

Post-COVID-19 Era Forensics: Hospital Autopsies, New Methodologies, and Medicolegal Perspectives

 ,
,  ,
,  , and
, and
Abstract
1. Introduction
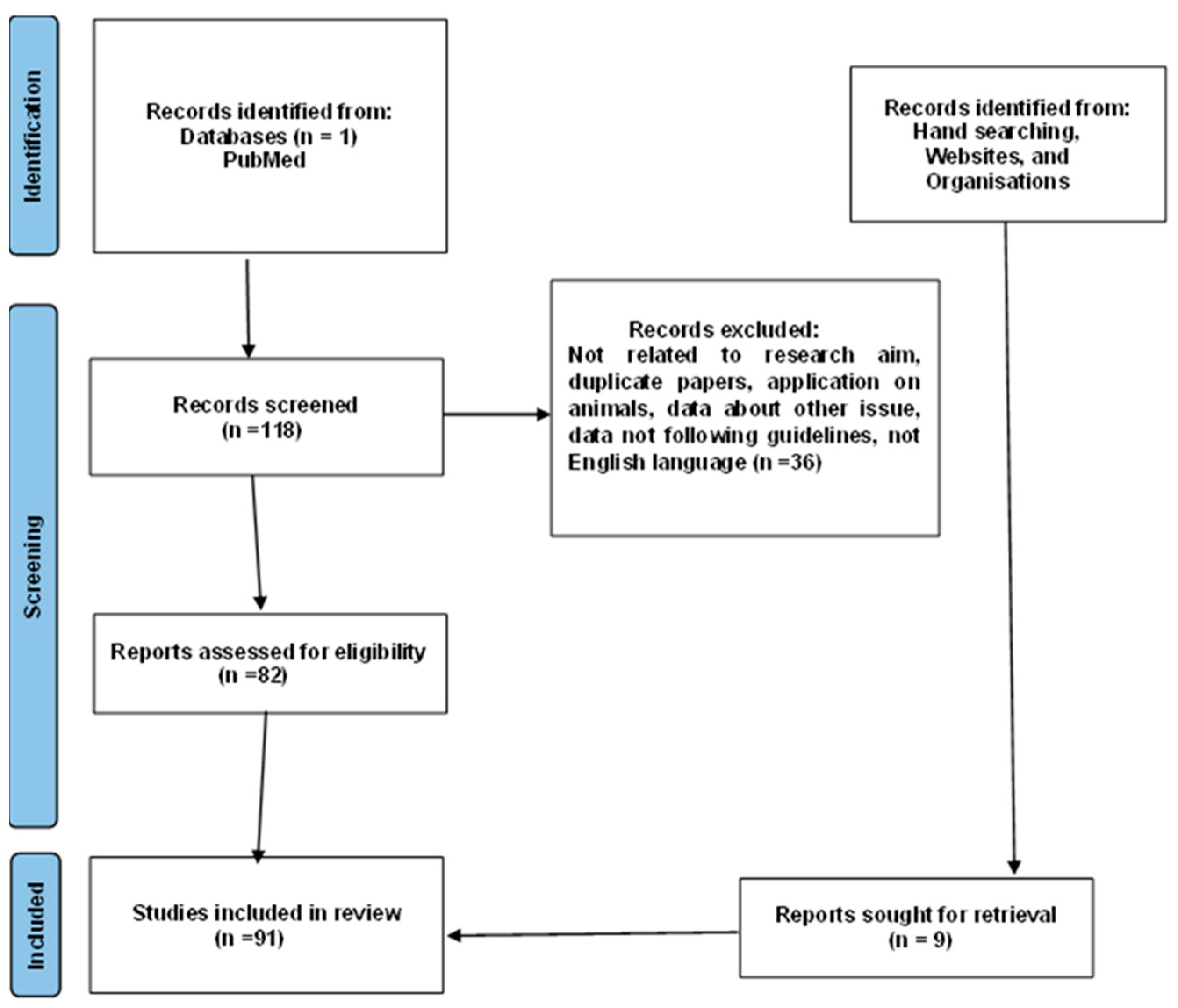
2. Materials and Methods
3. Results
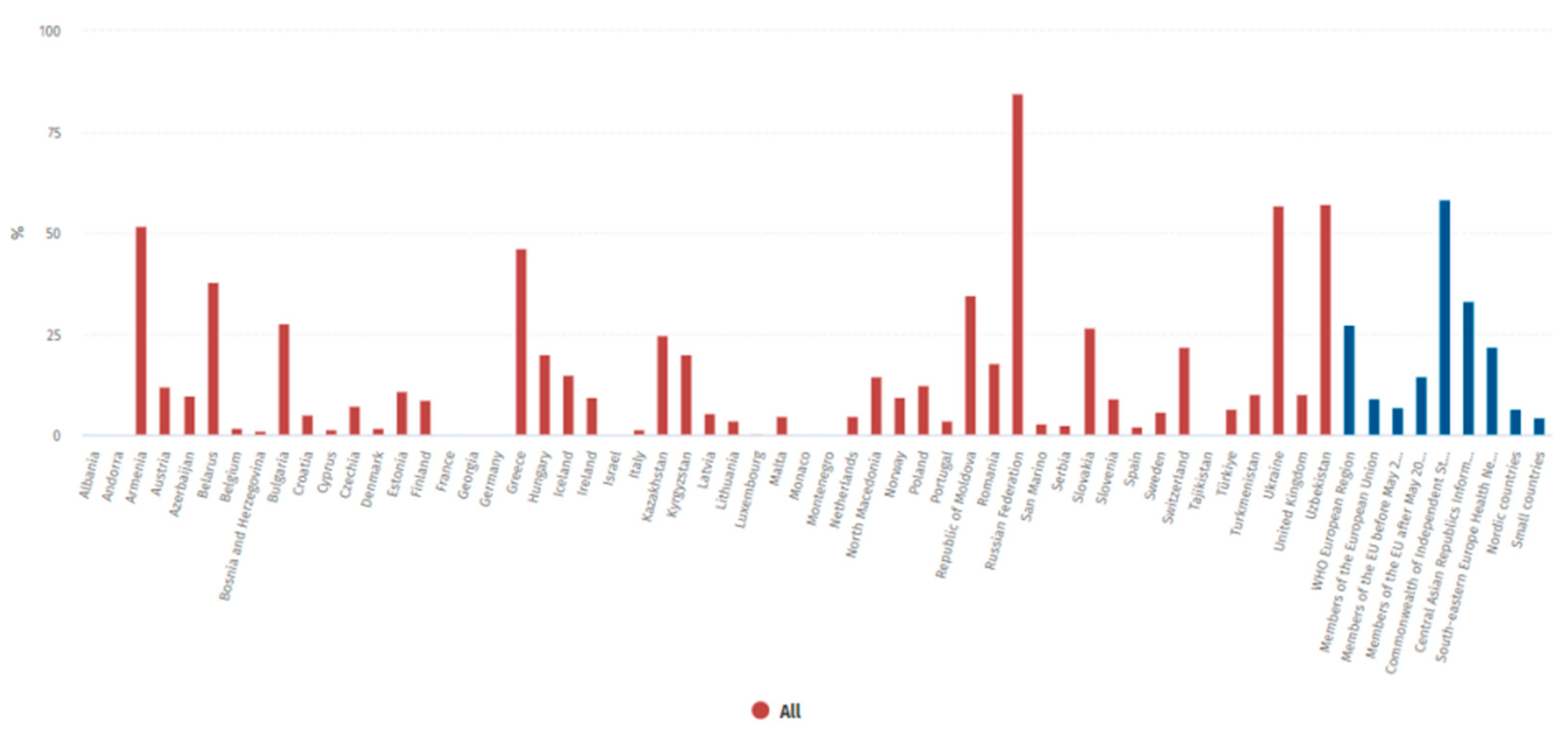
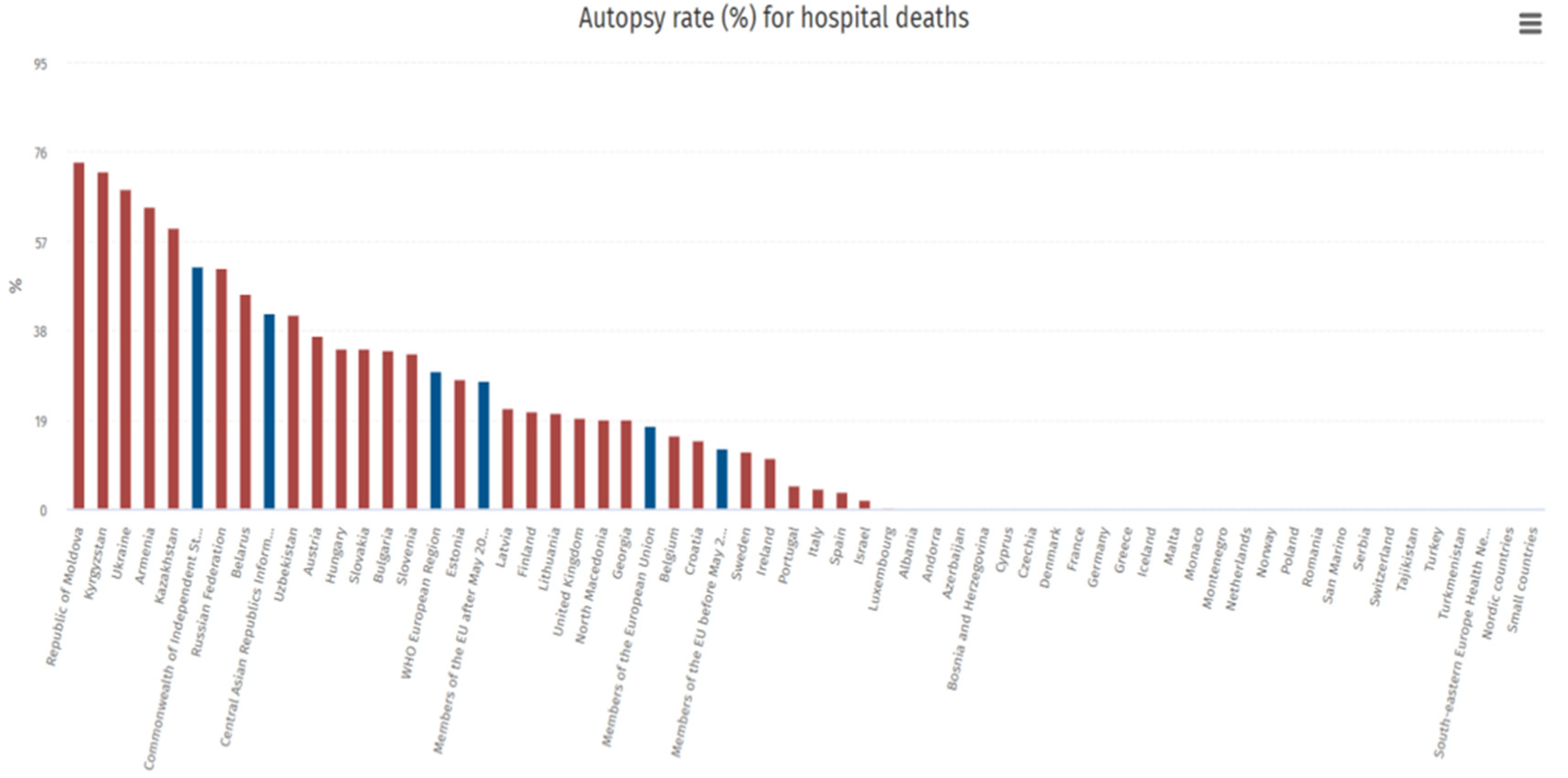
3.1. Autopsy Rates Are Constantly Declining in Western Countries
3.2. The Issue of Family Consent: Differences Between Countries
3.3. COVID-19 and Autopsies in Italy
- Judicial (local jurisdiction);
- Hospitals (organization by company);
- Checks on deceased subjects with no healthcare coverage (local health authority).
3.4. Forensic Doctors and Hospital Autopsies: Europe vs. USA

{kind=link}
{kind=link}
{kind=link}
| Country | Pathology | Forensic Pathology |
|---|---|---|
| Accreditation Council for Graduate Medical Education (United States) [70] | A minimum of 50 autopsy cases including exposure to forensic, pediatric, perinatal, and stillborn autopsies. | A minimum of 200 and no more than 300 autopsy cases |
| Royal College of Physicians and Surgeons of Canada [71] | No minimum number of autopsy cases. Accredited programs must have a volume and diversity of work available for teaching that must be adequate to meet the educational objectives of the program, with an adequate number of adult, pediatric, and forensic autopsies. | A minimum of 100 completed medicolegal post-mortem examinations including infant, children, and adult, with a wide range of natural and unnatural deaths, and 30% of the cases must be of a complex nature (homicides and criminally suspicious deaths) |
| The Royal College of Pathologists (United Kingdom) [72] | Stages A and B (2 years of basic histopathology training) requires 20 adult autopsy cases each year, with a total of two perinatal/pediatric autopsies. | Stage C (minimum of 30 months) requires 80 autopsy cases each year; Stage D (minimum of 6 months) requires 50 autopsy cases; also required to complete 3 months of pediatric pathology and 3 months of neuropathology |
| European Society of Pathology (E.S.P.) [1] | The autopsy should be coordinated by a specialist with proven experience and findings should only be performed by specialists in pathological anatomy or forensic pathology/forensics or possibly by specialists in training under direct supervision. Finally, to ensure adequate expertise, there is a minimum number of annual autopsies per individual team member, equal to at least 50 diagnostic findings and annual judicial autopsies. | The autopsy should be coordinated by a specialist with proven experience and findings should only be performed by specialists in pathological anatomy or forensic pathology/forensics or possibly by specialists in training under direct supervision. Finally, to ensure adequate expertise, there is a minimum number of annual autopsies per individual team member, equal to at least 50 diagnostic findings and annual judicial autopsies |
3.5. What Can Get in the Way of Hospital Autopsies? Does Family Consent Have Any Bearing?
- Infants who died suddenly within one year of life without apparent cause.
- Fetuses who died after the twenty-fifth week of gestation, also without apparent cause.
3.6. If Not Legal, What Reasons for Declining Autopsies? And What of the New Technologies?
3.7. COVID-19 and the Reasserted Value of Hospital Autopsies
4. Discussion
What Can Be Envisioned?
5. Conclusions
6. Limitations
Author Contributions
Funding
Conflicts of Interest
References
- Alfsen, G.C.; Gulczyński, J.; Kholová, I.; Latten, B.; Martinez, J.; Metzger, M.; Michaud, K.; Pontinha, C.M.; Rakislova, N.; Rotman, S.; et al. Code of Practice for Medical Autopsies: A Minimum Standard Position Paper for Pathology Departments Performing Medical (Hospital) Autopsies in Adults. Virchows Arch. 2022, 480, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Autopsy in the 21st Century: Best Practices and Future Directions [PDF] [7totf7fq9r40]. Available online: https://vdoc.pub/documents/autopsy-in-the-21st-century-best-practices-and-future-directions-7totf7fq9r40 (accessed on 13 December 2023).
- Zinserling, V. Infectious Pathology of the Respiratory Tract; Springer International Publishing: Cham, Switzerland, 2021; ISBN 978-3-030-66324-7. [Google Scholar]
- Napoletano, G.; Putrino, A.; Marinelli, E.; Zaami, S.; De Paola, L. Dental Identification System in Public Health: Innovations and Ethical Challenges: A Narrative Review. Healthcare 2024, 12, 1828. [Google Scholar] [CrossRef] [PubMed]
- Volonnino, G.; Paola, L.D.; Spadazzi, F.; Serri, F.; Ottaviani, M.; Zamponi, M.V.; Arcangeli, M.; Russa, R.L. Artificial intelligence and Forensic Medicine: The state of the art and future perspectives. Clin. Ter. 2024, 175, 193–202. [Google Scholar] [CrossRef] [PubMed]
- King, L.S.; Meehan, M.C. A History of the Autopsy. A Review. Am. J. Pathol. 1973, 73, 514–544. [Google Scholar]
- Cecchetto, G.; Bajanowski, T.; Cecchi, R.; Favretto, D.; Grabherr, S.; Ishikawa, T.; Kondo, T.; Montisci, M.; Pfeiffer, H.; Bonati, M.R.; et al. Back to the Future—Part 1. The Medico-Legal Autopsy from Ancient Civilization to the Post-Genomic Era. Int. J. Leg. Med. 2017, 131, 1069–1083. [Google Scholar] [CrossRef]
- Sakellariou, S.; Patsouris, E. Pathology in Greece. Pathologe 2015, 36 (Suppl. 2), 158–161. [Google Scholar] [CrossRef]
- Zampieri, F.; Zanatta, A.; Thiene, G. An Etymological “Autopsy” of Morgagni’s Title: De Sedibus et Causis Morborum per Anatomen Indagatis (1761). Hum. Pathol. 2014, 45, 12–16. [Google Scholar] [CrossRef]
- Participation, E. Anatomy Act. 1984. Available online: https://www.legislation.gov.uk/ukpga/1984/14/contents (accessed on 25 September 2024).
- Riggs, C. An Autopsic Art: Drawings of ‘Dr Granville’s Mummy’ in the Royal Society Archives. Notes Rec. R. Soc. J. Hist. Sci. 2016, 70, 107–133. [Google Scholar] [CrossRef]
- A Trusted Partner in Patient Care|The Joint Commission. Available online: https://www.jointcommission.org/ (accessed on 12 December 2023).
- Gitto, L.; Serinelli, S.; Busardò, F.P.; Panebianco, V.; Bolino, G.; Maiese, A. Can Post-Mortem Computed Tomography Be Considered an Alternative for Autopsy in Deaths Due to Hemopericardium? J. Geriatr. Cardiol. 2014, 11, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Hamza, A. Declining Rate of Autopsies: Implications for Anatomic Pathology Residents. Autops. Case Rep. 2017, 7, 1–2. [Google Scholar] [CrossRef]
- Rosendahl, A.; Mjörnheim, B.; Eriksson, L.C. Autopsies and Quality of Cause of Death Diagnoses. SAGE Open Med. 2021, 9, 20503121211037169. [Google Scholar] [CrossRef]
- Loughrey, M.B.; McCluggage, W.G.; Toner, P.G. The Declining Autopsy Rate and Clinicians’ Attitudes. Ulst. Med. J. 2000, 69, 83–89. [Google Scholar]
- WHO European Health Information at Your Fingertips. Available online: https://gateway.euro.who.int/en/indicators/hfa_544-6400-autopsy-rate-for-hospital-deaths/ (accessed on 13 December 2023).
- Chatelain, D.; Brevet, M.; Guernou, M.; Manaouil, C.; Leclercq, F.; Bruniau, A.; Cordonnier, C.; Sevestre, H. Adult autopsies in a French university hospital (CHU Amiens) for the period 1975–2005. Ann. Pathol. 2007, 27, 269–283. [Google Scholar] [CrossRef]
- Dell’Aquila, M.; Vetrugno, G.; Grassi, S.; Stigliano, E.; Oliva, A.; Rindi, G.; Arena, V. Postmodernism and the Decline of the Clinical Autopsy. Virchows Arch. 2021, 479, 861–863. [Google Scholar] [CrossRef] [PubMed]
- LOI No 94-653 Du 29 Juillet 1994 Relative Au Respect Du Corps Humain (1); 1994. Available online: https://affairesjuridiques.aphp.fr/textes/loi-n-94-653-du-29-juillet-1994-relative-au-respect-du-corps-humain/ (accessed on 25 October 2024).
- Krankenhausstrukturgesetz (KHSG). Available online: https://www.bundesgesundheitsministerium.de/service/gesetze-und-verordnungen/detail/krankenhausstrukturgesetz-khsg.html (accessed on 1 February 2025).
- Participation, E. Human Tissue Act. 2004. Available online: https://www.legislation.gov.uk/ukpga/2004/30/contents (accessed on 1 February 2025).
- BOE-A-1980-13662 Ley 29/1980, de 21 de Junio, de Autopsias Clínicas. Available online: https://www.boe.es/buscar/act.php?id=BOE-A-1980-13662 (accessed on 1 February 2025).
- Connolly, A.J.; Finkbeiner, W.E.; Ursell, P.C.; Davis, R.L. Legal, Social, and Ethical Issues. In Autopsy Pathology: A Manual and Atlas; Elsevier: Amsterdam, The Netherlands, 2016; pp. 15–23. [Google Scholar] [CrossRef]
- Tamsen, F.; Alafuzoff, I. When Is a Postmortem Examination Carried out? A Retrospective Analysis of All Swedish Deaths 1999–2018. Virchows Arch. 2023, 482, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.U.; Khan, M.S.; Navar, A.M.; Warraich, H.J.; Singh, J.; Cainzos-Achirica, M.; Michos, E.D. The Changing Profile of Autopsies in Cardiovascular Deaths in the United States, 2003–2018. Am. J. Cardiol. 2021, 140, 150–151. [Google Scholar] [CrossRef]
- Moretti, M.; Malhotra, A.; Visonà, S.D.; Finley, S.J.; Osculati, A.M.M.; Javan, G.T. The Roles of Medical Examiners in the COVID-19 Era: A Comparison between the United States and Italy. Forensic Sci. Med. Pathol. 2021, 17, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Basso, C.; Stone, J.R. Autopsy in the Era of Advanced Cardiovascular Imaging. Eur. Heart J. 2022, 43, 2461–2468. [Google Scholar] [CrossRef]
- Kircher, T.; Nelson, J.; Burdo, H. The Autopsy as a Measure of Accuracy of the Death Certificate. N. Engl. J. Med. 1985, 313, 1263–1269. [Google Scholar] [CrossRef]
- Landefeld, C.S.; Chren, M.M.; Myers, A.; Geller, R.; Robbins, S.; Goldman, L. Diagnostic Yield of the Autopsy in a University Hospital and a Community Hospital. N. Engl. J. Med. 1988, 318, 1249–1254. [Google Scholar] [CrossRef]
- Scarl, R.; Parkinson, B.; Arole, V.; Hardy, T.; Allenby, P. The Hospital Autopsy: The Importance in Keeping Autopsy an Option. Autops. Case Rep. 2022, 12, e2021333. [Google Scholar] [CrossRef]
- Goldman, L. Autopsy 2018: Still Necessary, Even If Occasionally Not Sufficient. Circulation 2018, 137, 2686–2688. [Google Scholar] [CrossRef] [PubMed]
- Sapino, A.; Facchetti, F.; Bonoldi, E.; Gianatti, A.; Barbareschi, M. Società Italiana di Anatomia Patologica e Citologia—SIAPEC The Autopsy Debate during the COVID-19 Emergency: The Italian Experience. Virchows Arch. 2020, 476, 821–823. [Google Scholar] [CrossRef] [PubMed]
- Download di: Circolare del Ministero della Salute n. 11392 del 1°. Aprile 2020. Available online: https://sso.agc.gov.sg/SL/HSA2020-S835-2023?DocDate=20231214 (accessed on 13 December 2023).
- Marozzi, F. Esami autoptici COVID-19: La posizione ufficiale di SIMLA e del GIPF. Società Italiana di Medicina Legale e delle Assicurazioni. 2020. Available online: https://www.simlaweb.it/esami-autoptici-covid19-la-posizione-ufficiale-di-simla-e-del-gipf/ (accessed on 13 December 2023).
- Emergency Circular n. 15280. Italian Ministry of Health 2nd May 2020. Available online: https://portale.fnomceo.it/wp-content/uploads/2020/05/Copia_DocPrincipale_Aggiornamento_Circolare_serv_funebri_28_5_2020.pdf (accessed on 26 September 2024).
- Circolare Ministero della Salute n. 18457 Del 28/05/2020. Available online: https://www.funerali.org/wp-content/uploads/File/Circolari/cs02005280.htm (accessed on 26 September 2024).
- Circolare (Ministero della Salute) 11-01-2021, n. 818|Indicenormativa.It. Available online: https://www.indicenormativa.it/norma/urn%3Anir%3Aministero.salute%3Acircolare%3A2021-01-11%3B818 (accessed on 13 December 2023).
- Riefolo, M.; Ambrosi, F.; De Palma, A.; Gallo, C.; Damiani, S. Management of Post-Mortem Examination in SARS-CoV-19 Infections. Pathologica 2023, 115, 257–262. [Google Scholar] [CrossRef]
- Hanley, B.; Lucas, S.B.; Youd, E.; Swift, B.; Osborn, M. Autopsy in Suspected COVID-19 Cases. J. Clin. Pathol. 2020, 73, 239–242. [Google Scholar] [CrossRef]
- Volonnino, G.; Spadazzi, F.; De Paola, L.; Arcangeli, M.; Pascale, N.; Frati, P.; La Russa, R. Healthcare Workers: Heroes or Victims? Context of the Western World and Proposals to Prevent Violence. Healthcare 2024, 12, 708. [Google Scholar] [CrossRef]
- Marinelli, S.; Basile, G.; Paola, L.D.E.; Napoletano, G.; Zaami, S. Consequences of COVID-19 Restrictions on Adolescent Mental Health and Drug Abuse Dynamics. Eur. Rev. Med. Pharmacol. Sci. 2024, 28, 836–851. [Google Scholar] [CrossRef]
- Wichmann, D.; Sperhake, J.-P.; Lütgehetmann, M.; Steurer, S.; Edler, C.; Heinemann, A.; Heinrich, F.; Mushumba, H.; Kniep, I.; Schröder, A.S.; et al. Autopsy Findings and Venous Thromboembolism in Patients With COVID-19: A Prospective Cohort Study. Ann. Intern. Med. 2020, 173, 268–277. [Google Scholar] [CrossRef]
- Maiese, A.; Manetti, A.C.; La Russa, R.; Di Paolo, M.; Turillazzi, E.; Frati, P.; Fineschi, V. Autopsy Findings in COVID-19-Related Deaths: A Literature Review. Forensic Sci. Med. Pathol. 2021, 17, 279–296. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Macor, P.; Durigutto, P.; Mangogna, A.; Bussani, R.; De Maso, L.; D’Errico, S.; Zanon, M.; Pozzi, N.; Meroni, P.L.; Tedesco, F. Multiple-Organ Complement Deposition on Vascular Endothelium in COVID-19 Patients. Biomedicines 2021, 9, 1003. [Google Scholar] [CrossRef]
- Frisoni, P.; Neri, M.; D’Errico, S.; Alfieri, L.; Bonuccelli, D.; Cingolani, M.; Di Paolo, M.; Gaudio, R.M.; Lestani, M.; Marti, M.; et al. Cytokine Storm and Histopathological Findings in 60 Cases of COVID-19-Related Death: From Viral Load Research to Immunohistochemical Quantification of Major Players IL-1β, IL-6, IL-15 and TNF-α. Forensic Sci. Med. Pathol. 2022, 18, 4–19. [Google Scholar] [CrossRef]
- CDC Healthcare Workers. Available online: https://archive.cdc.gov/www_cdc_gov/coronavirus/2019-ncov/hcp/guidance-postmortem-specimens.html (accessed on 20 November 2024).
- Infection Prevention and Control for the Safe Management of a Dead Body in the Context of COVID-19: Interim Guidance. Available online: https://www.who.int/publications-detail-redirect/infection-prevention-and-control-for-the-safe-management-of-a-dead-body-in-the-context-of-covid-19-interim-guidance (accessed on 13 December 2023).
- Hoyert, D.L. The Changing Profile of Autopsied Deaths in the United States, 1972–2007; US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics: Washington, DC, USA, 2011; pp. 1–8. [Google Scholar]
- McGuire, A.R.; DeJoseph, M.E.; Gill, J.R. An Approach to Iatrogenic Deaths. Forensic Sci. Med. Pathol. 2016, 12, 68–80. [Google Scholar] [CrossRef]
- Zanon, M.; Valentinuz, E.; Montanaro, M.; Radaelli, D.; Manfredi, A.; Bonuccelli, D.; Martelloni, M.; D’Errico, S. Is Hospital Autopsy Auditing Suitable for Clinical Risk Manage Ment? Actualities and Perspectives of Auditing in the Autopsy Room Following Italian Law 24/2017 on Patient Safety. Curr. Pharm. Biotechnol. 2021, 22, 1964–1970. [Google Scholar] [CrossRef] [PubMed]
- Rueckert, J. Elimination of the Autopsy Requirement by CMS. N. Engl. J. Med. 2020, 382, 683–684. [Google Scholar] [CrossRef]
- Lee, L.A.; Stephens, L.S.; Fligner, C.L.; Posner, K.L.; Cheney, F.W.; Caplan, R.A.; Domino, K.B. Autopsy Utilization in Medicolegal Defense of Anesthesiologists. Anesthesiology 2011, 115, 713–717. [Google Scholar] [CrossRef]
- Gartland, R.M.; Myers, L.C.; Iorgulescu, J.B.; Nguyen, A.T.; Yu-Moe, C.W.; Falcone, B.; Mitchell, R.; Kachalia, A.; Mort, E. Body of Evidence: Do Autopsy Findings Impact Medical Malpractice Claim Outcomes? J. Patient Saf. 2021, 17, 576–582. [Google Scholar] [CrossRef]
- Ondruschka, B.; Baier, C.; Dreßler, J.; Höch, A.; Bernhard, M.; Kleber, C.; Buschmann, C. Additional emergency medical measures in trauma-associated cardiac arrest. Anaesthesist 2017, 66, 924–935. [Google Scholar] [CrossRef] [PubMed]
- Beardmore, S.; Adeley, J.; Brookes, A.; Robinson, C.; Davendralingam, N.; Joseph, J.; McManoman, B.; Morgan, B. Impact of Changing from Autopsy to Post-Mortem CT in an Entire HM Coroner Region Due to a Shortage of Available Pathologists. Clin. Radiol. 2023, 78, 797–803. [Google Scholar] [CrossRef]
- Frati, P.; La Russa, R.; Duse, M. Editorial: Pediatric Specificities of Medical Liability: Improvement Measures in Pediatric Settings. Front. Pediatr. 2021, 9, 667020. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, M.C.; Reed, R.C. Pathologist Effort in the Performance of Fetal, Perinatal, and Pediatric Autopsies: A Survey of Practice. Arch. Pathol. Lab. Med. 2017, 141, 209–214. [Google Scholar] [CrossRef]
- Désilets, V.; Oligny, L.L.; Genetics Committee of the Society of Obstetricians and Gynaecology Canada; Family Physicians Advisory Committee. Medico–Legal Committee of the SOGC Fetal and Perinatal Autopsy in Prenatally Diagnosed Fetal Abnormalities with Normal Karyotype. J. Obstet. Gynaecol. Can. 2011, 33, 1047–1057. [Google Scholar] [CrossRef]
- Chowaniec, C.; Chowaniec, M.; Nowak, A.; Kobek, M. Sudden cardiac death—difficulties in passing a medico-legal opinion for a civil or insurance claim. Arch. Med. Sadowej Kryminol. 2007, 57, 72–77. [Google Scholar] [PubMed]
- Michaud, K.; Mangin, P.; Elger, B.S. Genetic Analysis of Sudden Cardiac Death Victims: A Survey of Current Forensic Autopsy Practices. Int. J. Leg. Med. 2011, 125, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Elger, B.; Michaud, K.; Mangin, P. When Information Can Save Lives: The Duty to Warn Relatives about Sudden Cardiac Death and Environmental Risks. Hastings Cent. Rep. 2010, 40, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Baiardi, S.; Rossi, M.; Capellari, S.; Parchi, P. Recent Advances in the Histo-Molecular Pathology of Human Prion Disease. Brain Pathol. 2019, 29, 278–300. [Google Scholar] [CrossRef] [PubMed]
- Rapkiewicz, A.V.; Mai, X.; Carsons, S.E.; Pittaluga, S.; Kleiner, D.E.; Berger, J.S.; Thomas, S.; Adler, N.M.; Charytan, D.M.; Gasmi, B.; et al. Megakaryocytes and Platelet-Fibrin Thrombi Characterize Multi-Organ Thrombosis at Autopsy in COVID-19: A Case Series. eClinicalMedicine 2020, 24, 100434. [Google Scholar] [CrossRef]
- Farshad, S.; Kanaan, C.; Savedchuk, S.; Karmo, D.S.; Halalau, A.; Swami, A. Systemic Lupus Erythematosus (SLE) with Acute Nephritis, Antineutrophil Cytoplasmic Antibody- (ANCA-) Associated Vasculitis, and Thrombotic Thrombocytopenic Purpura (TTP): A Rare Case Report with Literature Review. Case Rep. Rheumatol. 2019, 2019, 8750306. [Google Scholar] [CrossRef]
- Hammer, U.; Blaas, V.; Büttner, A.; Philipp, M. Autopsies for anatomical teaching and training in clinical forensic medicine. Chirurg 2015, 86, 1128–1131. [Google Scholar] [CrossRef]
- Hamilton, L.E. Teaching the Forensic Autopsy. Acad. Forensic Pathol. 2015, 5, 201–210. [Google Scholar] [CrossRef]
- Khalaf, Z.; Hamidpour, S. Adaptations of Pathology Residencies During COVID-19. Mo. Med. 2023, 120, 192–195. [Google Scholar]
- Accreditation Council for Graduate Medical Education. Available online: https://www.acgme.org (accessed on 26 September 2024).
- Royal College of Physicians and Surgeons of Canada. Forensic Pathology Training Experiences. Issued in May 2019. Available online: https://lmp.utoronto.ca/royal-college-physicians-and-surgeons-canada-academic-certification-program (accessed on 26 September 2024).
- Pathologists, T.R.C. of Autopsy Guidelines Series. Available online: https://www.rcpath.org/profession/guidelines/autopsy-guidelines-series.html (accessed on 26 September 2024).
- Schwanda-Burger, S.; Moch, H.; Muntwyler, J.; Salomon, F. Diagnostic Errors in the New Millennium: A Follow-up Autopsy Study. Mod. Pathol. 2012, 25, 777–783. [Google Scholar] [CrossRef]
- Roberts, I.S.D.; Benbow, E.W.; Bisset, R.; Jenkins, J.P.R.; Lee, S.H.; Reid, H.; Jackson, A. Accuracy of Magnetic Resonance Imaging in Determining Cause of Sudden Death in Adults: Comparison with Conventional Autopsy. Histopathology 2003, 42, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Buja, L.M.; Barth, R.F.; Krueger, G.R.; Brodsky, S.V.; Hunter, R.L. The Importance of the Autopsy in Medicine: Perspectives of Pathology Colleagues. Acad. Pathol. 2019, 6, 2374289519834041. [Google Scholar] [CrossRef]
- Maiese, A.; Gitto, L.; De Matteis, A.; Panebianco, V.; Bolino, G. Post Mortem Computed Tomography: Useful or Unnecessary in Gunshot Wounds Deaths? Two Case Reports. Leg. Med. 2014, 16, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Robb, T.J.; Tse, R.; Blenkiron, C. Reviving the Autopsy for Modern Cancer Evolution Research. Cancers 2021, 13, 409. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, A.; Osborn, M.; Nicholas, N. Hospital Autopsy: Endangered or Extinct? J. Clin. Pathol. 2015, 68, 601–604. [Google Scholar] [CrossRef]
- Weber, M.-A. Minimally invasive autopsy: An alternative to conventional autopsy? Radiologe 2009, 49, 397–398. [Google Scholar] [CrossRef] [PubMed]
- Fröhlich, S.; Ryan, O.; Murphy, N.; McCauley, N.; Crotty, T.; Ryan, D. Are Autopsy Findings Still Relevant to the Management of Critically Ill Patients in the Modern Era? Crit. Care Med. 2014, 42, 336–343. [Google Scholar] [CrossRef]
- Blokker, B.M.; Wagensveld, I.M.; Weustink, A.C.; Oosterhuis, J.W.; Hunink, M.G.M. Non-Invasive or Minimally Invasive Autopsy Compared to Conventional Autopsy of Suspected Natural Deaths in Adults: A Systematic Review. Eur. Radiol. 2016, 26, 1159–1179. [Google Scholar] [CrossRef] [PubMed]
- Das, A.; Chowdhury, R. Searching Cause of Death through Different Autopsy Methods: A New Initiative. J. Family Med. Prim. Care 2017, 6, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Di Paolo, M.; Maiese, A.; dell’Aquila, M.; Filomena, C.; Turco, S.; Giaconi, C.; Turillazzi, E. Role of Post Mortem CT (PMCT) in High Energy Traumatic Deaths. Clin. Ter. 2020, 171, e490–e500. [Google Scholar] [CrossRef]
- Bailo, P.; Gibelli, F.; Ricci, G.; Sirignano, A. Verbal Autopsy as a Tool for Defining Causes of Death in Specific Healthcare Contexts: Study of Applicability through a Traditional Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 11749. [Google Scholar] [CrossRef] [PubMed]
- Fiksel, J.; Gilbert, B.; Wilson, E.; Kalter, H.; Kante, A.; Akum, A.; Blau, D.; Bassat, Q.; Macicame, I.; Samo Gudo, E.; et al. Correcting for Verbal Autopsy Misclassification Bias in Cause-Specific Mortality Estimates. Am. J. Trop. Med. Hyg. 2023, 108, 66–77. [Google Scholar] [CrossRef] [PubMed]
- Rosen, T.; Safford, M.M.; Sterling, M.R.; Goyal, P.; Patterson, M.; Al Malouf, C.; Ballin, M.; Del Carmen, T.; LoFaso, V.M.; Raik, B.L.; et al. Development of the Verbal Autopsy Instrument for COVID-19 (VAIC). J. Gen. Intern. Med. 2021, 36, 3522–3529. [Google Scholar] [CrossRef]
- Kniep, I.; Lutter, M.; Ron, A.; Edler, C.; Püschel, K.; Ittrich, H.; Heller, M.; Heinemann, A. Postmortem imaging of the lung in cases of COVID-19 deaths. Radiologe 2020, 60, 927–933. [Google Scholar] [CrossRef] [PubMed]
- Kanchan, T.; Saraf, A.; Krishan, K.; Misra, S. The Advantages of Virtopsy during the Covid-19 Pandemic. Med. Leg. J. 2020, 88, 55–56. [Google Scholar] [CrossRef] [PubMed]
- Filograna, L.; Manenti, G.; Ampanozi, G.; Calcagni, A.; Ryan, C.P.; Floris, R.; Thali, M.J. Potentials of Post-Mortem CT Investigations during SARS-COV-2 Pandemic: A Narrative Review. Radiol. Med. 2022, 127, 383–390. [Google Scholar] [CrossRef]
- Huang, S.; Yang, J.; Fong, S.; Zhao, Q. Artificial Intelligence in the Diagnosis of COVID-19: Challenges and Perspectives. Int. J. Biol. Sci. 2021, 17, 1581–1587. [Google Scholar] [CrossRef] [PubMed]
- Zaeri, N. Artificial Intelligence and Machine Learning Responses to COVID-19 Related Inquiries. J. Med. Eng. Technol. 2023, 47, 301–320. [Google Scholar] [CrossRef]
- Frati, P.; Frati, A.; Salvati, M.; Marinozzi, S.; Frati, R.; Angeletti, L.R.; Piccirilli, M.; Gaudio, E.; Delfini, R. Neuroanatomy and Cadaver Dissection in Italy: History, Medicolegal Issues, and Neurosurgical Perspectives. J. Neurosurg. 2006, 105, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Karch, S.B.; Busardò, F.P.; Vaiano, F.; Portelli, F.; Zaami, S.; Bertol, E. Levamisole Adulterated Cocaine and Pulmonary Vasculitis: Presentation of Two Lethal Cases and Brief Literature Review. Forensic Sci. Int. 2016, 265, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Piersanti, V.; Napoletano, G.; David, M.C.; Umani Ronchi, F.; Marinelli, E.; De Paola, L.; Zaami, S. Sudden Death Due to Butane Abuse—An Overview. J. Forensic Leg. Med. 2024, 103, 102662. [Google Scholar] [CrossRef]
- Baggio, U.; Tortorella, V.; De Paola, L.; Berloco, T.; D’Antonio, G.; Mangiulli, T. A Rare Case of Suicide by Bleach Fatal Ingestion: A Case Report and a Literature Overview. Clin. Ter. 2024, 175, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Sperhake, J.-P. Autopsies of COVID-19 Deceased? Absolutely! Leg. Med. 2020, 47, 101769. [Google Scholar] [CrossRef] [PubMed]
- Scendoni, R.; Cingolani, M. What Do We Know about Pathological Mechanism and Pattern of Lung Injury Related to SARS-CoV-2 Omicron Variant? Diagn. Pathol. 2023, 18, 18. [Google Scholar] [CrossRef] [PubMed]
- Hirata, Y.; Iida, S.; Arashiro, T.; Nagasawa, S.; Saitoh, H.; Abe, H.; Ikemura, M.; Makino, Y.; Sawa, R.; Iwase, H.; et al. Impact of the COVID-19 Pandemic on Pathological Autopsy Practices in Japan. Pathol. Int. 2023, 73, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Duarte-Neto, A.N.; Monteiro, R.A.A.; da Silva, L.F.F.; Malheiros, D.M.A.C.; de Oliveira, E.P.; Theodoro-Filho, J.; Pinho, J.R.R.; Gomes-Gouvêa, M.S.; Salles, A.P.M.; de Oliveira, I.R.S.; et al. Pulmonary and Systemic Involvement in COVID-19 Patients Assessed with Ultrasound-Guided Minimally Invasive Autopsy. Histopathology 2020, 77, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Benson, P.V.; Litovsky, S.H.; Steyn, A.J.C.; Margaroli, C.; Iriabho, E.; Anderson, P.G. Use of Telepathology to Facilitate COVID-19 Research and Education through an Online COVID-19 Autopsy Biorepository. J. Pathol. Inform. 2021, 12, 48. [Google Scholar] [CrossRef] [PubMed]
- Gareev, I.; Gallyametdinov, A.; Beylerli, O.; Valitov, E.; Alyshov, A.; Pavlov, V.; Izmailov, A.; Zhao, S. The opportunities and challenges of telemedicine during COVID-19 pandemic. Front. Biosci. (Elite Ed.) 2021, 13, 291–298. [Google Scholar] [CrossRef]
- Vidua, R.K.; Duskova, I.; Bhargava, D.C.; Chouksey, V.K.; Pramanik, P. Dead Body Management amidst Global Pandemic of Covid-19. Med. Leg. J. 2020, 88, 80–83. [Google Scholar] [CrossRef]
- De-Giorgio, F.; Grassi, V.M.; Bergamin, E.; Cina, A.; Del Nonno, F.; Colombo, D.; Nardacci, R.; Falasca, L.; Conte, C.; d’Aloja, E.; et al. Dying “from” or “with” COVID-19 during the Pandemic: Medico-Legal Issues According to a Population Perspective. Int. J. Environ. Res. Public Health 2021, 18, 8851. [Google Scholar] [CrossRef] [PubMed]
- Aquila, I.; Ricci, P.; Bonetta, C.F.; Sacco, M.A.; Longhini, F.; Torti, C.; Mazzitelli, M.; Garofalo, E.; Bruni, A.; Trecarichi, E.M.; et al. Analysis of the Persistence Time of the SARS-CoV-2 Virus in the Cadaver and the Risk of Passing Infection to Autopsy Staff. Med. Leg. J. 2021, 89, 40–53. [Google Scholar] [CrossRef]
- Parekh, U.; Chariot, P.; Dang, C.; Stray-Pedersen, A.; Druid, H.; Sajantila, A. A Roadmap to the Safe Practice of Forensic Medicine in the COVID-19 Pandemic. J. Forensic Leg. Med. 2020, 76, 102036. [Google Scholar] [CrossRef] [PubMed]
- Edler, C.; Schröder, A.S.; Aepfelbacher, M.; Fitzek, A.; Heinemann, A.; Heinrich, F.; Klein, A.; Langenwalder, F.; Lütgehetmann, M.; Meißner, K.; et al. Dying with SARS-CoV-2 Infection-an Autopsy Study of the First Consecutive 80 Cases in Hamburg, Germany. Int. J. Leg. Med. 2020, 134, 1275–1284. [Google Scholar] [CrossRef] [PubMed]
- Geller, R.L.; Aungst, J.L.; Newton-Levinson, A.; Smith, G.P.; Mosunjac, M.B.; Mosunjac, M.I.; Cunningham, C.S.; Gowitt, G.T. Is It COVID-19? The Value of Medicolegal Autopsies during the First Year of the COVID-19 Pandemic. Forensic Sci. Int. 2022, 330, 111106. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.S.; Dmetrichuk, J.M.; Kim, P.; Pollanen, M.S. Postmortem Radiologic and Pathologic Findings in COVID-19: The Toronto Experience with Pre-Hospitalization Deaths in the Community. Forensic Sci. Int. 2021, 322, 110755. [Google Scholar] [CrossRef]
- Waidhauser, J.; Martin, B.; Trepel, M.; Märkl, B. Can Low Autopsy Rates Be Increased? Yes, We Can! Should Postmortem Examinations in Oncology Be Performed? Yes, We Should! A Postmortem Analysis of Oncological Cases. Virchows Arch. 2021, 478, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Schädler, J.; Azeke, A.T.; Ondruschka, B.; Steurer, S.; Lütgehetmann, M.; Fitzek, A.; Möbius, D. Concordance between MITS and Conventional Autopsies for Pathological and Virological Diagnoses. Int. J. Leg. Med. 2024, 138, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Meinhardt, J.; Streit, S.; Dittmayer, C.; Manitius, R.V.; Radbruch, H.; Heppner, F.L. The Neurobiology of SARS-CoV-2 Infection. Nat. Rev. Neurosci. 2024, 25, 30–42. [Google Scholar] [CrossRef] [PubMed]
- Cao, W. Autopsy Education and Rate: Effect of the COVID-19 Pandemic. Rhode Isl. Med. J. 2021, 104, 21–25. [Google Scholar]
- Latten, B.G.H.; Kubat, B.; van den Brandt, P.A.; Zur Hausen, A.; Schouten, L.J. Cause of Death and the Autopsy Rate in an Elderly Population. Virchows Arch. 2023, 483, 865–872. [Google Scholar] [CrossRef]
- Heinrich, F.; Mertz, K.D.; Glatzel, M.; Beer, M.; Krasemann, S. Using Autopsies to Dissect COVID-19 Pathogenesis. Nat. Microbiol. 2023, 8, 1986–1994. [Google Scholar] [CrossRef]
- Burton, J.L.; Underwood, J. Clinical, Educational, and Epidemiological Value of Autopsy. Lancet 2007, 369, 1471–1480. [Google Scholar] [CrossRef] [PubMed]
- Del Duca, F.; Manetti, A.C.; Maiese, A.; Napoletano, G.; Ghamlouch, A.; Pascale, N.; Giorgio, B.; Paola, F.; Russa, R.L. Death Due to Anaphylactic Reaction: The Role of the Forensic Pathologist in an Accurate Postmortem Diagnosis. Medicina 2023, 59, 2184. [Google Scholar] [CrossRef] [PubMed]
- Crouch, E.E.; Damas, C.; Bartrug, W.C.; Shamiyeh, A.; Scelfo, M.; Dreyfus, M.; Gano, D.; Segal, S.; Franck, L.S. Parents’ Views on Autopsy, Organ Donation, and Research Donation After Neonatal Death. JAMA Netw. Open 2023, 6, e2341533. [Google Scholar] [CrossRef]
| Regulation | Issuing Institution | Release Date | Most Relevant Indications |
|---|---|---|---|
| Circular no. 11392 [34] | Ministry of Health | 1 April 2020 | During the emergency phase, autopsies and diagnostic tests should not be conducted on confirmed COVID-19 cases, regardless of whether death occurred in the hospital or at home. |
| SIMLA letter to the Minister of Health [35] | Italian Society of Forensic Medicine | 4 April 2020 (signed by President Prof. Zoja and the Secretary-General Prof. Di Mauro). | A request is made to restructure and adapt autopsy rooms nationwide to meet BSL-3 standards or, at a minimum, to upgrade at least one autopsy room in each provincial capital municipality to comply with the essential technical requirements. |
| Emergency Circular no. 15280 [36] | Italian Ministry of Health | 2 May 2020 | Throughout the emergency phase, autopsies and diagnostic tests must not be performed on confirmed COVID-19 cases, irrespective of whether death occurred in a hospital ward or at home. |
| Circular no. 18457 [37] | Ministry of Health | 28 May 2020. | Previously issued Ministerial Circulars did not aim to prohibit autopsies but only recommended limiting them to safeguard the health of healthcare workers and auxiliary personnel. |
| SIMLA/Italian Society of Forensic Pathologists (GIPF) Communique [35] | Italian Society of Forensic Medicine, signed by Prof. C. Campobasso and G Di Vella | 4 June 2020 | The lack of anatomical biocontainment rooms required to ensure the proper execution of autopsy activities across the country, as well as the safety of healthcare professionals and mortuary staff, represents a critical issue that must be addressed. |
| Circular no. 818 [38] | Ministry of Health | 11 January 2021 | The document no longer includes language “advising against” the execution of autopsies on COVID-19 subjects, effectively lifting the previous restrictions on conducting clinical-forensic autopsy examinations. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaami, S.; Napoletano, G.; Marinelli, E.; Sablone, S.; De Paola, L.; Introna, F. Post-COVID-19 Era Forensics: Hospital Autopsies, New Methodologies, and Medicolegal Perspectives. Forensic Sci. 2025, 5, 8. https://doi.org/10.3390/forensicsci5010008
Zaami S, Napoletano G, Marinelli E, Sablone S, De Paola L, Introna F. Post-COVID-19 Era Forensics: Hospital Autopsies, New Methodologies, and Medicolegal Perspectives. Forensic Sciences. 2025; 5(1):8. https://doi.org/10.3390/forensicsci5010008
Chicago/Turabian StyleZaami, Simona, Gabriele Napoletano, Enrico Marinelli, Sara Sablone, Lina De Paola, and Francesco Introna. 2025. "Post-COVID-19 Era Forensics: Hospital Autopsies, New Methodologies, and Medicolegal Perspectives" Forensic Sciences 5, no. 1: 8. https://doi.org/10.3390/forensicsci5010008
APA StyleZaami, S., Napoletano, G., Marinelli, E., Sablone, S., De Paola, L., & Introna, F. (2025). Post-COVID-19 Era Forensics: Hospital Autopsies, New Methodologies, and Medicolegal Perspectives. Forensic Sciences, 5(1), 8. https://doi.org/10.3390/forensicsci5010008