the caudal non-operative segment compared to the initial non-operative cervical spine [10]. According to Wu, Meng, Liu, and colleagues (2019), the maximum increase in facet contact force was 50.7% in the cephalad non-operative segment, 54.3% in the intermediate non-operative segment, and 37.6% in the caudal non-operative segment in the non-contiguous ACDF model compared to the initial non-operative cervical spine.
4. Discussion
This study represents the first systematic review to examine the biomechanics of non-contiguous ACDF, CDA, and HCS to date, with numerous systematic reviews examining the biomechanics and clinical outcomes for these cervical surgeries performed in a contiguous manner in the literature [1,2,3,4,5,12,13,14]. CDDD is a common clinical spinal pathology that has been historically treated with ACDF, although procedures such as CDA and HCS are gaining popularity in the literature [12,15,24,25,26]. These procedures have been advocated as traditional ACDF has been associated with various long-term adverse events, such as adjacent segment disease (ASD), in which increased ROM from non-operative segments above and below the fusion level accelerate CDDD [15,27,28,29,30]. Due to this fact, there has been extensive research in the literature comparing these three cervical surgeries, when performed in a contiguous manner, to one another in terms of clinical and biomechanical outcomes [1,2,3,4,5,12,14,15].
Though a recent meta-analysis by Hollyer and colleagues (2020) concluded that contiguous HCS results in less ROM at the adjacent non-operative cervical segments compared to contiguous ACDF, it was unknown if these changes would continue or shift when comparing non-contiguous HCS versus non-contiguous ACDF [15]. The results of this systematic review indicated that non-contiguous two-level HCS experienced less drastic changes in range-of-motion (ROM), as well as decreased intervertebral disc pressure (IDP), compared to non-contiguous two-level ACDF. This is evident in the included study by Wu, Meng, Liu, and colleagues (2019), which demonstrates that non-contiguous two-level HCS, regardless of variant, had less of an impact on the intermediate non-operative segment compared to non-contiguous two-level ACDF [9]. As increased ROM has the potential to cause ASD and accelerate CDDD, this finding in both contiguous and non-contiguous HCS cautiously suggests a possible benefit of HCS over ACDF in this metric. However, it remains to be seen how these biomechanical differences between non-contiguous HCS and non-contiguous ACDF impact clinical outcomes and actual rates of ASD and subsequent reoperation. Due to the relatively high incidence and burden of ASD after cervical surgeries involving segmental fusion, more research is needed on this subject in regard to non-contiguous cervical surgeries for the possible prevention of ASD at nearby segments [27,28,29,30]. Notably, the results of this study are far from proving the superiority of non-contiguous HCS compared to non-contiguous ACDF for biomechanical outcomes, let alone clinical outcomes. Similar to the larger systematic review and meta-analysis by Hollyer and colleagues (2020) concerning contiguous cervical surgeries, the low number of studies, combined with the low quality of evidence, inhibits any solid recommendation from being made [15]. However, this study has value in that it lays the foundation for future research on the biomechanical and kinematic outcomes comparing non-contiguous HCS and non-contiguous ACDF, as well as provides a framework based on the current literature given the paucity of evidence on this subject.
When examining CDA biomechanical outcomes, it is important to note that one of the original purposes of the CDA procedure was to preserve motion and decrease force at the operative segment to prevent ASD. It is not surprising that many studies have then examined these biomechanical outcomes for contiguous CDA procedures [1,5,12,13,14]. However, this systematic review adds to the literature by showing that non-contiguous two-level CDA resulted in more cervical ROM and less non-operative segment facet contact force compared to non-contiguous two level ACDF. As with HCS, the superiority of CDA over ACDF has yet to be proven for contiguous procedures, let alone for non-contiguous procedures [15]. Yet, this study compiles data that indicates similar ROM and force outcomes occur in non-contiguous models. Unfortunately, this study could not comment on biomechanical comparisons between non-contiguous HCS and non-contiguous CDA, which is a comparison that needs to be explored more in the literature. The landmark meta-analysis by Hollyer and colleagues (2020) indicated that although patients treated with HCS had a quicker return to work than patients treated with ACDF, patients treated with CDA had a quicker return to work than HCS patients. Therefore, future biomechanical comparisons need to be performed between non-contiguous HCS and non-contiguous ACDF to investigate these relationships.
This systematic review also indicated that there was less cephalad and caudad non-operative segment ROM in non-contiguous two-level ACDF compared to contiguous three-level ACDF. Although far from proving superiority, the findings of this study suggest that spine surgeons choosing between ACDF variants for non-contiguous CDDD should consider non-contiguous ACDF as a potential viable treatment option, given the risk of ASD [27,28,29,30]. However, high-quality randomized controlled trials are needed before any solid recommendations can be made when choosing contiguous or non-contiguous ACDF for non-contiguous CDDD. Despite these factors, this systematic review paves the way for future research to further investigate these possible biomechanical relationships and the subsequent impact on patient outcomes.
There are certainly multiple limitations that impact the interpretation of these biomechanical results regarding non-contiguous ACDF, CDA, and HCS. First, although comprehensive of all the currently published articles on this subject, this systematic review was only able to include five articles on this topic, with a total sample size of seven human cadavers and sixteen FEMs constructed from human CT images. Therefore, the certainty of this data is “very low”, as indicated by the GRADE scale, due to the small sample size leading to the risk of bias, as well as the non-randomized nature of the included articles. Due to the heterogeneity of the data from the five included articles, a meta-analysis could not be performed and a narrative approach to systematic review was undertaken. High-quality studies with similar methodology should be performed in the future to allow for meta-analysis. Furthermore, this study mostly focused on surgical levels C3–C4 and C5–C6, which limits applicability and generalizability to non-contiguous cervical surgeries at other levels of the cervical spine. It is unknown how biomechanics and/or kinematics may differ with higher or lower cervical spine surgeries. Likewise, the included articles in this systematic review only tested two-level non-contiguous cervical surgeries, suggesting that the impact of multi-level non-contiguous cervical surgeries remains unknown. Future research should focus on studies with larger sample sizes, as well as cervical surgeries in different locations throughout the cervical spine with varying levels of fusion. Another limitation of this study is that all of the subjects/models were representative of healthy or mildly diseased cervical spines. As non-contiguous ACDF, CDA, and HCS are treatments for advanced CDDD, it is unknown how biomechanics may change with identical experiments performed on models with severe CDDD [15]. More research is needed to explore the biomechanics of non-contiguous cervical surgeries in patients with severe CDDD, as well as how these biomechanical outcomes translate to clinical outcomes. Finally, more research is needed in live human patients, likely through advanced imaging studies, as cadavers and/or models have limitations and different variables compared to live subjects.
5. Conclusions
This systematic review suggested that non-contiguous two-level HCS could experience less drastic ROM changes throughout the cervical spine and decreased IDP compared to non-contiguous two-level ACDF. In this study, non-contiguous two-level ACDF resulted in more non-operative segment facet contact force than non-contiguous two-level CDA and more IDP than non-contiguous two-level HCS. Contiguous three-level ACDF results in more non-operative segment ROM compared to non-contiguous two-level ACDF, indicating the potential for viable treatment alternatives for non-contiguous CDDD. Overall, biomechanical outcomes for non-contiguous cervical procedures are similar to those of contiguous cervical procedures. More research with high-level-evidence studies is needed to determine the biomechanical impact on clinical outcomes and investigate the potential superiority of one cervical procedure over another for non-contiguous CDDD.
Author Contributions
Conceptualization, A.T.A., K.C.W., A.N.B., K.T.C. and J.C.H.; methodology, A.T.A., A.N.B., A.F., K.S., K.T.C. and J.C.H.; software, A.N.B.; validation, A.T.A., K.C.W., A.M., A.N.B., K.T.C. and J.C.H.; formal analysis, A.N.B.; investigation, A.N.B., A.F. and K.S.; resources, A.N.B., A.F., K.S., K.T.C. and J.C.H.; data curation, A.N.B.; writing—original draft preparation, A.N.B.; writing—review and editing, A.T.A., K.C.W., A.M., A.N.B., K.T.C. and J.C.H.; visualization, A.T.A., K.T.C. and J.C.H.; supervision, A.T.A., K.T.C. and J.C.H.; project administration, A.T.A., A.N.B., K.T.C. and J.C.H.; funding acquisition, none. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No data are available for this study, as all data are publicly available.
Acknowledgments
Thank you to Duke University and Cleveland Clinic Akron General for the support in conducting this project.
Conflicts of Interest
A.T.A. receives consulting fees from QPIX. All other authors declare no conflict of interest.
References
- Safavi-Abbasi, S.; Reyes, P.M.; Abjornson, C.; Crawford, N.R. Feasibility and Biomechanics of Multilevel Arthroplasty and Combined Cervical Arthrodesis and Arthroplasty. Clin. Spine Surg. 2016, 29, E522–E531. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.D.; Coric, D.; Khachatryan, A.; Brady, B.L.; Lillehaugen, T.; McCormack, M.; Dolman, W.B.; Ditto, R. A real-world analysis of hybrid CDA and ACDF compared to multilevel ACDF. BMC Musculoskelet. Disord. 2023, 24, 191. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Meng, F.; Ding, Y.; Li, J.; Han, J.; Zhang, X.; Dong, W. Comprehensive Analysis of Hybrid Surgery and Anterior Cervical Discectomy and Fusion in Cervical Diseases: A Meta-Analysis. Medicine 2020, 99, e19055. [Google Scholar] [CrossRef]
- Wu, T.-K.; Wang, B.-Y.; Meng, Y.; Ding, C.; Yang, Y.; Lou, J.-G.; Liu, H. Multilevel cervical disc replacement versus multilevel anterior discectomy and fusion: A meta-analysis. Medicine 2017, 96, e6503. [Google Scholar] [CrossRef] [PubMed]
- Jia, Z.; Mo, Z.; Ding, F.; He, Q.; Fan, Y.; Ruan, D. Hybrid surgery for multilevel cervical degenerative disc diseases: A systematic review of biomechanical and clinical evidence. Eur. Spine J. 2014, 23, 1619–1632. [Google Scholar] [CrossRef]
- Brinjikji, W.; Luetmer, P.; Comstock, B.; Bresnahan, B.; Chen, L.; Deyo, R.; Halabi, S.; Turner, J.; Avins, A.; James, K.; et al. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. Am. J. Neuroradiol. 2015, 36, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Sun, S.; Zhang, T.; Kong, C.; Wang, W.; Lu, S. Biomechanical comparison of noncontiguous cervical disc arthroplasty and noncontiguous cervical discectomy and fusion in the treatment of noncontinuous cervical degenerative disc disease: A finite element analysis. J. Orthop. Surg. Res. 2020, 15, 36. [Google Scholar] [CrossRef]
- Sun, X.; Zhang, Q.; Cao, L.; Wang, J.; Huang, J.; Liu, Y.; Zhang, Y.; Song, Z.; Tang, W.; Chen, Y.; et al. Biomechanical effects of hybrid constructions in the treatment of noncontinuous cervical spondylopathy: A finite element analysis. J. Orthop. Surg. Res. 2023, 18, 57. [Google Scholar] [CrossRef]
- Wu, T.-K.; Meng, Y.; Liu, H.; Wang, B.-Y.; Hong, Y.; Rong, X.; Ding, C.; Chen, H. Biomechanical effects on the intermediate segment of noncontiguous hybrid surgery with cervical disc arthroplasty and anterior cervical discectomy and fusion: A finite element analysis. Spine J. 2019, 19, 1254–1263. [Google Scholar] [CrossRef]
- Wu, T.-K.; Meng, Y.; Wang, B.-Y.; Rong, X.; Hong, Y.; Ding, C.; Chen, H.; Liu, H. Biomechanics following skip-level cervical disc arthroplasty versus skip-level cervical discectomy and fusion: A finite element-based study. BMC Musculoskelet. Disord. 2019, 20, 49. [Google Scholar] [CrossRef]
- Finn, M.A.; Samuelson, M.M.; Bishop, F.; Bachus, K.N.; Brodke, D.S. Two-level noncontiguous versus three-level anterior cervical discectomy and fusion: A biomechanical comparison. Spine 2011, 36, 448–453. [Google Scholar] [CrossRef]
- Liu, B.; Zeng, Z.; Van Hoof, T.; Kalala, J.P.; Liu, Z.; Wu, B. Comparison of hybrid constructs with 2-level artificial disc replacement and 2-level anterior cervical discectomy and fusion for surgical reconstruction of the cervical spine: A kinematic study in whole cadavers. Med. Sci. Monit. 2015, 21, 1031–1037. [Google Scholar] [CrossRef]
- Lee, M.J.; Dumonski, M.; Phillips, F.M.; Voronov, L.I.; Renner, S.M.; Carandang, G.; Havey, R.M.; Patwardhan, A.G. Disc replacement adjacent to cervical fusion: A biomechanical comparison of hybrid construct versus two-level fusion. Spine 2011, 36, 1932–1939. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, B.W.; Hu, N.; Zorn, C.M.; McAfee, P.C. Biomechanical comparison of single- and two-level cervical arthroplasty versus arthrodesis: Effect on adjacent-level spinal kinematics. Spine J. 2010, 10, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Hollyer, M.A.; Gill, E.C.; Ayis, S.; Demetriades, A.K. The safety and efficacy of hybrid surgery for multilevel cervical degenerative disc disease versus anterior cervical discectomy and fusion or cervical disc arthroplasty: A systematic review and meta-analysis. Acta Neurochir. 2020, 162, 289–303. [Google Scholar] [CrossRef]
- Zhang, Z.; Li, Y.; Jiang, W. A comparison of zero-profile anchored spacer (ROI-C) and plate fixation in 2-level noncontiguous anterior cervical discectomy and fusion- a retrospective study. BMC Musculoskelet. Disord. 2018, 19, 119. [Google Scholar] [CrossRef]
- Qizhi, S.; Lei, S.; Peijia, L.; Hanping, Z.; Hongwei, H.; Junsheng, C.; Jianmin, L. A Comparison of Zero-Profile Devices and Artificial Cervical Disks in Patients With 2 Noncontiguous Levels of Cervical Spondylosis. Clin. Spine Surg. 2016, 29, E61–E66. [Google Scholar] [CrossRef] [PubMed]
- Kan, L.; Kang, J.; Gao, R.; Chen, X.; Jia, L. Clinical and radiological results of two hybrid reconstructive techniques in noncontiguous 3-level cervical spondylosis. J. Neurosurg. Spine 2014, 21, 944–950. [Google Scholar] [CrossRef]
- Shi, S.; Zheng, S.; Li, X.-F.; Yang, L.-L.; Liu, Z.-D.; Yuan, W. Comparison of a Stand-Alone Anchored Spacer Versus Plate-Cage Construct in the Treatment of Two Noncontiguous Levels of Cervical Spondylosis: A Preliminary Investigation. World Neurosurg. 2016, 89, 285–292. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (Minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Bao, W.; Wang, Z.; Zhou, F.; Zou, J.; Jiang, W.; Yang, H.; Zhang, Z.; Zhu, X. Comparison of the clinical effects of zero-profile anchored spacer (ROI-C) and conventional cage-plate construct for the treatment of noncontiguous bilevel of cervical degenerative disc disease (CDDD): A minimum 2-year follow-up. Medicine 2018, 97, e9808. [Google Scholar] [CrossRef]
- Wang, H.-R.; Li, X.-L.; Dong, J.; Yuan, F.-L.; Zhou, J. Skip-level anterior cervical discectomy and fusion with self-locking stand-alone PEEK cages for the treatment of 2 noncontiguous levels of cervical spondylosis. J. Spinal Disord. Tech. 2013, 26, E286–E292. [Google Scholar] [CrossRef]
- Dong, L.; Xu, Z.; Chen, X.; Wang, D.; Li, D.; Liu, T.; Hao, D. The change of adjacent segment after cervical disc arthroplasty compared with anterior cervical discectomy and fusion: A meta-analysis of randomized controlled trials. Spine J. 2017, 17, 1549–1558. [Google Scholar] [CrossRef] [PubMed]
- Harada, G.K.; Tao, Y.; Louie, P.K.; Basques, B.A.; Galbusera, F.; Niemeyer, F.; Wilke, H.; Goldberg, E.; An, H.S.; Samartzis, D. Cervical spine MRI phenotypes and prediction of pain, disability and adjacent segment degeneration/disease after ACDF. J. Orthop. Res. 2021, 39, 657–670. [Google Scholar] [CrossRef]
- Carrier, C.S.; Bono, C.M.; Lebl, D.R. Evidence-based analysis of adjacent segment degeneration and disease after ACDF: A systematic review. Spine J. 2013, 13, 1370–1378. [Google Scholar] [CrossRef] [PubMed]
- Broida, S.E.; Murakami, K.; Abedi, A.; Meisel, H.-J.; Hsieh, P.; Wang, J.; Jain, A.; Buser, Z.; Yoon, S.T. Clinical risk factors associated with the development of adjacent segment disease in patients undergoing ACDF: A systematic review. Spine J. 2023, 23, 146–156. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhang, B.; Liu, H.; Wu, Y.; Zhu, Q. Cervical disc arthroplasty versus anterior cervical discectomy and fusion for incidence of symptomatic adjacent segment disease: A meta-analysis of prospective randomized controlled trials. Spine 2016, 41, 1493–1502. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).