1. Introduction
Annually, approximately 33 per 100,000 infants are diagnosed with abusive head trauma (AHT), also known as Shaken baby syndrome (SBS), in hospitals within the United States [
1]. Infant AHT generally refers to conditions resulting with or without direct impact to the skull which leads to injuries within the cranium [
2]. The diagnosis of SBS is often based on signs such as subdural, subarachnoid, and retinal hemorrhages [
3]. While intentional shaking is widely recognized as a cause of these injuries, the potential for similar forces resulting from improper or accidental handling of infants has not been fully explored.
Contrary to the implications of the phrase “Shaken Baby Syndrome,” evidence shows that the act of shaking alone may not generate sufficient forces to cause the severe intracranial injuries typically associated with SBS. These studies involve infant models to prevent harm to an actual infant, and have reported that head accelerations during shaking generally peak around 8.5 G-force [
4]. In a another study, similar results of shaking a baby produced head accelerations of 10–15 G-forces [
5] and another producing mean peak head accelerations of 18.6 G-forces in the fore-aft direction [
6].
Because there is not a validated threshold of G-force that definitively cause infant head injuries, comparing magnitude of forces during different tasks allows for inference of potential trauma. Car safety experiments demonstrate 29.3 G-forces with simulated 18-mph car accidents and 5.2 G-forces in 5-mph bumper car collisions. These simulated collisions have adult dummies in car seats with the body in a semi-reclined position. This is similar to the position of infants during the head shaking tasks described above. However, other researchers have shown that impacts from babies falling over 1 m falls can result in head accelerations over 200 G-force [
7]. This much larger force may be generated both because of the supine position of the body, and the direct impact of the head with a surface, however is highly dependent upon the stiffness of the infant model used, as well as the rigidity of the surface that can alter the impulse.
While research has focused on head accelerations resulting from shaking or falls [
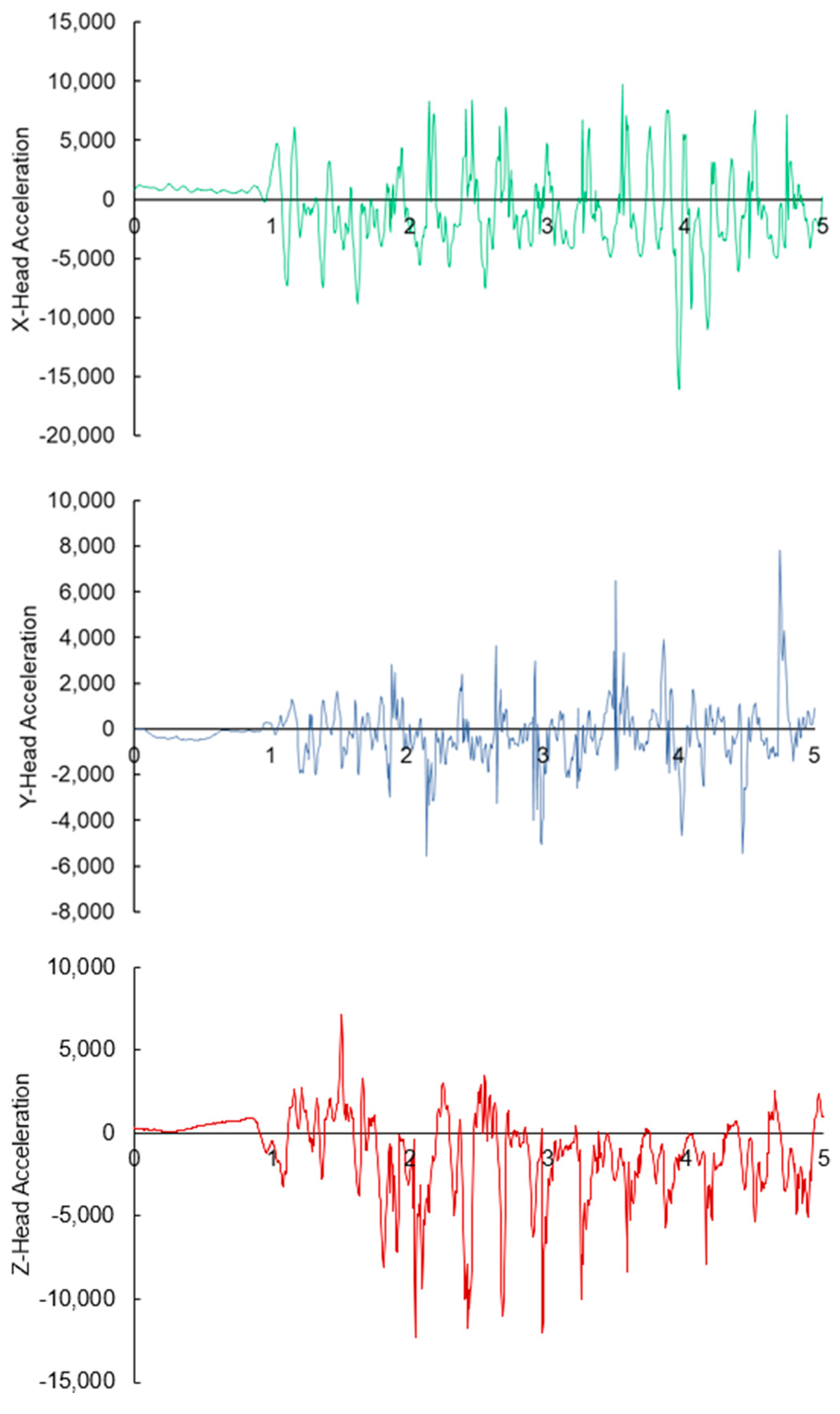
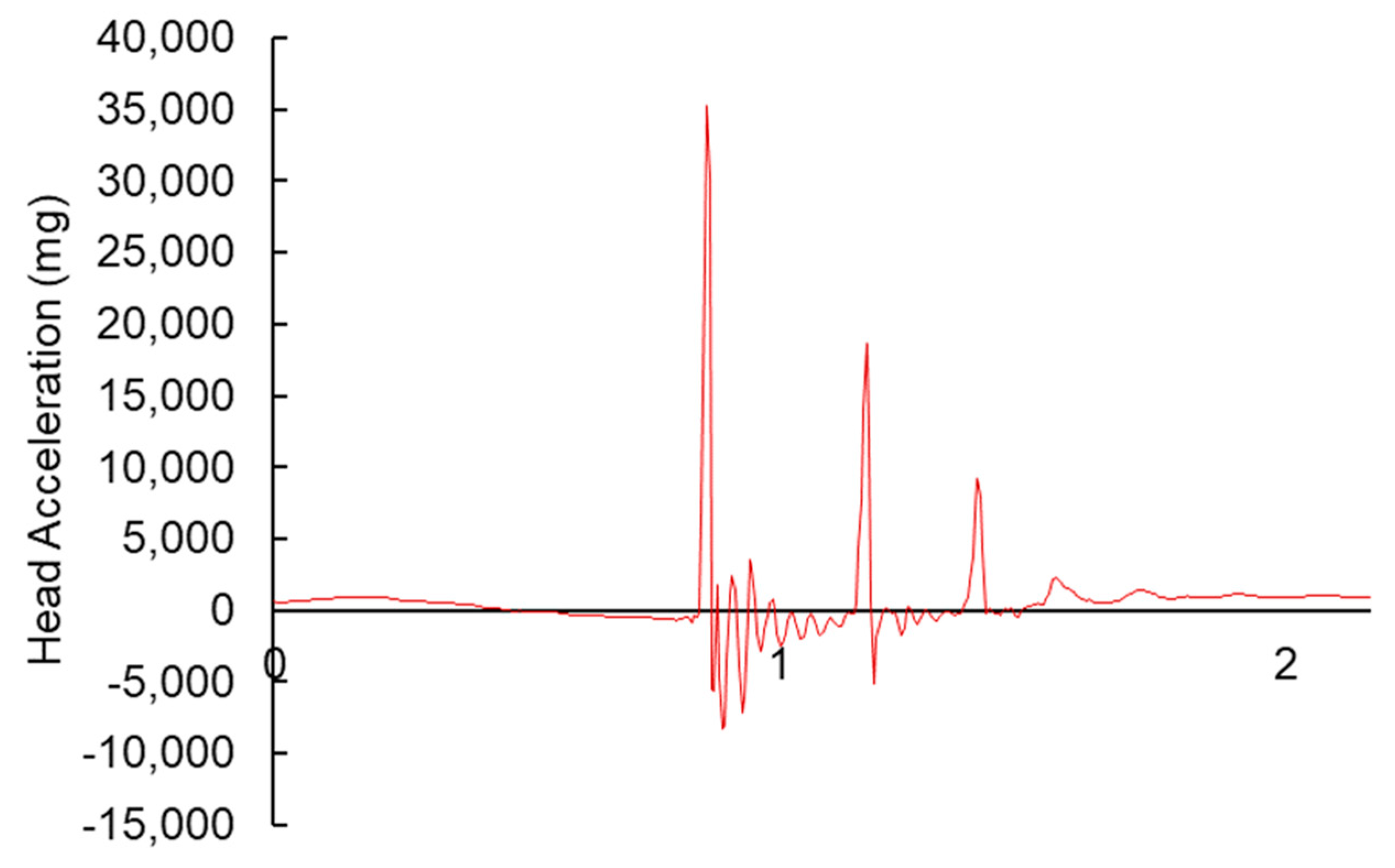
8], less attention has been given to other scenarios such as placing infants on hard surfaces without proper head support. The potential for such actions to produce high G-forces and cause trauma comparable to SBS remains poorly understood, especially in cases of accidental abusive head trauma. As such, the purpose of this study was to determine infant head G-forces in two conditions: (1) shaking a baby at maximum force, and (2) placing the infant on a table with the head unsupported. To ensure repeatability, we compared forces between two participants, and to identify whether differences in forces exist between placing on a table and forces identified in other studies during shaking, we compared forces during these tasks. We hypothesized that head accelerations would be significantly higher in placing an infant on a table with the head unsupported compared to shaking an infant at maximum force.
4. Discussion
Linear G-forces have been implicated in causing significant head injuries in infants, particularly in the context of abusive head trauma (AHT) [
9]. In this study, we hypothesized that improper handling, such as placing an infant on a table without head support, could generate G-forces comparable to or even exceeding those associated with intentional shaking. Our findings confirmed this hypothesis, demonstrating that peak head accelerations during unsupported placement of the infant model on a table were over 300% higher than those recorded during maximum exertion shaking. These results highlight that G-forces produced in everyday scenarios, such as placing an infant on a hard surface without supporting the head, can exceed those generated during violent shaking.
When compared to known magnitudes, the G-forces observed in this study bring a new perspective in understanding the biomechanical forces on SBS. The peak head acceleration from placing an infant model on the table exceeds the 29.3 G-forces experienced in an 18-mph car crash and exceed the 5.2 G-forces head accelerations recorded in a 5-mph bumper car collision [
10]. The results from these prior studies, and compared to the results of this current study, highlight the potential for significant head injury in scenarios lacking malicious intent or due to improper handling of infants.
Previous studies have raised concerns about the traditional diagnostic criteria for SBS [
11]. From a biomechanical perspective, the G-forces induced on shaking a baby to create intracranial damage would induce significant spinal cord damage rather than head injuries [
12,
13]. This inherently makes sense as the infant’s head is the heaviest segment of the infant body, and the weak neck muscles would be unable to control forces acting on the vertebrae and spinal cord. This raises concerns about the role of other forms of trauma, including those that may occur unintentionally, in producing similar intracranial damage. While the autopsy report in this case study reported intramuscular cervical hemorrhages, it is important to note that the cervical hemorrhages aren’t as severe as expected from actual shaking of a baby [
12]. It is plausible that an unsupported head while delivering back blows or placing the baby on the table with the head unsupported could have caused the intramuscular cervical hemorrhages given the high G-forces. Our findings suggest that it may be more appropriate to consider other forms of trauma, including those from unintentional mishandling, as contributing factors to head injuries in infants. The classic maximum exertion shaking was shown to produce 9–15 G-forces in prior work [
5]. The prior study used an infant model that was 3.18 kg. This was not similar to the size of the 5.08 kg infant model used in this study. Even with the mass discrepancy, this study’s results confirmed prior work showing that maximum exerted shaking of an infant produced approximately 11 G-Forces [
4,
5]. It is important to clarify, however, that similar acceleration values across studies using different infant model masses do not imply that acceleration remains constant across all body sizes during shaking. When the same amount of effort is applied to heavier infants, the resulting accelerations would generally be lower, not equal. Moreover, while this study focused on acceleration values, the force experienced upon impact (e.g., when the head strikes a surface) is directly proportional to mass. For a given deceleration, a more massive head would result in a proportionally greater impact force. Therefore, a real infant, especially one heavier than the model used in this study, may experience substantially greater forces during head impact, even if acceleration magnitudes are similar. This distinction is important when interpreting biomechanical outcomes across different infant sizes and highlights the need for future studies using size-scaled models and force measurements. With that in mind, the size of this model was smaller than the reported case. Since force is directly influenced by the mass of the object, a larger infant could experience even greater forces when placed on a table without head support. Furthermore, it is important to consider the improper handling of an infant as the head accelerations during the transfer of an infant to a table with the unsupported head resulted in 316% higher G-forces than maximum exertion of shaking an infant.
It is important to acknowledge that Shaken Baby Syndrome (SBS) injuries are multifactorial and often involve a combination of biomechanical forces beyond linear accelerations alone. Previous research has emphasized that rotational (angular) accelerations significantly contribute to the characteristic injuries observed in SBS, including subdural hemorrhage, retinal hemorrhage, and cerebral edema. Furthermore, spinal injuries or cervical trauma may occur due to the unique biomechanical interactions of shaking motions. The current study specifically quantified linear accelerations during certain non-recommended handling scenarios, but did not measure rotational accelerations or spinal forces. Therefore, while the high linear G-forces reported in this study demonstrate the potential for injury from isolated impacts, comprehensive diagnosis of SBS should consider all biomechanical components and associated clinical diagnostic criteria. As such, the current findings demonstrate that improper handling can produce head accelerations greater than those observed during maximum shaking, this study does not establish a direct causal relationship between these accelerations and specific injuries such as subdural or retinal hemorrhages. Injury determination requires consideration of tissue-level responses, injury thresholds, and validated models, none of which were within the scope of this preliminary investigation. Therefore, our results should be interpreted as highlighting the potential for elevated head loading, rather than as definitive evidence of traumatic injury from improper handling alone.
Several methodological limitations must be recognized in interpreting these findings. First, this study utilized a single silicone infant surrogate, which inherently does not fully replicate the biomechanical properties of human infants. Silicone models differ significantly in tissue elasticity, skull compliance, cerebrospinal fluid distribution, and internal anatomical complexity compared to a living infant. Such discrepancies may influence the measured head accelerations and limit direct clinical generalizations. The selection of this surrogate was based on ethical considerations prohibiting the use of live infants and practical constraints associated with more sophisticated anthropomorphic test devices (ATDs). Second, the small sample size of only two participants without prior infant-handling experience, further limits the generalizability of our results and introduces potential inter-operator variability. Although participants were trained briefly to standardize handling, individual differences in technique likely persisted. Third, although the Head Injury Criterion (HIC) is a widely accepted metric for estimating head injury risk in adult populations, this study did not compute HIC values due to the sampling frequency limitations of the inertial measurement unit (200 Hz). Accurate HIC calculation requires high-resolution acceleration data—typically ≥1000 Hz—to capture the rapid dynamics of head impacts. Future investigations should employ higher-frequency data acquisition systems to enable valid computation of HIC and support the development of age-specific injury risk curves for infants. Fourth, while this study reports peak linear accelerations as a first-order estimate of head loading, we acknowledge that peak acceleration alone is an imperfect predictor of injury. More advanced biomechanical models, including stress–strain analyses and finite element simulations, offer greater insight into tissue-level deformations and injury mechanisms, particularly for bridging veins and subdural spaces. Future studies should incorporate such models to improve understanding of how mechanical loading translates to specific intracranial injuries. Our current findings highlight relative differences in mechanical input across scenarios but do not represent a comprehensive biomechanical injury prediction framework. Furthermore, future studies should consider using more physiologically accurate ATDs, computational models validated against pediatric biomechanical data, and larger participant pools with varied infant-handling expertise to enhance validity and applicability of results.
While the medical reports concluded that this was a case of infant homicide, it may be important to understand that blunt trauma may also stem from improper handling which can result in accidental trauma and high amounts of head acceleration in infants. Consideration of the entire medical incident is important to help determine whether the blunt trauma was accidental or intention. In this case study, the father’s account of the incident suggests unintentional harm may have occurred. This father found his infant in medical distress and possibly choking. The emotional stress and trauma of this on the parent could have caused him to handle his infant with the dire intention of reviving and seeking medical attention. The mechanical data from this study demonstrated that such scenarios with no malicious intent can still pose a severe risk to an infant. This study highlights the importance of supporting an infant’s head during handling to prevent accidental injury, and further highlights that SBS warrants additional context of the situation before ascribing malintent on a caregiver.





{kind=link}
{kind=link}
{kind=link}