Biochemical Changes in Salivary pH and Its Correlation to Hemoglobin Levels, Calcium and Phosphate Ion Concentrations among Pregnant Women, Tanzania: A Cross-Sectional Study


Abstract
:1. Background
2. Methods
2.1. Study Design
2.2. Sample Size and Study Participant Selection Procedure
2.3. Saliva Collection
2.4. Study Variables
2.5. Data Management and Analysis
3. Results
3.1. Study Participant’s Demographic and Clinical Characteristics
3.2. Description of Saliva Electrolytes Values
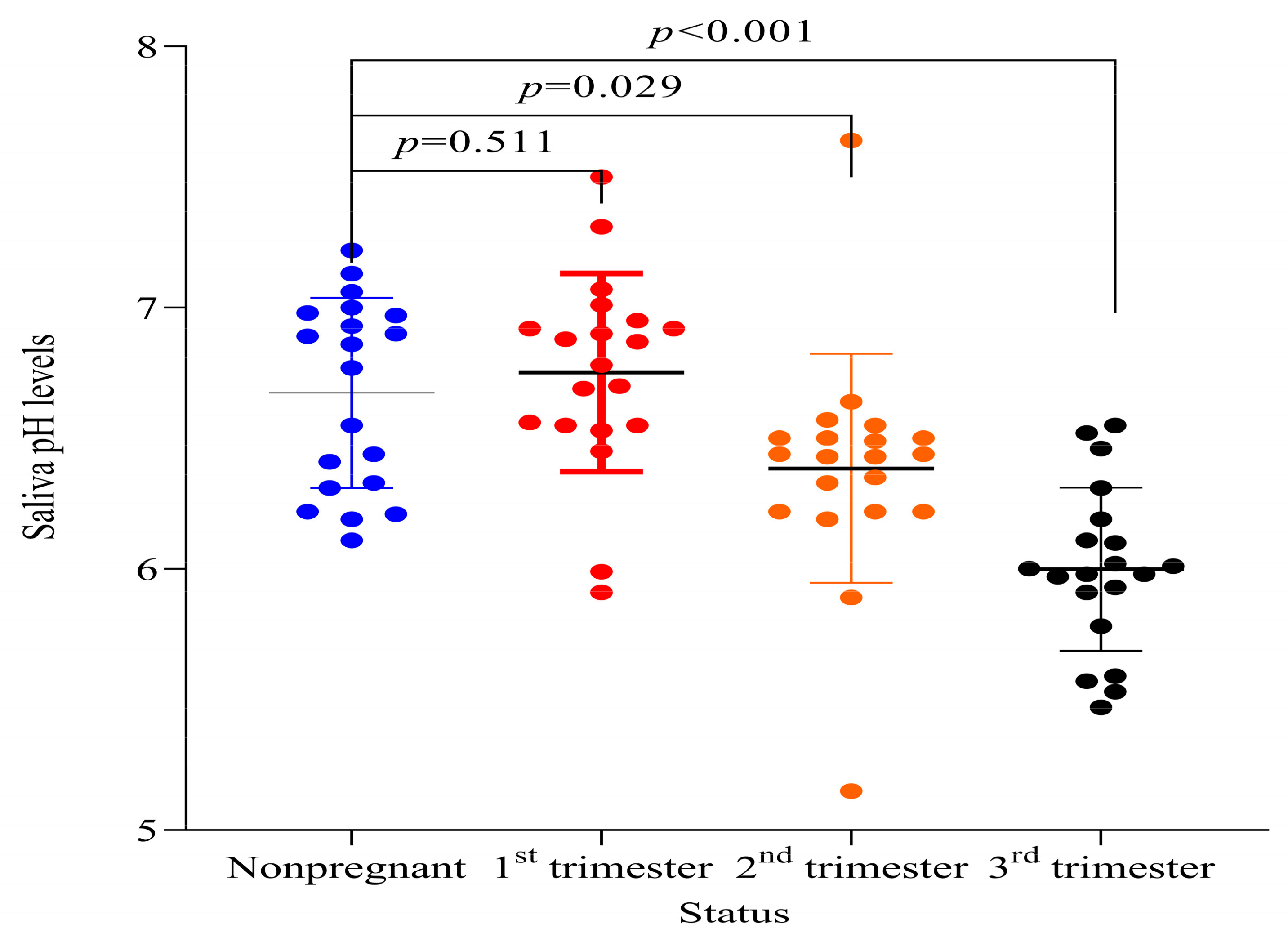
3.3. Saliva pH
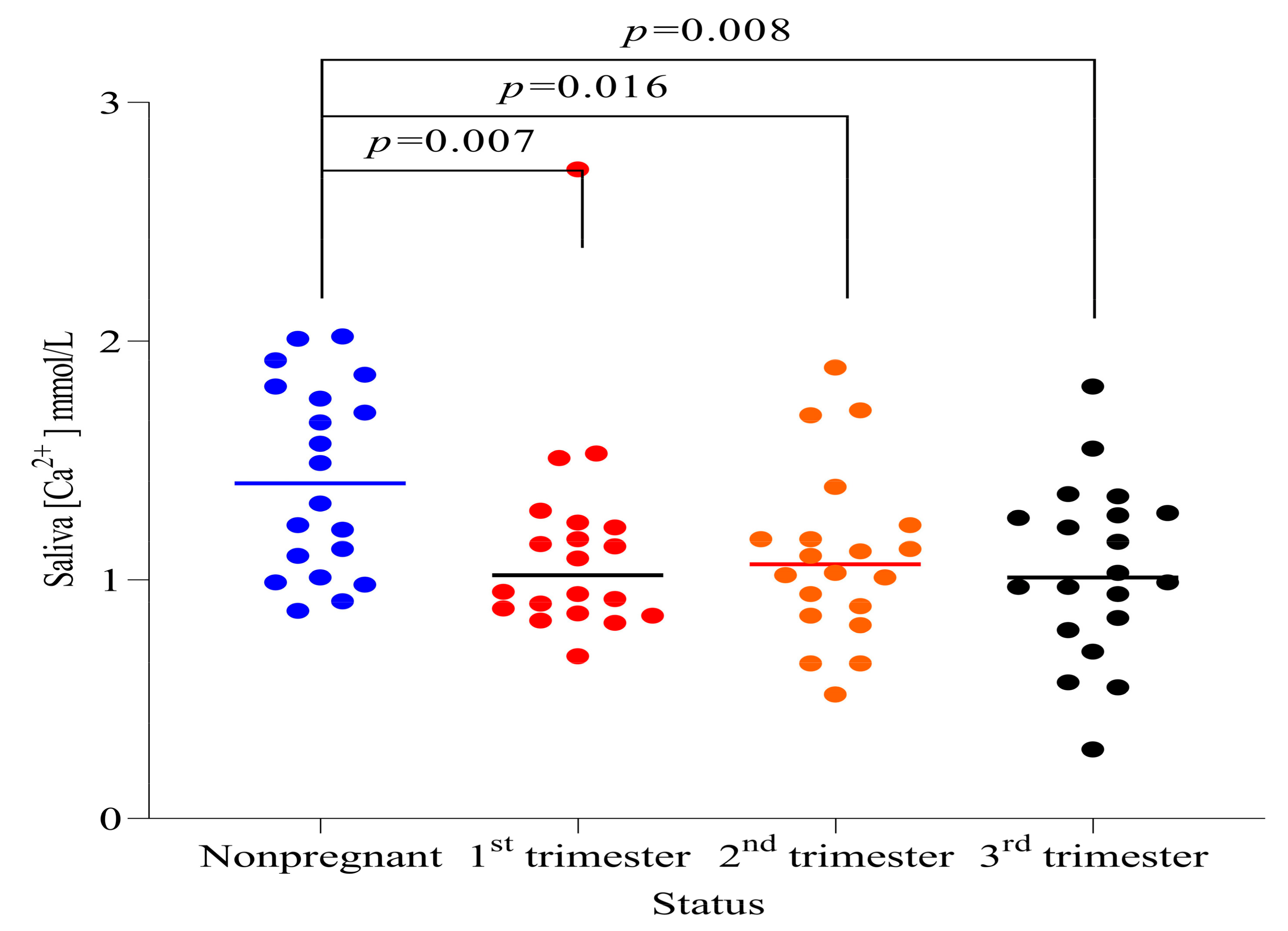
3.4. Saliva Calcium Ion Concentration
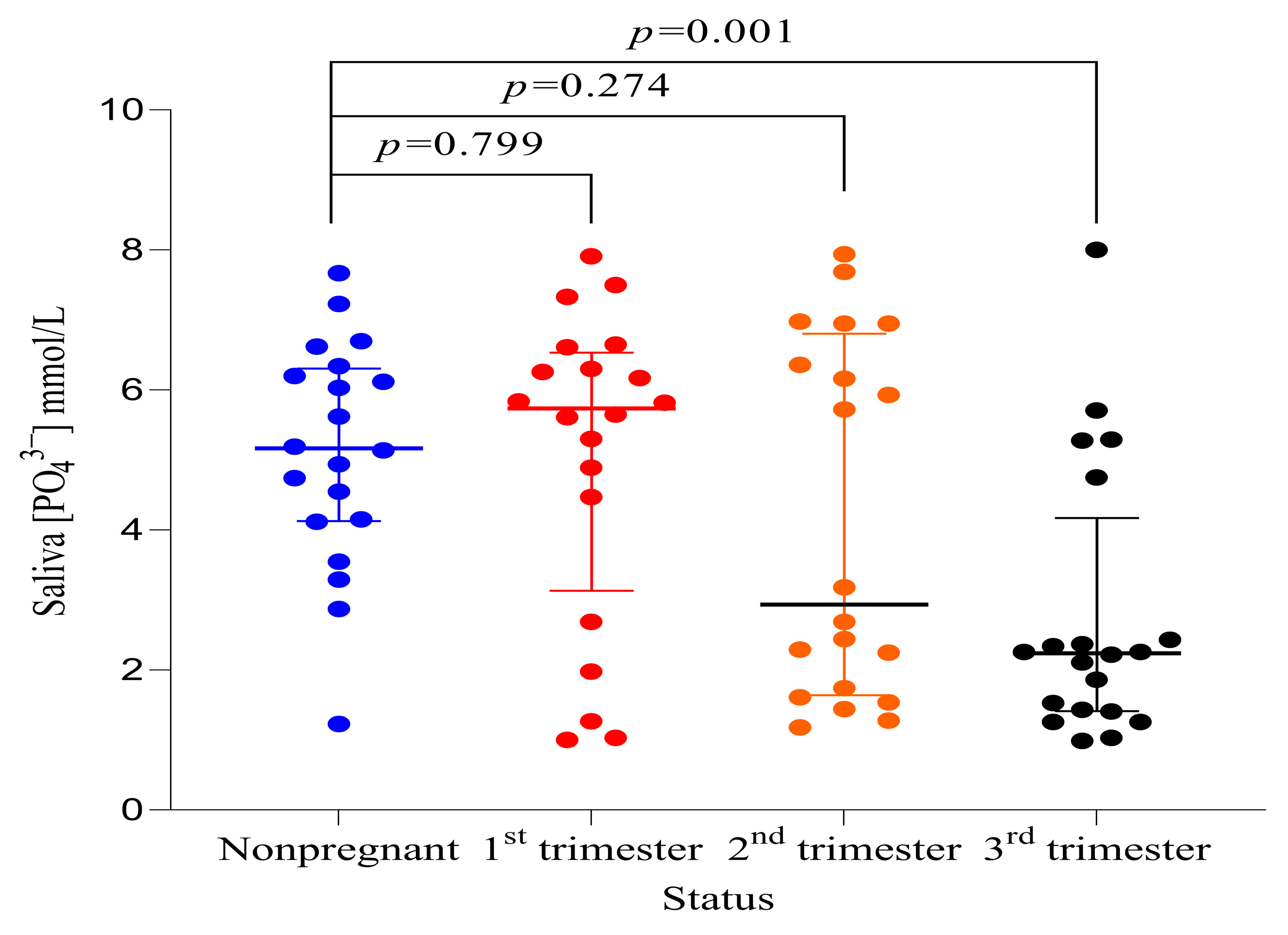
3.5. Saliva Phosphate Ion Concentration
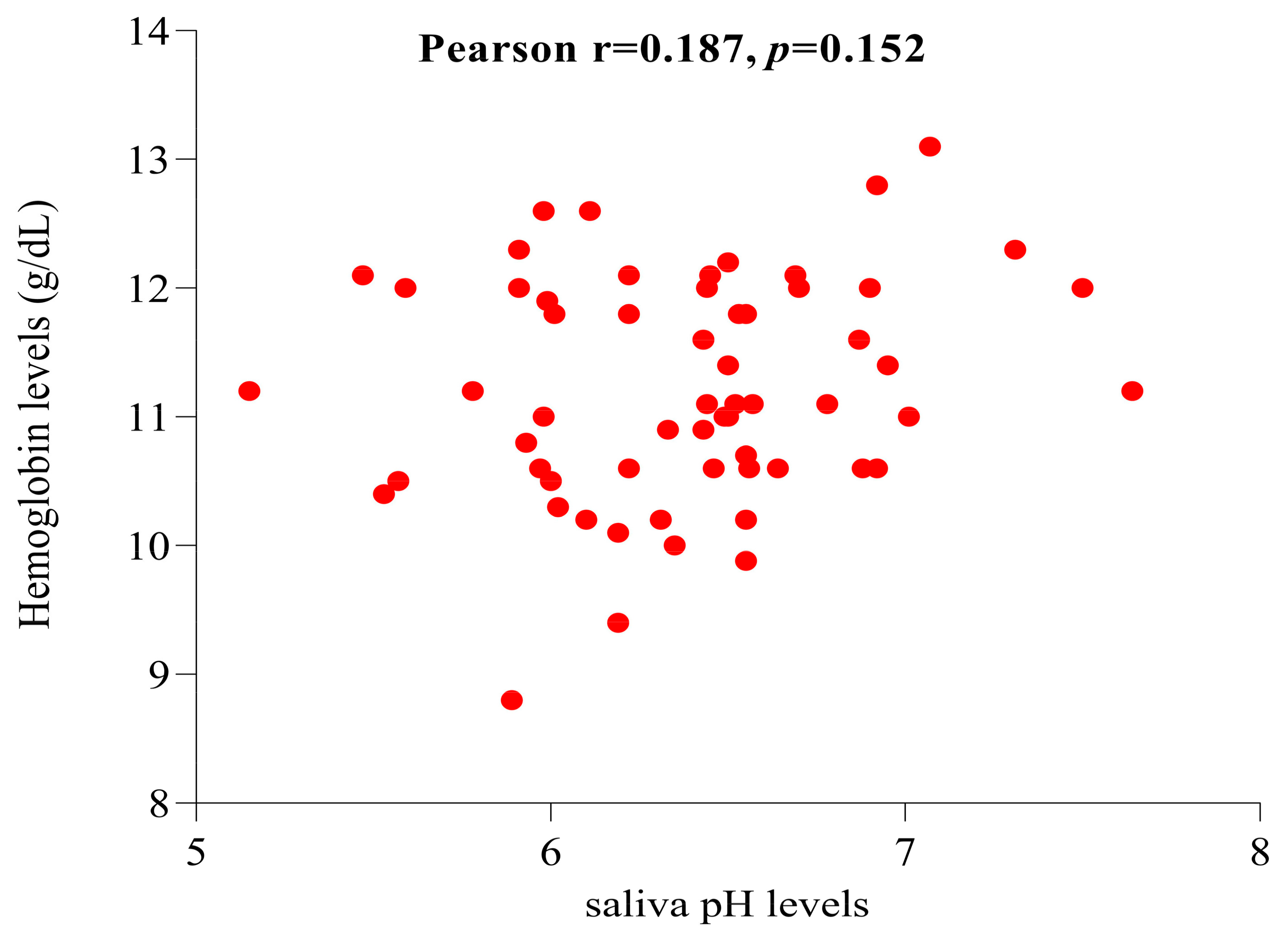
3.6. Correlation of Saliva pH Levels and Hemoglobin Levels among Pregnant Women
4. Discussion
5. Conclusions
6. Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Proctor, G.B. The physiology of salivary secretion. Periodontol. 2000 2016, 70, 11–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spielman, A.I.; D’Abundo, S.; Field, R.B.; Schmale, H. Protein Analysis of Human von Ebner Saliva and a Method for its Collection from the Foliate Papillae. J. Dent. Res. 2016, 72, 1331–1335. [Google Scholar] [CrossRef] [PubMed]
- De Almeida, P.D.V.; Grégio, A.M.T.; Machado, M.Â.N.; De Lima, A.A.S.; Azevedo, L.R. Saliva composition and functions: A comprehensive review. J. Contemp. Dent. Pract. 2008, 9, 72–80. [Google Scholar] [PubMed]
- Saher, F.; Khurshid, Z.; Zafar, M.S.; Mohammed, F.; Khurram, S.A. Salivary Glands. In An Illustrated Guide to Oral Histology; Wiley Online: Hoboken, NJ, USA, 2021; pp. 147–166. [Google Scholar]
- Maddu, N.; Maddu, N. Functions of Saliva. Saliva and Salivary Diagnostics. 2019. Available online: https://www.intechopen.com/state.item.id (accessed on 29 November 2022).
- Kumar, B.; Kashyap, N.; Avinash, A.; Chevvuri, R.; Sagar, M.K.; Shrikant, K. The composition, function and role of saliva in maintaining oral health: A review. Int. J. Contemp. Dent. Med. Rev. 2017, 220, 011217. [Google Scholar]
- Humphrey, S.P.; Williamson, R.T. A review of saliva: Normal composition, flow, and function. J. Prosthet. Dent. 2001, 85, 162–169. [Google Scholar] [CrossRef]
- Abou Neel, E.A.; Aljabo, A.; Strange, A.; Ibrahim, S.; Coathup, M.; Young, A.M.; Bozec, L.; Mudera, V. Demineralization–remineralization dynamics in teeth and bone. Int. J. Nanomed. 2016, 11, 4743. [Google Scholar] [CrossRef] [PubMed]
- Preethi, B.P.; Pyati, A.; Dodawad, R. Evaluation of flow rate, ph, buffering capacity, calcium, total protein and total antioxidant levels of saliva in caries free and caries active children—An in vivo study. Biomed. Res. 2010, 25, 425–428. [Google Scholar] [CrossRef] [Green Version]
- Mohamed, W.E.; Abou El Fadl, R.K.; Thabet, R.A.; Helmi, M.; Kamal, S.H. Iron deficiency anaemia and early childhood caries: A cross-sectional study. Aust. Dent. J. 2021, 66, S27–S36. [Google Scholar] [CrossRef]
- Joel, A.M.M.; Zurisadai, N.A.; Alejandra, L.A.; Hector, M.H.N.; Jany, A.J.D.V.; Alma, N.C.P.; Sosa-Martinez, L.R.; De La Garza-Ramos, M.A. The importance of pH, salivary flow and different dental caries risk factors in pregnant women. J. Dent. Oral Hyg. 2018, 10, 18–22. [Google Scholar] [CrossRef]
- Deshpande, A.N.; Sudani, U.; Wadhwa, M.; Joshi, N.; Patel, K.S.; Jain, A. Association of Anthropometric Measurements, Hemoglobin Level and Salivary Parameters among Caries-free and S-ECC Children. Int. J. Clin. Pediatr. Dent. 2022, 15 (Suppl. S2), S164. [Google Scholar]
- Salvolini, E.; Di Giorgio, R.; Curatola, A.; Mazzanti, L.; Fratto, G. Biochemical modifications of human whole saliva induced by pregnancy. BJOG 1998, 105, 656–660. [Google Scholar] [CrossRef]
- Rio, R.; Azevedo, Á.; Simões-Silva, L.; Marinho, J.; Silva, M.J.; Sampaio-Maia, B. The biochemistry of saliva throughout pregnancy. Med. Express 2015, 2, M150506. Available online: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S2358-04292015000500006&lng=en&nrm=iso&tlng=en (accessed on 20 April 2021). [CrossRef] [Green Version]
- Rockenbach, M.I.; Marinho, S.A.; Veeck, E.B.; Lindemann, L.; Shinkai, R.S. Salivary flow rate, pH, and concentrations of calcium, phosphate, and sIgA in Brazilian pregnant and non-pregnant women. Head Face Med. 2006, 2, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, A.; Qureshi, B.; Qureshi, A.; Imtiaz, Y.; Qadeer, S. Correlation of salivary characteristics with high risk of dental caries; A clinical investigation. Future Dent. J. 2017, 4, 72–75. [Google Scholar] [CrossRef]
- Naseem, M.; Khurshid, Z.; Khan, H.A.; Niazi, F.; Zohaib, S.; Zafar, M.S. Oral health challenges in pregnant women: Recommendations for dental care professionals. Saudi J. Dent. Res. 2016, 7, 138–146. [Google Scholar] [CrossRef] [Green Version]
- Hemalatha, V.T.; Manigandan, T.; Sarumathi, T.; Aarthi Nisha, V.; Amudhan, A. Dental Considerations in Pregnancy-A Critical Review on the Oral Care. J. Clin. Diagn. Res. 2013, 7, 948. [Google Scholar]
- Mwangosi, I.E.A.T.; Kiango, M.M. Oral health experience during pregnancy and dental service utilization in Bariadi District, Tanzania. Tanzan J. Health Res. 2012, 14, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soe, M.M.; Sullivan, K.M. Documentation of Sample Size for Comparing Two Means. 2005. Available online: https://www.openepi.com/PDFDocs/SSMeanDoc.pdf (accessed on 20 April 2021).
- Sevón, L.; Laine, M.A.; Karjalainen, S.; Doroguinskaia, A.; Helenius, H.; Kiss, E.; Lehtonen-Veromaa, M. Effect of Age on Flow-Rate, Protein and Electrolyte Composition of Stimulated Whole Saliva in Healthy, Non-Smoking Women. Open Dent. J. 2008, 2, 89. [Google Scholar] [CrossRef] [Green Version]
- Yousefi, M.; Parvaie, P.; Riahi, S.M. Systematic Review Salivary Factors Related to Caries in Pregnancy A Systematic Review and Meta-Analysis. J. Am. Dent. Assoc. 2020, 151, 576–588. [Google Scholar] [CrossRef]
- Nieuw Amerongen, A.V.; Veerman, E.C.I. Saliva—The defender of the oral cavity. Oral Dis. 2002, 8, 12–22. [Google Scholar] [CrossRef] [Green Version]
- Dawes, C. What is the critical pH and why does a tooth dissolve in acid? J. Can. Dent. Assoc. 2003, 69, 722–724. [Google Scholar]
- Chan, M.; WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; World Health Organization: Geneva, Switzerland, 2011.
- Naveen, S.; Asha, M.L.; Shubha, G.; Bajoria, A.A.; Jose, A.A. Salivary Flow Rate, pH and Buffering Capacity in Pregnant and Non Pregnant Women-A Comparative Study. JMED Res. 2014, 2014, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Migliario, M.; Bindi, D.; Surico, A.; DE Deprini, S.; Minsenti, F.; Pezzotti, B.; Melle, P.L.F.B. Changes in salivary flow rate and pH in pregnancy. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1804–1810. [Google Scholar] [PubMed]
- Rakchanok, N.; Amporn, D.; Yoshida, Y.; Harun-Or-Rashid, M.D.; Sakamoto, J. Dental caries and gingivitis among pregnant and non-pregnant women in Chiang Mai, Thailand. Nagoya J. Med. Sci. 2010, 72, 43–50. [Google Scholar] [PubMed]
- Lasisi, T.J.; Ugwuadu, P.N. Pregnancy related changes in human salivary secretion and composition in a Nigerian population. Afr. J. Med. Med. Sci. 2014, 43, 347–351. [Google Scholar] [PubMed]
- Zhou, J.; Jiang, N.; Wang, Z.; Li, L.; Zhang, J.; Ma, R.; Nie, H.; Li, Z. Influences of pH and iron concentration on the salivary microbiome in individual humans with and without caries. Appl. Environ. Microbiol. 2017, 83, e02412-16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guimares, A.N.; Silva-Mato, A.; Siqueira, F.M.; Cyrino, R.M.; Cota, L.O.M.; Costa, F.O. Very low and low birth weight associated with maternal periodontitis. J. Clin. Periodontol. 2012, 39, 1024–1031. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.S.; Bhayat, A.; Zafar, M.S.; Al-Samadani, K.H. The Impact of Hyposalivation on Quality of Life (QoL) and Oral Health in the Aging Population of Al Madinah Al Munawarrah. Int. J. Environ. Res. Public Health 2017, 14, 445. [Google Scholar] [CrossRef] [Green Version]
- Rubana, I.E.; Aulik, I.V. Buffer function of hemoglobin. Res. Sport. Med. Int. J. 2009, 1, 125–126. [Google Scholar] [CrossRef]
- Schroth, R.J.; Levi, J.; Kliewer, E.; Friel, J.; Moffatt, M.E.K. Association between iron status, iron deficiency anaemia, and severe early childhood caries: A case-control study. BMC Pediatr. 2013, 13, 22. [Google Scholar] [CrossRef] [Green Version]
- Abdallah, M.A.; Abed, H.H.; Hamza, G.; Alsahafi, E.N. The association between dmft index and haemoglobin levels in 3-6 year-old Saudi children with anaemia: A cross sectional study. J. Taibah Univ. Med. Sci. 2016, 11, 72–76. [Google Scholar] [CrossRef] [Green Version]
- Hashemi, A.; Bahrololoomi, Z.; Pediatric SSIJ. Undefined Relationship between Early Childhood Caries and Anemia: A Systematic Review. 2018. Available online: https://www.semanticscholar.org/paper/Relationship-Between-Early-Childhood-Caries-and-A-Hashemi-Bahrololoomi/404e665e2fd99db8077fa94452a09e06e3992a97 (accessed on 21 April 2023).
- Mahantesha, T.; Parveen Reddy, K.M.; Ellore, V.P.K.; Ramagoni, N.K.; Iitagi, V.; Anitha, K.S. Evaluation and association of iron deficiency anaemia with salivary pH and buffering capacity. Natl. J. Physiol. Pharm. Pharmacol. 2014, 4, 229. [Google Scholar] [CrossRef]
- Lilienthal, B. Buffering systems in the mouth. Oral Surg. Oral Med. Oral Pathol. 1955, 8, 828–841. [Google Scholar] [CrossRef] [PubMed]
- Koppolu, P.; Sirisha, S.; Penala, S.; Reddy, P.K.; Alotaibi, D.H.; Abusalim, G.S.; Lingam, A.S.; Mukhtar, A.H.; Barakat, A.; AlMokhatieb, A.A. Correlation of Blood and Salivary pH Levels in Healthy, Gingivitis, and Periodontitis Patients before and after Non-Surgical Periodontal Therapy. Diagnostics 2022, 12, 97. [Google Scholar] [CrossRef]
- Easwaran, H.N.; Annadurai, A.; Muthu, M.S.; Sharma, A.; Patil, S.S.; Jayakumar, P.; Jagadeesan, A.; Nagarajan, U.; Pasupathy, U.; Wadgave, U. Early Childhood Caries and Iron Deficiency Anaemia: A Systematic Review and Meta-Analysis. Caries Res. 2022, 56, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Bakhshi, M.; Sabet, M.S.; Hashemi, E.S.; Bakhtiari, S.; Tofangchiha, M.; Marhabi, S.A.; Alirezaei, S. Evaluation of biochemical changes in unstimulated salivary, calcium, phosphorous and total protein during pregnancy. Afr. J. Biotechnol. 2012, 11, 2078–2082. [Google Scholar]
- Bhattarai, K.R.; Kim, H.R.; Chae, H.J. Compliance with Saliva Collection Protocol in Healthy Volunteers: Strategies for Managing Risk and Errors. Int. J. Med. Sci. 2018, 15, 823. [Google Scholar] [CrossRef] [Green Version]
- Aps, J.K.M.; Martens, L.C. Review: The physiology of saliva and transfer of drugs into saliva. Forensic. Sci. Int. 2005, 150, 119–131. [Google Scholar] [CrossRef]
- Hara, A.T.; Karlinsey, R.L.; Zero, D.T. Dentine remineralisation by simulated saliva formulations with different Ca and Pi contents. Caries Res. 2008, 42, 51–56. [Google Scholar] [CrossRef]
- Navazesh, M. Methods for collecting saliva. Ann. N. Y. Acad. Sci. 1993, 694, 72–77. [Google Scholar] [CrossRef]
- Greenhalgh, T. How to read a paper. Getting Your Bearings (Deciding What the Paper Is About). Br. Med. J. 1997, 315, 243. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-Pregnant (n = 20) | Pregnant (n = 60) | p-Value | |||
|---|---|---|---|---|---|
| Mean ± SD | |||||
| Weight (kg) | 63.6 ± 12.13 | 66.18 ± 9.94 | 0.344 | ||
| Height (cm) | 157.95 ± 9.93 | 157.26 ± 7.33 | 0.743 | ||
| Frequency (%) | Frequency (%) | ||||
| BMI | Underweight (<18.5) | 6 (30) | 1 (1.67) | ||
| Normal weight (18.5–24.9) | 12 (60) | 17 (28.33) | |||
| Overweight (25–29.9) | 2 (10) | 34 (56.67) | |||
| Obese (30–39.9) | 0 (0) | 8 (13.33) | |||
| Hb levels | Severe anemia (<7 g/dL) | 0 (0) | |||
| Moderate (7–9.9 g/dL) | 3 (5) | ||||
| Mild (10–10.9 g/dL) | 20 (33.33) | ||||
| Non-anemic (≥11 g/dL) | 37 (61.67) | ||||
| Non-Pregnant (n = 20) | (Pregnant n = 60) | |||
|---|---|---|---|---|
| Median (IQR) | Median (IQR) | z-Value | Exact p-Value | |
| Saliva [Ca2+] mmol/L | 1.41 (1.06–1.79) | 1.03 (0.86–1.25) | −3.145 | 0.001 |
| Saliva [PO43−] mmol/L | 5.17 (4.14–6.27) | 2.94 (1.68–6.17) | −1.733 | 0.084 |
| Mean ± (SD) | t-value | p-value | ||
| Saliva pH | 6.67 (0.36) | 6.38 (0.49) | −2.49 | 0.015 |
| Non-pregnant | First trimester | Second trimester | Third trimester | |
| [Ca2+]/[PO43−] ratios (Mean ± SD) | 0.35 ± 0.31 | 0.33 ± 0.33 | 0.40 ± 0.32 | 0.53 ± 0.36 |
| Correlation between saliva pH and [Ca2+]/[PO43−] ratios | Spearman’s r | 95% Confidence Interval of r | p-value | |
| −0.274 | −0.471 to −0.051 | 0.014 | ||
| Variable | (H) | Degree of Freedom | p-Value | |
|---|---|---|---|---|
| Saliva [Ca2+] mmol/L | 9.91 | 3 | 0.019 ** | |
| Saliva [PO43−] mmol/L | 12.36 | 3 | 0.006 ** | |
| R2 | F | |||
| Saliva pH | 0.3932 | 16.42 | 3.76 | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mbembela, O.; Ngarashi, D.; Nyamuryekung’e, K.K. Biochemical Changes in Salivary pH and Its Correlation to Hemoglobin Levels, Calcium and Phosphate Ion Concentrations among Pregnant Women, Tanzania: A Cross-Sectional Study. Oral 2023, 3, 325-336. https://doi.org/10.3390/oral3030027
Mbembela O, Ngarashi D, Nyamuryekung’e KK. Biochemical Changes in Salivary pH and Its Correlation to Hemoglobin Levels, Calcium and Phosphate Ion Concentrations among Pregnant Women, Tanzania: A Cross-Sectional Study. Oral. 2023; 3(3):325-336. https://doi.org/10.3390/oral3030027
Chicago/Turabian StyleMbembela, Oscar, Davis Ngarashi, and Kasusu Klint Nyamuryekung’e. 2023. "Biochemical Changes in Salivary pH and Its Correlation to Hemoglobin Levels, Calcium and Phosphate Ion Concentrations among Pregnant Women, Tanzania: A Cross-Sectional Study" Oral 3, no. 3: 325-336. https://doi.org/10.3390/oral3030027
APA StyleMbembela, O., Ngarashi, D., & Nyamuryekung’e, K. K. (2023). Biochemical Changes in Salivary pH and Its Correlation to Hemoglobin Levels, Calcium and Phosphate Ion Concentrations among Pregnant Women, Tanzania: A Cross-Sectional Study. Oral, 3(3), 325-336. https://doi.org/10.3390/oral3030027