
The Subadult Virtual Anthropology Database (SVAD): An Accessible Repository of Contemporary Subadult Reference Data


Abstract
:1. The Need for Contemporary Subadult Reference Samples
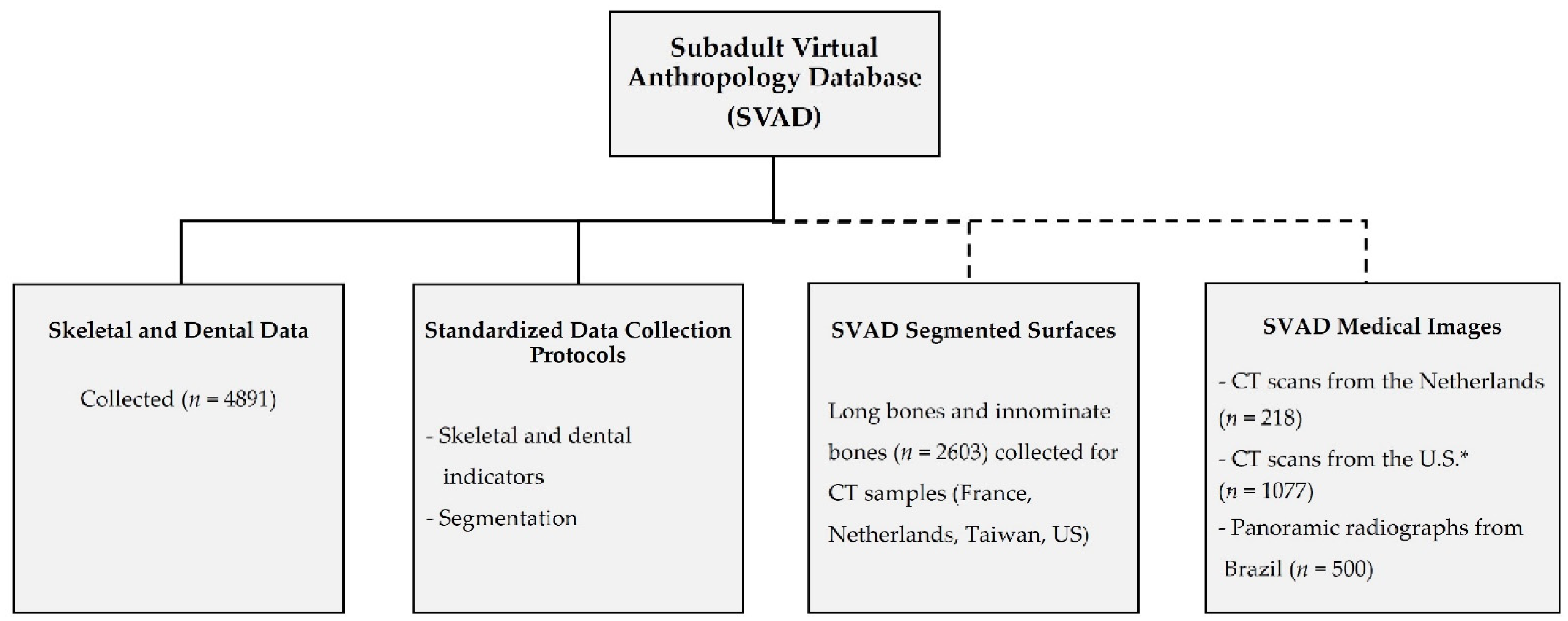
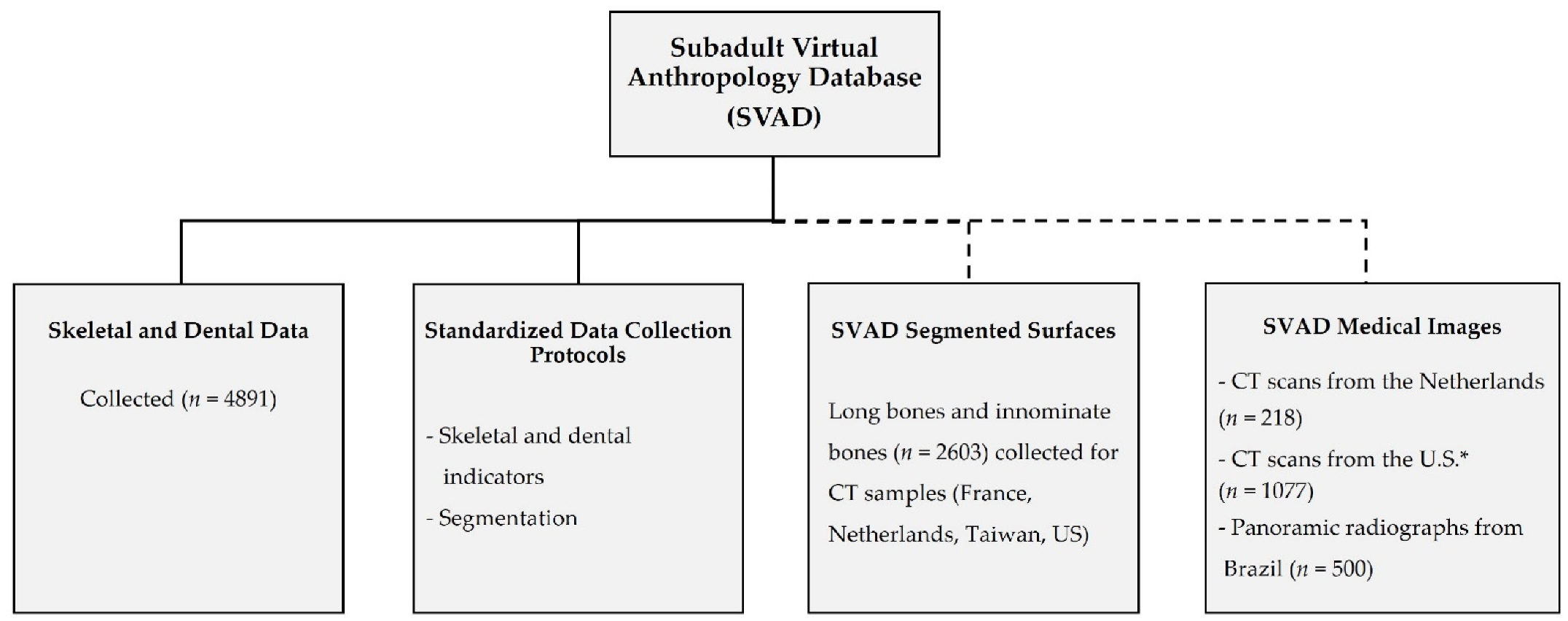
2. The SVAD
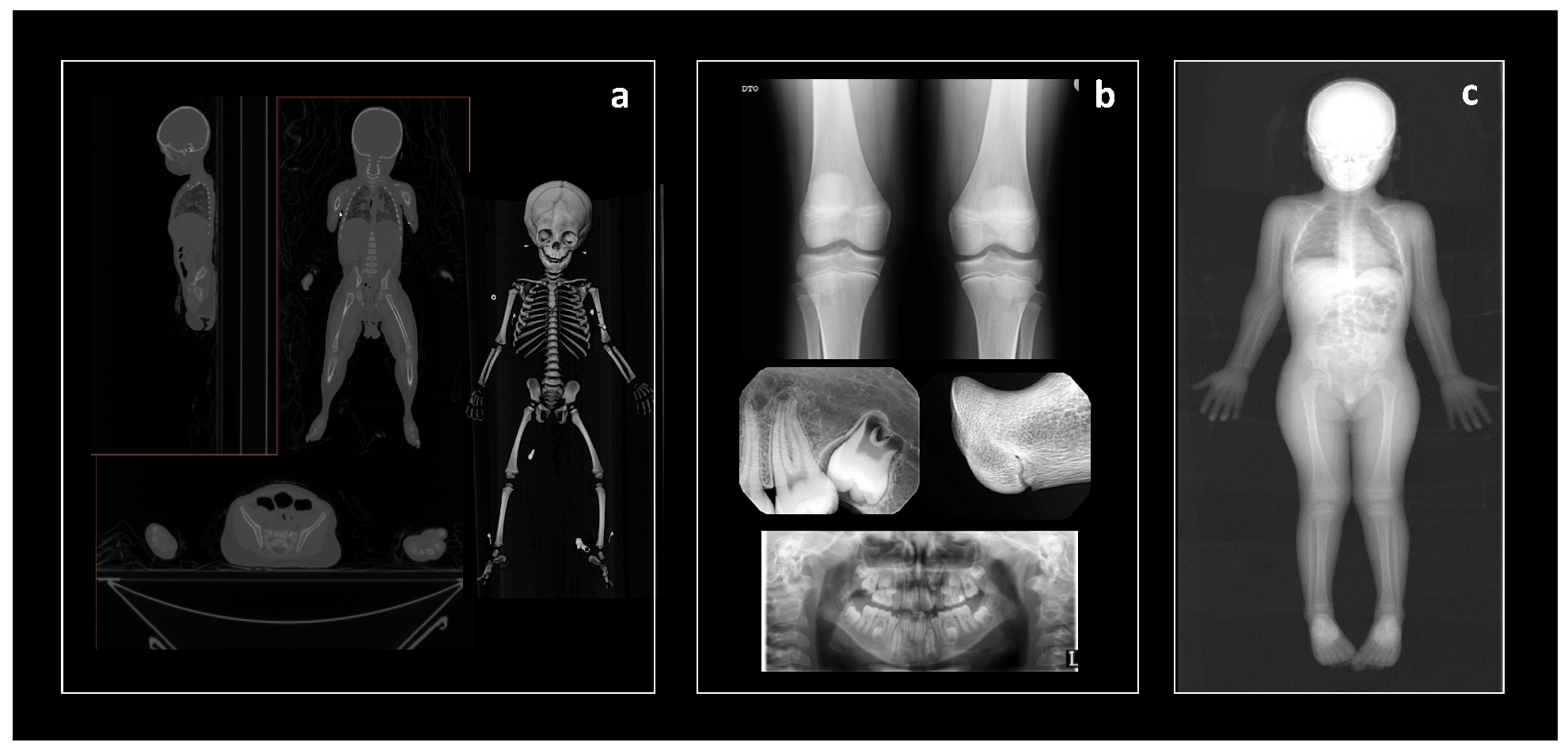
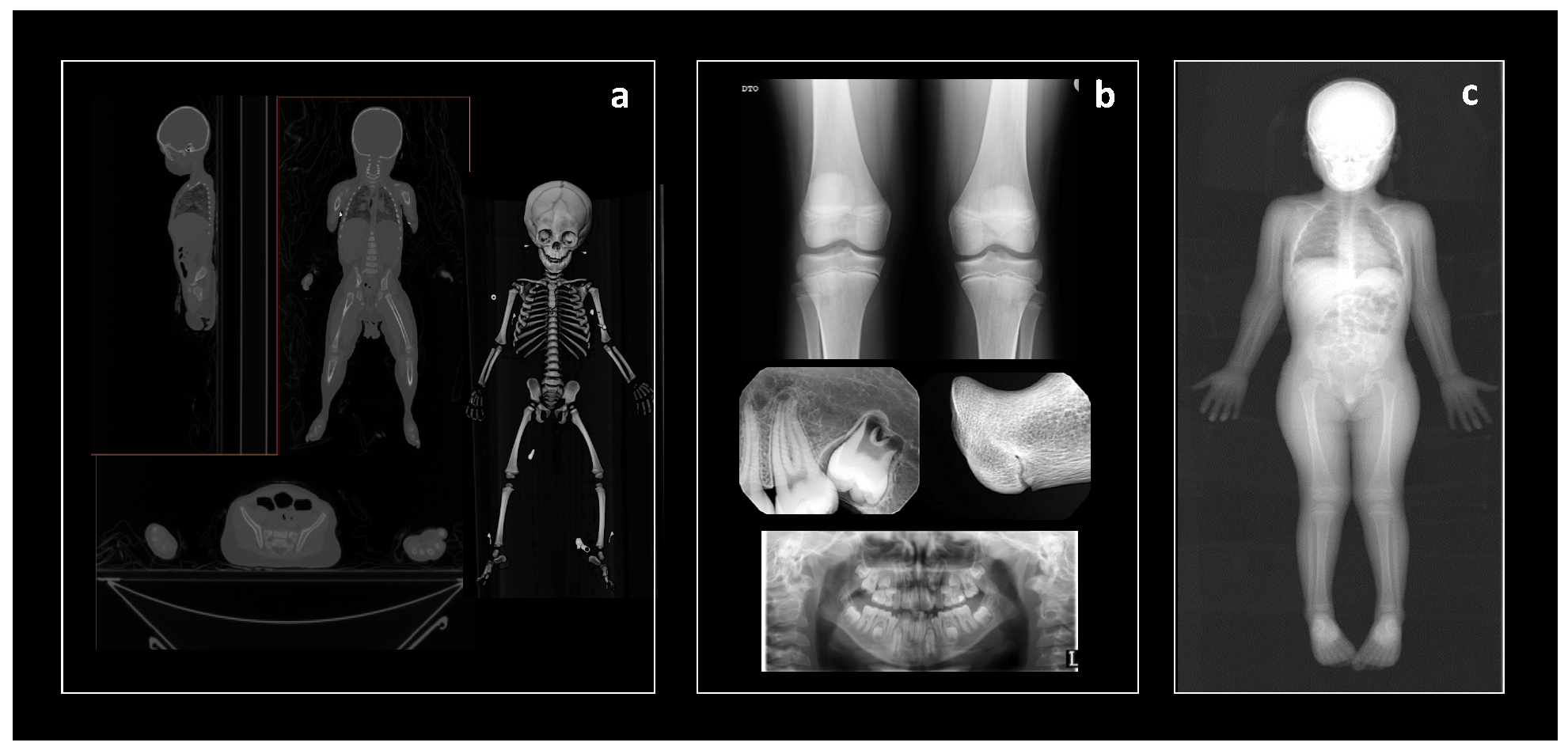
2.1. Collaborations, Contributions, and Imaging Modalities
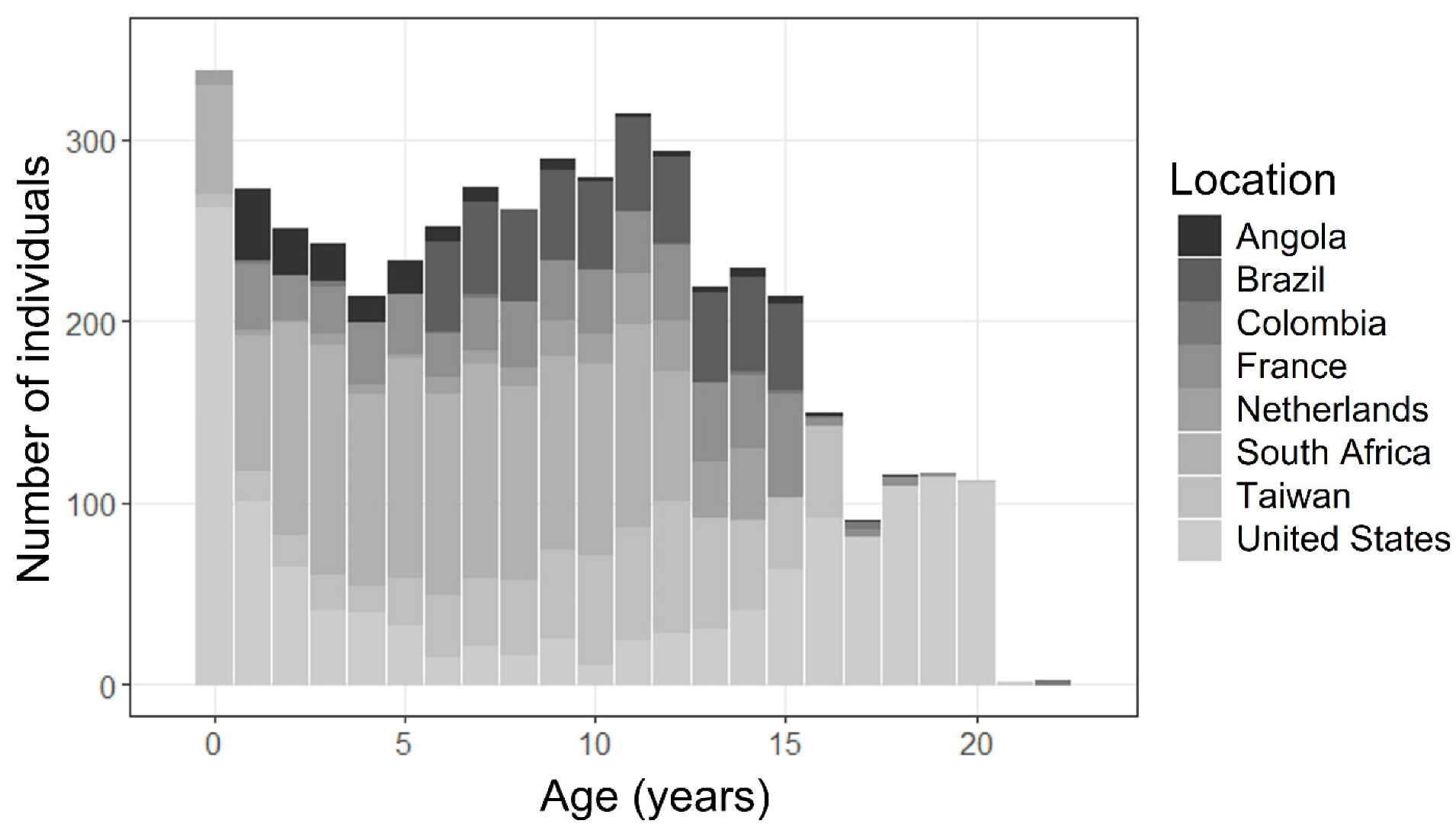
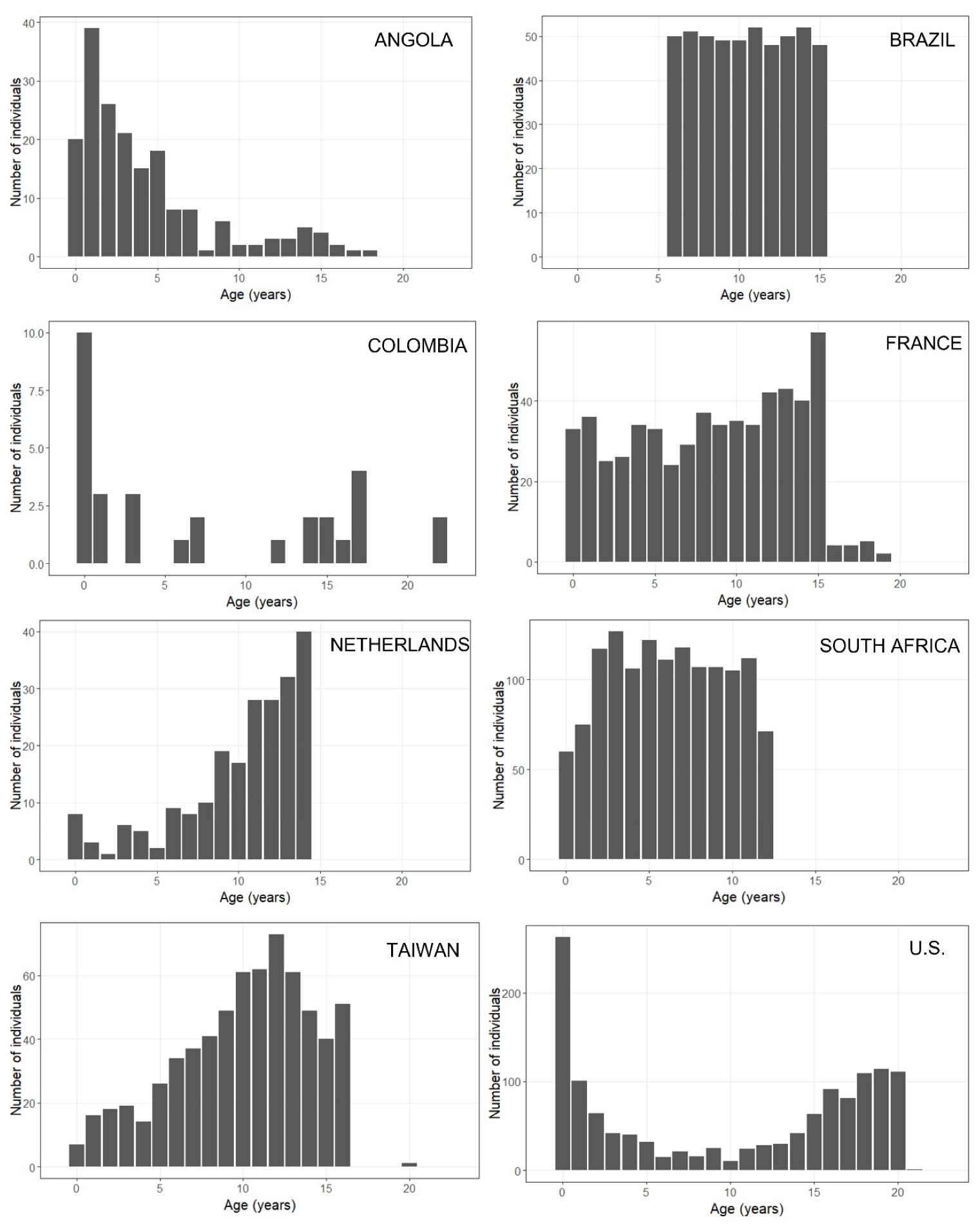
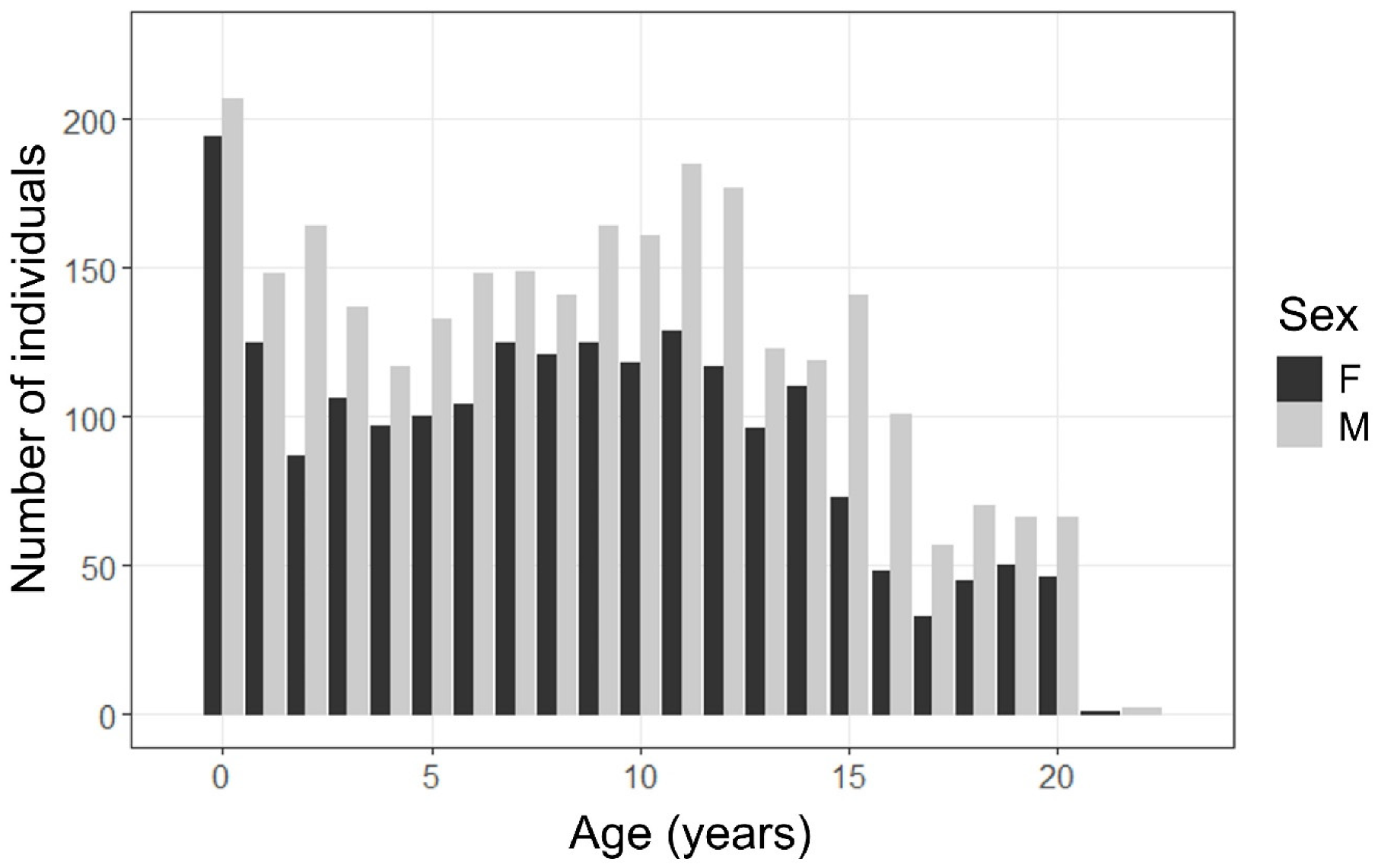
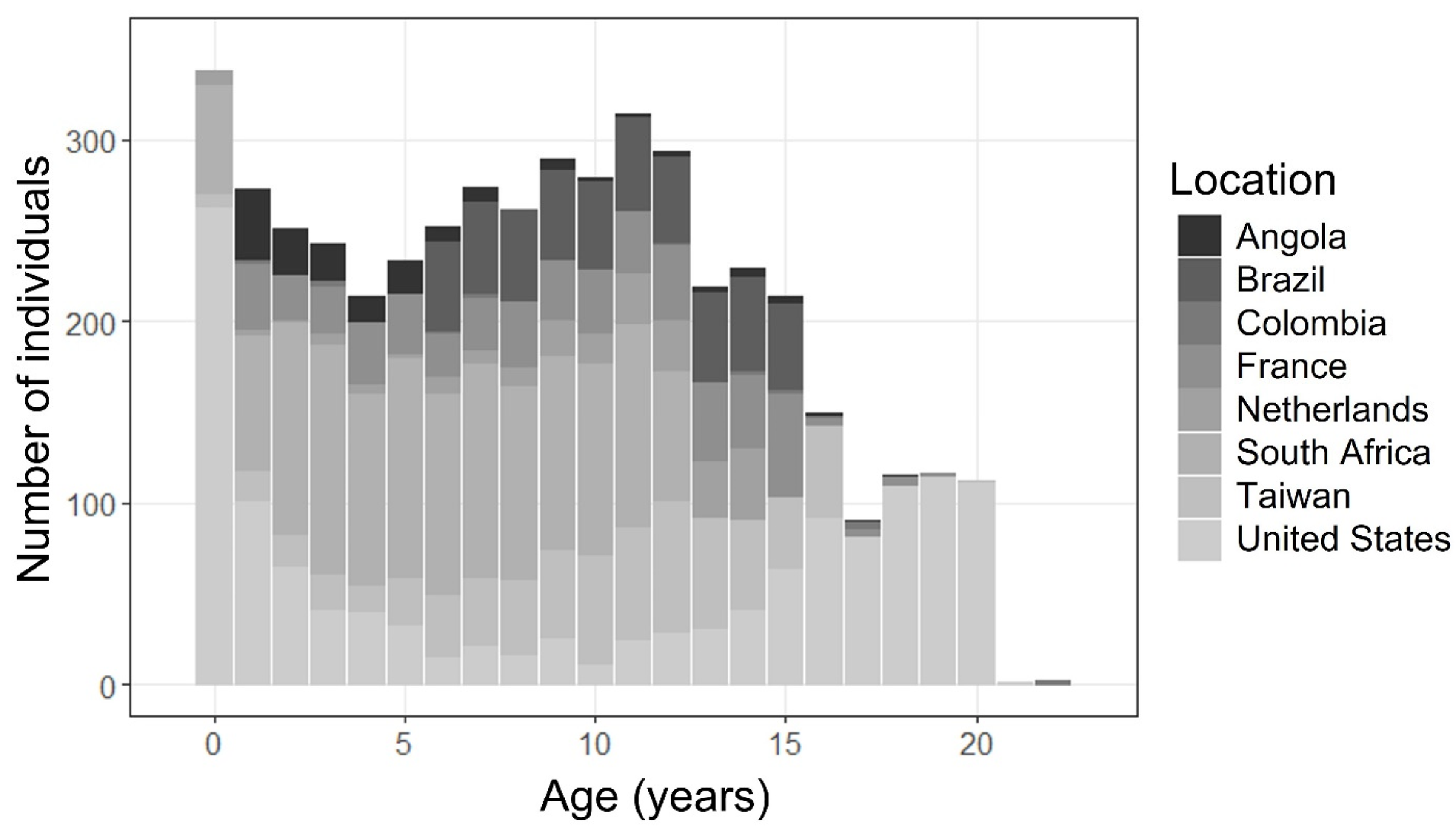
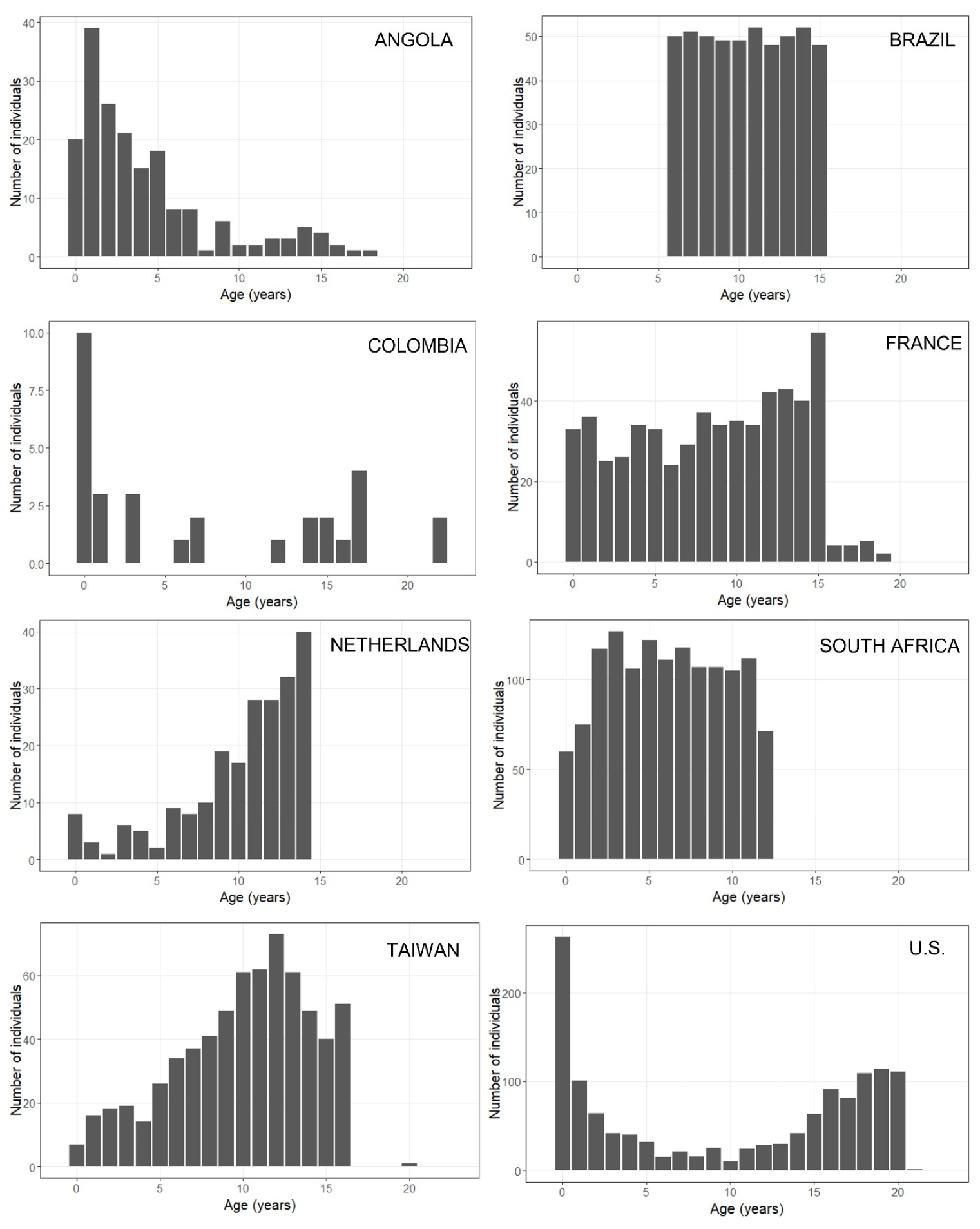
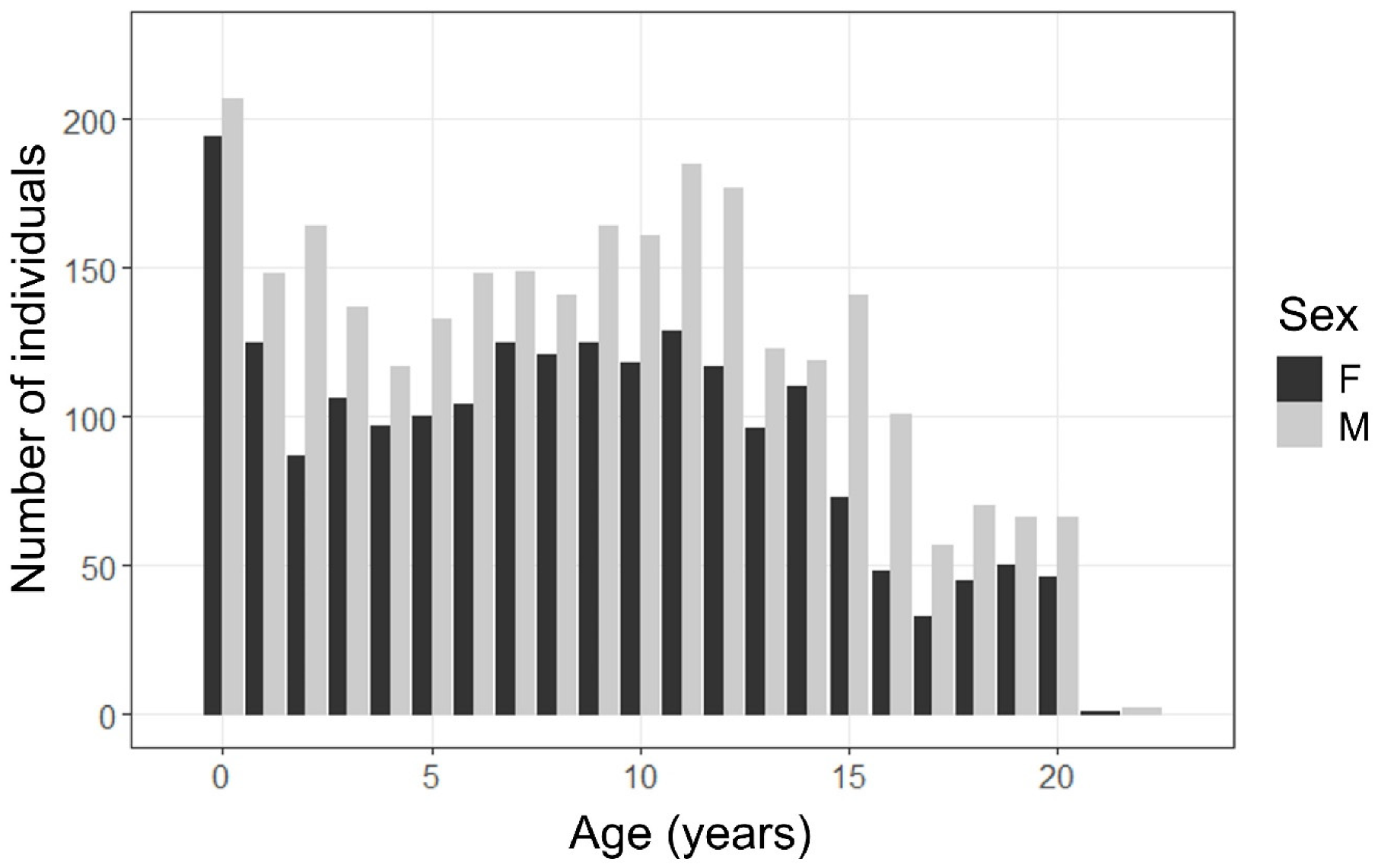
2.2. Sample Demographics
2.3. Derivatives
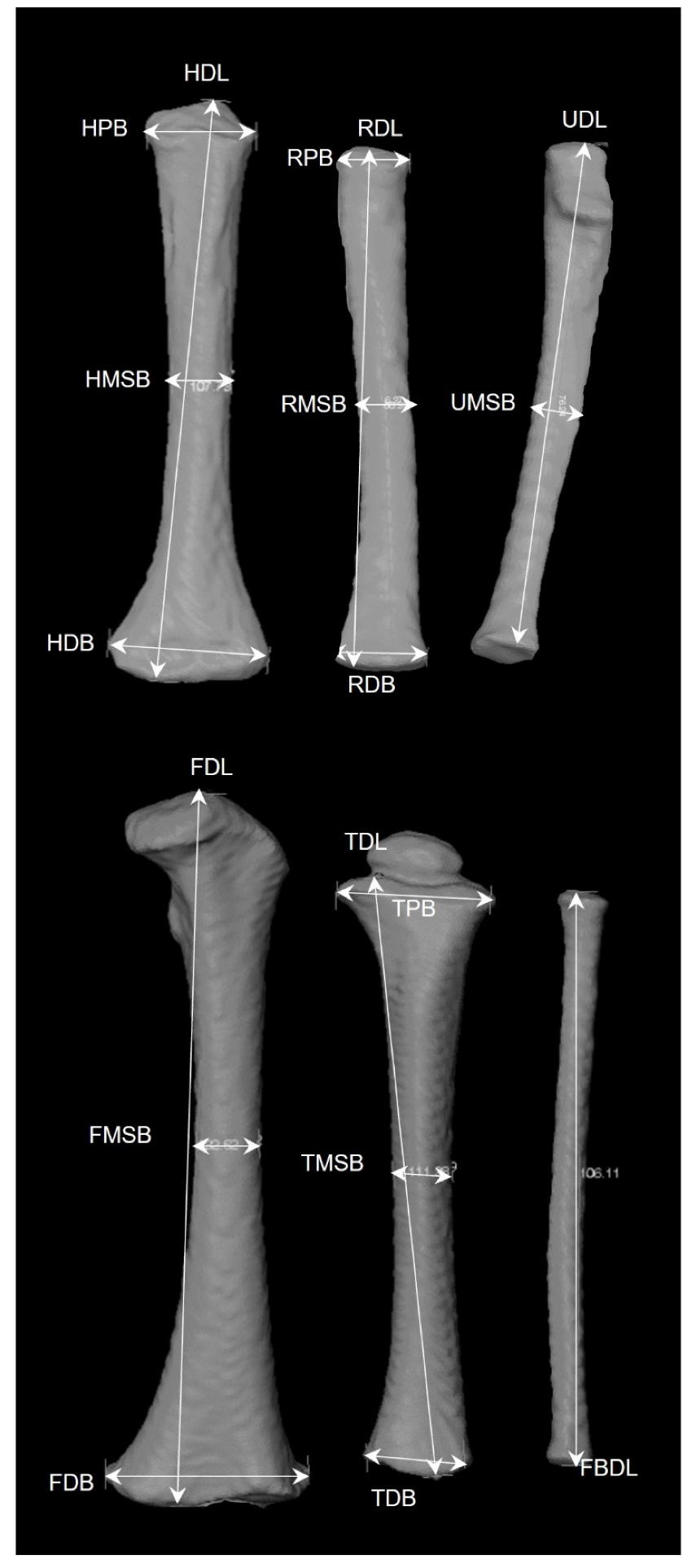
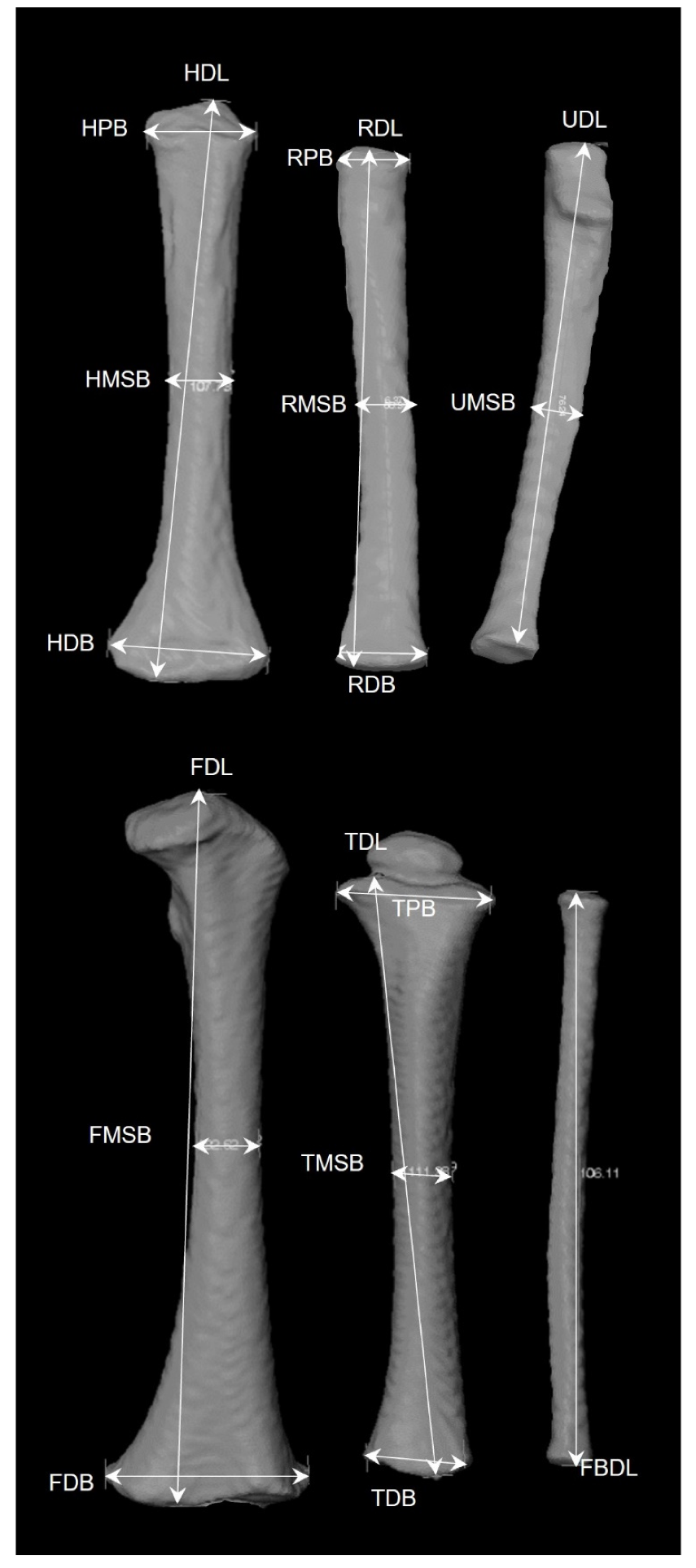
2.3.1. Diaphyseal Data
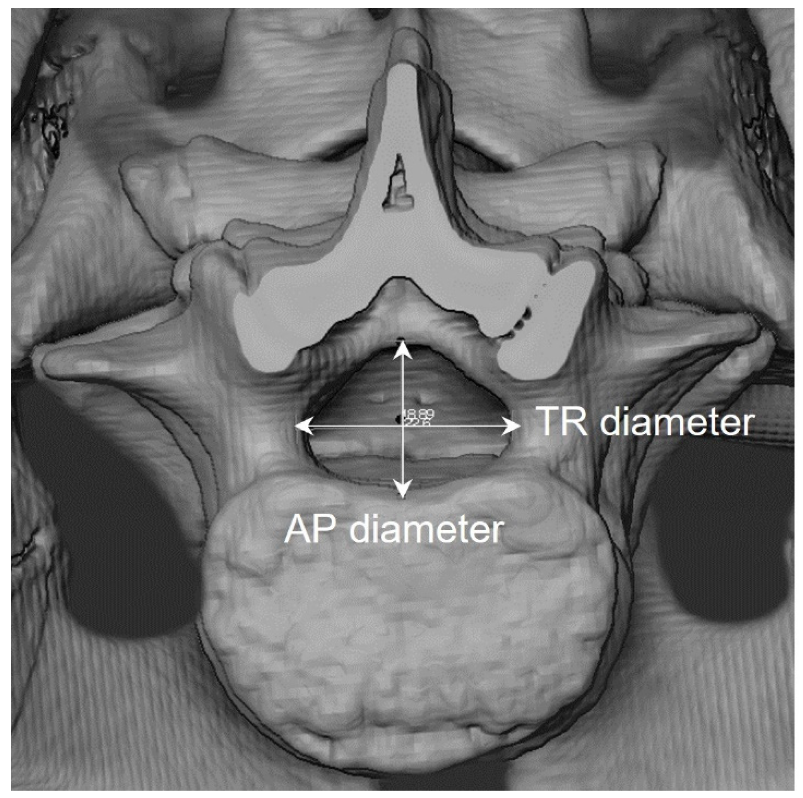
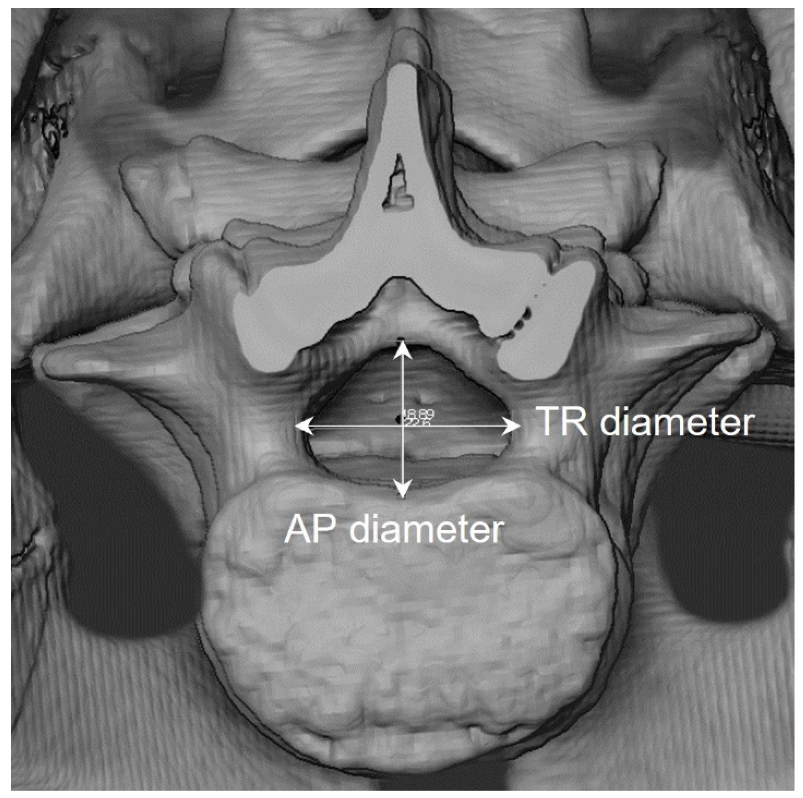
2.3.2. Vertebral Neural Canal Measurements (VNC)
2.3.3. Dental Development
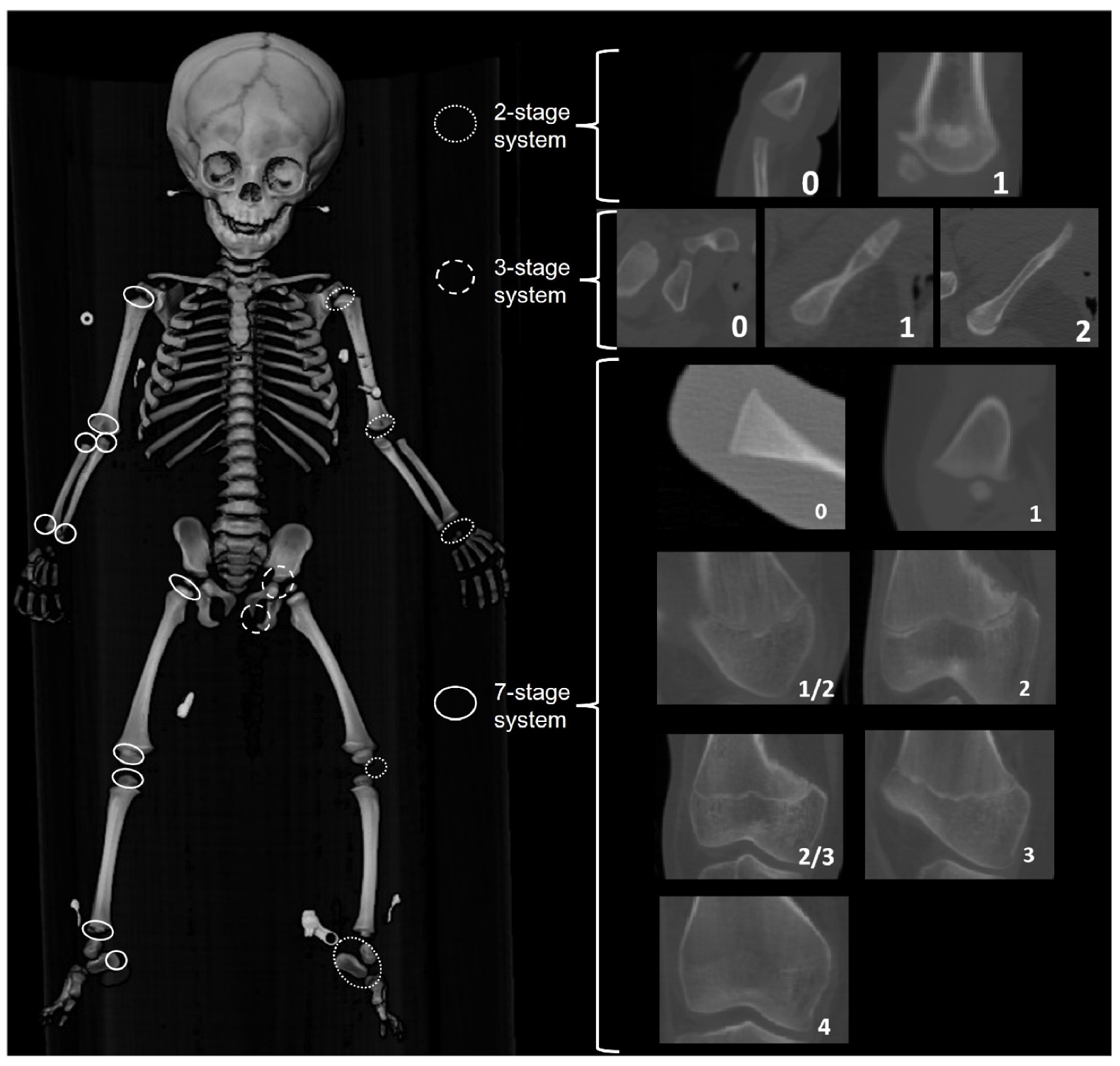
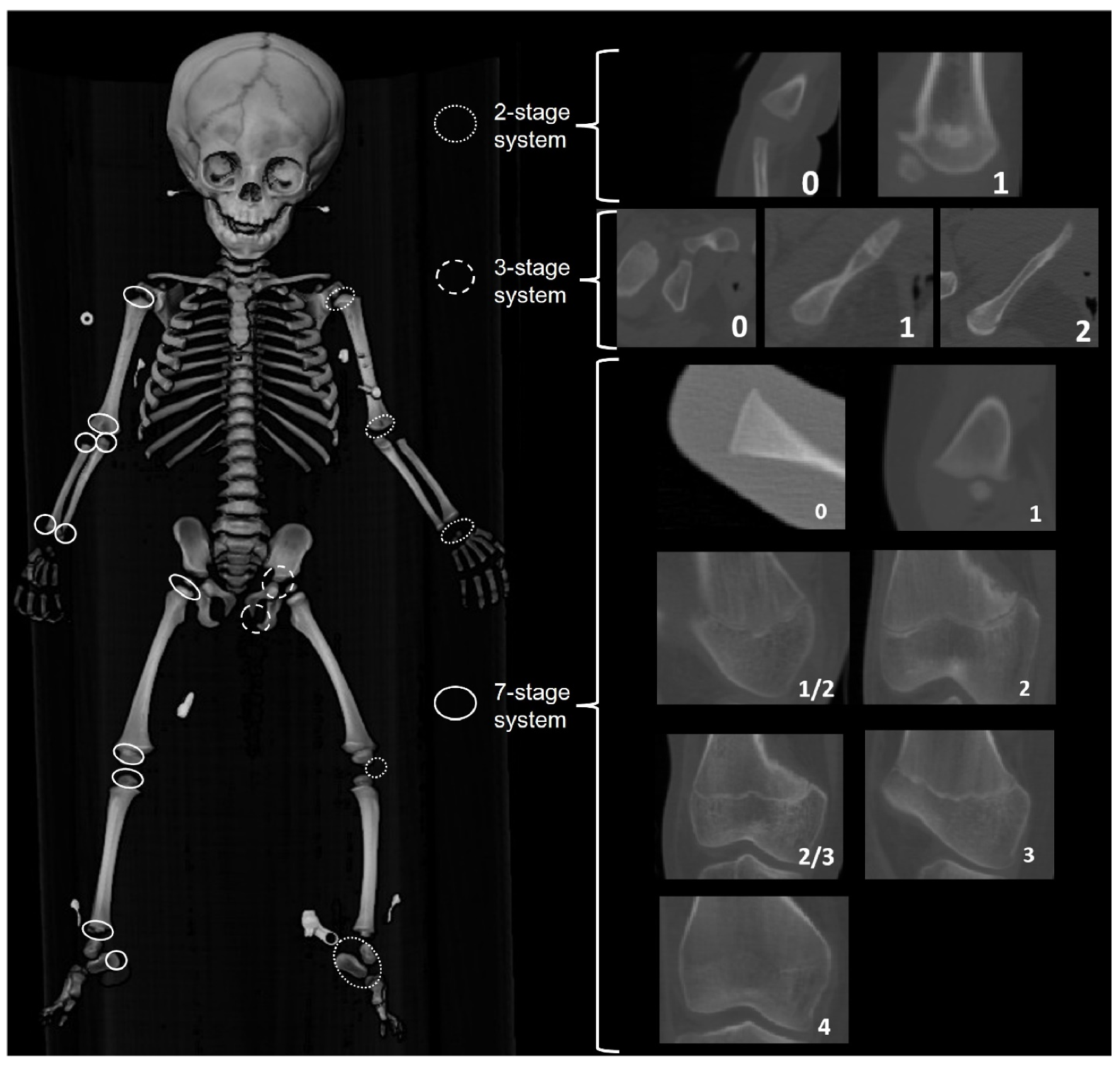
2.3.4. Epiphyseal Fusion (EF)
2.4. Observer Error and Agreement
3. Access and Expansion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aleman, I.; Irurita, J.; Valencia, A.R.; Martinez, A.; Lopez-Lazaro, S.; Viciano, J.; Botella, M.C. Brief communication: The Granada osteological collection of identified infants and young children. Am. J. Phys. Anthropol. 2012, 149, 606–610. [Google Scholar] [CrossRef]
- Cattaneo, C.; Mazzarelli, D.; Cappella, A.; Castoldi, E.; Mattia, M.; Poppa, P.; De Angelis, D.; Vitello, A.; Biehler-Gomez, L. A modern documented Italian identified skeletal collection of 2127 skeletons: The CAL Milano Cemetery Skeletal Collection. Forensic Sci. Int. 2018, 287, 219.e1–219.e5. [Google Scholar] [CrossRef]
- L’Abbé, E.N.; Loots, M.; Meiring, J.H. The Pretoria Bone Collection: A modern South African skeletal sample. Homo 2005, 56, 197–205. [Google Scholar] [CrossRef]
- Meadows Jantz, L.; Jantz, R. The Anthropology Research Facility, University of Tennessee. In The Forensic Anthropology Laboratory; Warren, M.W., Walsh-Haney, H.A., Freas, L., Eds.; CRC Press: Boca Raton, FL, USA, 2008; pp. 7–21. [Google Scholar]
- Molleson, T.; Cox, M. The Middling Sort (The Spitalfields Project, CBA Research Report 86); Council for British Archaeology: London, UK, 1993; Volume 2, p. 231. [Google Scholar]
- Cardoso, H.F. Brief communication: The collection of identified human skeletons housed at the Bocage Museum (National Museum of Natural History), Lisbon, Portugal. Am. J. Phys. Anthr. 2006, 129, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Maresh, M.M. Linear growth of long bones of extremities from infancy through adolescence: Continuing studies. AMA Am. J. Dis. Child. 1955, 89, 725–742. [Google Scholar] [CrossRef] [PubMed]
- Albanese, J. Identified Skeletal Reference Collections and the Study of Human Variation. Master’s Thesis, McMaster University, Hamilton, ON, Canada, 2003. [Google Scholar]
- Saunders, S.R.; De Vito, C. Subadult skeletons in the Raymond Dart Anatomical Collection: Research potential. Hum. Evol. 1991, 6, 421–434. [Google Scholar] [CrossRef]
- Stull, K.E.; Wolfe, C.A.; Corron, L.K.; Heim, K.; Hulse, C.N.; Pilloud, M. A Comparison of Subadult Skeletal and Dental Development Based on Living and Deceased Samples. Am. J. Phys. Anthropol. 2021, 175, 36–58. [Google Scholar] [CrossRef]
- Saunders, S.R.; Hoppa, R.D. Growth deficit in survivors and non-survivors: Biological mortality bias in subadult skeletal samples. Yearb. Phys. Anthropol. 1993, 36, 127–151. [Google Scholar] [CrossRef]
- Wood, J.W.; Milner, G.R.; Harpending, H.C.; Weiss, K.M.; Cohen, M.N.; Eisenberg, L.E.; Hutchinson, D.L.; Jankauskas, R.; Cesnys, G.; Cesnys, G.; et al. The osteological paradox: Problems of inferring prehistoric health from skeletal samples. Curr. Anthropol. 1992, 33, 343–370. [Google Scholar] [CrossRef]
- Konigsberg, L.; Frankenberg, S.R. Bayes in biological anthropology. Am. J. Phys. Anthropol. 2013, 57, 153–184. [Google Scholar] [CrossRef]
- Langley-Shirley, N.; Jantz, R.L. A Bayesian Approach to Age Estimation in Modern Americans from the Clavicle. J. Forensic Sci. 2010, 55, 571–583. [Google Scholar] [CrossRef] [PubMed]
- Beheim, B. Reproducible Research as Our New Default. Anthropol. News 2016, 57, e57–e58. [Google Scholar] [CrossRef]
- Martin, M.A. Biological Anthropology in 2018: Grounded in Theory, Questioning Contexts, Embracing Innovation. Am. Anthropol. 2019, 121, 417–430. [Google Scholar] [CrossRef]
- Dirkmaat, D.C.; Cabo, L.L.; Ousley, S.D.; Symes, S.A. New perspectives in forensic anthropology. Am. J. Phys. Anthropol. 2008, 137, 33–52. [Google Scholar] [CrossRef]
- Işcan, M.Y. Rise of forensic anthropology. Am. J. Phys. Anthropol. 1988, 31, 203–229. [Google Scholar] [CrossRef]
- Ubelaker, D.H. A history of forensic anthropology. Am. J. Phys. Anthropol. 2018, 165, 915–923. [Google Scholar] [CrossRef] [Green Version]
- Simmons-Ehrhardt, T. Open osteology: Medical imaging databases as skeletal collections. Forensic Imag. 2021, 26, 200462. [Google Scholar] [CrossRef]
- Colman, K.L.; de Boer, H.H.; Dobbe, J.G.; Liberton, N.P.T.J.; Stull, K.E.; van Eijnaten, M.; Streekstra, G.J.; Oostra, R.J.; Van Rijn, R.R.; van der Merwe, A.E. Virtual forensic anthropology: The accuracy of osteometric analysis of 3D bone models derived from clinical computed tomography (CT) scans. Forensic Sci. Int. 2019, 304, 109963. [Google Scholar] [CrossRef]
- Colman, K.L.; Dobbe, J.G.G.; Stull, K.E.; Ruijter, J.M.; Oostra, R.J.; van Rijn, R.R. The geometrical precision of virtual bone models derived from clinical computed tomography data for forensic anthropology. Int. J. Legal Med. 2017, 131, 1155–1163. [Google Scholar] [CrossRef] [Green Version]
- Stock, M.K.; Garvin, H.M.; Corron, L.K.; Hulse, C.N.; Cirillo, L.E.; Klales, A.R.; Colman, K.L.; Stull, K.E. The importance of processing procedures and threshold values in CT scan segmentation of skeletal elements: An example using the immature os coxa. Forensic Sci. Int. 2020, 309, 110232. [Google Scholar] [CrossRef]
- Garvin, H.; Stock, M.K. The utility of advanced imaging in forensic anthropology. Acad. Forensic Pathol. 2016, 6, 499–516. [Google Scholar] [CrossRef] [PubMed]
- Stull, K.E.; L’Abbé, E.N.; Steiner, S. Measuring distortion of skeletal elements in Lodox Statscan-generated images. Clin. Anat. 2013, 26, 780–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brough, A.; Bennett, J.; Morgan, B. Anthropological measurement of the juvenile clavicle using multi-detector computed tomography—Affirming reliability. J. Forensic Sci. 2013, 58, 946–951. [Google Scholar] [CrossRef]
- Corron, L.; Marchal, F.; Condemi, S.; Chaumoître, K.; Adalian, P. Evaluating the consistency, repeatability and reproducibility of osteometric data on dry bone surfaces, scanned dry bone surfaces and scanned bone surfaces from living individuals. Bull. Mém. Société D’Anthropologie Paris 2017, 29, 33–53. [Google Scholar] [CrossRef]
- Corron, L.K.; Stock, M.K.; Cole, S.J.; Hulse, C.N.; Garvin, H.M.; Klales, A.R.; Stull, K.E. Standardizing ordinal subadult age indicators: Testing for observer agreement and consistency across modalities. Forensic Sci. Int. 2021, 320, 110687. [Google Scholar] [CrossRef] [PubMed]
- Franco, A.; Vetter, F.; de Fatima Coimbra, E.; Fernandes, A.; Thevissen, P. Comparing third molar root development staging in panoramic radiography, extracted teeth, and cone beam computed tomography. Int. J. Legal Med. 2019, 134, 347–353. [Google Scholar] [CrossRef]
- Spake, L.; Meyers, J.; Blau, S.; Cardoso, H.; Lottering, N. A simple and software-independent protocol for the measurement of post-cranial bones in anthropological contexts using thin slab maximum intensity projection. Forensic Imag. 2020, 20, 200354. [Google Scholar] [CrossRef]
- Stull, K.E.; Tise, M.L.; Ali, Z.; Fowler, D.R. Accuracy and reliability of measurements obtained from computed tomography 3D volume rendered images. Forensic Sci. Int. 2014, 238, 133–140. [Google Scholar] [CrossRef] [Green Version]
- De Tobel, J.; Ottow, C.; Widek, T.; Klasinc, I.; Mörnstad, H.; Thevissen, P.W.; Verstraete, K.L. Dental and Skeletal Imaging in Forensic Age Estimation: Disparities in Current Approaches and the Continuing Search for Optimization. Semin. Musculoskelet. Radiol. 2020, 24, 510–522. [Google Scholar] [CrossRef]
- Berry, S.D.; Edgar, H.J.H. Announcement: The New Mexico Decedent Image Database. Forensic Imag. 2021, 24, 200436. [Google Scholar] [CrossRef]
- Ousley, S. A Radiographic Database for Estimating Biological Parameters in Modern Subadults; NIJ Award 2008-DN-BX-K152—Final Technical Report; Mercyhurst University: Erie, PA, USA, 2013; p. 58. [Google Scholar]
- National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research. The Belmont Report: Ethical Principles and Guidelines for the Protection of Human Subjects of Research; U.S. Department of Health and Human Services: Washington, DC, USA, 1979; p. 10.
- Bidgood, W.D.; Horii, S.C.; Prior, F.W.; Van Syckle, D.E. Understanding and Using DICOM, the Data Interchange Standard for Biomedical Imaging. J. Am. Med. Inform. Assoc. 1997, 4, 199–212. [Google Scholar] [CrossRef] [Green Version]
- Johnson, A.E.; Pollard, T.; Berkowitz, S.J.; Greenbaum, N.R.; Lungren, M.P.; Deng, C.; Mark, R.G.; Horng, S. MIMIC-CXR: A large publicly available database of labeled chest radiographs. arXiv 2019, arXiv:1901.07042. [Google Scholar]
- Deyle, S.; Wagner, A.; Benneker, L.M.; Jeger, V.; Eggli, S.; Bonel, H.M.; Zimmermann, H.; Exadaktylos, A.K. Could Full-body Digital X-ray (LODOX-Statscan) Screening in Trauma Challenge Conventional Radiography? J. Trauma Inj. Infect. Crit. Care 2009, 66, 418–422. [Google Scholar] [CrossRef] [Green Version]
- Monsalve Vargas, T.; Isaza, J. Estudio biosocial de una muestra de restos óseos provenientes de la colección osteológica de referencia de la Universidad de Antioquia. Bol. Antropol. 2014, 29, 28–55. [Google Scholar]
- Food and Drug Administration Pediatric X-ray Imaging. 2018. Available online: https://www.fda.gov/radiation-emitting-products/medical-imaging/pediatric-x-ray-imaging (accessed on 1 November 2021).
- Hon, K.L.; Nelson, E.A. Gender disparity in paediatric hospital admissions. Ann. Acad. Med. Singap. 2006, 35, 882–888. [Google Scholar]
- Zachariasse, J.M.; Borensztajn, D.M.; Nieboer, D.; Alves, C.F.; Greber-Platzer, S.; Keyzer-Dekker, C.M.G.; Maconochie, I.K.; Steyerberg, E.W.; Smit, F.J.; Moll, H.A. Sex-specific differences in children attending the emergency department: Prospective observational study. BMJ Open 2020, 10, e035918. [Google Scholar] [CrossRef]
- Lostao, L.; Blane, D.; Gimeno, D.; Netuveli, G.; Regidor, E. Socioeconomic patterns in use of private and public health services in Spain and Britain: Implications for equity in health care. Health Place 2014, 25, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Morris, S.; Sutton, M.; Gravelle, H. Inequity and inequality in the use of health care in England: An empirical investigation. Soc. Sci. Med. 2005, 60, 1251–1266. [Google Scholar] [CrossRef]
- Regidor, E.; Martínez, D.; Calle, M.E.; Astasio, P.; Ortega, P.; Domínguez, V. Socioeconomic patterns in the use of public and private health services and equity in health care. BMC Health Serv. Res. 2008, 8, 183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, S.; Holubkov, R.; Dean, J.M.; Meert, K.L.; Berg, R.A.; Carcillo, J.; Newth, C.J.L.; Harrison, R.E.; Pollack, M.M.; CPCCRN. PICU Autopsies: Rates, Patient Characteristics, and the Role of the Medical Examiner. Pediatr. Crit Care Med. 2018, 19, 1137–1145. [Google Scholar] [CrossRef]
- Sorenson, S.B. Gender disparities in injury mortality: Consistent, persistent, and larger than you’d think. Am. J. Public Health 2011, 101 (Suppl. S1), S353–S358. [Google Scholar] [CrossRef]
- Stull, K.E.; Corron, L.K. Subadult Virtual Anthropology Database (SVAD) Data Collection Protocol: Amira. August 2021. Available online: https://zenodo.org/record/5348411#.YdVRQ9pByUk (accessed on 1 November 2021). [CrossRef]
- Stull, K.E.; Corron, L.K. Subadult Virtual Anthropology Database (SVAD) Data Collection Protocol: Epiphyseal Fusion, Diaphyseal Dimensions, Dental Development Stages, Vertebral Neural Canal Dimensions. August 2021. Available online: https://zenodo.org/record/5348392#.YdVLBlko-Uk (accessed on 1 November 2021). [CrossRef]
- Stull, K.E. KScollect: Purpose-Built App for Collecting Data for Future Inclusion in KidStats. 2017. Available online: https://github.com/geanes/KScollect (accessed on 1 November 2021).
- Fazekas, I.; Kosa, F. Forensic Fetal Osteology; Budapest, Hungary, 1978. [Google Scholar]
- Moore-Jansen, P.; Ousley, S.; Jantz, R. Data Collection Procedures for Forensic Skeletal Material; Department of Anthropology, The University of Tennessee: Knoxville, TN, USA, 1994. [Google Scholar]
- Stull, K.E.; L’Abbé, E.N.; Ousley, S.D. Using multivariate adaptive regression splines to estimate subadult age from diaphyseal dimensions. Am. J. Phys. Anthropol. 2014, 154, 376–386. [Google Scholar] [CrossRef] [Green Version]
- Robinson, C.; Eisma, R.; Morgan, B. Anthropological measurement of lower limb and foot bones using multi-detector computed tomography. J. Forensic Sci. 2008, 53, 1289–1295. [Google Scholar] [CrossRef]
- Watts, R. Non-specific indicators of stress and their association with age at death in medieval York: Using stature and vertebral neural canal size to examine the effects of stress occurring during different periods of development. Int. J. Osteoarchaeol. 2011, 21, 568–576. [Google Scholar] [CrossRef]
- Watts, R. Lumbar vertebral canal size in adults and children: Observations from a skeletal sample from London, England. Homo—J. Comp. Hum. Biol. 2013, 64, 120–128. [Google Scholar] [CrossRef] [PubMed]
- AlQahtani, S.J.; Hector, M.P.; Liversidge, H.M. Brief communication: The London atlas of Human tooth development and eruption. Am. J. Phys. Anthropol. 2010, 142, 461–490. [Google Scholar] [CrossRef]
- Moorrees, C.; Fanning, E.; Hunt, E.E. Age variation of formation stages for ten permanent teeth. J. Dent. Res. 1963, 42, 1490–1502. [Google Scholar] [CrossRef]
- Vanbelle, S. A New Interpretation of the Weighted Kappa Coefficients. Psychometrika 2016, 81, 399–410. [Google Scholar] [CrossRef] [PubMed]
- De Tobel, J.; Fieuws, S.; Hillewig, E.; Phlypo, I.; van Wikj, M.; de Haas, M.; Politis, C.; Verstraete, K.; Thevissen, P.W. Multi-factorial age estimation: A Bayesian approach combining dental and skeletal magnetic resonance imaging. Forensic Sci. Int. 2020, 306, 110054. [Google Scholar] [CrossRef]
- Lottering, N.; MacGregor, D.M.; Barry, M.D.; Reynolds, M.S.; Gregory, L.S. Introducing standardized protocols for anthropological measurement of virtual subadult crania using computed tomography. J. Forensic Radiol. Imaging 2014, 2, 34–38. [Google Scholar] [CrossRef]
- Stock, M.K.; Stull, K.E.; Garvin, H.M.; Klales, A. Development of Modern Human Subadult Age and Sex Estimation Standards Using Multi-Slice Computed Tomography Images from Medical Examiner’s Offices; International Society for Optics and Photonics: Bellingham, DC, USA, 2016; Volume 9967, p. 99670E. [Google Scholar]
- Berry, S.D.; Edgar, H.J.H. Extracting and Standardizing Medical Examiner Data to Improve Health. AMIA Jt. Sum. Transl. Sci. Proc. 2020, 2020, 63–70. [Google Scholar]
- Lottering, N.; MacGregor, D.; Alston, C.; Watson, D.; Gregory, L.S. Introducing computed tomography standards for age estimation of modern Australian subadults using postnatal ossification timings of select cranial and cervical sites. J. Forensic Sci. 2016, 61, S39–S52. [Google Scholar] [CrossRef]
- Liebenberg, L.; Kruger, G.C. Standardization and quality assurance in skeletal landmark placement and osteometry. Forensic Sci. Int. 2020, 308, 110168. [Google Scholar] [CrossRef] [PubMed]
- Allen, C.; Mehler, D.M.A. Open science challenges, benefits and tips in early career and beyond. PLoS Biol. 2019, 17, e3000246. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Continent | Country | Sample Size (by Sex) | Age Range (Years) | Deceased/Living |
|---|---|---|---|---|
| Africa | Angola | N = 186 (99 F, 87 M) | 0–15 years | Living |
| South Africa | N = 1352 (531 F, 821 M) | 0–12 years | Living | |
| South America | Colombia | N = 31 (5 F, 26 M) | 0–22 years | Deceased |
| Brazil | N = 500 (248 F, 252 M) | 0–15 years | Living | |
| Europe | France | N = 578 (260 F, 318 M) | 0–15 years | Living |
| The Netherlands | N = 218 (109 F, 107 M) | 0–15 years | Living | |
| Asia | Taiwan | N = 730 (306 F, 424 M) | 0–16 years | Living |
| North America | United States (Maryland) | N = 244 (96 F, 148 M) | 0–20 years | Deceased |
| United States (New Mexico) | N = 1077 (441 F, 636 M) | 0–21 years | Deceased |
| Country | Partner Institution | Context | Modality | Derivatives | Availability |
|---|---|---|---|---|---|
| Angola | Departamento de Ciências da Vida, University of Coimbra and private medical cabinets from Luanda, Angola | Private practice | Conventional radiograph | Epiphyseal fusion stages Dental development stages | Derivatives |
| South Africa | Red Cross War Memorial Children’s Hospital, Cape Town Hospital | Hospital | Lodox Statscan | Dental development stagesEpiphyseal fusion stages Long bone dimensions | Derivatives |
| Forensic Pathology Services, Salt River, Cape Town | Forensic | Lodox Statscan | Long bone dimensions | Derivatives | |
| Colombia | Universidad de Antioquia, Medellin | Forensic | Dry bone (long bone dimensions and epiphyseal fusion) Conventional radiograph (dental development and epiphyseal fusion) | Long bone dimensions VNC diameters Epiphyseal fusion stages Dental development stages | Radiographs and derivatives |
| Brazil | Universidade de São Paulo (FOUSP) | Dental Practice | Panoramic radiograph | Dental development stages | Panoramic radiographs and derivatives |
| France | Public hospital services of Marseille (AP-HM) | Hospital | CT scan | Long bone dimensions VNC diameters Epiphyseal fusion stages Dental development stages Segmented bone surfaces | Derivatives |
| The Netherlands | Amsterdam Medical Center (Hospital) | Hospital | CT scan | Long bone dimensions VNC diameters Epiphyseal fusion stages Dental development stages Segmented bone surfaces | CT scans and derivatives |
| Taiwan | National Taiwan University Hospital, Taipei City | Hospital | CT scan | Long bone dimensions VNC diameters Epiphyseal fusion stages Dental development stages Segmented bone surfaces | Derivatives |
| United States * | Office of the Chief Medical Examiner, Baltimore, Maryland | Medico-legal | CT scan | Long bone dimensions Epiphyseal fusion stages | Derivatives |
| University of New Mexico Health Sciences Center, Office of the Medical Investigator, Albuquerque, New Mexico | Medico-legal | CT scan | Long bone dimensions VNC diameters Epiphyseal fusion stages Dental development stages Pelvic landmarks Segmented bone surfaces | CT scans ** and derivatives |
| Stage | Monoradicular Teeth | Pluriradicular Teeth | Description |
|---|---|---|---|
| 1 |  |  | Initial cusp formation |
| 2 |  |  | Coalescence of cusps |
| 3 |  |  | Cusp outline complete |
| 4 |  |  | Crown half completed with dentine formation |
| 5 |  |  | Crown three quarters completed |
| 6 |  |  | Crown completed with defined pulp roof |
| 7 |  |  | Initial root formation with diverge edges |
| 8 |  |  | Root length less than crown length |
| 9 |  |  | Root length equals crown length |
| 10 |  |  | Three quarters of root length developed with diverge ends |
| 11 |  |  | Root length completed with parallel ends |
| 12 |  |  | Apex closed (root ends converge) with wide periodontal ligament |
| 13 |  |  | Apex closed with normal periodontal ligament width |
| Intra-Observer Error | Inter-Observer Error | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TEM (mm) | TEM (%) | TEM (mm) | TEM (%) | |||||||||
| MIN | MAX | AVG | MIN | MAX | AVG | MIN | MAX | AVG | MIN | MAX | AVG | |
| Long Bone Dimensions | 0.0426 | 0.364 | 0.156 | 0.069 | 1.723 | 0.502 | 0.0354 | 0.34 | 0.133 | 0.098 | 0.877 | 0.453 |
| Vertebral Neural Canal | 0.024 | 0.178 | 0.103 | 0.161 | 1.104 | 0.589 | 0.118 | 0.358 | 0.193 | 0.672 | 2.117 | 1.127 |
| Intra-Observer Error | Inter-Observer Error | |||||
|---|---|---|---|---|---|---|
| Cohen’s Kappa | Cohen’s Kappa | |||||
| MIN | MAX | AVG | MIN | MAX | AVG | |
| Epiphyseal fusion stages * | 0.545 | 1.00 | 0.974 | 0.501 | 1.00 | 0.930 |
| Dental development stages * | 0.687 | 1.00 | 0.939 | 0.774 | 1.00 | 0.965 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stull, K.E.; Corron, L.K. The Subadult Virtual Anthropology Database (SVAD): An Accessible Repository of Contemporary Subadult Reference Data. Forensic Sci. 2022, 2, 20-36. https://doi.org/10.3390/forensicsci2010003
Stull KE, Corron LK. The Subadult Virtual Anthropology Database (SVAD): An Accessible Repository of Contemporary Subadult Reference Data. Forensic Sciences. 2022; 2(1):20-36. https://doi.org/10.3390/forensicsci2010003
Chicago/Turabian StyleStull, Kyra E., and Louise K. Corron. 2022. "The Subadult Virtual Anthropology Database (SVAD): An Accessible Repository of Contemporary Subadult Reference Data" Forensic Sciences 2, no. 1: 20-36. https://doi.org/10.3390/forensicsci2010003
APA StyleStull, K. E., & Corron, L. K. (2022). The Subadult Virtual Anthropology Database (SVAD): An Accessible Repository of Contemporary Subadult Reference Data. Forensic Sciences, 2(1), 20-36. https://doi.org/10.3390/forensicsci2010003