

Advances in Understanding Chronic Traumatic Encephalopathy: A Systematic Review of Clinical and Pathological Evidence
 , , , , , ,
, , , , , ,
Abstract
1. Introduction
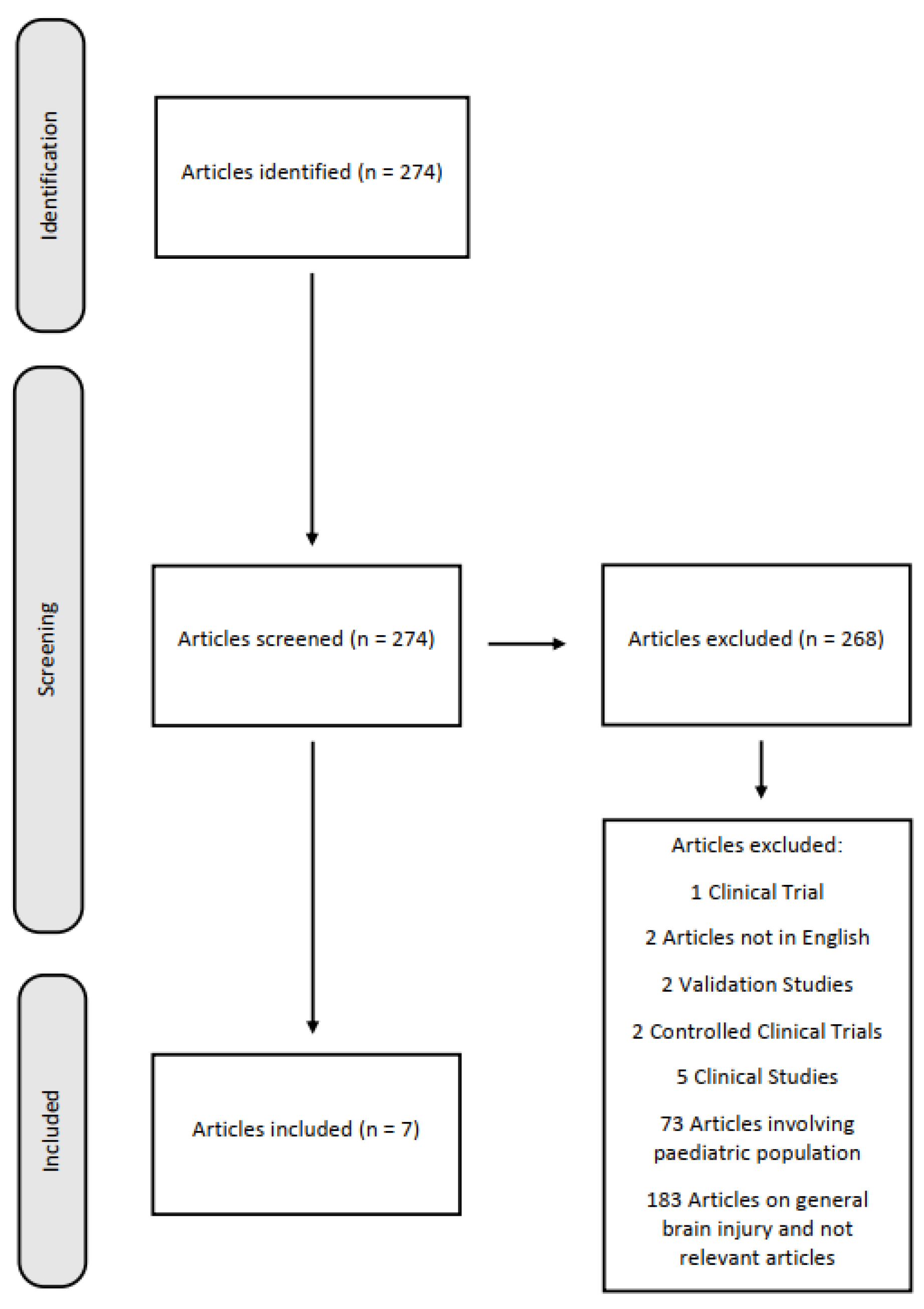
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TBI | Traumatic Brain Injury |
| CTE | Chronic Traumatic Encephalopathy |
| NFTs | Neurofibrillary Tangles |
| NINDS | National Institute of Neurological Disorders and Stroke |
| NIBIB | National Institute of Biomedical Imaging and Bioengineering |
| TES | Traumatic Encephalopathy Syndrome |
| TDP-43 | Transactive response DNA-binding protein 43 |
References
- Pinchi, E.; Frati, A.; Cipolloni, L.; Aromatario, M.; Gatto, V.; La Russa, R.; Pesce, A.; Santurro, A.; Fraschetti, F.; Frati, P.; et al. Clinical-Pathological Study on β-APP, IL-1β, GFAP, NFL, Spectrin II, 8OHdG, TUNEL, MiR-21, MiR-16, MiR-92 Expressions to Verify DAI-Diagnosis, Grade and Prognosis. Sci. Rep. 2018, 8, 2387. [Google Scholar] [CrossRef]
- Benevento, M.; d’Amati, A.; Nicolì, S.; Ambrosi, L.; Baj, J.; Ferorelli, D.; Ingravallo, G.; Solarino, B. Dura Mater and Survival Time Determination in Individuals Who Died after Traumatic Brain Injury: A Preliminary Study. Forensic Sci. Med. Pathol. 2025, 21, 107–114. [Google Scholar] [CrossRef]
- Omalu, B.I.; Fitzsimmons, R.P.; Hammers, J.; Bailes, J. Chronic Traumatic Encephalopathy in a Professional American Wrestler. J. Forensic Nurs. 2010, 6, 130–136. [Google Scholar] [CrossRef]
- Omalu, B.I.; Bailes, J.; Hammers, J.L.; Fitzsimmons, R.P. Chronic Traumatic Encephalopathy, Suicides and Parasuicides in Professional American Athletes: The Role of the Forensic Pathologist. Am. J. Forensic Med. Pathol. 2010, 31, 130–132. [Google Scholar] [CrossRef]
- Scanlon, M.M.; Shields, M.M.; Perl, D.P.; Priemer, D.S. Chronic Traumatic Encephalopathy Pathognomonic Lesions Occurring in Isolation Adjacent to Infiltrative and Non-Infiltrative White Matter Lesions. J. Neuropathol. Exp. Neurol. 2024, 83, 695–700. [Google Scholar] [CrossRef]
- Turk, K.W.; Budson, A.E. Chronic Traumatic Encephalopathy. Continuum 2019, 25, 187–207. [Google Scholar] [CrossRef]
- Byard, R.; Tiemensma, M.; Buckland, M.E.; Vink, R. Chronic Traumatic Encephalopathy (CTE)-Features and Forensic Considerations. Forensic Sci. Med. Pathol. 2023, 19, 620–624. [Google Scholar] [CrossRef] [PubMed]
- Tiemensma, M.; Byard, R.W.; Vink, R.; Affleck, A.J.; Blumbergs, P.; Buckland, M.E. Chronic Traumatic Encephalopathy (CTE) in the Context of Longstanding Intimate Partner Violence. Acta Neuropathol. 2024, 148, 1. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.I.; Bernick, C.; Dodick, D.W.; Mez, J.; Mariani, M.L.; Adler, C.H.; Alosco, M.L.; Balcer, L.J.; Banks, S.J.; Barr, W.B.; et al. National Institute of Neurological Disorders and Stroke Consensus Diagnostic Criteria for Traumatic Encephalopathy Syndrome. Neurology 2021, 96, 848–863. [Google Scholar] [CrossRef] [PubMed]
- Eaton, R.G.; Lonser, R.R. History of Biological, Mechanistic, and Clinical Understanding of Concussion. Neurosurg. Focus 2024, 57, E2. [Google Scholar] [CrossRef] [PubMed]
- De Simone, S.; Vittorio, S.; Cipolloni, L.; Bibbò, R.; Gurgoglione, G.; Fazio, N.D.; Bosco, M.A. Men’s Suicide by Self-Abdominal Cut and Disembowelment: A Literature Review and Analysis of Three Cases. Available online: https://www.jomh.org/articles/10.31083/j.jomh1807158 (accessed on 17 June 2025).
- McKee, A.C.; Stein, T.D.; Huber, B.R.; Crary, J.F.; Bieniek, K.; Dickson, D.; Alvarez, V.E.; Cherry, J.D.; Farrell, K.; Butler, M.; et al. Chronic Traumatic Encephalopathy (CTE): Criteria for Neuropathological Diagnosis and Relationship to Repetitive Head Impacts. Acta Neuropathol. 2023, 145, 371–394. [Google Scholar] [CrossRef]
- Fesharaki-Zadeh, A. Navigating the Complexities of Traumatic Encephalopathy Syndrome (TES): Current State and Future Challenges. Biomedicines 2023, 11, 3158. [Google Scholar] [CrossRef]
- Saulle, M.; Greenwald, B.D. Chronic Traumatic Encephalopathy: A Review. Rehabil. Res. Pract. 2012, 2012, 816069. [Google Scholar] [CrossRef]
- Peacock, W.F.; Kuehl, D.; Bazarian, J.; Singer, A.J.; Cannon, C.; Rafique, Z.; d’Etienne, J.P.; Welch, R.; Clark, C.; Diaz-Arrastia, R. Defining Acute Traumatic Encephalopathy: Methods of the “HEAD Injury Serum Markers and Multi-Modalities for Assessing Response to Trauma” (HeadSMART II) Study. Front. Neurol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- McKee, A.C.; Cantu, R.C.; Nowinski, C.J.; Hedley-Whyte, E.T.; Gavett, B.E.; Budson, A.E.; Santini, V.E.; Lee, H.-S.; Kubilus, C.A.; Stern, R.A. Chronic Traumatic Encephalopathy in Athletes: Progressive Tauopathy after Repetitive Head Injury. J. Neuropathol. Exp. Neurol. 2009, 68, 709–735. [Google Scholar] [CrossRef] [PubMed]
- Tharmaratnam, T.; Iskandar, M.A.; Tabobondung, T.C.; Tobbia, I.; Gopee-Ramanan, P.; Tabobondung, T.A. Chronic Traumatic Encephalopathy in Professional American Football Players: Where Are We Now? Front. Neurol. 2018, 9, 445. [Google Scholar] [CrossRef]
- Arciniega, H.; Baucom, Z.H.; Tuz-Zahra, F.; Tripodis, Y.; John, O.; Carrington, H.; Kim, N.; Knyazhanskaya, E.E.; Jung, L.B.; Breedlove, K.; et al. Brain Morphometry in Former American Football Players: Findings from the DIAGNOSE CTE Research Project. Brain 2024, 147, 3596–3610. [Google Scholar] [CrossRef]
- Omalu, B.; Bailes, J.; Hamilton, R.L.; Kamboh, M.I.; Hammers, J.; Case, M.; Fitzsimmons, R. Emerging Histomorphologic Phenotypes of Chronic Traumatic Encephalopathy in American Athletes. Neurosurgery 2011, 69, 173–183. [Google Scholar] [CrossRef]
- van Amerongen, S.; Kamps, S.; Kaijser, K.K.M.; Pijnenburg, Y.A.L.; Scheltens, P.; Teunissen, C.E.; Barkhof, F.; Ossenkoppele, R.; Rozemuller, A.J.M.; Stern, R.A.; et al. Severe CTE and TDP-43 Pathology in a Former Professional Soccer Player with Dementia: A Clinicopathological Case Report and Review of the Literature. Acta Neuropathol. Commun. 2023, 11, 77. [Google Scholar] [CrossRef]
- Castellani, R.J.; Perry, G. Tau Biology, Tauopathy, Traumatic Brain Injury, and Diagnostic Challenges. J. Alzheimer’s Dis. 2019, 67, 447–467. [Google Scholar] [CrossRef]
- Ruchika, F.; Shah, S.; Neupane, D.; Vijay, R.; Mehkri, Y.; Lucke-Wold, B. Understanding the Molecular Progression of Chronic Traumatic Encephalopathy in Traumatic Brain Injury, Aging and Neurodegenerative Disease. Int. J. Mol. Sci. 2023, 24, 1847. [Google Scholar] [CrossRef]
- Blaylock, R.L.; Maroon, J. Immunoexcitotoxicity as a Central Mechanism in Chronic Traumatic Encephalopathy—A Unifying Hypothesis. Surg. Neurol. Int. 2011, 2, 107. Available online: https://www.semanticscholar.org/paper/Immunoexcitotoxicity-as-a-central-mechanism-in-Blaylock-Maroon/83d4fb51df4b528715345e2d7d819f98c5bbcfcb (accessed on 27 July 2025). [CrossRef] [PubMed]
- Falcon, B.; Zivanov, J.; Zhang, W.; Murzin, A.G.; Garringer, H.J.; Vidal, R.; Crowther, R.A.; Newell, K.L.; Ghetti, B.; Goedert, M.; et al. Novel Tau Filament Fold in Chronic Traumatic Encephalopathy Encloses Hydrophobic Molecules. Nature 2019, 568, 420–423. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Pearce, A.J.; Sy, J.; Lee, M.; Harding, A.; Mobbs, R.; Batchelor, J.; Suter, C.M.; Buckland, M.E. Chronic Traumatic Encephalopathy in a Former Australian Rules Football Player Diagnosed with Alzheimer’s Disease. Acta Neuropathol. Commun. 2020, 8, 23. [Google Scholar] [CrossRef]
- Del Bigio, M.R.; Krawitz, S.; Sinha, N. Chronic Traumatic Encephalopathy-Neuropathologic Change in a Routine Neuropathology Service: 7-Year Follow-Up. J. Neuropathol. Exp. Neurol. 2023, 82, 948–957. [Google Scholar] [CrossRef]
- De Paola, L.; Tripi, D.; Napoletano, G.; Marinelli, E.; Montanari Vergallo, G.; Zaami, S. Violence against Women within Italian and European Context: Italian “Pink Code”—Major Injuries and Forensic Expertise of a Socio-Cultural Problem: A Narrative Review. Forensic Sci. 2024, 4, 264–276. [Google Scholar] [CrossRef]
- Mez, J.; Daneshvar, D.H.; Kiernan, P.T.; Abdolmohammadi, B.; Alvarez, V.E.; Huber, B.R.; Alosco, M.L.; Solomon, T.M.; Nowinski, C.J.; McHale, L.; et al. Clinicopathological Evaluation of Chronic Traumatic Encephalopathy in Players of American Football. JAMA 2017, 318, 360–370. [Google Scholar] [CrossRef]
- Brenner, L.A.; Ignacio, R.V.; Blow, F.C. Suicide and Traumatic Brain Injury among Individuals Seeking Veterans Health Administration Services. J. Head Trauma Rehabil. 2011, 26, 257–264. [Google Scholar] [CrossRef]
- Wortzel, H.S.; Shura, R.D.; Brenner, L.A. Chronic Traumatic Encephalopathy and Suicide: A Systematic Review. BioMed Res. Int. 2013, 2013, 424280. [Google Scholar] [CrossRef] [PubMed]
- Piersanti, V.; Napoletano, G.; David, M.C.; Umani Ronchi, F.; Marinelli, E.; De Paola, L.; Zaami, S. Sudden Death Due to Butane Abuse—An Overview. J. Forensic Leg. Med. 2024, 103, 102662. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristic | Chronic Traumatic Encephalopathy | Alzheimer’s Disease |
|---|---|---|
| p-tau Aggregates | Aggregates of hyperphosphorylated tau (p-tau) in glial cells (e.g., astrocytes), neurons, and cell processes, within the vicinity of small vasculature and in the cortical sulci. Typically presents in an irregular, “spot-like” pattern in perivascular spaces. Also found in the superficial layer (II-III) of the cerebral cortex and in areas 2 and 4 of the hippocampus. | The locations of p-tau NFTs should largely overlap with those of Aβ amyloid, as well as their presence in the hippocampus. |
| Neurofibrillary Tangles Dimensions | Neurofibrillary Tangles are usually larger in size. | Neurofibrillary Tangles are generally smaller in size. |
| Amyloid-Beta Plaques | Amyloid-Beta plaques may be found in a diffuse pattern in sporadic loci, or may be absent. | The primary diagnostic criterion is the post-mortem finding of amyloid-beta plaques and neuritic amyloid plaques in a laminar distribution (in the middle frontal gyrus, the superior and middle temporal gyri, and the inferior parietal lobule). Secondary depositions may also be found in the cerebellum and basal ganglia. |
| TDP-43 Aggregates | Transactive response DNA-binding protein 43 (TDP-43) aggregates are a common finding in the vast majority of Chronic Traumatic Encephalopathy cases, co-localized with p-tau neurofibrillary tangles. Sampling should first be taken from the amygdala and hippocampus. | TDP-43 aggregates are present, but are not co-localized with neurofibrillary tangles. |
| Authors | N. of Cases | Year of Publication | Sex | Age of Death | Profession | Neurological Symptoms and Cognitive and Neuropsychiatric Impairments | Cause of Death | Neuropathology Findings | Toxicological Analysis | History of Traumatic Brain Injury/Clinical History |
|---|---|---|---|---|---|---|---|---|---|---|
| Omalu et al. [3] | 1 | 2010 | male | 40 years old | Professional Wrestler | Reported | Suicide by hanging after killing his wife and son | Neurofibrillary Tangles and Ghost Tangles in the neocortex, subcortical ganglia, and substantia nigra. | Positive for Alprazolam (blood), Hydrocodone (blood), and Testosterone (urine) | Reported |
| Omalu et al. [4] | 5 | 2010 | 5 male | 50 years old 45 years old 44 years old 36 years old 40 years old | 4 professional American football players 1 professional American wrestler | 5 reported | 1 myocardial infarction 1 suicide by ingesting ethylene glycol 1 suicide by a gunshot wound of the head 1 died in traffic accident during a 40-mile-per-hour high-speed police chase 1 suicide by hanging | 1 tau-immunopositive Neurofibrillary Tangles and neuritic threads in the neocortex, subcortical ganglia, and brainstem nuclei, accompanied by amyloid plaques in the neocortex; 4 tau-immunopositive Neurofibrillary Tangles and neuritic threads in the neocortex, subcortical ganglia, and brainstem nuclei without amyloid plaques. | Not reported | Reported |
| Scanlon et al. [5] | 3 | 2024 | 3 male | 41 years old 46 years old 52 years old | 1 former service member of the Navy 1 Service member in the Special Forces 1 Military veteran | Not reported | 1 acute pulmonary embolism 1 glioblastoma 1 acute myocardial infarction | 3 isolated Chronic Traumatic Encephalopathy pathognomonic lesions adjacent to the underlying white matter | Not reported | 1 motor vehicle accident and sustained a traumatic brain injury associated with loss of consciousness 1 combat deployment, participation in boxing 1 participation in wrestling and American Football in High School |
| Tiemensma et al. [8] | 2 | 2024 | 2 female | Fourth decade of life Fifth decade of life | Not reported | Not reported | 1 alleged assault 1 struck by motor vehicle | 1 perivascular foci of neuronal p-tau immunoreactivity at sulcal depths; 1 perivascular foci of neuronal p-tau immunoreactivity in left dorsolateral frontal cortex and at sulcal depths. | Not reported | 2 repeated head injury in the context of longstanding Intimate Partner Violence |
| Van Amerongen et al. [20] | 1 | 2023 | male | 63 years old | Professional soccer player | Reported | COVID-19 infection | 1 frontal and parietal cortex, neuronal tau pathology was found with predilection of sulcal depths and perivascular regions | Not reported | Decent had experienced multiple collisions that involved head impact playing soccer, at least once leading to loss of consciousness. |
| Pearce et al. [26] | 1 | 2020 | male | Ninth decade of life | Australian rules football player | Reported | Not reported | 1 Tau pathology was found with predilection of sulcal depths and perivascular regions; Beta-amyloid and neuritic plaques | Not reported | The decedent had played more than 350 first-grade matches of Australian Rule Football over 19 years. |
| Del Bigio et al. [27] | 16 | 2023 | 14 male 2 female | 2 35-year-olds 37 years old 42 years old 2 44-year-olds 2 46 years old 47 years old 2 50-year-old 51 years old 2 52-year-olds 54 years old 61 years old | Not reported | Reported | 4 Homicide 1 Sudden death, complications of chronic alcoholism 1 Smoke inalation 1 Hypertrophic cardiomiopaty and congestive heart failure 2 Undetermined 1 Choked on food 1 Probable seizure + dilated cardiomyopathy 1 Acute subdural hematoma with minimal external evidence of head trauma 1 Sepsis secondary to scalp wound infection 1 Alcohol toxicity/hypothermia 1 Accidental head trauma + cardiac arrest + hypothermia 1 Ischemic heart disease + metastatic carcinoma in mediastinum | 16 Chronic Traumatic Encephalopathy p-tau immunoreactivity ranging from a single small focus to widespread abnormalities (7 high Chronic Traumatic Encephalopathy, 9 low Chronic Traumatic Encephalopathy) | Not reported | 5 Alcohol and drug abuse 1 Alcohol abuse, alcohol withdrawal seizures/post-traumatic epilepsy 3 Alcohol abuse 1 Short limb dwarfism, cognitive delay, blind from ret- inal detachments, seizures 1 Alcohol, cocaine, methamphetamine, and marijuana use; schizophrenia 1 Cerebral palsy with spastic diplegia and cognitive delay sec- ondary to perinatal hypoxia, suspected fetal alcohol spectrum disorder 1 Seizure disorder since infancy, long-time abuse of solvents and alcohol, Wer- nicke-Korsakoff syndrome 1 Hypoxic brain damage at birth (breech pre- sentation and cord prolapse), cognitive delay, seizure disor- der; chronic alcohol abuse; diabetes mel- litus type 2 1 Headaches and several Assaults 1 Abusive head trauma at 10 months age, mild hydrocephalus (shunt nonfunction- ing), cognitive delay, chronic alcohol abuse |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orsini, F.; Pollice, G.; Carpano, F.; Cipolloni, L.; Cioffi, A.; Cecannecchia, C.; Bibbò, R.; De Simone, S. Advances in Understanding Chronic Traumatic Encephalopathy: A Systematic Review of Clinical and Pathological Evidence. Forensic Sci. 2025, 5, 33. https://doi.org/10.3390/forensicsci5030033
Orsini F, Pollice G, Carpano F, Cipolloni L, Cioffi A, Cecannecchia C, Bibbò R, De Simone S. Advances in Understanding Chronic Traumatic Encephalopathy: A Systematic Review of Clinical and Pathological Evidence. Forensic Sciences. 2025; 5(3):33. https://doi.org/10.3390/forensicsci5030033
Chicago/Turabian StyleOrsini, Francesco, Giovanni Pollice, Francesco Carpano, Luigi Cipolloni, Andrea Cioffi, Camilla Cecannecchia, Roberta Bibbò, and Stefania De Simone. 2025. "Advances in Understanding Chronic Traumatic Encephalopathy: A Systematic Review of Clinical and Pathological Evidence" Forensic Sciences 5, no. 3: 33. https://doi.org/10.3390/forensicsci5030033
APA StyleOrsini, F., Pollice, G., Carpano, F., Cipolloni, L., Cioffi, A., Cecannecchia, C., Bibbò, R., & De Simone, S. (2025). Advances in Understanding Chronic Traumatic Encephalopathy: A Systematic Review of Clinical and Pathological Evidence. Forensic Sciences, 5(3), 33. https://doi.org/10.3390/forensicsci5030033