
Anabolic–Androgenic Steroids and Brain Damage: A Review of Evidence and Medico-Legal Implications


 , , ,
, , , 
Abstract
1. Introduction
2. Neuroanatomical Effects of Anabolic–Androgenic Steroids
3. Cognitive Impairments Associated with Anabolic–Androgenic Steroid Use
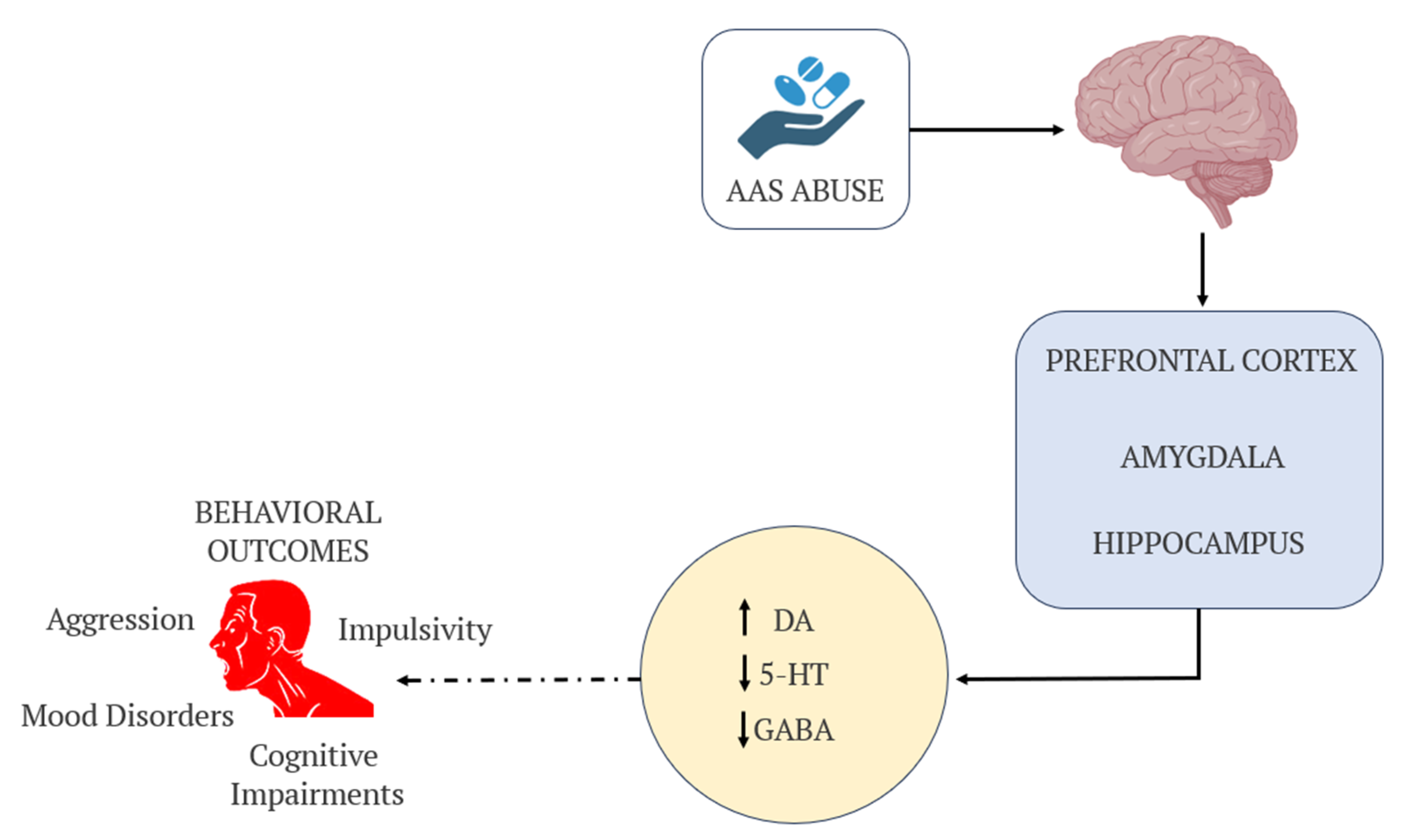
4. Behavioral Changes and Mental Health Implications
5. Enhancing Accuracy and Efficiency in Medical Record Management with AI
6. AASs Use Among Women
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AASs | Anabolic–androgenic steroids. |
| ARs | Androgen receptors. |
| CNS | Central nervous system. |
| fMRI | Functional magnetic resonance imaging. |
| GABA | Gamma-aminobutyric acid. |
| HPA | Hypothalamic–pituitary–adrenal. |
| HPG | Hypothalamic–pituitary–gonadal. |
| LDL | Low-density lipoprotein. |
| HDLs | High-density lipoprotein. |
| ROS | Reactive oxygen species. |
References
- Wenbo, Z.; Yan, Z. The Uses of Anabolic Androgenic Steroids Among Athletes; Its Positive and Negative Aspects-A Literature Review. J. Multidiscip. Healthc. 2023, 16, 4293–4305. [Google Scholar] [CrossRef] [PubMed]
- Goldman, A.; Basaria, S. Adverse Health Effects of Androgen Use. Mol. Cell Endocrinol. 2018, 464, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Tauchen, J.; Jurášek, M.; Huml, L.; Rimpelová, S. Medicinal Use of Testosterone and Related Steroids Revisited. Molecules 2021, 26, 1032. [Google Scholar] [CrossRef] [PubMed]
- Agriesti, F.; Tataranni, T.; Pacelli, C.; Scrima, R.; Laurenzana, I.; Ruggieri, V.; Cela, O.; Mazzoccoli, C.; Salerno, M.; Sessa, F.; et al. Nandrolone Induces a Stem Cell-like Phenotype in Human Hepatocarcinoma-Derived Cell Line Inhibiting Mitochondrial Respiratory Activity. Sci. Rep. 2020, 10, 2287. [Google Scholar] [CrossRef] [PubMed]
- Fadah, K.; Gopi, G.; Lingireddy, A.; Blumer, V.; Dewald, T.; Mentz, R.J. Anabolic Androgenic Steroids and Cardiomyopathy: An Update. Front. Cardiovasc. Med. 2023, 10, 1214374. [Google Scholar] [CrossRef] [PubMed]
- Piacentino, D.; Kotzalidis, G.D.G.; Casale, A.; Aromatario, M.; Pomara, C.; Girardi, P.; Sani, G.; del Casale, A.; Aromatario, M.; Pomara, C.; et al. Anabolic-Androgenic Steroid Use and Psychopathology in Athletes. A Systematic Review. Curr. Neuropharmacol. 2014, 13, 101–121. [Google Scholar] [CrossRef] [PubMed]
- Sessa, F.; Salerno, M.; Bertozzi, G.; Cipolloni, L.; Messina, G.; Aromatario, M.; Polo, L.; Turillazzi, E.; Pomara, C. MiRNAs as Novel Biomarkers of Chronic Kidney Injury in Anabolic-Androgenic Steroid Users: An Experimental Study. Front. Pharmacol. 2020, 11, 563756. [Google Scholar] [CrossRef] [PubMed]
- Bertozzi, G.; Sessa, F.; Albano, G.D.G.D.; Sani, G.; Maglietta, F.; Roshan, M.H.K.M.H.K.; Volti, G.L.G.L.; Bernardini, R.; Avola, R.; Pomara, C.; et al. The Role of Anabolic Androgenic Steroids in Disruption of the Physiological Function in Discrete Areas of the Central Nervous System. Mol. Neurobiol. 2017, 55, 5548–5556. [Google Scholar] [CrossRef] [PubMed]
- Cardenas-Iniguez, C.; Burnor, E.; Herting, M.M. Neurotoxicants, the Developing Brain, and Mental Health. Biol. Psychiatry Glob. Open Sci. 2022, 2, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Zundel, C.G.; Ryan, P.; Brokamp, C.; Heeter, A.; Huang, Y.; Strawn, J.R.; Marusak, H.A. Air Pollution, Depressive and Anxiety Disorders, and Brain Effects: A Systematic Review. Neurotoxicology 2022, 93, 272–300. [Google Scholar] [CrossRef] [PubMed]
- Barone, R.; Pitruzzella, A.; Marino Gammazza, A.; Rappa, F.; Salerno, M.; Barone, F.; Sangiorgi, C.; D’Amico, D.; Locorotondo, N.; Di Gaudio, F.; et al. Nandrolone Decanoate Interferes with Testosterone Biosynthesis Altering Blood–Testis Barrier Components. J. Cell Mol. Med. 2017, 21, 1636–1647. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Lee, H.; Woo, S.; Lee, H.; Park, J.; Kim, T.; Fond, G.; Boyer, L.; Rahmati, M.; Smith, L.; et al. Global, Regional, and National Trends in Drug Use Disorder Mortality Rates across 73 Countries from 1990 to 2021, with Projections up to 2040: A Global Time-Series Analysis and Modelling Study. eClinicalMedicine 2025, 79, 102985. [Google Scholar] [CrossRef] [PubMed]
- Schwartzer, J.J.; Ricci, L.A.; Melloni, R.H. Interactions between the Dopaminergic and GABAergic Neural Systems in the Lateral Anterior Hypothalamus of Aggressive AAS-Treated Hamsters. Behav. Brain Res. 2009, 203, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Pomara, C.; Neri, M.; Bello, S.; Fiore, C.; Riezzo, I.; Turillazzi, E. Neurotoxicity by Synthetic Androgen Steroids: Oxidative Stress, Apoptosis, and Neuropathology: A Review. Curr. Neuropharmacol. 2014, 13, 132–145. [Google Scholar] [CrossRef] [PubMed]
- Hauger, L.E.; Westlye, L.T.; Fjell, A.M.; Walhovd, K.B.; Bjørnebekk, A. Structural Brain Characteristics of Anabolic–Androgenic Steroid Dependence in Men. Addiction 2019, 114, 1405–1415. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, R.L.; Lumia, A.R.; McGinnis, M.Y. Androgenic Anabolic Steroid Exposure during Adolescence: Ramifications for Brain Development and Behavior. Horm. Behav. 2013, 64, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Sessa, F.; Esposito, M.; Salerno, M. Experimental Studies on Androgen Administration in Animal Models: Current and Future Perspectives. Curr. Opin. Endocrinol. Diabetes Obes. 2022, 29, 566–585. [Google Scholar] [CrossRef] [PubMed]
- Solomon, Z.J.; Mirabal, J.R.; Mazur, D.J.; Kohn, T.P.; Lipshultz, L.I.; Pastuszak, A.W. Selective Androgen Receptor Modulators: Current Knowledge and Clinical Applications. Sex. Med. Rev. 2019, 7, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Kanayama, G.; Brower, K.J.; Wood, R.I.; Hudson, J.I.; Pope, H.G. Anabolic-Androgenic Steroid Dependence: An Emerging Disorder. Addiction 2009, 104, 1966–1978. [Google Scholar] [CrossRef] [PubMed]
- Morrison, T.R.; Sikes, R.W.; Melloni, R.H. Anabolic Steroids Alter the Physiological Activity of Aggression Circuits in the Lateral Anterior Hypothalamus. Neuroscience 2016, 315, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Weiss, N.H.; Sullivan, T.P.; Tull, M.T. Explicating the Role of Emotion Dysregulation in Risky Behaviors: A Review and Synthesis of the Literature with Directions for Future Research and Clinical Practice. Curr. Opin. Psychol. 2015, 3, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Hinds, J.A.; Sanchez, E.R. The Role of the Hypothalamus–Pituitary–Adrenal (HPA) Axis in Test-Induced Anxiety: Assessments, Physiological Responses, and Molecular Details. Stresses 2022, 2, 146–155. [Google Scholar] [CrossRef]
- Karin, O.; Raz, M.; Tendler, A.; Bar, A.; Korem Kohanim, Y.; Milo, T.; Alon, U. A New Model for the HPA Axis Explains Dysregulation of Stress Hormones on the Timescale of Weeks. Mol. Syst. Biol. 2020, 16, e9510. [Google Scholar] [CrossRef] [PubMed]
- Sessa, F.; Polito, R.; Li Rosi, G.; Salerno, M.; Esposito, M.; Pisanelli, D.; Ministeri, F.; Messina, A.; Carotenuto, M.; Chieffi, S.; et al. Neurobiology and Medico-Legal Aspects of Suicides among Older Adults: A Narrative Review. Front. Psychiatry 2024, 15, 1449526. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, K.L.; Porter, D.M.; Henderson, L.P. Anabolic Androgenic Steroids Induce Age-, Sex-, and Dose-Dependent Changes in GABAA Receptor Subunit MRNAs in the Mouse Forebrain. Neuropharmacology 2002, 43, 634–645. [Google Scholar] [CrossRef] [PubMed]
- Masonis, A.E.T.; McCarthy, M.P. Effects of the Androgenic/Anabolic Steroid Stanozolol on GABAA Receptor Function: GABA-Stimulated 36Cl- Influx and [35S] TBPS Binding. J. Pharmacol. Exp. Ther. 1996, 279, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Petito, A.; Altamura, M.; Iuso, S.; Padalino, F.A.; Sessa, F.; D’Andrea, G.; Margaglione, M.; Bellomo, A. The Relationship between Personality Traits, the 5HTT Polymorphisms, and the Occurrence of Anxiety and Depressive Symptoms in Elite Athletes. PLoS ONE 2016, 11, e0156601. [Google Scholar] [CrossRef] [PubMed]
- Bertozzi, G.; Salerno, M.; Pomara, C.; Sessa, F. Neuropsychiatric and Behavioral Involvement in Aas Abusers. A Literature Review. Medicina 2019, 55, 396. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Copeland, J.L.; Van Helder, W. Effect of Training Status and Exercise Mode on Endogenous Steroid Hormones in Men. J. Appl. Physiol. 2004, 96, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Pope, H.G.; Kanayama, G.; Hudson, J.I. Risk Factors for Illicit Anabolic-Androgenic Steroid Use in Male Weightlifters: A Cross-Sectional Cohort Study. Biol. Psychiatry 2012, 71, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Sessa, F.; Salerno, M.; Di Mizio, G.; Bertozzi, G.; Messina, G.; Tomaiuolo, B.; Pisanelli, D.; Maglietta, F.; Ricci, P.; Pomara, C. Anabolic Androgenic Steroids: Searching New Molecular Biomarkers. Front. Pharmacol. 2018, 9, 1321. [Google Scholar] [CrossRef] [PubMed]
- Salerno, M.; Cascio, O.; Bertozzi, G.; Sessa, F.; Messina, A.; Monda, V.; Cipolloni, L.; Biondi, A.; Daniele, A.; Pomara, C. Anabolic Androgenic Steroids and Carcinogenicity Focusing on Leydig Cell: A Literature Review. Oncotarget 2018, 9, 19415–19426. [Google Scholar] [CrossRef] [PubMed]
- Sessa, F.; Franco, S.; Picciocchi, E.; Geraci, D.; Chisari, M.G.; Marsala, G.; Polito, A.N.; Sorrentino, M.; Tripi, G.; Salerno, M.; et al. Addictions Substance Free during Lifespan. Acta Medica Mediterr. 2018, 34, 2081–2087. [Google Scholar]
- Westlye, L.T.; Kaufmann, T.; Alnæs, D.; Hullstein, I.R.; Bjørnebekk, A. Brain Connectivity Aberrations in Anabolic-Androgenic Steroid Users. Neuroimage Clin. 2017, 13, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Scarth, M.; Bjørnebekk, A. Androgen Abuse and the Brain. Curr. Opin. Endocrinol. Diabetes Obes. 2021, 28, 604–614. [Google Scholar] [CrossRef] [PubMed]
- Bjørnebekk, A.; Kaufmann, T.; Hauger, L.E.; Klonteig, S.; Hullstein, I.R.; Westlye, L.T. Long-Term Anabolic–Androgenic Steroid Use Is Associated With Deviant Brain Aging. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2021, 6, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, M.J.; Janes, A.C.; Hudson, J.I.; Brennan, B.P.; Kanayama, G.; Kerrigan, A.R.; Jensen, J.E.; Pope, H.G. Brain and Cognition Abnormalities in Long-Term Anabolic-Androgenic Steroid Users. Drug Alcohol. Depend. 2015, 152, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Olsen, C.M. Natural Rewards, Neuroplasticity, and Non-Drug Addictions. Neuropharmacology 2011, 61, 1109–1122. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S.; Nasca, C.; Gray, J.D. Stress Effects on Neuronal Structure: Hippocampus, Amygdala, and Prefrontal Cortex. Neuropsychopharmacology 2016, 41, 3–23. [Google Scholar] [CrossRef] [PubMed]
- Amaya, J.M.; Sips, H.C.M.; Viho, E.M.G.; Kroon, J.; Meijer, O.C. Restricted Effects of Androgens on Glucocorticoid Signaling in the Mouse Prefrontal Cortex and Midbrain. Front. Endocrinol. (Lausanne) 2023, 14, 1292024. [Google Scholar] [CrossRef] [PubMed]
- Kalinine, E.; Zimmer, E.R.; Zenki, K.C.; Kalinine, I.; Kazlauckas, V.; Haas, C.B.; Hansel, G.; Zimmer, A.R.; Souza, D.O.; Müller, A.P.; et al. Nandrolone-Induced Aggressive Behavior Is Associated with Alterations in Extracellular Glutamate Homeostasis in Mice. Horm. Behav. 2014, 66, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Nelson, B.S.; Hildebrandt, T.; Wallisch, P. Anabolic–Androgenic Steroid Use Is Associated with Psychopathy, Risk-Taking, Anger, and Physical Problems. Sci. Rep. 2022, 12, 9133. [Google Scholar] [CrossRef] [PubMed]
- Wallin-Miller, K.; Li, G.; Kelishani, D.; Wood, R.I. Anabolic-Androgenic Steroids Alter Decision Making in a Balanced Rodent Model of the Iowa Gambling Task. Behav. Neurosci. 2018, 132, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Raine, A. Prefrontal Structural and Functional Brain Imaging Findings in Antisocial, Violent, and Psychopathic Individuals: A Meta-Analysis. Psychiatry Res. Neuroimaging 2009, 174, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Barth, C.; Villringer, A.; Sacher, J. Sex Hormones Affect Neurotransmitters and Shape the Adult Female Brain during Hormonal Transition Periods. Front. Neurosci. 2015, 9, 37. [Google Scholar] [CrossRef] [PubMed]
- Olufunmilayo, E.O.; Gerke-Duncan, M.B.; Holsinger, R.M.D. Oxidative Stress and Antioxidants in Neurodegenerative Disorders. Antioxidants 2023, 12, 517. [Google Scholar] [CrossRef] [PubMed]
- Schieber, M.; Chandel, N.S. ROS Function in Redox Signaling and Oxidative Stress. Curr. Biol. 2014, 24, R453–R462. [Google Scholar] [CrossRef] [PubMed]
- Shao, F.; Wang, X.; Wu, H.; Wu, Q.; Zhang, J. Microglia and Neuroinflammation: Crucial Pathological Mechanisms in Traumatic Brain Injury-Induced Neurodegeneration. Front. Aging Neurosci. 2022, 14, 825086. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Hui, E.S.; Kranz, G.S.; Chang, J.R.; de Luca, K.; Pinto, S.M.; Chan, W.W.; Yau, S.Y.; Chau, B.K.; Samartzis, D.; et al. Potential Mechanisms Underlying the Accelerated Cognitive Decline in People with Chronic Low Back Pain: A Scoping Review. Ageing Res. Rev. 2022, 82, 101767. [Google Scholar] [CrossRef] [PubMed]
- Mikulska, J.; Juszczyk, G.; Gawrońska-Grzywacz, M.; Herbet, M. Hpa Axis in the Pathomechanism of Depression and Schizophrenia: New Therapeutic Strategies Based on Its Participation. Brain Sci. 2021, 11, 1298. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Xu, F.; Yang, L.; Tuolihong, L.; Wang, X.; Du, Z.; Zhang, Y.; Yin, X.; Li, Y.; Lu, K.; et al. Involvement of the GABAergic System in PTSD and Its Therapeutic Significance. Front. Mol. Neurosci. 2023, 16, 1052288. [Google Scholar] [CrossRef] [PubMed]
- Ramey, T.; Regier, P.S. Cognitive Impairment in Substance Use Disorders. CNS Spectr. 2019, 24, 102–113. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Cocimano, G.; Ministrieri, F.; Rosi, G.L.; Nunno, N.D.; Messina, G.; Sessa, F.; Salerno, M. Smart Drugs and Neuroenhancement: What Do We Know? Front. Biosci.-Landmark 2021, 26, 347–359. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.S.; Mitre, M.C.; Brinck-Johnsen, T. Anabolic-Androgenic Steroid and Adrenal Steroid Effects on Hippocampal Plasticity. Brain Res. 1995, 679, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Miranda, M.; Morici, J.F.; Zanoni, M.B.; Bekinschtein, P. Brain-Derived Neurotrophic Factor: A Key Molecule for Memory in the Healthy and the Pathological Brain. Front. Cell Neurosci. 2019, 13, 363. [Google Scholar] [CrossRef] [PubMed]
- Kok, A. Cognitive Control, Motivation and Fatigue: A Cognitive Neuroscience Perspective. Brain Cogn. 2022, 160, 105880. [Google Scholar] [CrossRef] [PubMed]
- Nimgampalle, M.; Chakravarthy, H.; Sharma, S.; Shree, S.; Bhat, A.R.; Pradeepkiran, J.A.; Devanathan, V. Neurotransmitter Systems in the Etiology of Major Neurological Disorders: Emerging Insights and Therapeutic Implications. Ageing Res. Rev. 2023, 89, 101994. [Google Scholar] [CrossRef] [PubMed]
- Mhillaj, E.; Morgese, M.G.; Tucci, P.; Bove, M.; Schiavone, S.; Trabace, L. Effects of Anabolic-Androgens on Brain Reward Function. Front. Neurosci. 2015, 9, 295. [Google Scholar] [CrossRef] [PubMed]
- Gomides, L.; Oliveira, L.A.; Mayers, N.; Lacerda, F.B.; Santos, J.P.B.; Borcard Filho, B.; Assunção, I.N.; Cupertino, M.; Santana, M.G. Neurological consequences of abusive use of anabolic-androgenic steroids. Tempus–Actas Saúde Coletiva 2019, 13, 102–122. [Google Scholar] [CrossRef]
- Pope, H.G.; Wood, R.I.; Rogol, A.; Nyberg, F.; Bowers, L.; Bhasin, S. Adverse Health Consequences of Performance-Enhancing Drugs: An Endocrine Society Scientific Statement. Endocr. Rev. 2014, 35, 341–375. [Google Scholar] [CrossRef] [PubMed]
- Wood, R.I.; Armstrong, A.; Fridkin, V.; Shah, V.; Najafi, A.; Jakowec, M. ’Roid Rage in Rats? Testosterone Effects on Aggressive Motivation, Impulsivity and Tyrosine Hydroxylase. Physiol. Behav. 2013, 110–111, 6–12. [Google Scholar] [CrossRef] [PubMed]
- McGinnis, M.Y. Anabolic Androgenic Steroids and Aggression: Studies Using Animal Models. Ann. N. Y. Acad. Sci. 2004, 1036, 399–415. [Google Scholar] [CrossRef] [PubMed]
- Salem, N.A.; Alnahdi, H.S. The Impact of Nandrolone Decanoate Abuse on Experimental Animal Model: Hormonal and Biochemical Assessment. Steroids 2020, 153, 108526. [Google Scholar] [CrossRef] [PubMed]
- Kanayama, G.; Hudson, J.I.J.I.; Pope, H.G.H.G. Long-Term Psychiatric and Medical Consequences of Anabolic-Androgenic Steroid Abuse: A Looming Public Health Concern? Drug Alcohol Depend 2008, 98, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Thiblin, I.; Finn, A.; Ross, S.B.; Stenfors, C. Increased Dopaminergic and 5-Hydroxytryptaminergic Activities in Male Rat Brain Following Long-Term Treatment with Anabolic Androgenic Steroids. Br. J. Pharmacol. 1999, 126, 1301–1306. [Google Scholar] [CrossRef] [PubMed]
- Karagun, B.; Altug, S. Anabolic-Androgenic Steroids Are Linked to Depression and Anxiety in Male Bodybuilders: The Hidden Psychogenic Side of Anabolic Androgenic Steroids. Ann. Med. 2024, 56, 2337717. [Google Scholar] [CrossRef] [PubMed]
- Norman, C.; Harries, R.L.; Reid, R.; Nisbet, L.A.; Nic Daéid, N. Changing Trends in Anabolic-Androgenic Steroid Use within Scottish Prisons: Detection, Prevalence, and Quantitation. Drug Test. Anal. 2024, 17, 858–867. [Google Scholar] [CrossRef] [PubMed]
- Kreutz, J.; Potemkin, M.; Shah, H.; Lam, D.; Patel, P.; Doyle-Baker, P.K. A Qualitative Exploration of Family Physicians and People Who Use Anabolic Steroids: Barriers to Accessing Evidence-Based Care. Perform. Enhanc. Health 2025, 13, 100319. [Google Scholar] [CrossRef]
- Zoob Carter, B.N.; Boardley, I.D. Development and Validation of Dependence and Craving Measures Specific to Athletes Who Use Anabolic-Androgenic Steroids. Front. Psychol. 2024, 15, 1347211. [Google Scholar] [CrossRef] [PubMed]
- Bagatell, C.J.; Bremner, W.J. Androgens in Men—Uses and Abuses. N. Engl. J. Med. 1996, 334, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Madea, B.; Grellner, W.; Musshoff, F.; Dettmeyer, R. Medico-Legal Aspects of Doping. J. Clin. Forensic Med. 1998, 5, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Klötz, F.; Petersson, A.; Isacson, D.; Thiblin, I. Violent Crime and Substance Abuse: A Medico-Legal Comparison between Deceased Users of Anabolic Androgenic Steroids and Abusers of Illicit Drugs. Forensic Sci. Int. 2007, 173, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Bertozzi, G.; Sessa, F.; Maglietta, F.; Cipolloni, L.; Salerno, M.; Fiore, C.; Fortarezza, P.; Ricci, P.; Turillazzi, E.; Pomara, C. Immunodeficiency as a Side Effect of Anabolic Androgenic Steroid Abuse: A Case of Necrotizing Myofasciitis. Forensic Sci. Med. Pathol. 2019, 15, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Griffith, R.; McNamee, M.; Phillips, N. On the Duty of the Doctor Not to Disclose Athlete Doping Data without Consent. Int. J. Sport. Policy 2011, 3, 191–203. [Google Scholar] [CrossRef]
- Yuan, B.; Li, J. The Policy Effect of the General Data Protection Regulation (GDPR) on the Digital Public Health Sector in the European Union: An Empirical Investigation. Int. J. Environ. Res. Public Health 2019, 16, 1070. [Google Scholar] [CrossRef] [PubMed]
- Bjørnebekk, A.; Walhovd, K.B.; Jørstad, M.L.; Due-Tønnessen, P.; Hullstein, I.R.; Fjell, A.M. Structural Brain Imaging of Long-Term Anabolic-Androgenic Steroid Users and Nonusing Weightlifters. Biol. Psychiatry 2017, 82, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Hildebrandt, T.; Langenbucher, J.W.; Flores, A.; Harty, S.; Berlin, H.A. The Influence of Age of Onset and Acute Anabolic Steroid Exposure on Cognitive Performance, Impulsivity, and Aggression in Men. Psychol. Addict. Behav. 2014, 28, 1096–1104. [Google Scholar] [CrossRef] [PubMed]
- Damião, B.; Rossi-Junior, W.C.; Guerra, F.D.R.; Marques, P.P.; Nogueira, D.A.; Esteves, A. Anabolic Steroids and Their Effects of on Neuronal Density in Cortical Areas and Hippocampus of Mice. Braz. J. Biol. 2021, 81, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Bond, P.; Smit, D.L.; de Ronde, W. Anabolic–Androgenic Steroids: How Do They Work and What Are the Risks? Front. Endocrinol. (Lausanne) 2022, 13, 1059473. [Google Scholar] [CrossRef] [PubMed]
- Zelleroth, S.; Stam, F.; Nylander, E.; Kjellgren, E.; Gising, J.; Larhed, M.; Grönbladh, A.; Hallberg, M. The Decanoate Esters of Nandrolone, Testosterone, and Trenbolone Induce Steroid Specific Memory Impairment and Somatic Effects in the Male Rat. Horm. Behav. 2024, 161, 105501. [Google Scholar] [CrossRef] [PubMed]
- Havnes, I.A.; Jørstad, M.L.; Innerdal, I.; Bjørnebekk, A. Anabolic-Androgenic Steroid Use among Women—A Qualitative Study on Experiences of Masculinizing, Gonadal and Sexual Effects. Int. J. Drug Policy 2021, 95, 102876. [Google Scholar] [CrossRef] [PubMed]
- Basile, J.R.; Binmadi, N.O.; Zhou, H.; Yang, Y.H.; Paoli, A.; Proia, P. Supraphysiological Doses of Performance Enhancing Anabolic-Androgenic Steroids Exert Direct Toxic Effects on Neuron-like Cells. Front. Cell Neurosci. 2013, 7, 69. [Google Scholar] [CrossRef] [PubMed]
- Sharif-Nia, H.; Sivarajan Froelicher, E.; Gorgulu, O.; Osborne, J.W.; Błachnio, A.; Rezazadeh Fazeli, A.; Goudarzian, A.H.; Kaveh, O. The Relationship among Positive Body Image, Body Esteem, and Eating Attitude in Iranian Population. Front. Psychol. 2024, 15, 1304555. [Google Scholar] [CrossRef] [PubMed]
- Baceviciene, M.; Jankauskiene, R. Changes in Sociocultural Attitudes towards Appearance, Body Image, Eating Attitudes and Behaviours, Physical Activity, and Quality of Life in Students before and during COVID-19 Lockdown. Appetite 2021, 166, 105452. [Google Scholar] [CrossRef] [PubMed]
- Yager, Z.; O’Dea, J.A. Relationships between Body Image, Nutritional Supplement Use, and Attitudes towards Doping in Sport among Adolescent Boys: Implications for Prevention Programs. J. Int. Soc. Sports Nutr. 2014, 11, 13. [Google Scholar] [CrossRef] [PubMed]
- Nunno, N.D.; Esposito, M.; Argo, A.; Salerno, M.; Sessa, F. Pharmacogenetics and Forensic Toxicology: A New Step towards a Multidisciplinary Approach. Toxics 2021, 11, 18. [Google Scholar] [CrossRef] [PubMed]
- Bertozzi, G.; Maglietta, F.; Sessa, F.; Scoto, E.; Cipolloni, L.; Di Mizio, G.; Salerno, M.; Pomara, C. Traumatic Brain Injury: A Forensic Approach. A Literature Review. Curr. Neuropharmacol. 2020, 18, 538–550. [Google Scholar] [CrossRef] [PubMed]
- Di Girolamo, F.G.; Biasinutto, C.; Mangogna, A.; Fiotti, N.; Vinci, P.; Pisot, R.; Mearelli, F.; Simunic, B.; Roni, C.; Biolo, G. Metabolic Consequences of Anabolic Steroids, Insulin, and Growth Hormone Abuse in Recreational Bodybuilders: Implications for the World Anti-Doping Agency Passport. Sports Med. Open 2024, 10, 28. [Google Scholar] [CrossRef] [PubMed]
- Bonnecaze, A.K.; O’Connor, T.; Burns, C.A. Harm Reduction in Male Patients Actively Using Anabolic Androgenic Steroids (AAS) and Performance-Enhancing Drugs (PEDs): A Review. J. Gen. Intern. Med. 2021, 36, 2055–2064. [Google Scholar] [CrossRef] [PubMed]
- Al Bishi, K.A.; Afify, A. Prevalence and Awareness of Anabolic Androgenic Steroids (AAS) among Gymnasts in the Western Province of Riyadh, Saudi Arabia. Electron. Physician 2017, 9, 6050–6057. [Google Scholar] [CrossRef] [PubMed]
- de Ronde, W.; Smit, D.L. Anabolic Androgenic Steroid Abuse in Young Males. Endocr. Connect. 2020, 9, R102–R111. [Google Scholar] [CrossRef] [PubMed]
- Ding, J.B.; Ng, M.Z.; Huang, S.S.; Ding, M.; Hu, K. Anabolic-Androgenic Steroid Misuse: Mechanisms, Patterns of Misuse, User Typology, and Adverse Effects. J. Sports Med. 2021, 2021, 7497346. [Google Scholar] [CrossRef] [PubMed]
- Nieschlag, E.; Vorona, E. Mechanisms in Endocrinology: Medical Consequences of Doping with Anabolic Androgenic Steroids: Effects on Reproductive Functions. Eur. J. Endocrinol. 2015, 173, R47–R58. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, J.M.; Avant, R.A.; Charchenko, C.M.; Westerman, M.E.; Ziegelmann, M.J.; Miest, T.S.; Trost, L.W. Impact of Anabolic Androgenic Steroids on Sexual Function. Transl. Androl. Urol. 2018, 7, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Salerno, M.; Calvano, G.; Agliozzo, R.; Ficarra, V.; Sessa, F.; Favilla, V.; Cimino, S.; Pomara, C. Impact of Anabolic Androgenic Steroids on Male Sexual and Reproductive Function: A Systematic Review. Panminerva Med. 2023, 65, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Licciardello, G.; Privitera, F.; Iannuzzi, S.; Liberto, A.; Sessa, F.; Salerno, M. Forensic Post-Mortem Investigation in AAS Abusers: Investigative Diagnostic Protocol. A Systematic Review. Diagnostics 2021, 11, 1307. [Google Scholar] [CrossRef] [PubMed]
- Linhares, B.L.; Miranda, E.P.; Cintra, A.R.; Reges, R.; Torres, L.O. Use, Misuse and Abuse of Testosterone and Other Androgens. Sex. Med. Rev. 2022, 10, 583–595. [Google Scholar] [CrossRef] [PubMed]
- Fyksen, T.S.; Vanberg, P.; Gjesdal, K.; von Lueder, T.G.; Bjørnerheim, R.; Steine, K.; Atar, D.; Halvorsen, S. Cardiovascular Phenotype of Long-Term Anabolic-Androgenic Steroid Abusers Compared with Strength-Trained Athletes. Scand. J. Med. Sci. Sports 2022, 32, 1170–1181. [Google Scholar] [CrossRef] [PubMed]
- Petrovic, A.; Vukadin, S.; Sikora, R.; Bojanic, K.; Smolic, R.; Plavec, D.; Wu, G.Y.; Smolic, M. Anabolic Androgenic Steroid-Induced Liver Injury: An Update. World J. Gastroenterol. 2022, 28, 3071–3080. [Google Scholar] [CrossRef] [PubMed]
- Sessa, F.; Salerno, M.; Cipolloni, L.; Bertozzi, G.; Messina, G.; Di Mizio, G.; Asmundo, A.; Pomara, C. Anabolic-Androgenic Steroids and Brain Injury: MiRNA Evaluation in Users Compared to Cocaine Abusers and Elderly People. Aging 2020, 12, 15314–15327. [Google Scholar] [CrossRef] [PubMed]
- Albano, G.D.; Amico, F.; Cocimano, G.; Liberto, A.; Maglietta, F.; Esposito, M.; Rosi, G.L.; Di Nunno, N.; Salerno, M.; Montana, A. Adverse Effects of Anabolic-Androgenic Steroids: A Literature Review. Healthcare 2021, 9, 97. [Google Scholar] [CrossRef] [PubMed]
- Wood, R.I. Anabolic-Androgenic Steroid Dependence? Insights from Animals and Humans. Front. Neuroendocr. 2008, 29, 490–506. [Google Scholar] [CrossRef] [PubMed]
- Kanayama, G.; Brower, K.J.; Wood, R.I.; Hudson, J.I.; Pope, H.G. Treatment of Anabolic-Androgenic Steroid Dependence: Emerging Evidence and Its Implications. Drug Alcohol. Depend. 2010, 109, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Abrahin, O.; Félix Souza, N.S.; de Sousa, E.C.; Santos, A.M.; Bahrke, M.S. Anabolic–Androgenic Steroid Use among Brazilian Women: An Exploratory Investigation. J. Subst. Use 2016, 22, 246–252. [Google Scholar] [CrossRef]
- Scott, H.M.; Mason, J.I.; Sharpe, R.M. Steroidogenesis in the Fetal Testis and Its Susceptibility to Disruption by Exogenous Compounds. Endocr. Rev. 2009, 30, 883–925. [Google Scholar] [CrossRef] [PubMed]
- Piatkowski, T.; Whiteside, B.; Robertson, J.; Henning, A.; Lau, E.H.Y.; Dunn, M. What Is the Prevalence of Anabolic-Androgenic Steroid Use among Women? A Systematic Review. Addiction 2024, 119, 2088–2100. [Google Scholar] [CrossRef] [PubMed]
- Brinks, A.L.; Needle, C.D.; Spindler, A.J.; Brody, A.M.; Scandagli, I.; Oh, C.; Shapiro, J.; Lo Sicco, K.I.; Tawanwongsri, W. Alopecia in Female Athletes Using Androgenic and Anabolic Steroids: Pathophysiology and Management. Int. J. Dermatol. 2025. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Magnolini, R.; Kaeppeli, M.; Schori, D.; Bruggmann, P.; Senn, O. Evaluation of Implementing Drug Checking Services for Anabolic Androgenic Steroids in Switzerland: A Pilot Study. Harm Reduct. J. 2025, 22, 100. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Brain Region | Observed Effects | Implications |
|---|---|---|
| Hippocampus | Volume reduction, impaired neurogenesis | Memory deficits, cognitive dysfunction, impaired learning |
| Amygdala | Hypertrophy, altered neurotransmitter balance (serotonin, dopamine) | Increased aggression, emotional instability, heightened stress response |
| Prefrontal Cortex | Structural abnormalities, decreased activity in fMRI studies | Impaired impulse control, risky decision making, antisocial behaviors |
| Mechanism | Observed Effects | Implications |
|---|---|---|
| Oxidative Stress | Increased reactive oxygen species (ROS), reduced antioxidant defenses | Neuronal damage, accelerated neurodegeneration |
| Neuroinflammation | Chronic microglial activation, elevated cytokines | Synaptic dysfunction, cognitive decline, mood disorders |
| Neurotransmitter Imbalance | Disrupted dopamine, serotonin, and GABA signaling | Increased risk of addiction, mood disorders, and aggression |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chisari, M.G.; Esposito, M.; Alloca, S.; Franco, S.; Francaviglia, M.; Volonnino, G.; Rinaldi, R.; Di Fazio, N.; Di Mauro, L. Anabolic–Androgenic Steroids and Brain Damage: A Review of Evidence and Medico-Legal Implications. Forensic Sci. 2025, 5, 31. https://doi.org/10.3390/forensicsci5030031
Chisari MG, Esposito M, Alloca S, Franco S, Francaviglia M, Volonnino G, Rinaldi R, Di Fazio N, Di Mauro L. Anabolic–Androgenic Steroids and Brain Damage: A Review of Evidence and Medico-Legal Implications. Forensic Sciences. 2025; 5(3):31. https://doi.org/10.3390/forensicsci5030031
Chicago/Turabian StyleChisari, Mario Giuseppe, Massimiliano Esposito, Salvatore Alloca, Sabrina Franco, Martina Francaviglia, Gianpietro Volonnino, Raffaella Rinaldi, Nicola Di Fazio, and Lucio Di Mauro. 2025. "Anabolic–Androgenic Steroids and Brain Damage: A Review of Evidence and Medico-Legal Implications" Forensic Sciences 5, no. 3: 31. https://doi.org/10.3390/forensicsci5030031
APA StyleChisari, M. G., Esposito, M., Alloca, S., Franco, S., Francaviglia, M., Volonnino, G., Rinaldi, R., Di Fazio, N., & Di Mauro, L. (2025). Anabolic–Androgenic Steroids and Brain Damage: A Review of Evidence and Medico-Legal Implications. Forensic Sciences, 5(3), 31. https://doi.org/10.3390/forensicsci5030031