
The COMPASS-COVID-19-ICU Study: Identification of Factors to Predict the Risk of Intubation and Mortality in Patients with Severe COVID-19

 ,
, 
 , ,
, ,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Biomarkers of Hypercoagulability, Endothelial Activation and Inflammation
2.3. Statistical Analysis
3. Results
3.1. Hypercoagulability, Cellular Activation and Inflammation Biomarkers
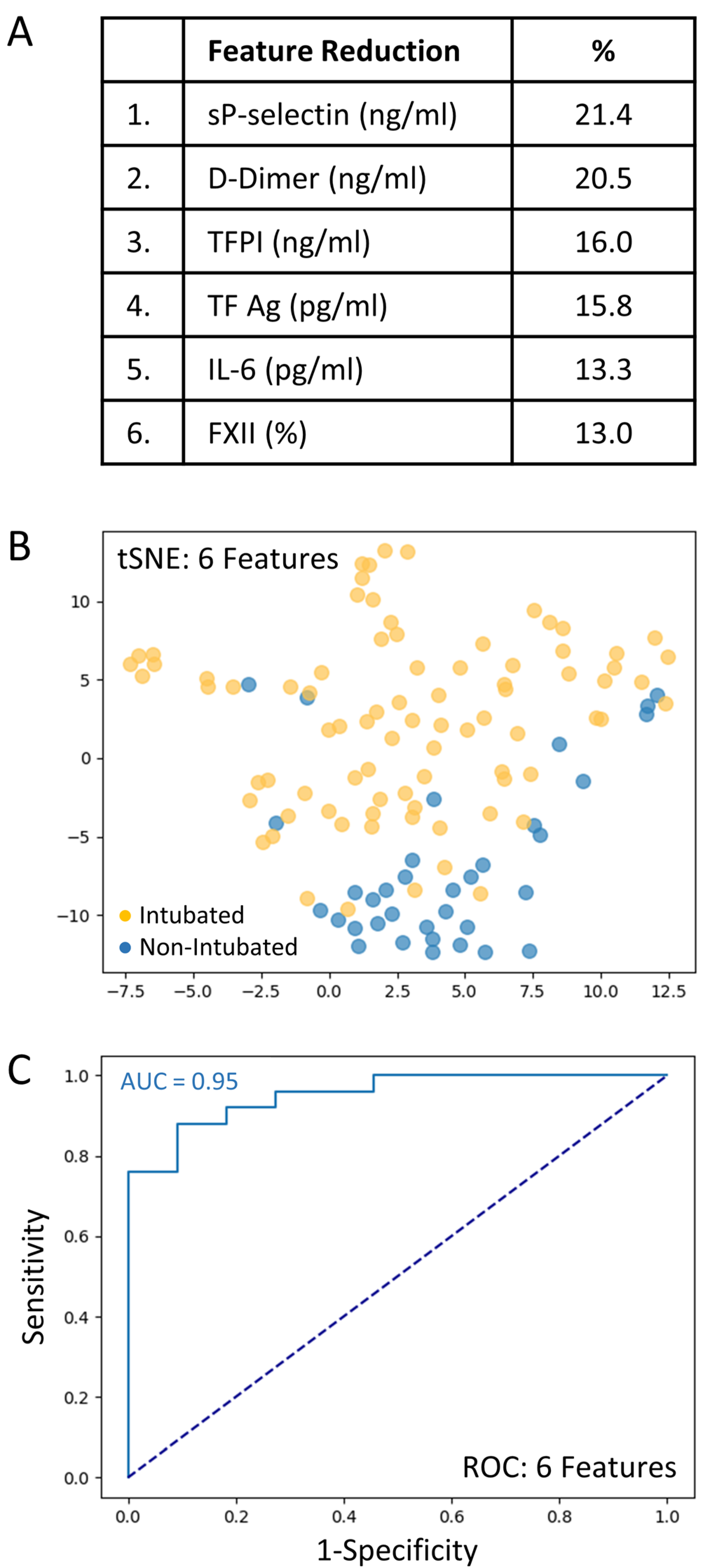
3.2. Risk Assessment for Intubation Using Machine Learning
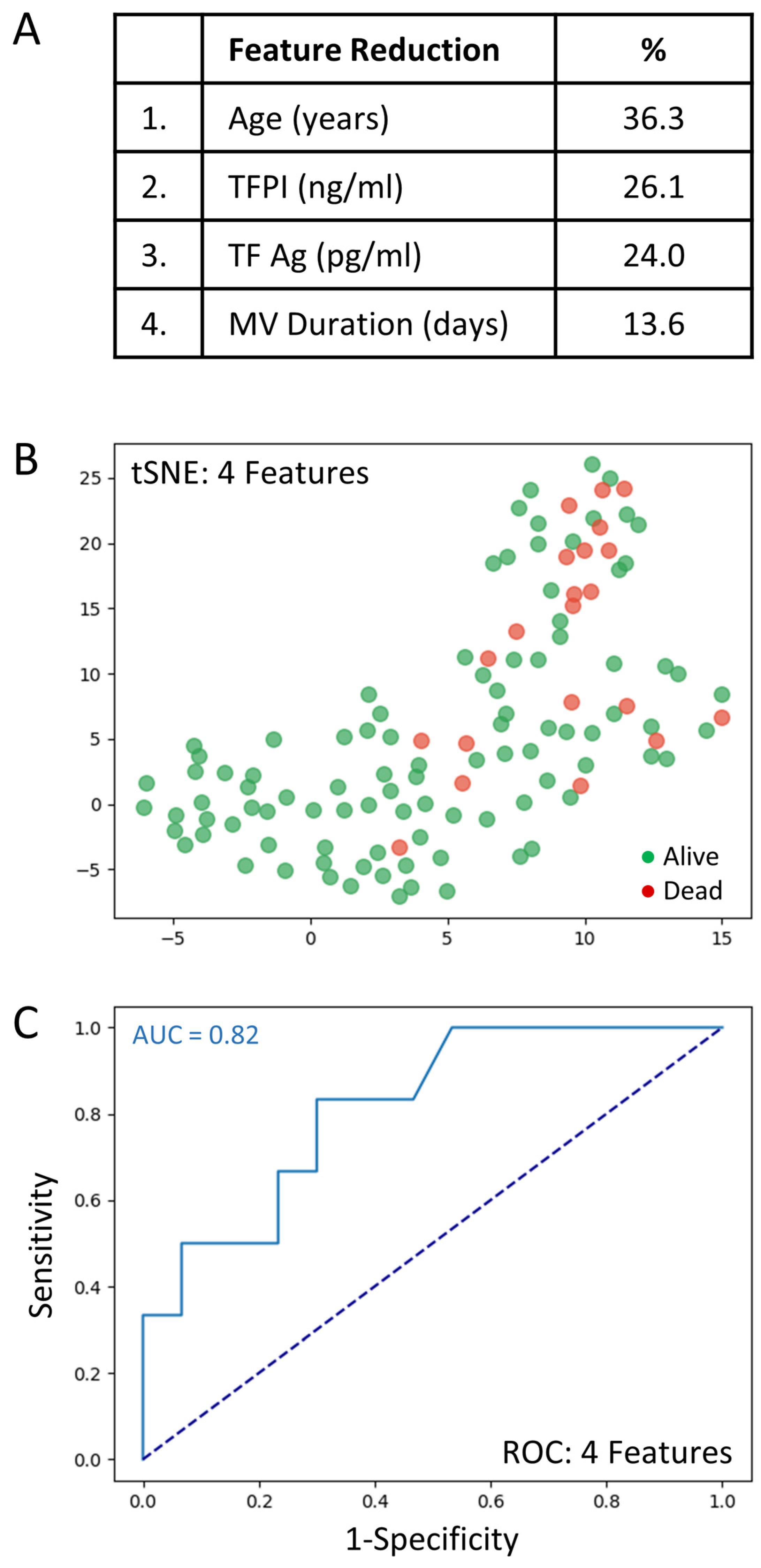
3.3. Risk Assessment for Death Using Machine Learning
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Cui, J.; Li, F.; Shi, Z.-L. Origin and evolution of pathogenic coronaviruses. Nat. Rev. Microbiol. 2019, 17, 181–192. [Google Scholar] [CrossRef] [Green Version]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.-M.; Wang, W.; Song, Z.-G.; Hu, Y.; Tao, Z.-W.; Tian, J.-H.; Pei, Y.-Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Wan, Y.; Shang, J.; Graham, R.; Baric, R.S.; Li, F. Receptor Recognition by the Novel Coronavirus from Wuhan: An Analysis Based on Decade-Long Structural Studies of SARS Coronavirus. J. Virol. 2020, 94, e00127-20. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.J.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef]
- Vaarala, M.H.; Porvari, K.S.; Kellokumpu, S.; Kyllönen, A.P.; Vihko, P.T. Expression of transmembrane serine protease TMPRSS2 in mouse and human tissues. J. Pathol. 2001, 193, 134–140. [Google Scholar] [CrossRef]
- Fraser, D.D.; Cepinskas, G.; Slessarev, M.; Martin, C.; Daley, M.; Miller, M.R.; O’Gorman, D.B.; Gill, S.E.; Patterson, E.K.; dos Santos, C.C. Inflammation Profiling of Critically Ill Coronavirus Disease 2019 Patients. Crit. Care Explor. 2020, 2, e0144. [Google Scholar] [CrossRef]
- Han, H.; Ma, Q.; Li, C.; Liu, R.; Zhao, L.; Wang, W.; Zhang, P.; Liu, X.; Gao, G.; Liu, F.; et al. Profiling serum cytokines in COVID-19 patients reveals IL-6 and IL-10 are disease severity predictors. Emerg. Microbes Infect. 2020, 9, 1123–1130. [Google Scholar] [CrossRef] [PubMed]
- Song, W.-C.; Fitzgerald, G.A. COVID-19, microangiopathy, hemostatic activation, and complement. J. Clin. Investig. 2020, 130, 3950–3953. [Google Scholar] [CrossRef] [PubMed]
- Colman, R.W.; Schmaier, A.H. Contact system: A vascular biology modulator with anticoagulant, profibrinolytic, antiadhesive, and proinflammatory attributes. Blood 1997, 90, 3819–3843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maglakelidze, N.; Manto, K.M.; Craig, T.J. A Review: Does Complement or the Contact System Have a Role in Protection or Pathogenesis of COVID-19? Pulm. Ther. 2020, 6, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Baker, C.J.; Smith, S.A.; Morrissey, J.H. Polyphosphate in thrombosis, hemostasis, and inflammation. Res. Pract. Thromb. Haemost. 2018, 3, 18–25. [Google Scholar] [CrossRef]
- Yang, H.; Xie, W.; Xue, X.; Yang, K.; Ma, J.; Liang, W.; Zhao, Q.; Zhou, Z.; Pei, D.; Ziebuhr, J.; et al. Design of Wide-Spectrum Inhibitors Targeting Coronavirus Main Proteases. PLoS Biol. 2005, 3, e324. [Google Scholar] [CrossRef]
- Maas, C.; Renné, T. Coagulation factor XII in thrombosis and inflammation. Blood 2018, 131, 1903–1909. [Google Scholar] [CrossRef] [Green Version]
- Goodall, K.; Poon, I.; Phipps, S.; Hulett, M.D. Soluble Heparan Sulfate Fragments Generated by Heparanase Trigger the Release of Pro-Inflammatory Cytokines through TLR-4. PLoS ONE 2014, 9, e109596. [Google Scholar] [CrossRef]
- Fraser, D.D.; Patterson, E.K.; Slessarev, M.; Gill, S.E.; Martin, C.; Daley, M.; Miller, M.R.; Patel, M.A.; dos Santos, C.C.; Bosma, K.J.; et al. Endothelial Injury and Glycocalyx Degradation in Critically Ill Coronavirus Disease 2019 Patients: Implications for Microvascular Platelet Aggregation. Crit. Care Explor. 2020, 2, e0194. [Google Scholar] [CrossRef]
- Nadir, Y.; Brenner, B. Relevance of Heparan Sulfate and Heparanase to Severity of COVID-19 in the Elderly. Semin. Thromb. Hemost. 2021, 47, 348–350. [Google Scholar] [CrossRef]
- Funtowicz, S.; Ravetz, J. Post-normal science. In Encyclopedia of Ecological Economics; International Society for Ecological Economics: Boston, MA, USA, 2003. [Google Scholar]
- Massaro, G.; Lecis, D.; Martuscelli, E.; Chiricolo, G.; Sangiorgi, G.M. Clinical Features and Management of COVID-19-Associated Hypercoagulability. Card Electrophysiol. Clin. 2022, 14, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Gerotziafas, G.T.; Sergentanis, T.N.; Voiriot, G.; Lassel, L.; Papageorgiou, C.; Elabbadi, A.; Turpin, M.; Vandreden, P.; Papageorgiou, L.; Psaltopoulou, T.; et al. Derivation and Validation of a Predictive Score for Disease Worsening in Patients with COVID-19. Thromb. Haemost. 2020, 120, 1680–1690. [Google Scholar] [CrossRef] [PubMed]
- van Dam, P.M.E.L.; Zelis, N.; van Kuijk, S.M.J.; Linkens, A.E.M.J.H.; Brüggemann, R.A.G.; Spaetgens, B.; van der Horst, I.C.C.; Stassen, P.M. Performance of prediction models for short-term outcome in COVID-19 patients in the emergency department: A retrospective study. Ann. Med. 2021, 53, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Alimadadi, A.; Aryal, S.; Manandhar, I.; Munroe, P.B.; Joe, B.; Cheng, X. Artificial intelligence and machine learning to fight COVID-19. Physiol. Genom. 2020, 52, 200–202. [Google Scholar] [CrossRef] [PubMed]
- Fraser, D.D.; Slessarev, M.; Martin, C.M.; Daley, M.; Patel, M.A.; Miller, M.R.; Patterson, E.K.; O’Gorman, D.B.; Gill, S.E.; Wishart, D.S.; et al. Metabolomics Profiling of Critically Ill Coronavirus Disease 2019 Patients: Identification of Diagnostic and Prognostic Biomarkers. Crit. Care Explor. 2020, 2, e0272. [Google Scholar] [CrossRef]
- Fraser, D.D.; Cepinskas, G.; Patterson, E.K.; Slessarev, M.; Martin, C.; Daley, M.; Patel, M.A.; Miller, M.R.; O’Gorman, D.B.; Gill, S.E.; et al. Novel Outcome Biomarkers Identified with Targeted Proteomic Analyses of Plasma from Critically Ill Coronavirus Disease 2019 Patients. Crit. Care Explor. 2020, 2, e0189. [Google Scholar] [CrossRef]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.P.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.-J.; Martin, I.B.; et al. The role of chest imaging in patient management during the COVID-19 pandemic: A multinational consensus statement from the fleischner Society. Chest 2020, 158, 106–116. [Google Scholar] [CrossRef]
- Phua, J.; Weng, L.; Ling, L.; Egi, M.; Lim, C.-M.; Divatia, J.V.; Shrestha, B.R.; Arabi, Y.M.; Ng, J.; Gomersall, C.D.; et al. Intensive care management of coronavirus disease 2019 (COVID-19): Challenges and recommendations. Lancet Respir. Med. 2020, 8, 506–517. [Google Scholar] [CrossRef]
- Hendriksen, J.M.T.; Geersing, G.J.; Moons, K.G.M.; de Groot, J. Diagnostic and prognostic prediction models. J. Thromb. Haemost. 2013, 11, 129–141. [Google Scholar] [CrossRef]
- Harrell, F.E., Jr.; Lee, K.L.; Mark, D.B. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Tang, C.; Garreau, D.; Luxburg, U. When do random forests fail? In Proceedings of the 32nd International Conference on Neural Information Processing Systems, Montréal, QC, Canada, 3–8 December 2018; Curran Associates Inc.: Red Hook, NY, USA, 2018; pp. 2987–2997. [Google Scholar]
- Hastie, T.; Tibshirani, R.; Friedman, J. The Elements of Statistical Learning, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2008; ISBN 0-387-95284-5. [Google Scholar]
- Cawley, C.G.; Talbot, N.L.C. On Over-fitting in Model Selection and Subsequent Selection Bias in Performance Evaluation. J. Mach. Learn. Res. 2010, 11, 2079–2107. [Google Scholar]
- Kursa, M.; Rudnicki, W. Feature Selection with the Boruta Package. J. Stat. Softw. 2010, 36, i02. [Google Scholar] [CrossRef] [Green Version]
- van der Maaten, L.; Hinton, G. Visualizing data using t-SNE. J. Mach. Learn. Res. 2008, 9, 2579–2605. [Google Scholar]
- Zhu, W.; Zeng, N.; Wang, N. Sensitivity, specificity, accuracy, associated confidence interval and ROC analysis with practical SAS® implementations. In Proceedings of the NESUG Proceedings: Health Care and Life Sciences, Baltimore, MD, USA, 14–17 November 2010; Available online: https://www.lexjansen.com/nesug/nesug10/hl/hl07.pdf (accessed on 4 March 2022).
- Wygrecka, M.; Birnhuber, A.; Seeliger, B.; Michalick, L.; Pak, O.; Schultz, A.-S.; Schramm, F.; Zacharias, M.; Gorkiewicz, G.; David, S.; et al. Altered fibrin clot structure and dysregulated fibrinolysis contribute to thrombosis risk in severe COVID-19. Blood Adv. 2021, 6, 1074–1087. [Google Scholar] [CrossRef]
- Ceballos, F.C.; Ryan, P.; Blancas, R.; Martin-Vicente, M.; Vidal-Alcántara, E.J.; Peréz-García, F.; Bartolomé, S.; Churruca-Sarasqueta, J.; Virseda-Berdices, A.; Martínez-González, O.; et al. Are Reduced Levels of Coagulation Proteins Upon Admission Linked to COVID-19 Severity and Mortality? Front. Med. 2021, 8, 718053. [Google Scholar] [CrossRef]
- Englert, H.; Rangaswamy, C.; Deppermann, C.; Sperhake, J.-P.; Krisp, C.; Schreier, D.; Gordon, E.; Konrath, S.; Haddad, M.; Pula, G.; et al. Defective NET clearance contributes to sustained FXII activation in COVID-19-associated pulmonary thrombo-inflammation. EBioMedicine 2021, 67, 103382. [Google Scholar] [CrossRef]
- Gerotziafas, G.T.; Catalano, M.; Colgan, M.-P.; Pecsvarady, Z.; Wautrecht, J.C.; Fazeli, B.; Olinic, D.-M.; Farkas, K.; Elalamy, I.; Falanga, A.; et al. Guidance for the Management of Patients with Vascular Disease or Cardiovascular Risk Factors and COVID-19: Position Paper from VAS-European Independent Foundation in Angiology/Vascular Medicine. Thromb. Haemost. 2020, 120, 1597–1628. [Google Scholar] [CrossRef]
- Short, S.A.P.; Gupta, S.; Brenner, S.K.; Hayek, S.S.; Srivastava, A.; Shaefi, S.; Singh, H.; Wu, B.; Bagchi, A.; Al-Samkari, H.; et al. d-dimer and Death in Critically Ill Patients with Coronavirus Disease 2019. Crit. Care Med. 2021, 49, e500–e511. [Google Scholar] [CrossRef]
- Gris, J.; Quéré, I.; Pérez-Martin, A.; Lefrant, J.; Sotto, A. Uncertainties on the prognostic value of D-dimers in COVID-19 patients. J. Thromb. Haemost. 2020, 18, 2066–2067. [Google Scholar] [CrossRef]
- Zhang, L. Response to “Uncertainties on the prognostic value of D-dimers in COVID-19 patients”. J. Thromb. Haemost. 2020, 18, 2067–2068. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated with Mortality among Patients with COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef]
- Liu, Q.; Huang, N.; Li, A.; Zhou, Y.; Liang, L.; Song, X.; Yang, Z.; Zhou, X. Effect of low-dose aspirin on mortality and viral duration of the hospitalized adults with COVID-19. Medicine 2021, 100, e24544. [Google Scholar] [CrossRef] [PubMed]
- Chow, J.H.; Khanna, A.K.; Kethireddy, S.; Yamane, D.; Levine, A.; Jackson, A.M.; McCurdy, M.T.; Tabatabai, A.; Kumar, G.; Park, P.; et al. Aspirin Use Is Associated with Decreased Mechanical Ventilation, Intensive Care Unit Admission, and In-Hospital Mortality in Hospitalized Patients with Coronavirus Disease 2019. Anesthesia Analg. 2021, 132, 930–941. [Google Scholar] [CrossRef] [PubMed]
- Billett, H.H.; Reyes-Gil, M.; Szymanski, J.; Ikemura, K.; Stahl, L.R.; Lo, Y.; Rahman, S.; Gonzalez-Lugo, J.D.; Kushnir, M.; Barouqa, M.; et al. Anticoagulation in COVID-19: Effect of Enoxaparin, Heparin, and Apixaban on Mortality. Thromb. Haemost. 2020, 120, 1691–1699. [Google Scholar] [CrossRef]
- Tang, N.; Bai, H.; Chen, X.; Gong, J.; Li, D.; Sun, Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J. Thromb. Haemost. 2020, 18, 1094–1099. [Google Scholar] [CrossRef]
- Parisi, R.; Costanzo, S.; Di Castelnuovo, A.; de Gaetano, G.; Donati, M.B.; Iacoviello, L. Different Anticoagulant Regimens, Mortality, and Bleeding in Hospitalized Patients with COVID-19: A Systematic Review and an Updated Meta-Analysis. Semin. Thromb. Hemost. 2021, 47, 372–391. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variables | ICU-COVID-19 Patients (n = 118) |
|---|---|
| Demographic Data | |
| Age (age in years) | 62.0 (52.3, 70.0) |
| Sex (male) | 82/118 (69%) |
| Body mass index | 27.6 (25.6, 30.1) |
| Cardiovascular risk factors and disease | |
| Obesity (BMI > 30) | 15/118 (13%) |
| Diabetes | 37/118 (31%) |
| Hypertension | 70/118 (59%) |
| Cardiovascular disease | 26/118 (22%) |
| Stroke | 74/118 (63%) |
| Obliterating arterial disease of the lower limbs | 4/118 (3%) |
| Acute myocardial infraction | 17/118 (14%) |
| Regular tobacco use | 10/118 (8%) |
| Non-vascular comorbidities | |
| Active cancer | 4/118 (3%) |
| Chronic Renal Disease | 9/118 (8%) |
| Dialysis in patients with chronic renal disease | 6/118 (5%) |
| Acute renal failure | 18/118 (15%) |
| Dialysis in patients with acute renal failure | 8/118 (7%) |
| Chronic obstructive pulmonary disease | 4/118 (3%) |
| Chronic respiratory insufficiency | 9/118 (8%) |
| Sickle cell anemia | 2/118 (2%) |
| Personal history of VTE | 3/118 (3%) |
| Antithrombotic treatment before hospital admission | |
| Anticoagulant treatment | 5/118 (4%) |
| Antiplatelet treatment | 26/118 (22%) |
| ICU related complication | |
| Hemoptysis | 3/118 (3%) |
| Choc | 53/118 (45%) |
| EER Dialysis | 23/118 (19%) |
| All Infections | 47/118 (40%) |
| Outcome | |
| Death | 21/118 (18%) |
| Intubation | 83/118 (70%) |
| Normal Reference Range | Control Group (n = 30) | ICU-COVID-19 Patients (n = 118) | |
|---|---|---|---|
| Complete blood count | |||
| Red blood cell count ×106/μL | 4.32–5.72 | 4.20 (2.82–6.32) | 4.17 (2.46–6.07) |
| White blood cell count | 4.0–10.0 | 6.20 (3.87–8.43) | 7.88 (2.20–72.46) * |
| Hematocrit (%) | 35.0–47.0 | 39 (38–46) | 34 (21–46) |
| Hemoglobin (g/dL) | 12.0–16.0 | 11.6 (12.2–14.3) | 11.9 (7–15.8) |
| Platelet count (×109/L) | 150–400 | 220 (180–350) | 214 (48–490) ** |
| Neutrophil count (%) | 1.5–7.0 | 4.5 (2.2–7.5) | 6.3 (0.78–21.6) * |
| Eosinophils (×109/L) | 0.03–0.7 | 0.05 (0.02–0.09) | 0.01 (0–0.84) |
| Basophil count (%) | <0.1 | 0.3 (0.1–0.6) | 1.0 (0–1) * |
| Lymphocyte count (%) | 1.5–4.0 | 2.10 ± 0.96 (1.8–2.12) | 0.75 (0.13–1110) * |
| Monocyte count (%) | 0.1–1.0 | 0.11 (0.1–0.3) | 0.29 (0.07–5.8) * |
| Routine coagulation tests | |||
| aPTT (ratio Patient/Control) | <1.21 | 1.11 (0.9–1.2) | 1.24 (0.81–3.02) * |
| PT (s) | <13.6 s | 11.2 (10–12) | 14.7 (11.9–34.7) * |
| Fibrinogen (g/L) | 1.8–4.0 | 2.41 ± (2–4) | 6.97 (3.95–10.0) * |
| Thrombin generation parameters | |||
| lag-time (min) | 2.1–3.8 | 2.5 (2.4–3.2) | 2.59 (1.4–5.7) |
| tt-Peak (min) | 4.0–6.6 | 5.0 (4–5.8) | 5.0 (3.1–16.7) |
| Peak (nM) | 222–330 | 284 (230–300) | 253 (12–463) ** |
| MRI (nM/min) | 60–120 | 109 (80–120) | 107 (2–250) |
| ETP (nMxmin) | 1000–1900 | 1520 (1200–1800) | 1077 (115–2170) * |
| Intrinsic and extrinsic clotting pathway parameters | |||
| Factor V (%) | 70–120 | 90 (80–110) | 121 (42–214) * |
| Factor VIIa (U/mL) | 65–130 | 75 (68–120) | 24 (3–188) * |
| Factor VIII (%) | 50–150 | 110 (90–120) | 143.0 (50–600) * |
| Factor XII (%) | 80–120 | 105 (85–115) | 70 (30–178) * |
| Natural coagulation inhibitors | |||
| Protein C (%) | 68–110 | 99 (85–110) | 93 (46–140) * |
| Protein S (%) | 70–115 | 86 (75–110) | 59 (10–112) * |
| TFPI (ng/mL) | 8–12 | 10 (9–11) | 31 (10–460) * |
| ATIII (%) | 80–120 | 98 (90–110) | 92 (51–131) ** |
| Fibrin degradation products | |||
| D-Dimers (μg/mL) | <0.50 | 0.3 (0.2–0.4) | 1723 (305–20,000) * |
| Fibrin Monomer (μg/mL) | 0.5–5.50 | 2.5 (1.5–3.3) | 5 (5–150) * |
| Procoagulant phospholipids and platelet activation | |||
| PPL—ct (s) | 42–85 | 63 (55–78) | 32 (13–68) * |
| P-selectin (ng/mL) | 82–42 | 63 (50–75) | 28 (10–71) * |
| Endothelial cell activation | |||
| Factor von Willebrand (%) | 70–150 | 90 (70–110) | 331 (43–764) * |
| TF (pg/mL) | 35–60 | 49 (35–60) | 71 (17–323) * |
| TM (ng/mL)) | 70–120 | 90 (75–110) | 72 (37–482) |
| MP-TF+ (pg/mL) | 0.05–1.00 | 0.85 (0.6–1) | 1.90 (1.1–7.5) * |
| Heparanase (ng/mL) | 0.08–0.16 | 0.1 (0.8–1.15) | 0.15 (0.1–3.1) |
| Complement—Cytokine—Kininogen | |||
| HMWK (µg/mL) | 70–90 | 77 (70–85) | 167 (89–800) * |
| C3a (ng/mL) | 880–2870 | 2100 (1200–2700) | 14,903 (1587–53,602) * |
| C5a (ng/mL) | 4.7–9.5 | 5.8 (4.8–9.2) | 6.1 (1.6–63.6) * |
| IL-6 (pg/mL) | 0–5 | 1.2 (0.8–1.5 | 15.6 (0.1–693) * |
| Variable | No Intubation (n = 35) | Intubation (n = 83) | p-Value * |
|---|---|---|---|
| sP-Selectin (ng/mL) | 19.5 (15.6, 27.5) | 29.9 (23.6, 41.1) | <0.0001 |
| D-Dimer (ng/mL) | 1124.0 (747.5, 1956.5) | 1878.0 (1448.0, 3243.0) | 0.0001 |
| TFPI free (ng/mL) | 20.5 (18.7, 28.2) | 39.4 (27.0, 58.5) | <0.0001 |
| TF Ag (pg/mL) | 54.7 (42.8, 66.8) | 80.5 (59.9, 102.2) | <0.0001 |
| IL-6 (pg/mL) | 5.0 (1.3, 11.1) | 29.7 (7.9, 76.6) | <0.0001 |
| FXII (%) | 84.0 (73.5, 94.0) | 62.0 (47.0, 73.0) | <0.0001 |
| Variable | Alive (n = 97) | Dead (n = 21) | p-Value * |
|---|---|---|---|
| Age (years) | 60 (51, 66) | 73 (70, 77) | <0.0001 |
| TFPI free (ng/mL) | 28.6 (20.8, 50.1) | 40.0 (35.4, 48.6) | 0.057 |
| TF Ag (pg/mL) | 66.4 (53.4, 94.6) | 89.5 (70.0, 115.4) | 0.044 |
| Duration of hospitalization in ICU (days) | 0 (0, 0) | 8 (0, 8) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gerotziafas, G.T.; Van Dreden, P.; Fraser, D.D.; Voiriot, G.; Patel, M.A.; Daley, M.; Elabbadi, A.; Rousseau, A.; Prassas, Y.; Turpin, M.; et al. The COMPASS-COVID-19-ICU Study: Identification of Factors to Predict the Risk of Intubation and Mortality in Patients with Severe COVID-19. Hemato 2022, 3, 204-218. https://doi.org/10.3390/hemato3010017
Gerotziafas GT, Van Dreden P, Fraser DD, Voiriot G, Patel MA, Daley M, Elabbadi A, Rousseau A, Prassas Y, Turpin M, et al. The COMPASS-COVID-19-ICU Study: Identification of Factors to Predict the Risk of Intubation and Mortality in Patients with Severe COVID-19. Hemato. 2022; 3(1):204-218. https://doi.org/10.3390/hemato3010017
Chicago/Turabian StyleGerotziafas, Grigoris T., Patrick Van Dreden, Douglas D. Fraser, Guillaume Voiriot, Maitray A. Patel, Mark Daley, Alexandre Elabbadi, Aurélie Rousseau, Yannis Prassas, Matthieu Turpin, and et al. 2022. "The COMPASS-COVID-19-ICU Study: Identification of Factors to Predict the Risk of Intubation and Mortality in Patients with Severe COVID-19" Hemato 3, no. 1: 204-218. https://doi.org/10.3390/hemato3010017
APA StyleGerotziafas, G. T., Van Dreden, P., Fraser, D. D., Voiriot, G., Patel, M. A., Daley, M., Elabbadi, A., Rousseau, A., Prassas, Y., Turpin, M., Marchetti, M., Papageorgiou, L., Terpos, E., Dimopoulos, M. A., Falanga, A., Fareed, J., Fartoukh, M., & Elalamy, I. (2022). The COMPASS-COVID-19-ICU Study: Identification of Factors to Predict the Risk of Intubation and Mortality in Patients with Severe COVID-19. Hemato, 3(1), 204-218. https://doi.org/10.3390/hemato3010017