
Gendered Analysis of Cyberbullying Victimization and Its Associations with Suicidality: Findings from the 2019 Youth Risk Behavior Survey



Abstract
:1. Introduction
1.1. Cyberbullying, Suicidality, and Depression
1.2. Gendered Risks for Suicidality: Sexual Violence and Sexual Orientation
1.3. Theoretical Foundations
1.4. Study Objectives
1.5. Study Hypotheses
2. Materials and Methods
2.1. Setting and Procedure
2.2. Measures
2.3. Data Analysis
3. Results
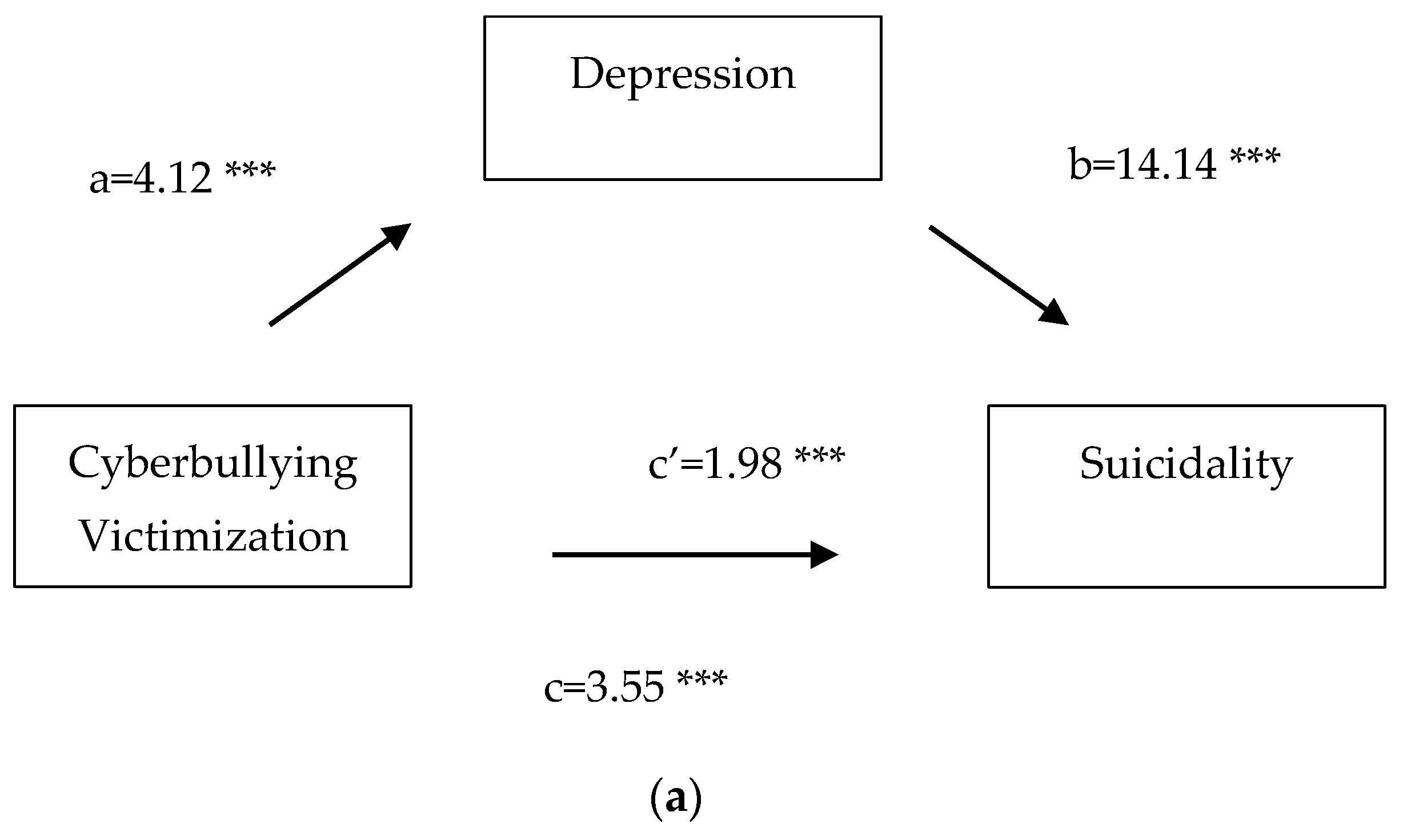
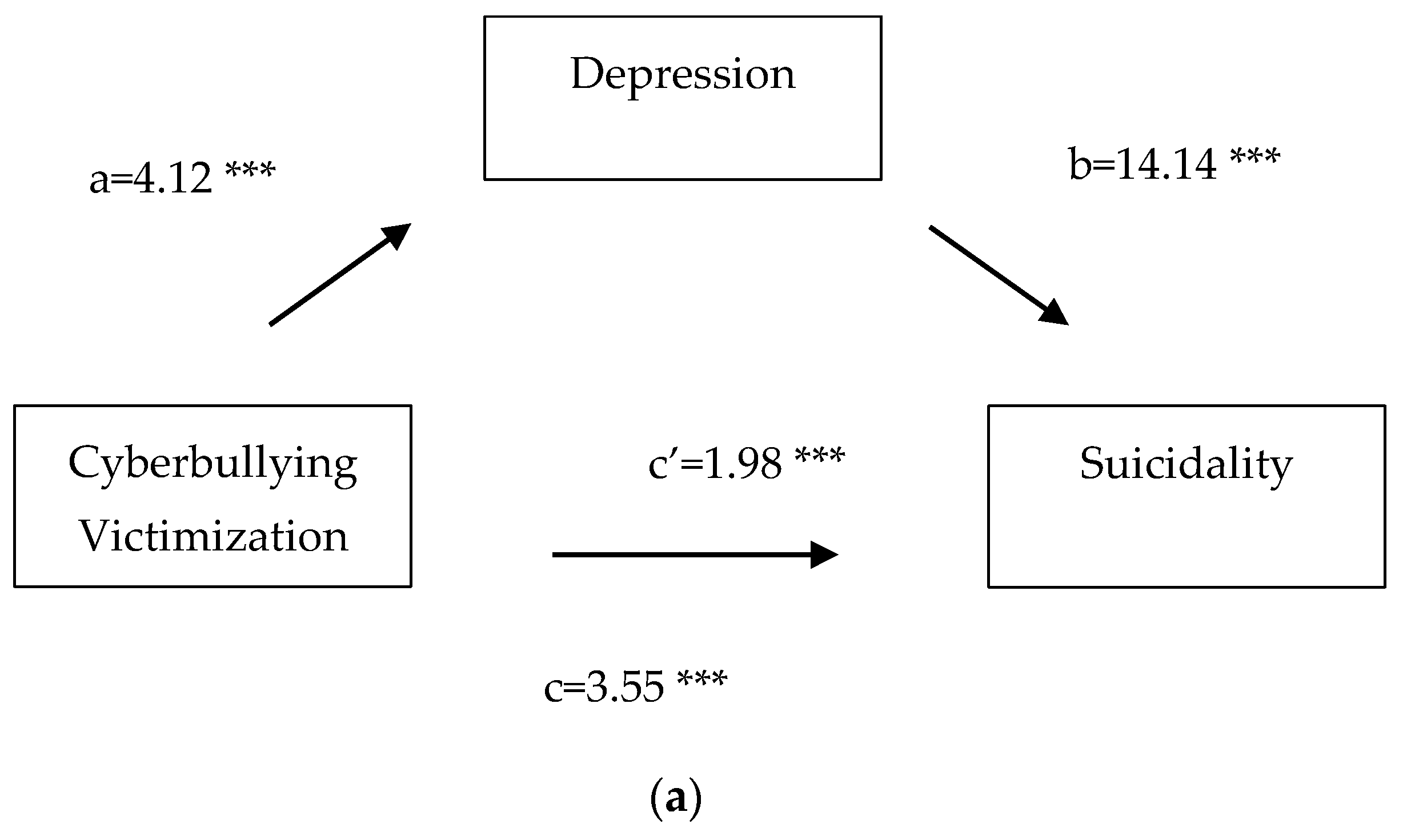
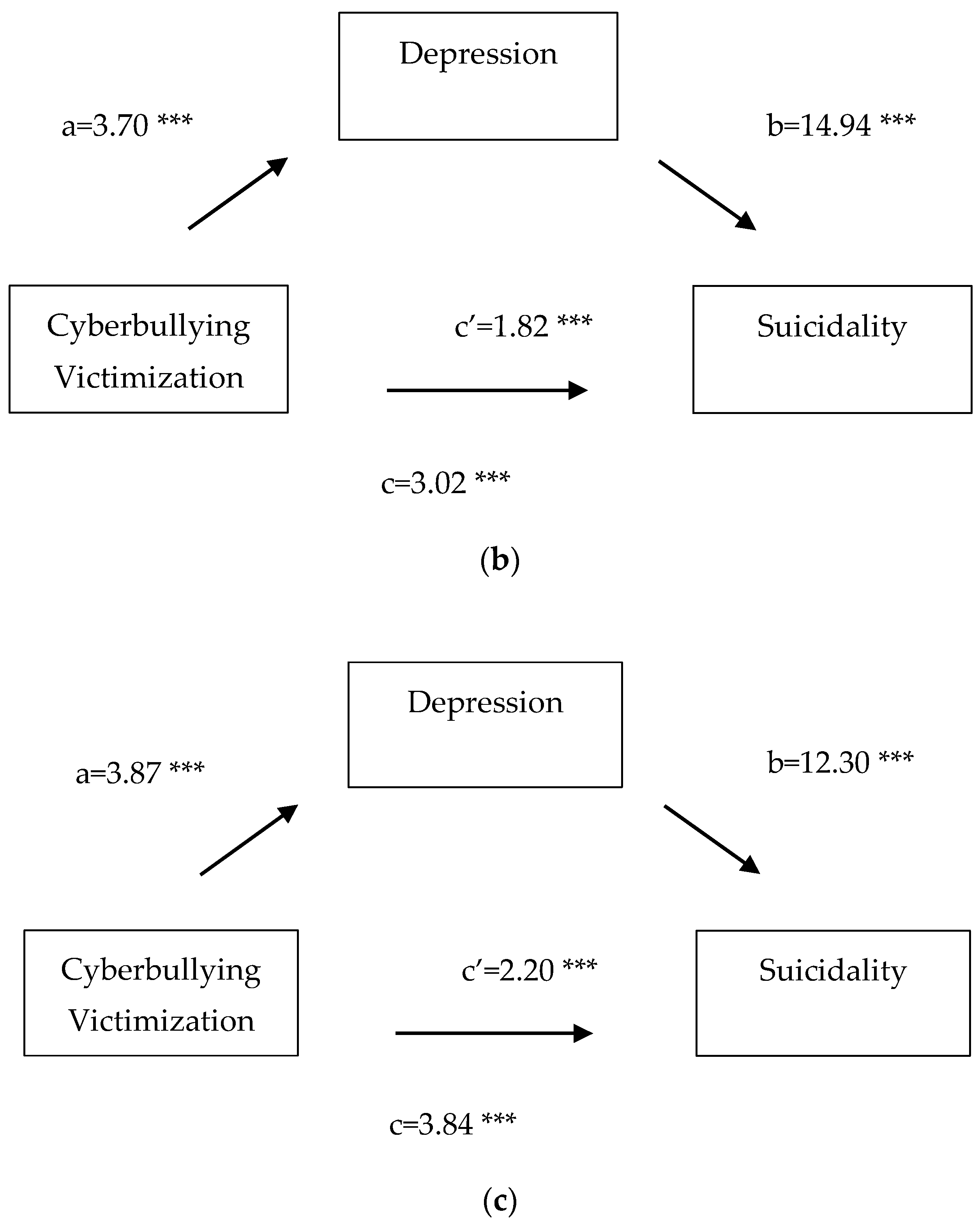
3.1. Mediation Analyses
3.2. Logistic Multiple Regression
3.3. CV and Sexual Violence Interaction Effects
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nixon, C.L. Current perspectives: The impact of cyberbullying on adolescent health. Adolesc. Health Med. Ther. 2014, 5, 143. [Google Scholar] [CrossRef] [Green Version]
- Center on Gender Equity and Health. Californians Experiences of Violence during Pandemic. 2021. Available online: https://geh.ucsd.edu/cal-vex/ (accessed on 19 April 2022).
- Copp, J.E.; Mumford, E.A.; Taylor, B.G. Online sexual harassment and cyberbullying in a nationally representative sample of teens: Prevalence, predictors, and consequences. J. Adolesc. 2021, 93, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Gunnell, D.; Kidger, J.; Elvidge, H. Adolescent mental health in crisis. BMJ 2018, 361, k2608. [Google Scholar] [CrossRef] [Green Version]
- Logrieco, G.; Marchili, M.R.; Roversi, M.; Villani, A. The paradox of Tik Tok anti-pro-anorexia videos: How social media can promote non-suicidal self-injury and anorexia. Int. J. Environ. Res. Public Health 2021, 18, 1041. [Google Scholar] [CrossRef]
- Pew Research Center. Teens, Social Media & Technology. Available online: https://www.pewresearch.org/internet/2018/05/31/teens-social-media-technology-2018/ (accessed on 19 April 2022).
- Basile, K.C.; Clayton, H.B.; DeGue, S.; Gilford, J.W.; Vagi, K.J.; Suarez, N.A.; Zwald, M.L.; Lowry, R. Interpersonal violence victimization among high school students—Youth Risk Behavior Survey, United States, 2019. MMWR Suppl. 2020, 69, 28. [Google Scholar] [CrossRef] [PubMed]
- Katzer, C.; Fetchenhauer, D.; Belschak, F. Cyberbullying: Who are the victims? A comparison of victimization in Internet chatrooms and victimization in school. J. Media Psychol. 2009, 21, 25–36. [Google Scholar] [CrossRef]
- Kiriakidis, S.P.; Kavoura, A. Cyberbullying: A review of the literature on harassment through the internet and other electronic means. Fam. Community Health 2010, 33, 82–93. [Google Scholar] [CrossRef]
- Espelage, D.L.; Hong, J.S.; Valido, A. Cyberbullying in the United States. In International Perspectives on Cyberbullying; Costanza Baldry, A., Blaya, C., Farrington, D.P., Eds.; Palgrave Macmillan: New York, NY, USA, 2018; pp. 65–99. [Google Scholar]
- Brody, N.; Vangelisti, A.L. Cyberbullying: Topics, strategies, and sex differences. Comput. Hum. Behav. 2017, 75, 739–748. [Google Scholar] [CrossRef]
- Alhajji, M.; Bass, S.; Dai, T. Cyberbullying, mental health, and violence in adolescents and associations with sex and race: Data from the 2015 Youth Risk Behavior Survey. Glob. Pediatr. Health 2019, 6, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Baiden, P.; Tadeo, S.K. Investigating the association between bullying victimization and suicidal ideation among adolescents: Evidence from the 2017 Youth Risk Behavior Survey. Child Abus. Negl. 2020, 102, 104417. [Google Scholar] [CrossRef] [PubMed]
- Holt, M.K.; Vivolo-Kantor, A.M.; Polanin, J.R.; Holland, K.M.; DeGue, S.; Matjasko, J.L.; Wolfe, M.; Reid, G. Bullying and suicidal ideation and behaviors: A meta-analysis. Pediatrics 2015, 135, e496–e509. [Google Scholar] [CrossRef] [Green Version]
- Hinduja, S.; Patchin, J. Bullying, cyberbullying, and suicide. Arch. Suicide Res. 2010, 14, 206–221. [Google Scholar] [CrossRef]
- Bannink, R.; Broeren, S.; van de Looij–Jansen, P.M.; de Waart, F.G.; Raat, H. Cyber and traditional bullying victimization as a risk factor for mental health problems and suicidal ideation in adolescents. PLoS ONE 2014, 9, e94026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Geel, M.; Vedder, P.; Tanilon, J. Relationship between peer victimization, cyberbullying, and suicide in children and adolescents: A meta-analysis. JAMA Pediatr. 2014, 168, 435–442. [Google Scholar] [CrossRef] [Green Version]
- Quintana-Orts, C.; Rey, L.; Neto, F. Beyond cyberbullying: Investigating when and how cybervictimization predicts suicidal ideation. J. Interpers. Violence 2022, 37, 935–957. [Google Scholar] [CrossRef] [PubMed]
- Sampasa-Kanyinga, H. Co-occurring cyberbullying and school bullying victimization and associations with mental health problems among Canadian middle and high school students. Violence Vict. 2017, 32, 671–687. [Google Scholar] [CrossRef]
- Lucas-Molina, B.; Pérez-Albéniz, A.; Fonseca-Pedrero, E. The potential role of subjective wellbeing and gender in the relationship between bullying or cyberbullying and suicidal ideation. Psychiatry Res. 2018, 270, 595–601. [Google Scholar] [CrossRef]
- Lamis, D.A.; Malone, P.S.; Langhinrichsen-Rohling, J.; Ellis, T.E. Body investment, depression, and alcohol use as risk factors for suicide proneness in college students. Crisis 2010, 31, 118–127. [Google Scholar] [CrossRef] [Green Version]
- Galaif, E.R.; Sussman, S.; Newcomb, M.D.; Locke, T.F. Suicidality, depression, and alcohol use among adolescents: A review of empirical findings. Int. J. Adolesc. Med. Health 2007, 19, 27–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kandel, D.B.; Raveis, V.H.; Davies, M. Suicidal ideation in adolescence: Depression, substance use, and other risk factors. J. Youth Adolesc. 1991, 20, 289–309. [Google Scholar] [CrossRef]
- Bilsen, J. Suicide and youth: Risk factors. Front. Psychiatry 2018, 9, 540. [Google Scholar] [CrossRef]
- Snakenborg, J.; Van Acker, R.; Gable, R.A. Cyberbullying: Prevention and intervention to protect our children and youth. Prev. Sch. Fail. Altern. Educ. Child. Youth 2011, 55, 88–95. [Google Scholar] [CrossRef]
- CDC. Suicide Rising across the US. Available online: https://www.cdc.gov/vitalsigns/suicide/index.html (accessed on 19 April 2022).
- Twenge, J.M.; Joiner, T.E.; Rogers, M.L.; Martin, G.N. Increases in depressive symptoms, suicide-related outcomes, and suicide rates among U.S. adolescents after 2010 and links to increased new media screen time. Clin. Psychol. Sci. 2017, 6, 3–17. [Google Scholar] [CrossRef] [Green Version]
- Miron, O.; Yu, K.-H.; Wilf-Miron, R.; Kohane, I.S. Suicide rates among adolescents and young adults in the United States, 2000–2017. JAMA 2019, 321, 2362–2364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barlett, C.P.; Simmers, M.M.; Roth, B.; Gentile, D. Comparing cyberbullying prevalence and process before and during the COVID-19 pandemic. J. Soc. Psychol. 2021, 161, 408–418. [Google Scholar] [CrossRef]
- Wold, S. COVID-19 Is Changing How, Why and How Much We’re Using Social Media. Available online: https://www.digitalcommerce360.com/2020/09/16/covid-19-is-changing-how-why-and-how-much-were-using-social-media/ (accessed on 19 April 2022).
- Johnson, J. Coronavirus: Impact on Online Usage in the U.S.—Statistics & Facts. Available online: https://www.statista.com/topics/6241/coronavirus-impact-on-online-usage-in-the-us/ (accessed on 19 April 2022).
- Gámez-Guadix, M.; Orue, I.; Smith, P.K.; Calvete, E. Longitudinal and reciprocal relations of cyberbullying with depression, substance use, and problematic internet use among adolescents. J. Adolesc. Health 2013, 53, 446–452. [Google Scholar] [CrossRef]
- Bottino, S.M.B.; Bottino, C.M.C.; Regina, C.G.; Correia, A.V.L.; Ribeiro, W.S. Cyberbullying and adolescent mental health: Systematic review. Cad. Saude Publica 2015, 31, 463–475. [Google Scholar] [CrossRef] [Green Version]
- Hamm, M.P.; Newton, A.S.; Chisholm, A.; Shulhan, J.; Milne, A.; Sundar, P.; Ennis, H.; Scott, S.D.; Hartling, L. Prevalence and effect of cyberbullying on children and young people: A scoping review of social media studies. JAMA Pediatr. 2015, 169, 770–777. [Google Scholar] [CrossRef]
- Fahy, A.E.; Stansfeld, S.A.; Smuk, M.; Smith, N.R.; Cummins, S.; Clark, C. Longitudinal associations between cyberbullying involvement and adolescent mental health. J. Adolesc. Health 2016, 59, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Carballo, J.J.; Llorente, C.; Kehrmann, L.; Flamarique, I.; Zuddas, A.; Purper-Ouakil, D.; Hoekstra, P.J.; Coghill, D.; Schulze, U.M.E.; Dittmann, R.W.; et al. Psychosocial risk factors for suicidality in children and adolescents. Eur. Child Adolesc. Psychiatry 2020, 29, 759–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CDC. Youth Risk Behavior Survey Data Summary & Trends Report: 2009–2019. Available online: https://www.cdc.gov/healthyyouth/data/yrbs/pdf/YRBSDataSummaryTrendsReport2019-508.pdf (accessed on 19 April 2022).
- Bauman, S.; Toomey, R.B.; Walker, J.L. Associations among bullying, cyberbullying, and suicide in high school students. J. Adolesc. 2013, 36, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Reed, K.P.; Nugent, W.; Cooper, R.L. Testing a path model of relationships between gender, age, and bullying victimization and violent behavior, substance abuse, depression, suicidal ideation, and suicide attempts in adolescents. Child. Youth Serv. Rev. 2015, 55, 128–137. [Google Scholar] [CrossRef]
- Litwiller, B.; Brausch, A. Cyber bullying and physical bullying in adolescent suicide: The role of violent behavior and substance use. J. Youth Adolesc. 2013, 42, 675–684. [Google Scholar] [CrossRef]
- Allison, S.; Roeger, L.; Martin, G.; Keeves, J. Gender differences in the relationship between depression and suicidal ideation in young adolescents. Aust. N. Z. J. Psychiatry 2001, 35, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Aboujaoude, E.; Savage, M.W.; Starcevic, V.; Salame, W.O. Cyberbullying: Review of an old problem gone viral. J. Adolesc. Health 2015, 57, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Dodge, A. Digitizing rape culture: Online sexual violence and the power of the digital photograph. Crime Media Cult. 2016, 12, 65–82. [Google Scholar] [CrossRef]
- Ehman, A.C.; Gross, A.M. Sexual cyberbullying: Review, critique, & future directions. Aggress. Violent Behav. 2019, 44, 80–87. [Google Scholar] [CrossRef]
- Henry, N.; Flynn, A.; Powell, A. Technology-facilitated domestic and sexual violence: A review. Violence Against Women 2020, 26, 1828–1854. [Google Scholar] [CrossRef]
- Baiden, P.; Xiao, Y.; Asiedua-Baiden, G.; LaBrenz, C.A.; Boateng, G.O.; Graaf, G.; Muehlenkamp, J.J. Sex differences in the association between sexual violence victimization and suicidal behaviors among adolescents. J. Affect. Disord. Rep. 2020, 1, 100011. [Google Scholar] [CrossRef]
- Tucker, J.S.; Ewing, B.A.; Espelage, D.L.; Green, H.D.; De La Haye, K.; Pollard, M.S. Longitudinal associations of homophobic name-calling victimization with psychological distress and alcohol use during adolescence. J. Adolesc. Health 2016, 59, 110–115. [Google Scholar] [CrossRef] [Green Version]
- Kimmel, M.S.; Mahler, M. Adolescent masculinity, homophobia, and violence. Am. Behav. Sci. 2003, 46, 1439–1458. [Google Scholar] [CrossRef]
- D’augelli, A.R.; Pilkington, N.W.; Hershberger, S.L. Incidence and mental health impact of sexual orientation victimization of lesbian, gay, and bisexual youths in high school. Sch. Psychol. Q. 2002, 17, 148–167. [Google Scholar] [CrossRef]
- Wang, C.C.; Lin, H.C.; Chen, M.H.; Ko, N.Y.; Chang, Y.P.; Lin, I.M.; Yen, C.F. Effects of traditional and cyber homophobic bullying in childhood on depression, anxiety, and physical pain in emerging adulthood and the moderating effects of social support among gay and bisexual men in Taiwan. Neuropsychiatr. Dis. Treat. 2018, 14, 1309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espelage, D.L.; Valido, A.; Hatchel, T.; Ingram, K.M.; Huang, Y.; Torgal, C. A literature review of protective factors associated with homophobic bullying and its consequences among children & adolescents. Aggress. Violent Behav. 2019, 45, 98–110. [Google Scholar] [CrossRef]
- Chu, C.; Buchman-Schmitt, J.M.; Stanley, I.H.; Hom, M.A.; Tucker, R.P.; Hagan, C.R.; Rogers, M.L.; Podlogar, M.C.; Chiurliza, B.; Ringer-Moberg, F.B.; et al. The interpersonal theory of suicide: A systematic review and meta-analysis of a decade of cross-national research. Psychol. Bull. 2017, 143, 1313. [Google Scholar] [CrossRef]
- Joiner, T. Why People Die by Suicide; Harvard University Press: Cambridge, MA, USA, 2005. [Google Scholar]
- Joiner, T.E.; Van Orden, K.A.; Witte, T.K.; Rudd, M.D. The Interpersonal Theory of Suicide: Guidance for Working with Suicidal Clients; American Psychological Association: Washington, DC, USA, 2009. [Google Scholar] [CrossRef]
- Azami, M.S.; Taremian, F. Victimization in traditional and cyberbullying as risk factors for substance use, self-harm and suicide attempts in high school students. Scand. J. Child Adolesc. Psychiatry Psychol. 2020, 8, 101. [Google Scholar] [CrossRef] [PubMed]
- Eidi, A.; Delam, H. Internet addiction is likely to increase in home quarantine caused by coronavirus disease 2019 (COVID 19). J. Health Sci. Surveill. Syst. 2020, 8, 142–143. [Google Scholar] [CrossRef]
- Racine, N.; Cooke, J.E.; Eirich, R.; Korczak, D.J.; McArthur, B.; Madigan, S. Child and adolescent mental illness during COVID-19: A rapid review. Psychiatry Res. 2020, 292, 113307. [Google Scholar] [CrossRef] [PubMed]
- Redfield, R.R.; Bunnell, R.; Greenspan, A.; Kent, C.K.; Leahy, M.A.; Martinroe, J.C.; Spriggs, S.R.; Yang, T.; Doan, Q.M.; King, P.H.; et al. Overview and Methods for the Youth Risk Behavior Surveillance System—United States, 2019. MMWR 2020, 69, 1. [Google Scholar]
- Centers for Disease Control and Prevention. Methodology of the Youth Risk Behavior Surveillance System—2013. MMWR 2013, 62, 1–20. [Google Scholar]
- Brener, N.D.; Billy, J.O.G.; Grady, W.R. Assessment of factors affecting the validity of self-reported health-risk behavior among adolescents: Evidence from the scientific literature. J. Adolesc. Health 2003, 33, 436–457. [Google Scholar] [CrossRef] [Green Version]
- Baron, R.; Kenny, D. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Lian, Q.; Su, Q.; Li, L.; Xie, M.; Hu, J. Trends and sex disparities in school bullying victimization among U.S. youth, 2011–2019. BMC Public Health 2020, 20, 1583. [Google Scholar] [CrossRef] [PubMed]
- Pontes, N.M.H.; Ayres, C.G.; Pontes, M.C.F. Trends in depressive symptoms and suicidality: Youth Risk Behavior Survey 2009–2017. Nurs. Res. 2020, 69, 176–185. [Google Scholar] [CrossRef]
- Kim, S.; Kimber, M.; Boyle, M.H.; Georgiades, K. Sex differences in the association between cyberbullying victimization and mental health, substance use, and suicidal ideation in adolescents. Can. J. Psychiatry 2019, 64, 126. [Google Scholar] [CrossRef] [PubMed]
- Tomasula, J.L.; Anderson, L.M.; Littleton, H.L.; Riley-Tillman, T.C. The association between sexual assault and suicidal activity in a national sample. Sch. Psychol. Q. 2012, 27, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Dir, A.L.; Bell, R.L.; Adams, Z.W.; Hulvershorn, L.A. Gender differences in risk factors for adolescent binge drinking and implications for intervention and prevention. Front. Psychiatry 2017, 8, 289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patten, M.; Carmichael, H.; Moore, A.; Velopulos, C. Circumstances of Suicide Among Lesbian, Gay, Bisexual and Transgender Individuals. J. Surg. Res. 2022, 270, 522–529. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Kleinman, A.; Good, B. Culture and Depression: Studies in the Anthropology and Cross-Cultural Psychiatry of Affect and Disorder; University of California Press: Berkeley, CA, USA, 1986. [Google Scholar]
- Kowalski, R.M.; Giumetti, G.W.; Schroeder, A.N.; Lattanner, M.R. Bullying in the digital age: A critical review and meta-analysis of cyberbullying research among youth. Psychol. Bull. 2014, 140, 1073–1137. [Google Scholar] [CrossRef]
- Extremera, N.; Quintana-Orts, C.; Mérida-López, S.; Rey, L. Cyberbullying victimization, self-esteem and suicidal ideation in adolescence: Does emotional intelligence play a buffering role? Front. Psychol. 2018, 9, 367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aldridge, J.M.; McChesney, K. The relationships between school climate and adolescent mental health and wellbeing: A systematic literature review. Int. J. Int. J. Educ. Res. 2018, 88, 121–145. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Unwt No. (Wt %) Total Sample (n = 10,309) | Unwt No. (Wt %) Female Subsample (n = 5333) | Unwt No. (Wt %) Male Subsample (n = 4976) | Chi-Square (df) p-Value | |
|---|---|---|---|---|
| Age | ||||
| 12 years or younger | 19 (0.1) | |||
| 13 years old | 9 (0.01) | |||
| 14 years old | 1176 (11.7) | |||
| 15 years old | 2613 (24.9) | |||
| 16 years old | 2769 (25.7) | |||
| 17 years old | 2426 (23.9) | |||
| 18 years or older | 1289 (13.6) | |||
| Gender | ||||
| Girls | 5333 (50.1) | - | - | - |
| Boys | 4976 (49.9) | - | - | - |
| Sexual Orientation | ||||
| Heterosexual | 8216 (84.6) | 3900 (77.8) | 4316 (91.4) | 439.80 (3) |
| Gay or lesbian | 278 (2.5) | 152 (2.8) | 126 (2.3) | p < 0.001 *** |
| Bisexual | 888 (8.8) | 732 (14.1) | 156 (3.6) | |
| Not sure | 399 (4.0) | 264 (5.4) | 135 (2.7) | |
| Race/Ethnicity | ||||
| White, non-Hispanic | 5408 (54.9) | 2787 (54.2) | 2621 (55.6) | 8.22 (3) |
| Black, non-Hispanic | 1220 (9.1) | 631 (8.6) | 589 (9.5) | p < 0.05 * |
| Hispanic/Latino | 2362 (25.6) | 1251 (26.7) | 1111 (24.5) | |
| Other races | 1099 (10.4) | 568 (10.5) | 531 (10.4) | |
| Grade Level | ||||
| 9th grade | 2704 (26.5) | 1436 (26.1) | 1268 (26.9) | 1.10 (3) |
| 10th grade | 2813 (25.6) | 1466 (25.8) | 1347 (25.4) | p = 0.78 |
| 11th grade | 2514 (24.2) | 1275 (24.3) | 1239 (24.1) | |
| 12th grade | 2236 (23.7) | 1139 (23.8) | 1097 (23.6) | |
| CV | 1644 (16.0) | 1104 (20.7) | 540 (11.3) | 183.82 (1) p < 0.001 *** |
| Suicidality | 2211 (20.1) | 1422 (25.2) | 789 (15.0) | 184.28 (1) p < 0.001 *** |
| Depression | 3865 (37.5) | 2499 (47.4) | 1366 (27.6) | 471.82 (1) p < 0.001 *** |
| SV | 975 (10.7) | 733 (16.6) | 242 (4.9) | 361.01 (1) p < 0.001 *** |
| Binge Drinking | 1201 (14.1) | 662 (15.1) | 539 (13.1) | 8.40 (1) p < 0.01 ** |
| Illicit Drug Use | 1185 (13.6) | 567 (13.2) | 618 (14.0) | 1.39 (1) p = 0.24 |
| Violence Engagement | 2020 (21.4) | 756 (15.1) | 1264 (27.9) | 253.058 (1) p < 0.001 *** |
| OR (95% CI) p Value | Model 1 AOR (95% CI) p Value | Model 2 AOR (95% CI) p Value | |
|---|---|---|---|
| (a) | |||
| CV | 3.55 (3.18, 3.96) p < 0.001 *** | 3.18 (2.82, 3.59) p < 0.001 *** | 1.64 (1.39, 1.93) p < 0.001 *** |
| Gender | |||
| Boys (ref) | - | - | - |
| Girls | - | 1.41 (1.26, 1.57) p < 0.001 *** | 1.10 (0.95, 1.27) p = 0.23 |
| Sexual Orientation | |||
| Heterosexual (ref) | - | - | - |
| Gay or lesbian | - | 3.97 (3.06, 5.14) p < 0.001 *** | 3.47 (2.44, 4.92) p < 0.001 *** |
| Bisexual | - | 4.95 (4.26, 5.75) p < 0.001 *** | 3.78 (3.11, 4.60) p < 0.001 *** |
| Not sure | - | 2.71 (2.18, 3.37) p < 0.001 *** | 2.48 (1.85, 3.32) p < 0.001 *** |
| Race/Ethnicity | |||
| White (ref) | - | - | - |
| Black | - | 1.26 (1.04, 1.51) p < 0.05 * | 1.28 (0.99, 1.64) p = 0.06 |
| Hispanic/Latino | - | 1.01 (0.89, 1.14) p = 0.91 | 0.80 (0.68, 0.94) p < 0.01 ** |
| Other races | - | 1.35 (1.15, 1.59) p < 0.001 *** | 1.40 (1.13, 1.74) p < 0.01 ** |
| Grade Level | |||
| 9th grade (ref) | - | - | - |
| 10th grade | - | 1.06 (0.91, 1.22) p = 0.47 | 0.95 (0.78, 1.14) p = 0.56 |
| 11th grade | - | 1.09 (0.94, 1.27) p = 0.24 | 0.99 (0.81, 1.19) p = 0.88 |
| 12th grade | - | 1.17 (1.01, 1.35) p < 0.05 * | 0.98 (0.81, 1.19) p = 0.85 |
| Depression | - | - | 11.14 (9.50, 13.05) p < 0.001 *** |
| SV | - | - | 1.55 (1.27, 1.88) p < 0.001 *** |
| Binge Drinking | - | - | 1.12 (0.93, 1.34) p = 0.25 |
| Illicit Drug Use | - | - | 2.00 (1.66, 2.41) p < 0.001 *** |
| Violence Engagement | - | - | 1.67 (1.42, 1.96) p < 0.001 *** |
| (b) | |||
| CV | 3.02 (2.64, 3.46) p < 0.001 *** | 3.07 (2.64, 3.58) p < 0.001 *** | 1.71 (1.39, 2.10) p < 0.001 *** |
| Sexual Orientation | |||
| Heterosexual (ref) | - | - | - |
| Gay or lesbian | - | 4.53 (3.21, 6.40) p < 0.001 *** | 4.25 (2.67, 6.78) p < 0.001 *** |
| Bisexual | - | 4.33 (3.65, 5.14) p < 0.001 *** | 3.15 (2.52, 3.95) p < 0.001 *** |
| Not sure | - | 2.60 (2.00, 3.38) p < 0.001 *** | 2.37 (1.67, 3.35) p < 0.001 *** |
| Race/Ethnicity | |||
| White (ref) | - | - | - |
| Black | - | 1.51 (1.18, 1.93) p < 0.001 *** | 1.68 (1.20, 2.34) p < 0.01 ** |
| Hispanic/Latino | - | 1.11 (0.95, 1.31) p = 0.19 | 0.89 (0.72, 1.09) p = 0.26 |
| Other races | - | 1.42 (1.14, 1.77) p < 0.05 * | 1.74 (1.30, 2.34) p < 0.001 *** |
| Grade Level | |||
| 9th grade (ref) | - | - | - |
| 10th grade | - | 1.01 (0.83, 1.21) p = 0.95 | 0.84 (0.66, 1.08) p = 0.17 |
| 11th grade | - | 0.98 (0.81, 1.19) p = 0.87 | 0.84 (0.65, 1.08) p = 0.17 |
| 12th grade | - | 1.09 (0.90, 1.31) p = 0.40 | 0.88 (0.68, 1.14) p = 0.35 |
| Depression | - | - | 13.08 (10.36, 16.51) p < 0.001 *** |
| SV | - | - | 1.60 (1.28, 1.99) p < 0.001 *** |
| Binge Drinking | - | - | 1.46 (1.15, 1.85) p < 0.01 ** |
| Illicit Drug Use | - | - | 1.61 (1.25, 2.07) p < 0.001 *** |
| Violence Engagement | - | - | 1.65 (1.30, 2.09) p < 0.001 *** |
| (c) | |||
| CV | 3.84 (3.19, 4.61) p < 0.001 *** | 3.53 (2.89, 4.32) p < 0.001 *** | 1.71 (1.30, 2.26) p < 0.001 *** |
| Sexual Orientation | |||
| Heterosexual (ref) | - | - | - |
| Gay or lesbian | - | 3.31 (2.21, 4.97) p < 0.001 *** | 2.82 (1.62, 4.91) p < 0.001 *** |
| Bisexual | - | 7.71 (5.64, 10.56) p < 0.001 *** | 7.89 (5.13, 12.12) p < 0.001 *** |
| Not sure | - | 2.87 (1.96, 4.20) p < 0.001 *** | 2.63 (1.51, 4.58) p < 0.001 *** |
| Race/Ethnicity | |||
| White (ref) | - | - | - |
| Black | - | 1.01 (0.75, 1.35) p = 0.97 | 0.96 (0.65, 1.43) p = 0.85 |
| Hispanic/Latino | - | 0.89 (0.73, 1.09) p = 0.27 | 0.74 (0.57, 0.96) p < 0.05 * |
| Other races | - | 1.27 (0.99, 1.64) p = 0.06 | 1.16 (0.84, 1.61) p = 0.37 |
| Grade Level | |||
| 9th grade (ref) | - | - | - |
| 10th grade | - | 1.13 (0.90, 1.43) p = 0.29 | 1.08 (0.80, 1.46) p = 0.63 |
| 11th grade | - | 1.27 (1.01, 1.60) p < 0.05 * | 1.22 (0.91, 1.65) p = 0.19 |
| 12th grade | - | 1.29 (1.03, 1.62) p < 0.05 * | 1.10 (0.81, 1.48) p = 0.54 |
| Depression | - | - | 9.36 (7.48, 11.72) p < 0.001 *** |
| SV | - | - | 1.38 (0.89, 2.14) p = 0.15 |
| Binge Drinking | - | - | 0.72 (0.53, 0.99) p < 0.05 * |
| Illicit Drug Use | - | - | 2.63 (1.99, 3.48) p < 0.001*** |
| Violence Engagement | - | - | 1.82 (1.44, 2.29) p < 0.001 *** |
| Model 1 AOR (95% CI) p Value | Model 2 AOR (95% CI) p Value | |
|---|---|---|
| (a) | ||
| CV | 3.28 (2.85, 3.76) p < 0.001 *** | - |
| SV | 4.07 (3.43, 4.81) p < 0.001 *** | - |
| CV × SV | 0.71 (0.54, 0.95) p < 0.05 * | - |
| Neither CV nor SV (ref) | - | - |
| SV only (No CV) | - | 2.10 (1.71, 2.58) p < 0.001 *** |
| CV only (No SV) | - | 1.69 (1.41, 2.03) p < 0.001 *** |
| Both CV and SV | - | 4.90 (3.86, 6.22) p < 0.001 *** |
| (b) | ||
| CV | 2.70 (2.25, 3.24) p < 0.001 *** | - |
| SV | 3.07 (2.51, 3.75) p < 0.001 *** | - |
| CV × SV | 0.90 (0.64, 1.26) p = 0.55 | - |
| Neither CV nor SV (ref) | - | - |
| SV only (No CV) | - | 1.50 (1.17, 1.92) p = 0.001 ** |
| CV only (No SV) | - | 1.32 (1.05, 1.66) p < 0.05 * |
| Both CV and SV | - | 3.65 (2.77, 4.81) p < 0.001 *** |
| (c) | ||
| CV | 3.83 (3.09, 4.74) p < 0.001 *** | - |
| SV | 5.61 (4.06, 7.76) p < 0.001 *** | - |
| CV × SV | 0.53 (0.30, 0.94) p < 0.05 * | - |
| Neither CV nor SV (ref) | - | - |
| SV only (No CV) | - | 3.66 (2.49, 5.39) p < 0.001 *** |
| CV only (No SV) | - | 2.50 (1.85, 3.38) p < 0.001 *** |
| Both CV and SV | - | 7.39 (4.50, 12.14) p < 0.001 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levine, R.S.; Bintliff, A.V.; Raj, A. Gendered Analysis of Cyberbullying Victimization and Its Associations with Suicidality: Findings from the 2019 Youth Risk Behavior Survey. Adolescents 2022, 2, 235-251. https://doi.org/10.3390/adolescents2020019
Levine RS, Bintliff AV, Raj A. Gendered Analysis of Cyberbullying Victimization and Its Associations with Suicidality: Findings from the 2019 Youth Risk Behavior Survey. Adolescents. 2022; 2(2):235-251. https://doi.org/10.3390/adolescents2020019
Chicago/Turabian StyleLevine, Rebecca S., Amy Vatne Bintliff, and Anita Raj. 2022. "Gendered Analysis of Cyberbullying Victimization and Its Associations with Suicidality: Findings from the 2019 Youth Risk Behavior Survey" Adolescents 2, no. 2: 235-251. https://doi.org/10.3390/adolescents2020019
APA StyleLevine, R. S., Bintliff, A. V., & Raj, A. (2022). Gendered Analysis of Cyberbullying Victimization and Its Associations with Suicidality: Findings from the 2019 Youth Risk Behavior Survey. Adolescents, 2(2), 235-251. https://doi.org/10.3390/adolescents2020019