
Assessment of Gait Following Locking Plate Fixation of a Tibial Segmental Defect and Cast Immobilization in Goats

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Goats
2.2. Surgery
2.3. Cast Immobilization
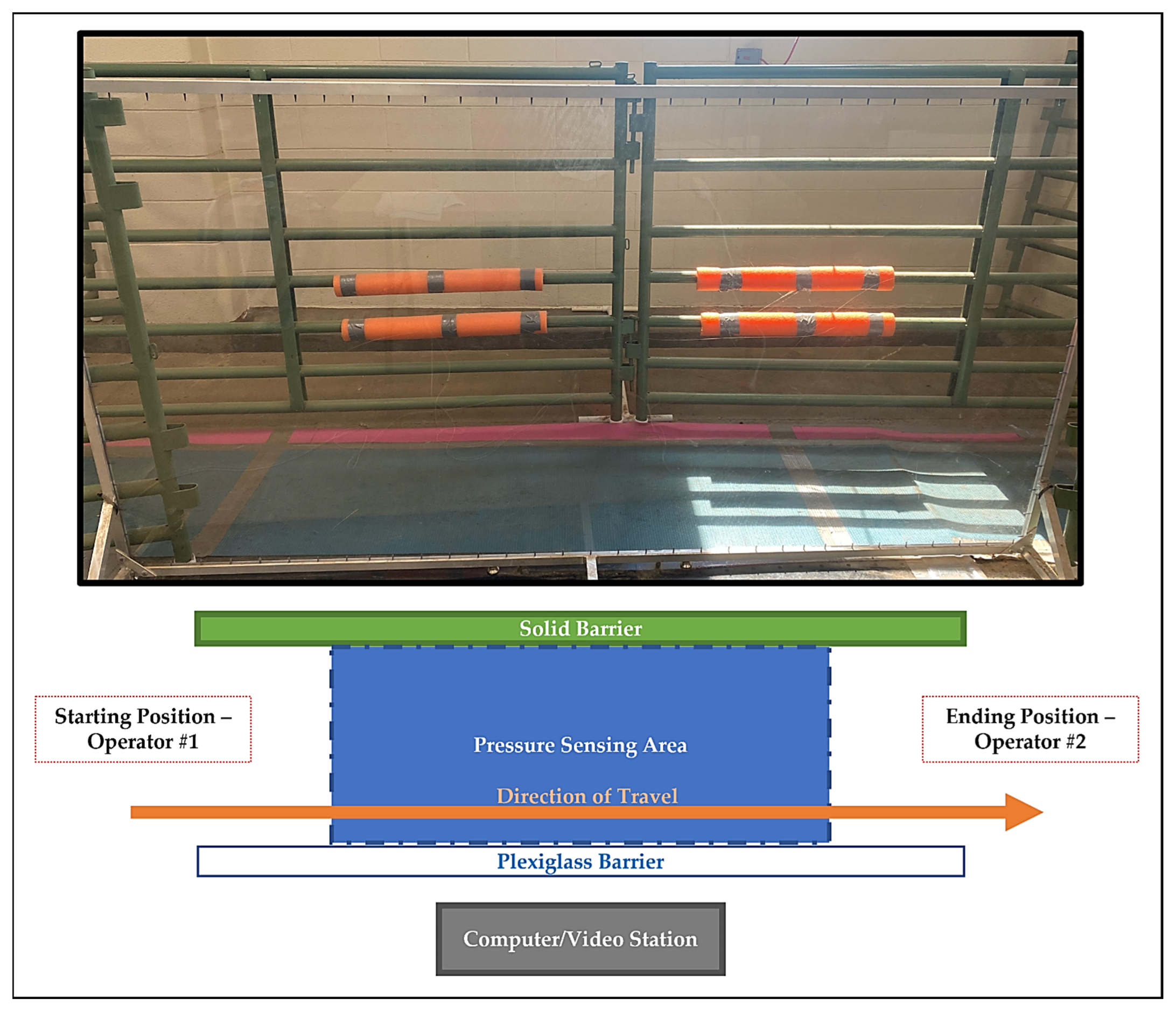
2.4. Biomechanical Data Collection
2.5. Asymmetry Indices
2.6. Statistical Analysis
3. Results
3.1. Goats
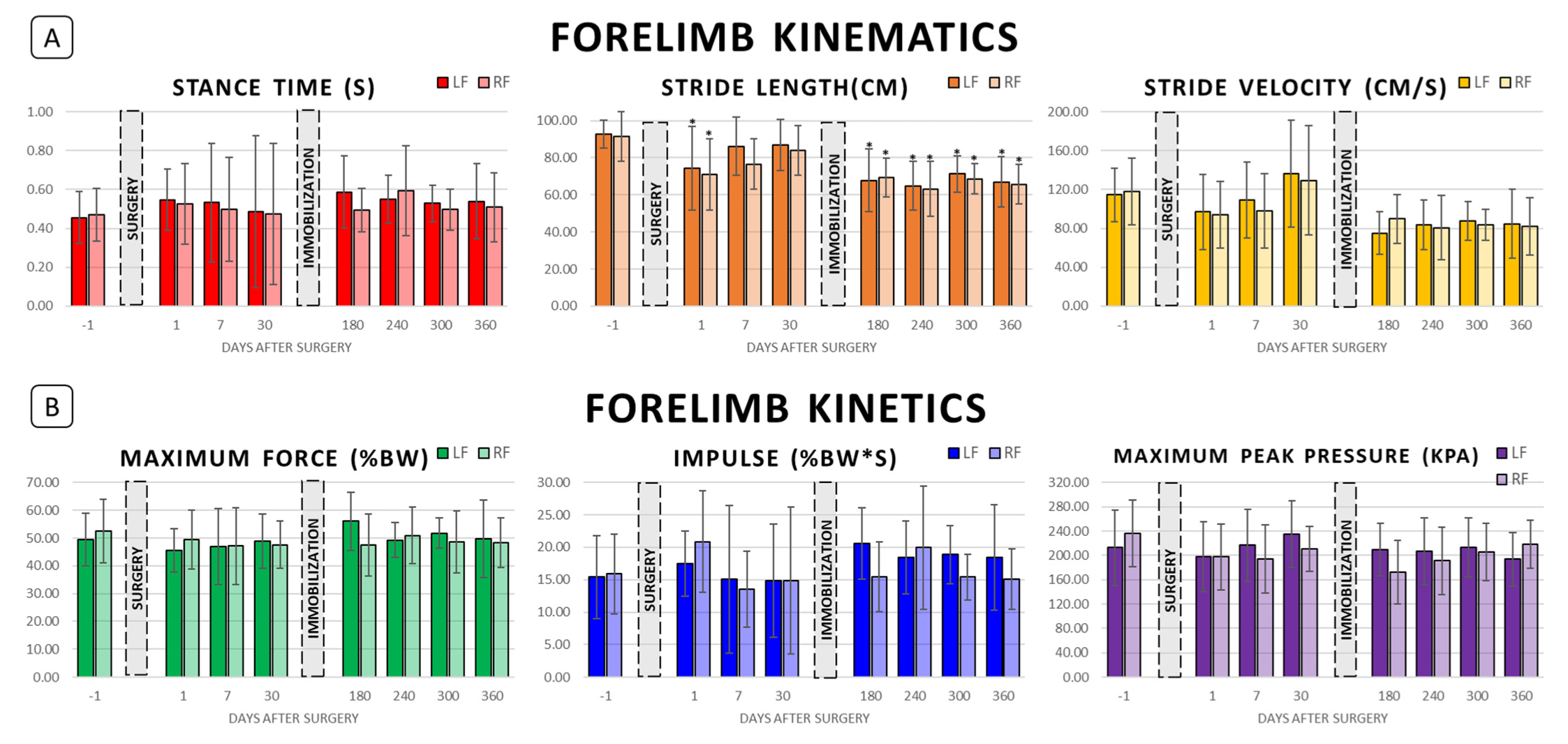
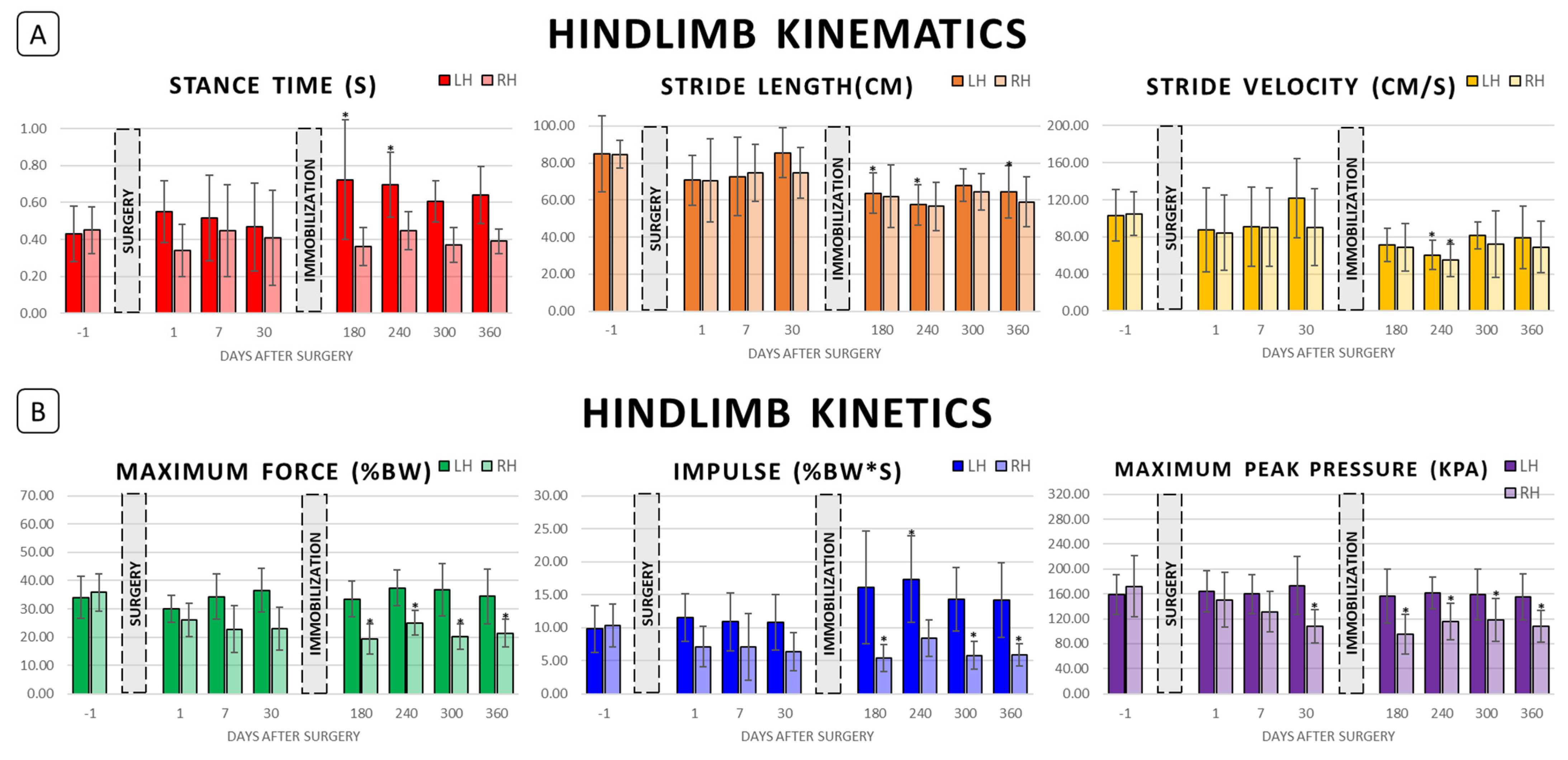
3.2. Post-Surgical Biomechanics (Days 1–30)
3.3. Post-Immobilization Biomechanics (Days 180–360)
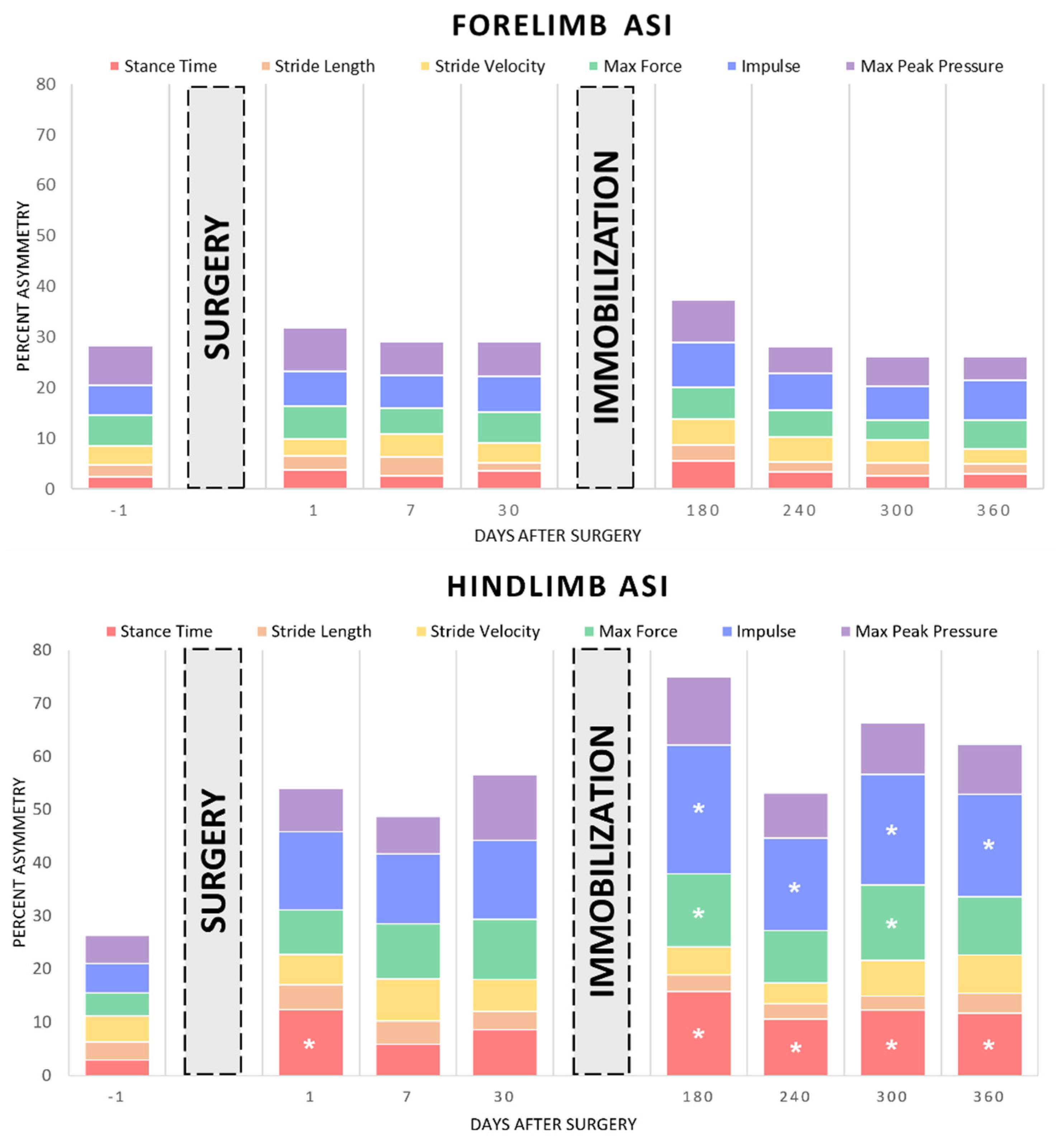
3.4. Asymmetry Indices
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dias, I.R.; Camassa, J.A.; Bordelo, J.A.; Babo, P.S.; Viegas, C.A.; Dourado, N.; Reis, R.L.; Gomes, M.E. Preclinical and Translational Studies in Small Ruminants (Sheep and Goat) as Models for Osteoporosis Research. Curr. Osteoporos. Rep. 2018, 16, 182–197. [Google Scholar] [CrossRef] [PubMed]
- Christou, C.; Oliver, R.A.; Pelletier, M.H.; Walsh, W.R. Ovine model for critical-size tibial segmental defects. Comp. Med. 2014, 64, 377–385. [Google Scholar] [PubMed]
- Atarod, M.; Frank, C.B.; Shrive, N.G. Kinematic and Kinetic Interactions During Normal and ACL-Deficient Gait: A Longitudinal In Vivo Study. Ann. Biomed. Eng. 2014, 42, 566–578. [Google Scholar] [CrossRef] [PubMed]
- Diogo, C.C.; Camassa, J.A.; Fonseca, B.; Maltez da Costa, L.; Pereira, J.E.; Filipe, V.; Couto, P.A.; Raimondo, S.; Armada-da-Silva, P.A.; Maurício, A.C.; et al. A Comparison of Two-Dimensional and Three-Dimensional Techniques for Kinematic Analysis of the Sagittal Motion of Sheep Hindlimbs During Walking on a Treadmill. Front. Vet. Sci. 2021, 8, 545708. [Google Scholar] [CrossRef] [PubMed]
- Grzeskowiak, R.M.; Rifkin, R.E.; Croy, E.G.; Steiner, R.C.; Seddighi, R.; Mulon, P.-Y.; Adair, H.S.; Anderson, D.E. Temporal Changes in Reverse Torque of Locking-Head Screws Used in the Locking Plate in Segmental Tibial Defect in Goat Model. Front. Surg. 2021, 8, 637268. [Google Scholar] [CrossRef] [PubMed]
- McKinley, T.O.; Natoli, R.M.; Fischer, J.P.; Rytlewski, J.D.; Scofield, D.C.; Usmani, R.; Kuzma, A.; Griffin, K.S.; Jewell, E.; Childress, P.; et al. Internal Fixation Construct and Defect Size Affect Healing of a Translational Porcine Diaphyseal Tibial Segmental Bone Defect. Mil. Med. 2021, 186, e1115–e1123. [Google Scholar] [CrossRef]
- Reichert, J.C.; Saifzadeh, S.; Wullschleger, M.E.; Epari, D.R.; Schütz, M.A.; Duda, G.N.; Schell, H.; Van Griensven, M.; Redl, H.; Hutmacher, D.W. The challenge of establishing preclinical models for segmental bone defect research. Biomaterials 2009, 30, 2149–2163. [Google Scholar] [CrossRef]
- McGovern, J.A.; Griffin, M.; Hutmacher, D.W. Animal models for bone tissue engineering and modelling disease. Dis. Model. Mech. 2018, 11, dmm033084. [Google Scholar] [CrossRef]
- Zeiter, S.; Koschitzki, K.; Alini, M.; Jakob, F.; Rudert, M.; Herrmann, M. Evaluation of Preclinical Models for the Testing of Bone Tissue-Engineered Constructs. Tissue Eng. Part C Methods 2020, 26, 107–117. [Google Scholar] [CrossRef]
- Xu, G.-H.; Liu, B.; Zhang, Q.; Wang, J.; Chen, W.; Liu, Y.-J.; Peng, A.Q.; Zhang, Y.-Z. Biomechanical comparison of gourd-shaped LCP versus LCP for fixation of comminuted tibial shaft fracture. J. Huazhong Univ. Sci. Technol. Med. Sci. 2013, 33, 250–257. [Google Scholar] [CrossRef]
- Stoffel, K.; Dieter, U.; Stachowiak, G.; Gächter, A.; Kuster, M.S. Biomechanical testing of the LCP—How can stability in locked internal fixators be controlled? Injury 2003, 34 (Suppl. 2), B11–B19. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, R.A.; Aithal, H.P.; Amarpal; Kinjavdekar, P.; Gope, P.C.; Madhu, D.N. Biomechanical properties of a novel locking compression plate to stabilize oblique tibial osteotomies in buffaloes. Vet. Surg. 2021, 50, 444–454. [Google Scholar] [CrossRef] [PubMed]
- Xue, Z.; Xu, H.; Ding, H.; Qin, H.; An, Z. Comparison of the effect on bone healing process of different implants used in minimally invasive plate osteosynthesis: Limited contact dynamic compression plate versus locking compression plate. Sci. Rep. 2016, 6, 37902. [Google Scholar] [CrossRef] [PubMed]
- Henkel, J.; Medeiros Savi, F.; Berner, A.; Fountain, S.; Saifzadeh, S.; Steck, R.; Epari, D.R.; Woodruff, M.A.; Knackstedt, M.; Schuetz, M.A.; et al. Scaffold-guided bone regeneration in large volume tibial segmental defects. Bone 2021, 153, 116163. [Google Scholar] [CrossRef]
- Reichert, J.C.; Cipitria, A.; Epari, D.R.; Saifzadeh, S.; Krishnakanth, P.; Berner, A.; Woodruff, M.A.; Schell, H.; Mehta, M.; Schuetz, M.A.; et al. A tissue engineering solution for segmental defect regeneration in load-bearing long bones. Sci. Transl. Med. 2012, 4, 141ra93. [Google Scholar] [CrossRef]
- Marcondes, G.D.M.; Paretsis, N.F.; Souza, A.F.D.; Ruivo, M.R.B.A.; Rego, M.A.F.; Nóbrega, F.S.; Cortopassi, S.R.G.; De Zoppa, A.L.D.V. Locking compression plate fixation of critical-sized bone defects in sheep. Development of a model for veterinary bone tissue engineering. Acta Cirúrgica Bras. 2021, 36, e360601. [Google Scholar] [CrossRef]
- Seebeck, P.; Thompson, M.S.; Parwani, A.; Taylor, W.R.; Schell, H.; Duda, G.N. Gait evaluation: A tool to monitor bone healing? Clin. Biomech. 2005, 20, 883–891. [Google Scholar] [CrossRef]
- Schell, H.; Thompson, M.S.; Bail, H.J.; Hoffmann, J.-E.; Schill, A.; Duda, G.N.; Lienau, J. Mechanical induction of critically delayed bone healing in sheep: Radiological and biomechanical results. J. Biomech. 2008, 41, 3066–3072. [Google Scholar] [CrossRef]
- Stewart, H.L.; Werpy, N.M.; McIlwraith, C.W.; Kawcak, C.E. Physiologic effects of long-term immobilization of the equine distal limb. Vet. Surg. 2020, 49, 840–851. [Google Scholar] [CrossRef]
- Oliveira Milani, J.G.P.; Matheus, J.P.C.; Gomide, L.B.; Volpon, J.B.; Shimano, A.C. Biomechanical Effects of Immobilization and Rehabilitation on the Skeletal Muscle of Trained and Sedentary Rats. Ann. Biomed. Eng. 2008, 36, 1641–1648. [Google Scholar] [CrossRef]
- Kaneguchi, A.; Ozawa, J.; Minamimoto, K.; Yamaoka, K. Morphological and biomechanical adaptations of skeletal muscle in the recovery phase after immobilization in a rat. Clin. Biomech. 2020, 75, 104992. [Google Scholar] [CrossRef] [PubMed]
- Clark, B.C.; Taylor, J.L.; Hoffman, R.L.; Dearth, D.J.; Thomas, J.S. Cast immobilization increases long-interval intracortical inhibition. Muscle Nerve 2010, 42, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Kannus, R.; Jòzsa, L.; Renström, R.; Järvtoen, M.; Kvist, M.; Lento, M.; Oja, P.; Vuorl, I. The effects of training, immobilization and remobilization on musculoskeletal tissue. Scand. J. Med. Sci. Sport. 1992, 2, 100–118. [Google Scholar] [CrossRef]
- Aufwerber, S.; Heijne, A.; Edman, G.; Grävare Silbernagel, K.; Ackermann, P.W. Early mobilization does not reduce the risk of deep venous thrombosis after Achilles tendon rupture: A randomized controlled trial. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, K.; Oga, S.; Goto, K.; Sakamoto, J.; Sasaki, R.; Honda, Y.; Kataoka, H.; Okita, M. Voluntary Forelimbs Exercise Reduces Immobilization-Induced Mechanical Hyperalgesia in the Rat Hind Paw. Pain Res. Manag. 2021, 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Caplan, N.; Forbes, A.; Radha, S.; Stewart, S.; Ewen, A.; Gibson, A.S.C.; Kader, D. Effects of 1 Week of Unilateral Ankle Immobilization on Plantar-Flexor Strength, Balance, and Walking Speed: A Pilot Study in Asymptomatic Volunteers. J. Sport Rehabil. 2015, 24, 156–162. [Google Scholar] [CrossRef]
- Nahm, N.; Bey, M.J.; Liu, S.; Guthrie, S.T. Ankle Motion and Offloading in Short Leg Cast and Low and High Fracture Boots. Foot Ankle Int. 2019, 40, 1416–1423. [Google Scholar] [CrossRef]
- Zhang, S.; Clowers, K.G.; Powell, D. Ground reaction force and 3D biomechanical characteristics of walking in short-leg walkers. Gait Posture 2006, 24, 487–492. [Google Scholar] [CrossRef]
- Kadel, N.J.; Segal, A.; Orendurff, M.; Shofer, J.; Sangeorzan, B. The Efficacy of Two Methods of Ankle Immobilization in Reducing Gastrocnemius, Soleus, and Peroneal Muscle Activity during Stance Phase of Gait. Foot Ankle Int. 2004, 25, 406–409. [Google Scholar] [CrossRef]
- Rifkin, R.E.; Grzeskowiak, R.M.; Mulon, P.-Y.; Adair, H.S.; Biris, A.S.; Dhar, M.; Anderson, D.E. Use of a pressure-sensing walkway system for biometric assessment of gait characteristics in goats. PLoS ONE 2019, 14, e0223771. [Google Scholar] [CrossRef]
- Reppert, E.J.; Kleinhenz, M.D.; Viscardi, A.; Montgomery, S.R.; Crane, A.R.; Coetzee, J.F. Development and evaluation of two different lameness models in meat goats, a pilot study. Transl. Anim. Sci. 2020, 4, txaa193. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.; Oliveira, M.D.; Nunes, T.; Stilwell, G. Making the case for developing alternative lameness scoring systems for dairy goats. Appl. Anim. Behav. Sci. 2015, 171, 94–100. [Google Scholar] [CrossRef]
- Battini, M.; Renna, M.; Giammarino, M.; Battaglini, L.; Mattiello, S. Feasibility and Reliability of the AWIN Welfare Assessment Protocol for Dairy Goats in Semi-extensive Farming Conditions. Front. Vet. Sci. 2021, 8, 731927. [Google Scholar] [CrossRef]
- Coetzee, J.F.; Mosher, R.A.; Anderson, D.E.; Robert, B.; Kohake, L.E.; Gehring, R.; White, B.J.; Kukanich, B.; Wang, C. Impact of oral meloxicam administered alone or in combination with gabapentin on experimentally induced lameness in beef calves1. J. Anim. Sci. 2014, 92, 816–829. [Google Scholar] [CrossRef] [PubMed]
- Netukova, S.; Duspivova, T.; Tesar, J.; Bejtic, M.; Baxa, M.; Ellederova, Z.; Szabo, Z.; Krupicka, R. Instrumented pig gait analysis: State-of-the-art. J. Vet. Behav. 2021, 45, 51–59. [Google Scholar] [CrossRef]
- Egenvall, A.; Marr, C.M.; Byström, A. Study design synopsis: How to conduct, prepare, analyse and report equine biomechanical studies. Equine Vet. J. 2021, 53, 645–648. [Google Scholar] [CrossRef]
- Connor, P.; Ross, A. Biometric recognition by gait: A survey of modalities and features. Comput. Vis. Image Underst. 2018, 167, 1–27. [Google Scholar] [CrossRef]
- Meijer, E.; Bertholle, C.P.; Oosterlinck, M.; Van Der Staay, F.; Back, W.; Van Nes, A. Pressure mat analysis of the longitudinal development of pig locomotion in growing pigs after weaning. BMC Vet. Res. 2014, 10, 37. [Google Scholar] [CrossRef] [PubMed]
- Meijer, E.; Oosterlinck, M.; Van Nes, A.; Back, W.; Van Der Staay, F.J. Pressure mat analysis of naturally occurring lameness in young pigs after weaning. BMC Vet. Res. 2014, 10, 193. [Google Scholar] [CrossRef]
- Fanchon, L.; Grandjean, D. Accuracy of asymmetry indices of ground reaction forces for diagnosis of hind limb lameness in dogs. Am. J. Vet. Res. 2007, 68, 1089–1094. [Google Scholar] [CrossRef]
- Kano, W.T.; Rahal, S.C.; Agostinho, F.S.; Mesquita, L.R.; Santos, R.R.; Monteiro, F.O.B.; Castilho, M.S.; Melchert, A. Kinetic and temporospatial gait parameters in a heterogeneous group of dogs. BMC Vet. Res. 2016, 12, 2. [Google Scholar] [CrossRef] [PubMed]
- National Research Council Committee for the Update of the Guide for the Care and Use of Laboratory Animals. The National Academies Collection: Reports Funded by National Institutes of Health. In Guide for the Care and Use of Laboratory Animals; National Academies Press (US): Washington, DC, USA; National Academy of Sciences: Washington, DC, USA, 2011. [Google Scholar]
- Johnson, N.A.; Fairhurst, C.; Brealey, S.D.; Cook, E.; Stirling, E.; Costa, M.; Divall, P.; Hodgson, S.; Rangan, A.; Dias, J.J. One-year outcome of surgery compared with immobilization in a cast for adults with an undisplaced or minimally displaced scaphoid fracture: A meta-analysis of randomized controlled trials. Bone Jt. J. 2022, 104, 953–962. [Google Scholar] [CrossRef] [PubMed]
- Schilling, B.K.; Falvo, M.J.; Chiu, L.Z.F. Force-velocity, impulse-momentum relationships: Implications for efficacy of purposefully slow resistance training. J. Sports Sci. Med. 2008, 7, 299–304. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Timepoint | N | Stance Time (s) | Swing Time (s) | Stride Time (s) | Stride Length (cm) | Stride Velocity (cm/s) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Forelimb | LF | RF | LF | RF | LF | RF | LF | RF | LF | RF | |
| Preop | 13 | 0.46 ± 0.13 | 0.47 ± 0.14 | 0.44 ± 0.19 | 0.39 ± 0.08 | 0.85 ± 0.29 | 0.84 ± 0.21 | 92.62 ± 7.65 | 91.54 ± 13.30 | 114.55 ± 27.55 | 117.91 ± 34.47 |
| Day 1 | 12 | 0.55 ± 0.16 | 0.53 ± 0.21 | 0.35 ± 0.07 | 0.37 ± 0.08 | 0.84 ± 0.22 | 0.88 ± 0.30 | 74.17 ± 15.15 a | 70.97 ± 19.23 a | 96.96 ± 38.51 | 94.30 ± 34.29 |
| Day 7 | 12 | 0.53 ± 0.30 | 0.50 ± 0.27 | 0.40 ± 0.14 | 0.41 ± 0.13 | 0.87 ± 0.26 | 0.88 ± 0.30 | 86.21 ± 12.26 | 76.59 ± 13.42 | 109.17 ± 39.45 | 98.14 ± 38.33 |
| Day 30 | 10 | 0.49 ± 0.39 | 0.48 ± 0.36 | 0.34 ± 0.09 | 0.35 ± 0.08 | 0.84 ± 0.57 | 0.81 ± 0.45 | 86.79 ± 13.17 | 84.02 ± 13.29 | 136.28 ± 55.33 | 129.42 ± 56.47 |
| Day 180 | 13 | 0.59 ± 0.19 | 0.49 ± 0.11 | 0.39 ± 0.12 | 0.44 ± 0.23 | 0.95 ± 0.23 | 0.85 ± 0.24 | 67.79 ± 16.85 a,b,c | 69.28 ± 10.57 a | 74.98 ± 21.87 c | 89.92 ± 25.17 |
| Day 240 | 13 | 0.55 ± 0.12 | 0.59 ± 0.23 | 0.37 ± 0.08 | 0.43 ± 0.15 | 0.85 ± 0.17 | 0.90 ± 0.32 | 64.86 ± 13.85 a,b,c | 63.21 ± 14.79 a,c | 83.50 ± 25.52 c | 80.81 ± 33.17 c |
| Day 300 | 13 | 0.53 ± 0.09 | 0.50 ± 0.11 | 0.37 ± 0.06 | 0.41 ± 0.09 | 0.86 ± 0.20 | 0.88 ± 0.18 | 71.23 ± 12.28 a | 68.68 ± 8.18 a,c | 87.51 ± 19.74 c | 83.68 ± 15.96 c |
| Day 360 | 13 | 0.54 ± 0.19 | 0.51 ± 0.18 | 0.42 ± 0.19 | 0.45 ± 0.16 | 0.96 ± 0.48 | 0.93 ± 0.36 | 66.95 ± 12.75 a,b,c | 65.68 ± 10.66 a,c | 84.74 ± 35.48 c | 81.72 ± 29.46 c |
| Timepoint | N | Stance Time (s) | Swing Time (s) | Stride Time (s) | Stride Length (cm) | Stride Velocity (cm/s) | |||||
| Hindlimb | LF | RF | LF | RF | LF | RF | LF | RF | LF | RF | |
| Preop | 13 | 0.43 ± 0.15 | 0.45 ± 0.13 | 0.48 ± 0.18 | 0.44 ± 0.10 | 0.87 ± 0.21 | 0.85 ± 0.18 | 84.90 ± 20.54 | 84.72 ± 7.52 | 103.31 ± 28.14 | 104.98 ± 23.52 |
| Day 1 | 12 | 0.55 ± 0.16 | 0.34 ± 0.14 | 0.46 ± 0.21 | 0.58 ± 0.23 | 0.88 ± 0.30 | 0.95 ± 0.31 | 70.71 ± 19.23 | 70.60 ± 22.58 | 87.38 ± 45.34 | 84.39 ± 40.59 |
| Day 7 | 12 | 0.52 ± 0.23 | 0.45 ± 0.25 | 0.41 ± 0.08 | 0.52 ± 0.16 | 0.88 ± 0.30 | 1.10 ± 0.75 | 76.59 ± 13.42 | 74.73 ± 15.52 | 90.89 ± 42.54 | 90.34 ± 42.41 |
| Day 30 | 10 | 0.47 ± 0.24 | 0.41 ± 0.26 | 0.40 ± 0.12 | 0.54 ± 0.20 | 0.81 ± 0.45 | 0.98 ± 0.44 | 84.02 ± 13.29 | 74.56 ± 13.72 | 121.86 ± 42.49 | 90.29 ± 41.60 |
| Day 180 | 13 | 0.72 ± 0.33 a | 0.36 ± 0.10 | 0.34 ± 0.06 | 0.62 ± 0.31 | 0.93 ± 0.15 | 1.01 ± 0.37 | 69.28 ± 10.57 a,c | 62.01 ± 16.78 a | 71.35 ± 18.23 c | 68.50 ± 25.79 |
| Day 240 | 13 | 0.70 ± 0.18 a | 0.45 ± 0.10 | 0.34 ± 0.08 | 0.69 ± 0.13 | 1.00 ± 0.19 | 1.09 ± 0.28 | 63.21 ± 14.79 a,c | 56.65 ± 13.07 a | 60.38 ± 15.86 a | 54.71 ± 17.73 a |
| Day 300 | 13 | 0.61 ± 0.11 | 0.37 ± 0.09 | 0.34 ± 0.07 | 0.59 ± 0.16 | 0.87 ± 0.14 | 0.99 ± 0.21 | 68.68 ± 8.18 | 64.36 ± 9.74 a | 81.43 ± 14.82 c | 72.13 ± 35.74 |
| Day 360 | 13 | 0.64 ± 0.15 | 0.39 ± 0.07 | 0.34 ± 0.10 | 0.62 ± 0.21 | 0.90 ± 0.20 | 0.97 ± 0.28 | 65.68 ± 10.66 a,c | 58.97 ± 13.52 a | 79.14 ± 33.73 c | 69.10 ± 27.80 |
| Timepoint | N | Maximum Vertical Force (%BW) | Impulse (%BW*s) | Maximum Peak Pressure (kPa) | |||
|---|---|---|---|---|---|---|---|
| Forelimb | LF | RF | LF | RF | LF | RF | |
| Preop | 13 | 49.49 ± 9.43 | 52.48 ± 11.50 | 15.42 ± 6.41 | 15.88 ± 6.16 | 212.62 ± 61.57 | 236.15 ± 54.94 |
| Day 1 | 12 | 45.49 ± 7.76 | 49.48 ± 10.57 | 17.49 ± 5.04 | 20.89 ± 7.88 | 198.25 ± 57.63 | 197.38 ± 53.92 |
| Day 7 | 12 | 46.93 ± 13.76 | 47.18 ± 13.83 | 15.11 ± 11.37 | 13.50 ± 5.84 | 216.44 ± 59.55 | 194.00 ± 56.39 |
| Day 30 | 10 | 48.86 ± 9.66 | 47.60 ± 8.63 | 14.84 ± 8.77 | 14.89 ± 11.29 | 234.70 ± 54.93 | 210.70 ± 36.74 |
| Day 180 | 13 | 56.02 ± 10.45 | 47.54 ± 11.23 | 20.58 ± 5.55 | 15.42 ± 5.39 | 209.54 ± 43.87 | 172.38 ± 52.81 |
| Day 240 | 13 | 49.23 ± 6.23 | 50.93 ± 10.20 | 18.42 ± 5.63 | 19.95 ± 9.55 | 206.31 ± 54.82 | 191.00 ± 55.90 |
| Day 300 | 13 | 51.89 ± 5.43 | 48.62 ± 11.07 | 18.87 ± 4.52 | 15.40 ± 3.52 | 213.17 ± 48.92 | 205.50 ± 47.35 |
| Day 360 | 13 | 49.73 ± 14.06 | 48.37 ± 8.95 | 18.42 ± 8.18 | 15.11 ± 4.70 | 193.85 ± 44.05 | 218.08 ± 39.67 |
| Timepoint | N | Maximum Vertical Force (%BW) | Impulse (%BW*s) | Maximum Peak Pressure (kPa) | |||
| Hindlimb | LH | RH | LH | RH | LH | RH | |
| Preop | 13 | 34.02 ± 7.55 | 35.79 ± 6.52 | 9.78 ± 3.59 | 10.34 ± 3.24 | 159.08 ± 31.90 | 172.23 ± 48.61 |
| Day 1 | 12 | 29.96 ± 4.71 | 25.99 ± 5.93 | 11.50 ± 3.59 | 7.11 ± 3.04 | 164.00 ± 33.65 | 150.25 ± 43.85 |
| Day 7 | 12 | 34.31 ± 7.95 | 22.78 ± 8.27 | 10.89 ± 4.40 | 7.09 ± 5.04 | 159.67 ± 31.08 | 131.22 ± 32.35 |
| Day 30 | 10 | 36.54 ± 7.75 | 23.03 ± 7.59 | 10.81 ± 4.20 | 6.34 ± 2.88 a | 173.40 ± 46.25 | 107.78 ± 26.60 a |
| Day 180 | 13 | 33.48 ± 6.39 | 19.37 ± 5.37 a | 16.07 ± 8.54 | 5.41 ± 2.08 a | 156.46 ± 42.97 | 95.46 ± 31.85 a,b |
| Day 240 | 13 | 37.44 ± 6.39 | 25.02 ± 4.33 a | 17.35 ± 6.54 a | 8.37 ± 2.77 | 161.77 ± 25.41 | 115.77 ± 29.30 a |
| Day 300 | 13 | 36.63 ± 9.30 | 20.17 ± 4.44 a | 14.28 ± 4.82 | 5.80 ± 2.11 a | 158.50 ± 40.68 | 118.17 ± 34.24 a |
| Day 360 | 13 | 34.38 ± 9.69 | 21.41 ± 4.86 a | 14.18 ± 5.64 | 5.86 ± 1.64 a | 155.08 ± 36.52 | 108.08 ± 25.37 a |
| Forelimb Asymmetry Indices | |||||||
|---|---|---|---|---|---|---|---|
| Timepoint | N | Stance Time | Stride Length | Stride Velocity | Max Force | Impulse | MPP |
| Preop | 13 | 2.39 ± 0.52 | 2.44 ± 0.85 | 3.65 ± 1.11 | 6.10 ± 1.40 | 5.90 ± 1.68 | 7.78 ± 1.32 |
| Day 1 | 12 | 3.76 ± 1.06 | 2.84 ± 0.88 | 3.21 ± 1.23 | 6.59 ± 1.47 | 6.90 ± 1.78 | 8.60 ± 2.41 |
| Day 7 | 12 | 2.50 ± 0.96 | 3.87 ± 1.14 | 4.46 ± 1.11 | 5.10 ± 1.19 | 6.50 ± 1.65 | 6.65 ± 2.19 |
| Day 30 | 10 | 3.53 ± 0.84 | 1.57 ± 0.68 | 3.98 ± 1.95 | 6.06 ± 1.33 | 7.10 ± 2.19 | 6.87 ± 1.00 |
| Day 180 | 13 | 5.47 ± 0.90 | 3.13 ± 0.69 | 5.13 ± 1.44 | 6.29 ± 1.12 | 8.95 ± 1.87 | 8.36 ± 1.54 |
| Day 240 | 13 | 3.39 ± 0.64 | 1.89 ± 0.61 | 5.04 ± 1.63 | 5.20 ± 1.06 | 7.39 ± 1.04 | 5.31 ± 1.22 |
| Day 300 | 13 | 2.52 ± 0.46 | 2.64 ± 0.59 | 4.50 ± 1.08 | 3.96 ± 1.29 | 6.65 ± 1.35 | 5.87 ± 0.77 |
| Day 360 | 13 | 3.07 ± 0.88 | 1.81 ± 0.40 | 3.03 ± 0.71 | 5.67 ± 1.37 | 7.90 ± 1.41 | 4.77 ± 1.00 |
| Hindlimb Asymmetry Indices | |||||||
| Timepoint | N | Stance Time | Stride Length | Stride Velocity | Max Force | Impulse | MPP |
| Preop | 13 | 2.97 ± 0.67 | 3.41 ± 0.89 | 4.83 ± 1.09 | 4.30 ± 0.81 | 5.53 ± 1.06 | 5.24 ± 1.22 |
| Day 1 | 12 | 12.35 ± 2.41 * | 4.72 ± 1.82 | 5.67 ± 2.02 | 8.37 ± 1.28 | 14.72 ± 2.79 | 8.16 ± 1.27 |
| Day 7 | 12 | 5.91 ± 1.33 | 4.38 ± 1.30 | 7.85 ± 1.80 | 10.40 ± 3.20 | 13.16 ± 3.19 | 7.06 ± 2.33 |
| Day 30 | 10 | 8.61 ± 3.34 | 3.44 ± 0.93 | 5.98 ± 2.26 | 11.38 ± 3.55 | 14.86 ± 4.36 | 12.31 ± 3.00 |
| Day 180 | 13 | 15.77 ± 1.71 * | 3.15 ± 1.25 | 5.25 ± 1.48 | 13.74 ± 2.19 * | 24.23 ± 2.10 * | 12.83 ± 2.57 |
| Day 240 | 13 | 10.61 ± 1.20 * | 2.83 ± 0.70 | 3.97 ± 1.19 | 9.84 ± 1.77 | 17.41 ± 2.19 * | 8.51 ± 1.53 |
| Day 300 | 13 | 12.26 ± 1.64 * | 2.68 ± 0.58 | 6.71 ± 1.16 | 14.17 ± 2.13 * | 20.80 ± 2.60 * | 9.71 ± 1.66 |
| Day 360 | 13 | 11.66 ± 1.38 * | 3.80 ± 0.97 | 7.20 ± 1.77 | 10.91 ± 1.98 | 19.35 ± 2.21 * | 9.35 ± 1.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bowers, K.M.; Terrones, L.D.; Croy, E.G.; Mulon, P.-Y.; Adair, H.S., III; Anderson, D.E. Assessment of Gait Following Locking Plate Fixation of a Tibial Segmental Defect and Cast Immobilization in Goats. Biomechanics 2022, 2, 575-590. https://doi.org/10.3390/biomechanics2040045
Bowers KM, Terrones LD, Croy EG, Mulon P-Y, Adair HS III, Anderson DE. Assessment of Gait Following Locking Plate Fixation of a Tibial Segmental Defect and Cast Immobilization in Goats. Biomechanics. 2022; 2(4):575-590. https://doi.org/10.3390/biomechanics2040045
Chicago/Turabian StyleBowers, Kristin M., Lori D. Terrones, Elizabeth G. Croy, Pierre-Yves Mulon, Henry S. Adair, III, and David E. Anderson. 2022. "Assessment of Gait Following Locking Plate Fixation of a Tibial Segmental Defect and Cast Immobilization in Goats" Biomechanics 2, no. 4: 575-590. https://doi.org/10.3390/biomechanics2040045
APA StyleBowers, K. M., Terrones, L. D., Croy, E. G., Mulon, P.-Y., Adair, H. S., III, & Anderson, D. E. (2022). Assessment of Gait Following Locking Plate Fixation of a Tibial Segmental Defect and Cast Immobilization in Goats. Biomechanics, 2(4), 575-590. https://doi.org/10.3390/biomechanics2040045