Abstract
Genetic risk information has relevance for patients’ blood relatives. However, cascade testing uptake in at-risk families is <50%. International research supports direct notification of at-risk relatives by health professionals (HPs), with patient consent. However, HPs express concerns about the privacy implications of this practice. Our privacy analysis, grounded in a clinically relevant hypothetical scenario, considers the types of personal information involved in direct notification of at-risk relatives and the application of Australian privacy regulations. It finds that collecting relatives’ contact details, and using those details (with patient consent) to notify relatives of possible genetic risk, does not breach Australian privacy law, providing that HPs adhere to regulatory requirements. It finds the purported “right to know” does not prevent disclosure of genetic information to at-risk relatives. Finally, the analysis confirms that the discretion available to HPs does not equate to a positive duty to warn at-risk relatives. Thus, direct notification of a patient’s at-risk relatives regarding medically actionable genetic information, with patient consent, is not a breach of Australian privacy regulations, providing it is conducted in accordance with the applicable principles set out. Clinical services should consider offering this service to patients where appropriate. National guidelines would assist with the clarification of the discretion for HPs.
Keywords:
privacy; genetics; ethics; genetic testing; cascade testing; medically actionable; risk notification; prevention Key Contribution:
Direct notification of patients’ relatives about their possible genetic risk by health professionals can support family communication and increase the uptake of cascade genetic testing for medically actionable conditions. Health professionals have historically had concerns about the privacy implications of this practice. This legal analysis considers the Commonwealth and state/territory privacy regulations in Australia; and concludes that this practice can be conducted in accordance with regulations in all jurisdictions.
1. Introduction
Genetic risk information has relevance for patients’ blood relatives, especially for medically actionable conditions. Health professionals (HPs) discuss the importance of risk notification with patients and commonly provide “family letters” for distribution to at-risk relatives. However, the uptake of cascade testing in at-risk families is <50% [1]. A recent Australian study [2] found relatives had not been notified of genetic risk in >50% of families. The burden of contacting relatives was identified as a significant barrier to notification, especially for affected patients, indicating a need for supported communication. One mechanism to assist with increased cascade testing uptake is direct notification of at-risk relatives by HPs, with patients’ consent. We note that disclosure of genetic results without patient consent is an important but separate topic, about which we have separately published [3].
The international literature supports the effectiveness of this practice, including strong public and patient support in multiple countries [1,4,5,6,7,8,9,10,11], with many studies recommending the consideration of direct contact of at-risk relatives by HPs. A 2022 systematic review and meta-analysis of 87 international studies found that direct contact increased the uptake of cascade genetic testing from 40% to 62% [12]. A 2016 Belgian study of BRCA1/2 families found that direct notification almost doubled the cascade testing rate [4]. Australian studies about familial hypercholesterolaemia (FH) (genetic high cholesterol), show strong support from the public [13] and patients [14] for direct notification. A 2006 South Australian study also demonstrated a significant increase in cascade testing uptake for cancer variants after direct notification by HPs, and received no complaints about breach of privacy from individuals who were contacted directly [15]. A recently published study by authors of this manuscript also demonstrated strong support for direct notification amongst >1000 members of the Australian public, including very few privacy concerns [16].
Despite strong international evidence for the effectiveness and acceptability of this practice, Australian HPs anecdotally express concerns about its privacy implications. There are no published legal analyses of this practice from an Australian privacy perspective, or published national guidelines, to guide and inform HPs regarding their discretion and obligations in this area.
2. Materials and Methods
Hypothetical case study
The following hypothetical case study (Figure 1) is used as the basis for this privacy analysis.
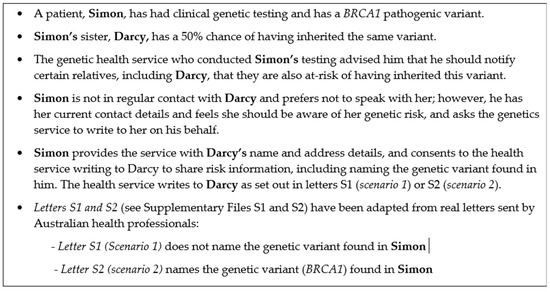
Figure 1.
Case study (hypothetical).
Legal analysis
This analysis will answer the following questions:
- 1.
- What are the relevant Australian Commonwealth and state/territory privacy regulations?
- 2.
- Are the types of information collected and used in Letters S1/S2 protected under privacy regulations?
- 3.
- Has the genetics service breached its privacy obligations by notifying Darcy directly in the hypothetical case study provided (Figure 1)?
This analysis is restricted to considering privacy implications of the collection, use and disclosure of personal information by HPs. It does not consider the impact of other regulations, such as restrictions on advertising or solicitation of business, that may apply to private HPs operating in a commercial setting.
3. Results
3.1. What Are the Relevant Australian Commonwealth and State/Territory Privacy Regulations?
The Privacy Act 1988 (Cth) (PA) is the key privacy legislation applicable to HPs working in the private sector in Australia, and includes 13 Australian Privacy Principles (APPs). Relevant regulations also exist in all Australian states and territories (some of which have specific privacy regimes) and apply to HPs working in the public (and, sometimes, private) sector.
Table 1 sets out the various pieces of legislation and regulations that apply across various states and territories in Australia.

Table 1.
Commonwealth, State and Territory regulations relevant to collection, use and disclosure of personal information (applied in Table 2).
It is clear that where patients freely consent to use or disclosure of their own personal information, there is no breach of their privacy. This assumes that consent to the disclosure has been properly obtained. In Supplementary Files S1 and S2, Simon has consented to the disclosure of his information and it is reasonable to assume that consent was properly obtained. Accordingly, this analysis will focus on Darcy’s privacy.
3.2. Are the Types of Information Collected and Used in Letters S1/S2 Protected under Privacy Regulations?
All “personal information” is protected under the PA. “Sensitive information” is a subset of personal information, and greater protection exists for information that is considered to be sensitive information (Figure 2). The State/Territory definitions are very similar.
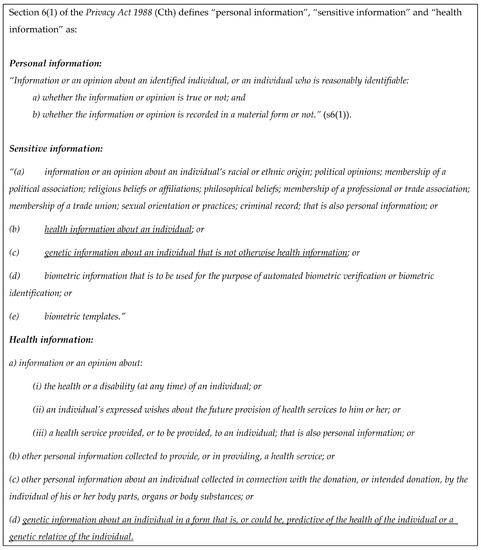
Figure 2.
Definitions of personal information, sensitive information, and health information.
There are two types of information that are being collected, used, and/or disclosed in this case study. The first type of information is Darcy’s contact details, and the second is the genetic information being included in the letter. This genetic information is both about Simon’s genetic status, and about Darcy’s possible genetic risk. In the discussion section we consider how the privacy regulations protect and regulate the use of this information.
The relevant Commonwealth APPs which apply to the collection, use, and/or disclosure of personal information in this context are APP 3 (Collection of solicited personal information), APP 5 (Notification of the collection of personal information) and APP 6 (Use or disclosure of personal information). Table 2 summarizes these APPs and their application to this question, as well as listing the applicable state/territory principles. Although the language in the state/territory regulations is not identical, their effect is the same with a few notable exceptions. Those exceptions are noted in Table 2 and described, where applicable, below.
Table 2.
Application of privacy regulations to collection, use or disclosure of contact information and health information (see Table 1 for relevant regulations).
4. Discussion
Has the genetics service breached its statutory privacy obligations by notifying Darcy directly in the hypothetical case study provided (Figure 1)?
4.1. How Is the Use of Each Type of Information Identified in the Case Study Regulated by the Relevant Regulations?
4.1.1. Darcy’s Contact Details
Individuals’ contact details, such as addresses and telephone numbers, are generally accepted to be personal information [17] (but not sensitive information), so their collection and/or use must comply with the requirements applicable to personal information.
4.1.2. The Genetic Information
Simon has consented to the disclosure of his genetic information in both scenarios, so the question to be addressed is whether the genetic information in the letters (that Darcy is at risk of inheriting a familial variant) is (a) sensitive information and (b) genetic information belonging to Darcy. Given the definition of personal information (see Figure 2) includes information or an opinion about an identified individual, whether it is true or not, information that identifies an individual’s risk of developing disease appears to be personal information. The definition of “sensitive information” clearly includes genetic information (whether it is health information or not), so any genetic information about Darcy will also be sensitive information.
Health information is defined to include, “genetic information about an individual in a form that is, or could be, predictive of the health of the individual or a genetic relative of the individual”. Letter S2 includes specific information about the familial genetic condition, that seems to fall within this definition as it is in a form that could be predictive of the health of Darcy or her genetic relative (Simon). However, Letter S1, which only refers generally to a relative having “a DNA change that increases the risk of developing an inherited medical condition”, is less obvious. Arguably, the fact that Darcy is at risk of inheriting an unnamed DNA variant is not specific enough to be health information about Darcy as it is not in a form that could be predictive of her health or her genetic relative’s health.
The question, then, is whether Darcy’s risk of inheriting an unnamed DNA variant from an unnamed relative is genetic information (that is not health information) about her. The PA and explanatory material do not consider what constitutes genetic information that is not health information [18], and there is no judicial interpretation to assist. However, the 2006 amendment of the PA to insert genetic information that is not health information into the definition of sensitive information arose from the recommendations of the Australian Law Reform Commission and Australian Health Ethics report Essentially Yours (ALRC 96) [19]. These recommendations were intended to cover, for example, “genetic information derived from parentage or other identification testing that is not predictive of health”.
The recent recommendations arising from the Australian Attorney General’s review of the PA, which recommend adding “genomic information” to the definition of sensitive information, do not further clarify this question [20]. This means that the information in Letter S2 is likely to be personal and sensitive information about Darcy, whereas the information in Letter S1 is likely to be personal information (as it is information about her), but it is unclear whether it is sensitive information. For this reason, it should be treated as sensitive information in this context to be prudent. Next, we will consider how the requirement that information must be about an “identified or reasonably identifiable” individual affects this categorization.
The definition of personal information (see Figure 2) applies to “Information or an opinion about an identified individual, or an individual who is reasonably identifiable”. Since (i) Darcy is identified and named and (ii) the familial genetic information is linked to her and used to inform the assessment of Darcy’s risk, the argument that the information contained in Letter S2 is Darcy’s personal (and sensitive) information is further supported. However, the information about Simon would not be Darcy’s personal information without this additional link to her risk, as a reasonably identifiable individual she needs to be “a subject matter of the information or opinion” [21]. If information about Simon’s genetic variant on its own became Darcy’s personal information through the sharing of the information in either letter, this would raise the question of whether Darcy could control Simon’s sharing of his own genetic information without her consent.
It is clear that the parliamentary intention does not support an interpretation that Darcy could interfere with Simon’s sharing of his own genetic information. Although statutory interpretation must prioritize the word of the text, parliamentary materials may be used to provide context [22]. The Explanatory Memorandum for the Privacy Legislation Amendment Bill 2006 (Cth) indicates that expressly including genetic information in the definitions (Figure 2) was intended to allow HPs’ discretion to advise relatives of genetic risk, even without patient consent [23]. However, this does not support an interpretation that Parliament intended to restrict individuals’ own autonomy with respect to their individual information. Darcy has no right to control the sharing of Simon’s personal information with others—that is Simon’s decision.
In summary:
- Darcy’s contact details are personal information and must be collected and used in accordance with the regulations applicable to personal information.
- The information contained in Letters S1 and S2 is Darcy’s personal information.
- The genetic information contained in Letter S2 (which names the specific gene) is likely to also be Darcy’s sensitive information, and must be used and/or disclosed in accordance with the regulations applicable to sensitive information.
- It is unclear whether the information contained in Letter S1 (which does not name the specific gene and provides general information only) is sensitive information, but to be prudent it should be used and/or disclosed in accordance with the regulations applicable to sensitive information.
- Simon’s genetic information alone is not Darcy’s personal information.
Next, we consider whether the collection, use and/or disclosure of the personal information was a breach of privacy, or conducted in accordance with the relevant regulations (Table 2).
4.2. Are the Proposed Uses a Breach of Privacy?
We have concluded that Darcy’s contact details and the information in Letters S1 and S2 are personal information, and the genetic information in Letter S2 (and potentially the information in Letter S1) is sensitive information belonging to Darcy. The purpose of the collection and use of the contact details, and the use and disclosure of the genetic information in the letter, was to notify Darcy about her potential genetic risk. Facilitating the use of personal information to advise genetic relatives of their potential genetic risk was the primary reason behind the amendments which were made to the PA in 2006 to include genetic information in the PA framework [23].
4.2.1. APP 3: Collection of Solicited Personal Information
APP 3 prohibits the collection of personal information unless reasonably necessary for the entity’s functions. Facilitation of cascade testing of at-risk relatives is a core function of genetics services [12,24,25,26,27,28,29,30,31,32], and communication of risk information to relatives by patients directly is frequently inadequate [2,29]. Accordingly, collecting Darcy’s personal information for this purpose sits squarely within its core functions. For sensitive information, APP 3 also requires the individual’s consent to collection. As contact details are not sensitive information, this aspect of APP 3 does not require Darcy’s consent for the collection of her contact information (although APP 5 requires her to be notified of certain things, as discussed below). This is consistent across all state/territory regulations other than in Western Australia (considered further below).
APP 3 also requires personal information be collected from individuals directly, unless unreasonable or impracticable to do so. The genetics service has no pre-existing relationship with Darcy, so collecting her contact details directly is clearly impracticable. Most states/territory regimes have similar effect, although Table 2 notes some differences in New South Wales and Western Australia. In New South Wales, s9 of the Privacy and Personal Information Protection Act 1998 (NSW) (PRIPA) does not include the “unless unreasonable or impracticable’ exemption. However, s26(1) allows for an exemption where compliance would prejudice the interests of the individual to whom the information relates. Clearly, at-risk relatives’ interests will be prejudiced if they cannot be notified of their medically actionable genomic risk [12,24,25,32,33].
In Western Australia, which does not have a privacy regime, the collection, use, and disclosure of personal information are regulated under the Health Services Act 2016 (WA), and is authorized if done with the consent of the person to whom it relates (s220(1)(a)). However, they can also be authorized under s220(1)(i) if any circumstances prescribed in the Health Services (Information) Regulations 2017 (WA) apply. Under s5(1)(a) of those regulations, collection, use, or disclosure is authorized if reasonably necessary to lessen or prevent a serious risk to the life, health, or safety of an individual. Although genetic information is not explicitly mentioned in the WA Regulations, these are almost the exact words that were inserted into the PA to allow the disclosure of information to a genetic relative regarding their genetic risk [23]. This supports the conclusion that the WA regulations allow the collection of Darcy’s contact information from Simon without her consent, for the purpose of lessening or preventing a serious risk to her health, due to genetic risk.
Accordingly, in all jurisdictions, there is support for the argument that the collection of contact details without Darcy’s consent for the purposes of notification to her about her potential genetic risk is allowed.
4.2.2. APP 5: Notification of Individuals
APP 5 requires entities who have collected personal information to take reasonable steps to notify individuals of matters including the entity’s contact details, the purpose of the collection (and any consequences flowing from not collecting the information), and mechanisms to complain about breach of privacy. These matters do not prevent the collection/use of contact details for risk notification, but must inform the content of any communication by HPs. Letters S1 and S2 have incorporated these requirements.
In addition to these Commonwealth PA obligations, which are largely mirrored by the various state/territory regulations, the Victorian Health Privacy Principles (HPP 1.7), require that reasonable steps are taken to ensure health information remains confidential when received from a recipient who is not the individual the health information is about. Some further general obligations to take reasonable steps to protect personal information are also found in the Commonwealth Australian Privacy Principles (APP 11.1); as well as those in Victoria (IPP 4.1/HPP 4.1); Australian Capital Territory (TPP 11/PP 4.1); New South Wales (HPP 5/PRIPA s12); Northern Territory (IPP 4.1); Queensland (IPP 4/NPP 4); South Australia (IPP 4(4)); and Tasmania (PIPP 4).
4.2.3. APP 6: Use or Disclosure of Personal Information
APP 6 (and similar state/territory principles) limits use of Darcy’s personal information once collected. Personal information collected for one purpose (the primary purpose) cannot be used for another purpose (a secondary purpose) without consent, unless an exception applies. Adding Darcy’s contact details (without consent) to a mailing list, for example, would not be related to the primary purpose and would be a privacy breach. Contacting her as a follow-up to the letter that was sent would be related to the primary purpose, and would not be a breach of privacy unless she had expressly requested not to be contacted further.
The use of the genetic information about Darcy (her genetic risk) is also governed by APP 6. However, there is no breach of privacy in disclosing Darcy’s own personal information (her potential genetic risk) to her. The “right not to know” might be raised here to argue that it is a breach of Darcy’s rights to directly contact her with this information, without her consent. However, this purported “right” is not an element of statutory privacy obligations, or a right recognized under Australian privacy regimes. Rather, it is an ethical element (linked to autonomy) to be balanced against other elements (including the ethical imperative to provide access to medically actionable risk information) [34,35]. Because of the significant preventive potential of medically actionable risk information, the “right not to know” is significantly outweighed by the ethical imperative to offer this information to at-risk individuals [10].
Further, s16B(4) of the PA further supports disclosing to Darcy her potential genetic risk. Even without Simon’s consent, disclosure to Darcy is permitted if “necessary to lessen or prevent a serious threat to [her] life, health or safety”. A genetic predisposition to cancer has been specifically recognized as a serious threat to life, health, or safety, “even where such a threat is not imminent” [23]. Thus, the purported “right not to know” does not prevent the disclosure of this information directly to Darcy, especially with Simon’s consent. However, informing other entities or individuals of Darcy’s risk, without her consent, would be a privacy breach (unless another statutory exception applies). Furthermore, if Darcy asked not to be contacted further after the initial contact was made the HP should respect her wishes.
An important final point is that the discretion to contact at-risk relatives directly with patient consent, as discussed throughout this analysis, does not equate to a positive duty on HPs to contact relatives directly and notify them of their risk. No such obligation has been created in Australia, either through legislative instruments or Australian judicial findings. Rather, this analysis has confirmed that the discretion to do so (with the patient’s consent) exists, and is supported by the regulations governing HPs’ collection, use, and disclosure of personal information in all jurisdictions in Australia.
In summary:
- This analysis supports a conclusion that collection of Darcy’s contact details without her consent is allowed under all Australian privacy regulations, for the purpose of notifying her of her possible genetic risk.
- Reasonable steps should be taken to protect Darcy’s personal information once collected.
- Darcy should be notified as soon as possible after her contact details are collected, about the purpose of the collection and avenues to complain about breach of privacy.
- Darcy’s personal information (her contact details) can only be used for the primary purpose for which it was collected (to notify her about her possible genetic risk), not for any other purpose (without her consent).
- Disclosure of Simon’s genetic information to Darcy is permitted with his consent.
- Disclosure of Darcy’s own genetic information to her is permitted, and the purported “right not to know” does not prevent the disclosure of this information to Darcy, though her autonomy should be respected if she chooses not to pursue this further once notified.
- There is no positive duty on HPs to contact relatives directly to notify them of their risk—the discretion available to HPs to notify patients’ at-risk relatives directly is not an obligation.
5. Conclusions
Direct notification of patients’ at-risk relatives regarding medically actionable genetic information, with patient consent, is not a breach of Australian privacy law, providing it is conducted in accordance with the applicable regulatory principles as discussed throughout this analysis. Australian clinical services should consider offering direct notification of at-risk relatives to assist patients with family communication. This analysis provides an important resource for clinical services and HPs considering their obligations and discretion in this area; however, harmonized national guidelines would assist with the clarification of the discretion for HPs.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/biotech12020045/s1, Supplementary file S1: Scenario 1 Letter; Supplementary file S2: Scenario 2 Letter.
Author Contributions
Conceptualization: J.T.; Methodology: J.T. and M.O.; formal analysis: J.T.; writing—original draft preparation: J.T.; writing—review and editing: K.N., T.B., and M.O.; supervision: M.O. All authors have read and agreed to the published version of the manuscript.
Funding
Australian Genomics receives funding from the National Health and Medical Research Council (Grants GNT1113531 and GNT2000001) and the Australian Government’s Medical Research Future Fund (MRFF).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
There is no associated data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Marleen van den Heuvel, L.; Stemkens, D.; van Zelst-Stams, W.A.G.; Willeboordse, F.; Christiaans, I. How to inform at-risk relatives? Attitudes of 1379 Dutch patients, relatives, and members of the general population. J. Genet. Couns. 2020, 29, 786–799. [Google Scholar] [CrossRef] [PubMed]
- Healey, E.; Taylor, N.; Greening, S.; Wakefield, C.E.; Warwick, L.; Williams, R.; Tucker, K. Quantifying family dissemination and identifying barriers to communication of risk information in Australian BRCA families. Genet. Med. 2017, 19, 1323–1331. [Google Scholar] [CrossRef]
- Tiller, J.; Bilkey, G.; Macintosh, R.; O’Sullivan, S.; Groube, S.; Palover, M.; Pachter, N.; Rothstein, M.; Lacaze, P.; Otlowski, M. Disclosing genetic information to family members without consent: Five Australian case studies. Eur. J. Med. Genet. 2020, 63, 104035. [Google Scholar] [CrossRef] [PubMed]
- Sermijn, E.; Delesie, L.; Deschepper, E.; Pauwels, I.; Bonduelle, M.; Teugels, E.; De Greve, J. The impact of an interventional counselling procedure in families with a BRCA1/2 gene mutation: Efficacy and safety. Fam. Cancer 2016, 15, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.C.; Dotson, W.D.; DeVore, C.S.; Bednar, E.M.; Bowen, D.J.; Ganiats, T.G.; Green, R.F.; Hurst, G.M.; Philp, A.R.; Ricker, C.N.; et al. Delivery of Cascade Screening for Hereditary Conditions: A Scoping Review of the Literature. Health Affairs 2018, 37, 801–808. [Google Scholar] [CrossRef]
- Henrikson, N.B.; Blasi, P.; Figueroa Gray, M.; Tiffany, B.T.; Scrol, A.; Ralston, J.D.; Fullerton, S.M.; Lim, C.Y.; Ewing, J.; Leppig, K.A. Patient and Family Preferences on Health System-Led Direct Contact for Cascade Screening. J. Pers. Med. 2021, 11, 538. [Google Scholar] [CrossRef]
- Dheensa, S.; Lucassen, A.; Fenwick, A. Limitations and Pitfalls of Using Family Letters to Communicate Genetic Risk: A Qualitative Study with Patients and Healthcare Professionals. J. Genet. Couns. 2018, 27, 689–701. [Google Scholar] [CrossRef]
- Aktan-Collan, K.; Haukkala, A.; Pylvänäinen, K.; Järvinen, H.J.; Aaltonen, L.A.; Peltomäki, P.; Rantanen, E.; Kääriäinen, H.; Mecklin, J.P. Direct contact in inviting high-risk members of hereditary colon cancer families to genetic counselling and DNA testing. J. Med. Genet. 2007, 44, 732–738. [Google Scholar] [CrossRef]
- Van den Heuvel, L.M.; Hoedemaekers, Y.M.; Baas, A.F.; Baars, M.J.; van Tintelen, J.P.; Smets, E.M.; Christiaans, I. A tailored approach to informing relatives at risk of inherited cardiac conditions: Results of a randomised controlled trial. Eur. J. Hum. Genet. 2022, 30, 203–210. [Google Scholar] [CrossRef]
- Newson, A.J. Why Genetics Services Should Contact At-Risk Relatives Directly. 2006. Available online: http://hdl.handle.net/2123/12242 (accessed on 1 November 2022).
- Marks, D.; Thorogood, M.; Neil, S.M. Cascade screening for familial hypercholesterolaemia: Implications of a pilot study for national screening programmes. J. Med. Screen. 2006, 13, 156–159. [Google Scholar] [CrossRef]
- Frey, M.K.; Ahsan, M.D.; Bergeron, H.; Lin, J.; Li, X.; Fowlkes, R.K.; Narayan, P.; Nitecki, R.; Rauh-Hain, J.A.; Moss, H.A.; et al. Cascade Testing for Hereditary Cancer Syndromes: Should We Move Toward Direct Relative Contact? A Systematic Review and Meta-Analysis. J. Clin. Oncol. 2022, 40, 4129–4143. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, S.; Molster, C.; Poke, S.; O’leary, P. Communicating Familial Hypercholesterolemia Genetic Information within Families. Genet. Test. Mol. Biomark. 2009, 13, 301–306. [Google Scholar] [CrossRef]
- Hardcastle, S.J.; Legge, E.; Laundy, C.S.; Egan, S.J.; French, R.; Watts, G.F.; Hagger, M.S. Patients’ Perceptions and Experiences of Familial Hypercholesterolemia, Cascade Genetic Screening and Treatment. Int. J. Behav. Med. 2015, 22, 92–100. [Google Scholar] [CrossRef]
- Suthers, G.K.; Armstrong, J.; McCormack, J.; Trott, D. Letting the family know: Balancing ethics and effectiveness when notifying relatives about genetic testing for a familial disorder. J. Med. Genet. 2006, 43, 665–670. [Google Scholar] [CrossRef]
- Tiller, J.; Stott, A.; Finlay, K.; Boughtwood, T.; Madelli, E.; Horton, A.; Winship, I.; Nowak, K.; Otlowski, M. Direct notification by health professionals of relatives at-risk of genetic conditions (with patient consent): Views of the Australian public. Eur. J. Hum. Genet, 2023; accepted. [Google Scholar]
- Australian Government Office of the Australian Information Commissioner. What Is Personal Information? Australian Government Office of the Australian Information Commissioner: Canberra, Australia, 2017. [Google Scholar]
- Paltiel, M.; Taylor, M.; Newson, A. Protection of genomic data and the Australian Privacy Act: When are genomic data ‘personal information’? Int. Data Priv. Law. 2023, 13, 47–62. [Google Scholar] [CrossRef]
- Australian Law Reform Commission. Essentially Yours: The Protection of Human. Genetic Information in Australia; Australian Law Reform Commission: Sydney, Australia, 2003. Available online: http://www.alrc.gov.au/publications/report-96 (accessed on 1 November 2022).
- Australian Government Attorney General’s Department. Privacy Act Review Report; Australian Government Attorney General’s Department. 2022. Available online: https://www.ag.gov.au/rights-and-protections/publications/privacy-act-review-report (accessed on 1 May 2023).
- Privacy Commissioner v Telstra Corp Ltd. FCAFC 4. 2017. Available online: https://www.ags.gov.au/sites/default/files/el253.pdf (accessed on 1 November 2022).
- Dharmananda, J. Using parliamentary materials in interpretation: Insights from parliamentary process. Univ. N. S. W. Law J. 2018, 41, 4–39. [Google Scholar] [CrossRef]
- Parliament of Australia. Bills Digest No. 9 2006–2007: Privacy Legislation Amendment Bill 2006. 2006. Available online: https://www.aph.gov.au/Parliamentary_Business/Bills_Legislation/bd/bd0607/07bd009 (accessed on 1 November 2022).
- Ademi, Z.; Watts, G.F.; Pang, J.; Sijbrands, E.J.; van Bockxmeer, F.M.; O’Leary, P.; Geelhoed, E.; Liew, D. Cascade screening based on genetic testing is cost-effective: Evidence for the implementation of models of care for familial hypercholesterolemia. J. Clin. Lipidol. 2014, 8, 390–400. [Google Scholar] [CrossRef]
- Bell, D.A.; Pang, J.; Burrows, S.; Bates, T.R.; van Bockxmeer, F.M.; Hooper, A.J.; O’Leary, P.; Burnett, J.R.; Watts, G.F. Effectiveness of genetic cascade screening for familial hypercholesterolaemia using a centrally co-ordinated clinical service: An Australian experience. Atherosclerosis 2015, 239, 93–100. [Google Scholar] [CrossRef]
- Courtney, E.; Chok, A.K.L.; Ting Ang, Z.L.; Shaw, T.; Li, S.T.; Yuen, J.; Ngeow, J. Impact of free cancer predisposition cascade genetic testing on uptake in Singapore. NPJ Genom. Med. 2019, 4, 22. [Google Scholar] [CrossRef]
- Frey, M.K.; Kahn, R.M.; Chapman-Davis, E.; Tubito, F.; Pires, M.; Christos, P.; Anderson, S.; Mukherjee, S.; Jordan, B.; Blank, S.V.; et al. Prospective Feasibility Trial of a Novel Strategy of Facilitated Cascade Genetic Testing Using Telephone Counseling. J. Clin. Oncol. 2020, 38, 1389–1397. [Google Scholar] [CrossRef] [PubMed]
- Ho, A.; Leach, E.; Virani, A.; Arbour, L.; Bartels, K.; Wong, E.K. Cascade testing for inherited arrhythmia conditions: Experiences and attitudes of family communication approaches for a Canadian cohort. J. Genet. Counsel. 2022, 31, 815–828. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, S.; Won, N.Y.; Dotson, W.D.; Wright, S.T.; Roberts, M.C. Barriers and facilitators for cascade testing in genetic conditions: A systematic review. Eur. J. Hum. Genet. 2020, 28, 1631–1644. [Google Scholar] [CrossRef]
- Tuffaha, H.W.; Mitchell, A.; Ward, R.L.; Connelly, L.; Butler, J.R.; Norris, S.; Scuffham, P.A. Cost-effectiveness analysis of germ-line BRCA testing in women with breast cancer and cascade testing in family members of mutation carriers. Genet. Med. 2018, 20, 985–994. [Google Scholar] [CrossRef]
- Human Genetics Society of Australasia. Submission to the Commonwealth Department of Health MBS Review Advisory Committee: Provision of Services by FHGSA Registered Clinical Genetic Counsellors. 2021. Available online: https://consultations.health.gov.au/medicare-reviews-unit/medicare-benefits-schedule-mbs-review-advisory-com/supporting_documents/HGSA%20Submission%20for%20MRAC%20Review.pdf (accessed on 1 January 2023).
- Forrest, L.E.; Delatycki, M.B.; Curnow, L.; Skene, L.; Aitken, M. Genetic health professionals and the communication of genetic information in families: Practice during and after a genetic consultation. Am. J. Med. Genet. Part A 2010, 152A, 1458–1466. [Google Scholar] [CrossRef] [PubMed]
- George, R.; Kovak, K.; Cox, S.L. Aligning policy to promote cascade genetic screening for prevention and early diagnosis of heritable diseases. J. Genet. Counsel. 2015, 24, 388–399. [Google Scholar] [CrossRef]
- Tiller, J.; Trainer, A.H.; Campbell, I.; Lacaze, P.A. Ethical and practical implications of returning genetic research results: Two Australian case studies. Med. J. Aust. 2021, 214, 259–262.e1. [Google Scholar] [CrossRef]
- Newson, A.J.; Humphries, S.E. Cascade testing in familial hypercholesterolaemia: How should family members be contacted? Eur. J. Hum. Genet. 2005, 13, 401–408. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).