
The Effects of Group Sandplay Therapy (GST) on Child Victims of Cyberbullying: Focusing on Internalizing and Externalizing Problems

 , , , , and
, , , , and
Abstract
1. Introduction
2. Methods
2.1. Study Design
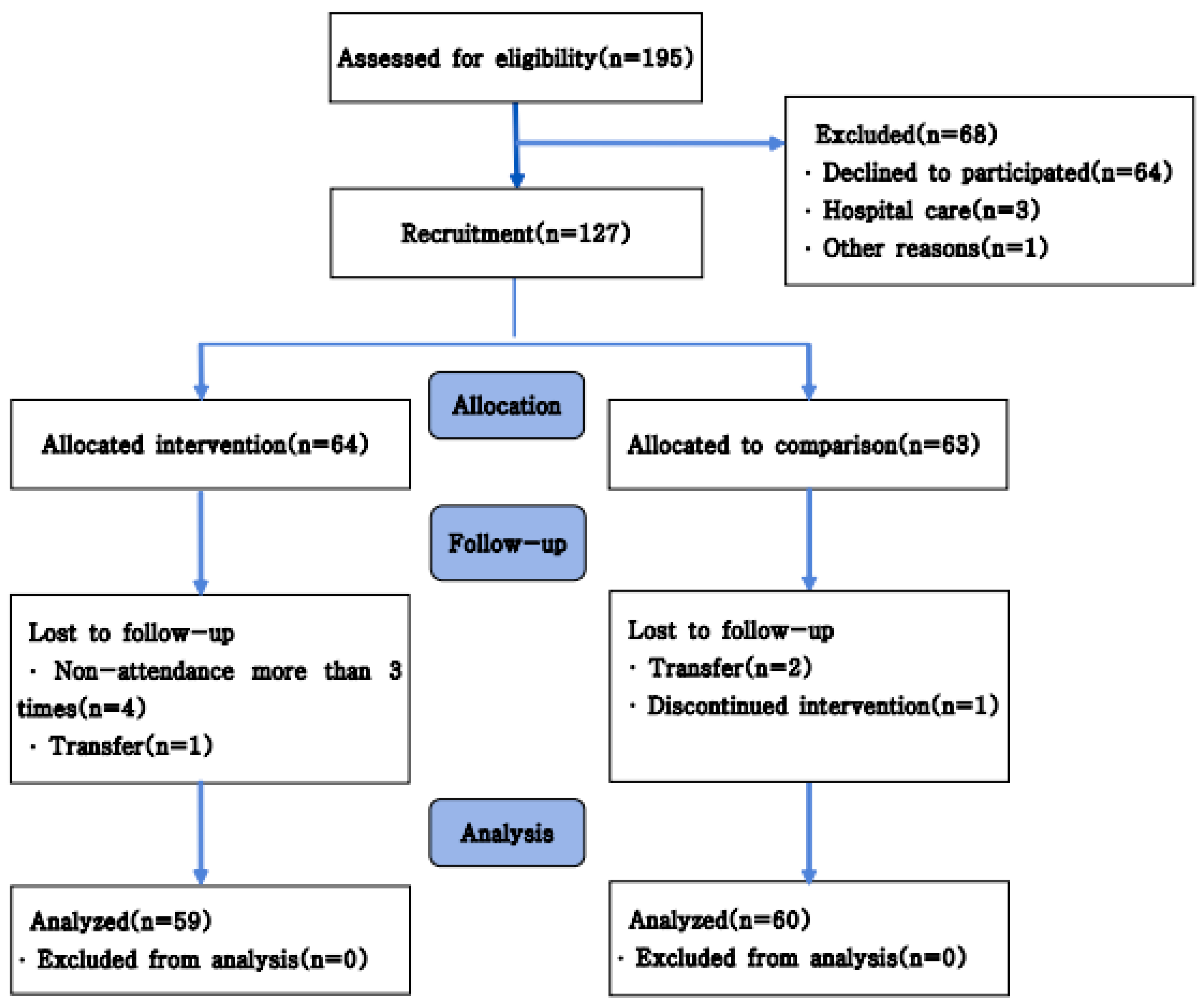
2.2. Participants
2.3. Intervention
2.4. Measures
Korean Youth Self Report: K-YSR
2.5. Statistical Analysis
2.6. Ethical Considerations and Informed Consent
3. Results
3.1. Demographic Characteristics
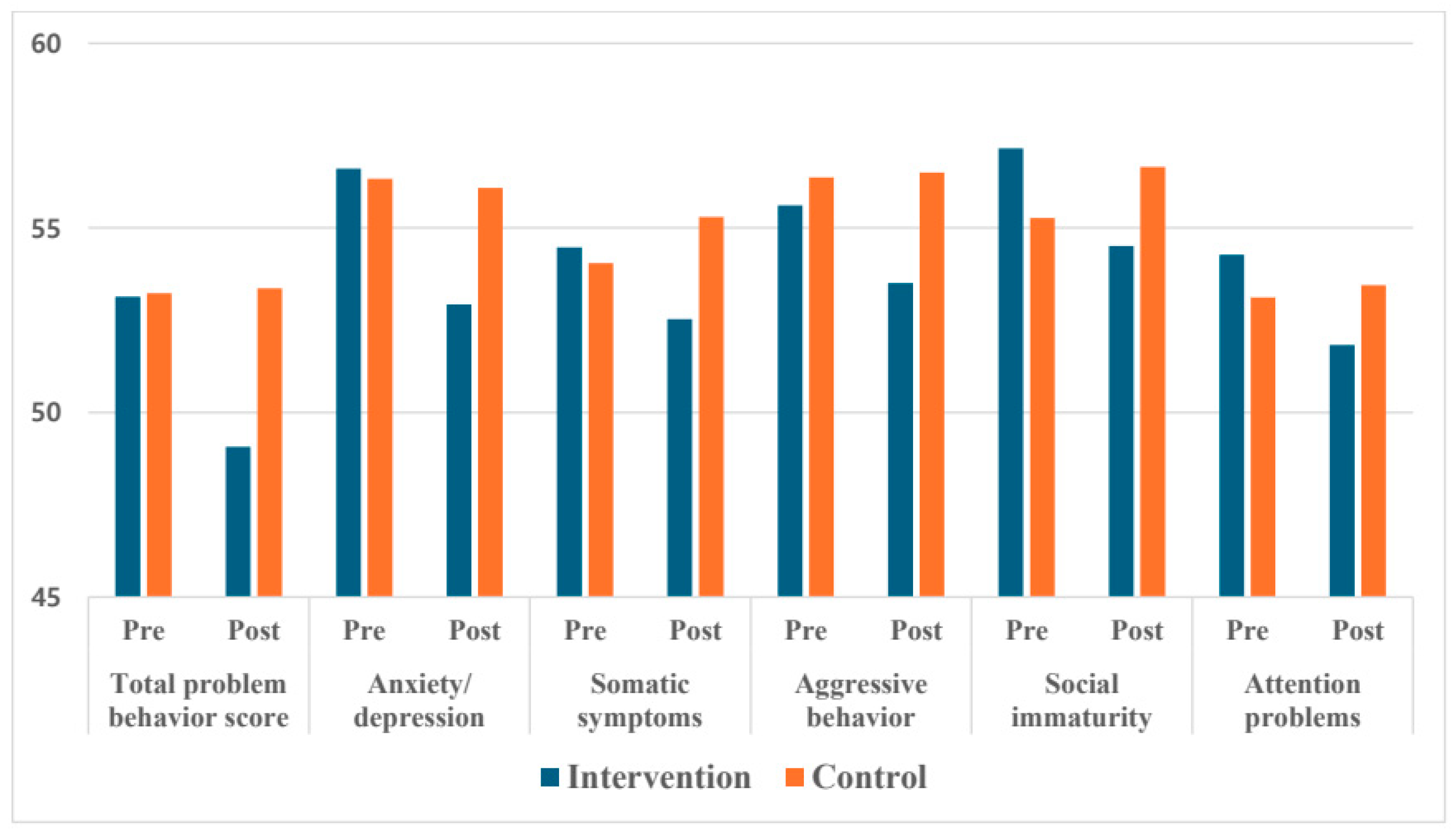
3.2. Changes in K-YSR After GST Intervention
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| GST | Group Sandplay Therapy |
References
- Beckman, L.; Hagquist, C.; Hellström, L. Does the Association with Psychosomatic Health Problems Differ between Cyberbullying and Traditional Bullying? Emot. Behav. Difficulties 2012, 17, 421–434. [Google Scholar] [CrossRef]
- Kowalski, R.M.; Giumetti, G.W.; Schroeder, A.N.; Lattanner, M.R. Bullying in the Digital Age: A Critical Review and Meta-Analysis of Cyberbullying Research among Youth. Psychol. Bull. 2014, 140, 1073–1137. [Google Scholar] [CrossRef]
- Fauman, M.A. Cyber Bullying: Bullying in the Digital Age. Am. J. Psychiatry 2008, 165, 780–781. [Google Scholar] [CrossRef]
- Li, C.; Wang, P.; Martin-Moratinos, M.; Bella-Fernández, M.; Blasco-Fontecilla, H. Traditional Bullying and Cyberbullying in the Digital Age and Its Associated Mental Health Problems in Children and Adolescents: A Meta-Analysis. Eur. Child Adolesc. Psychiatry 2022, 33, 2895–2909. [Google Scholar] [CrossRef] [PubMed]
- Umesh, B.; Ali, N.N.; Farzana, R.; Bindal, P.; Aminath, N.N. Student and Teachers Perspective on Cyber-Bullying. J. Forensic Psychol. 2018, 3, 1–6. [Google Scholar]
- Bhat, C.S.; Chang, S.-H.; Ragan, M.A. Cyberbullyingin Asia. Educ. Asia 2013, 18, 2. [Google Scholar]
- Kraft, E. Cyberbullying: A Worldwide Trend of Misusing Technology to Harass Others. WIT Trans. Inf. Commun. Technol. 2006, 36, 155–166. [Google Scholar]
- NIA Statistical Information System. 2024. Available online: https://www.nia.or.kr/site/nia_kor/ex/bbs/View.do?cbIdx=68302&bcIdx=26483&parentSeq=26483 (accessed on 1 January 2024).
- Mancheva, R. Psychosomatic and Behavioral Shanges in Victims of gyberbullying. Knowl.—Int. J. 2021, 47, 925–931. [Google Scholar]
- Hu, Y.; Bai, Y.; Pan, Y.; Li, S. Cyberbullying Victimization and Depression among Adolescents: A Meta-Analysis. Psychiatry Res. 2021, 305, 114198. [Google Scholar] [CrossRef]
- Gámez-Guadix, M.; Orue, I.; Smith, P.K.; Calvete, E. Longitudinal and Reciprocal Relations of Cyberbullying with Depression, Substance Use, and Problematic Internet Use Among Adolescents. J. Adolesc. Health 2013, 53, 446–452. [Google Scholar] [CrossRef]
- Fisher, B.W.; Gardella, J.H.; Teurbe-Tolon, A.R. Peer Cybervictimization Among Adolescents and the Associated Internalizing and Externalizing Problems: A Meta-Analysis. J. Youth Adolesc. 2016, 45, 1727–1743. [Google Scholar] [CrossRef]
- Sampasa-Kanyinga, H.; Lalande, K.; Colman, I. Cyberbullying Victimisation and Internalising and Externalising Problems among Adolescents: The Moderating Role of Parent–Child Relationship and Child’s Sex. Epidemiol. Psychiatr. Sci. 2020, 29, e8. [Google Scholar] [CrossRef]
- Patchin, J.W.; Hinduja, S. Cyberbullying Among Adolescents: Implications for Empirical Research. J. Adolesc. Health 2013, 53, 431–432. [Google Scholar] [CrossRef]
- Ybarra, M.L.; Diener-West, M.; Leaf, P.J. Examining the Overlap in Internet Harassment and School Bullying: Implications for School Intervention. J. Adolesc. Health 2007, 41, S42–S50. [Google Scholar] [PubMed]
- Freedle, L.R. Healing Trauma through Sandplay Therapy: A Neuropsychological Perspective. In The Routledge International Handbook of Sandplay Therapy; Routledge: London, UK, 2017; pp. 190–206. [Google Scholar]
- Dye, H. The Impact and Long-Term Effects of Childhood Trauma. J. Hum. Behav. Soc. Environ. 2018, 28, 381–392. [Google Scholar] [CrossRef]
- Vandebosch, H.; Van Cleemput, K. Cyberbullying among Youngsters: Profiles of Bullies and Victims. N. Media Soc. 2009, 11, 1349–1371. [Google Scholar] [CrossRef]
- Roesler, C. Sandplay Therapy: An Overview of Theory, Applications and Evidence Base. Arts Psychother. 2019, 64, 84–94. [Google Scholar] [CrossRef]
- Boik, B.; Goodwin, E.A. Sandplay Therapy: A Step by Step Manual for Psychotherapists of Diverse Orientation; WW Norton & Company: New York, NY, USA, 2000. [Google Scholar]
- Pearson, M.; Wilson, H. Sandplay Therapy: A Safe, Creative Space for Trauma Recovery. Aust. Couns. Res. J. 2019, 13, 20–24. [Google Scholar]
- Tornero, M.D.L.A.; Capella, C. Change during Psychotherapy through Sand Play Tray in Children That Have Been Sexually Abused. Front. Psychol. 2017, 8, 617. [Google Scholar] [CrossRef]
- Lee, S.; Jang, M. The Effect of Group Sandplay Therapy on Psychological Health and Resilience of Adolescent Survivors of Nepal Earthquake. J. Symb. Sandplay Ther. 2020, 11, 45–78. [Google Scholar] [CrossRef]
- Rousseau, C.; Benoit, M.; Lacroix, L.; Gauthier, M.-F. Evaluation of a Sandplay Program for Preschoolers in a Multiethnic Neighborhood. J. Child Psychol. Psychiatry 2009, 50, 743–750. [Google Scholar] [CrossRef]
- Matta, R.M.D.; Ramos, D.G. The Effectiveness of Sandplay Therapy in Children Who Are Victims of Maltreatment with Internalizing and Externalizing Behavior Problems. Estud. Psicol. 2021, 38, e200036. [Google Scholar] [CrossRef]
- Troshikhina, E. Sandplay Therapy for the Healing of Trauma. In Is This a Culture of Trauma? An Interdisciplinary Perspective; Brill: Leiden, The Netherlands, 2013; pp. 227–233. [Google Scholar]
- Kim, M. An Effect of Sandplay Therapy on PTSD Symptoms of Migrant Women Victims of Domestic Violence in South Korea. Adv. Sci. Lett. 2017, 23, 9594–9597. [Google Scholar] [CrossRef]
- Yeh, C.J.; Aslan, S.M.; Mendoza, V.E.; Tsukamoto, M. The Use of Sandplay Therapy in Urban Elementary Schools as a Crisis Response to the World Trade Center Attacks. Psychol. Res. 2015, 5, 413–427. [Google Scholar]
- Kowalski, R.M.; Limber, S.P.; Agatston, P.W. Cyber Bullying: The New Moral Frontier; Blackwell Publishing Ltd.: Oxford, UK, 2008; Volume 10, p. 9780470694176. [Google Scholar]
- Kalff, D.M. Introduction to Sandplay Therapy. J. Sandplay Ther. 1991, 1, 1–4. [Google Scholar]
- Kwak, H.J.; Ahn, U.K.; Lim, M.H. The Clinical Effects of School Sandplay Group Therapy on General Children with a Focus on Korea Child & Youth Personality Test. BMC Psychol. 2020, 8, 9. [Google Scholar] [CrossRef]
- Achenbach, T.M. Manual for the Youth Self-Report and 1991 Profile; University of Vermont Department of Psychiatry: Burlington, VT, USA, 1991. [Google Scholar]
- Oh, K.J.; Ha, E.H.; Lee, H.L.; Hong, K.E. Korean Youth Self Report; Seoul National University Press: Seoul, Republic of Korea, 2001. [Google Scholar]
- Ahn, U.K.; Kwak, H.J.; Lim, M.H. Minnesota Multiphasic Personality Inventory of School Sandplay Group Therapy with Maladjustment Behavior in Korean Adolescent. Medicine 2020, 99, e23272. [Google Scholar] [CrossRef] [PubMed]
- Roubenzadeh, S.; Abedin, A.; Heidari, M. Effectiveness of Sand Tray Short Term Group Therapy with Grieving Youth. Procedia—Soc. Behav. Sci. 2012, 69, 2131–2136. [Google Scholar] [CrossRef]
- Lee, H.S. Effects of Group Sand-Play Therapy on Children’s Improvement in Peer Relational Skills and Reduction in Behavioral Problems. Unpublished. Master’s Thesis, Namseoul University, Cheonan, Republic of Korea, 2010. [Google Scholar]
- Cao, J.; Jin, L.; Cui, C.; Cui, M. A Study on the Effects of Sandplay Therapy on Second Grade Middle School Students with PTSD. J. Symb. Sandplay Ther. 2019, 10, 75–103. [Google Scholar] [CrossRef]
- Han, Y.; Lee, Y.; Suh, J.H. Effects of a Sandplay Therapy Program at a Childcare Center on Children with Externalizing Behavioral Problems. Arts Psychother. 2017, 52, 24–31. [Google Scholar] [CrossRef]
- Flahive, M.W.; Ray, D. Effect of Group Sandtray Therapy with Preadolescents. J. Spec. Group Work 2007, 32, 362–382. [Google Scholar] [CrossRef]
- Sim, E.; Jang, M. Effects of Sandplay Therapy on Aggression and Brain Waves of Female Juvenile Delinquents. J. Symb. Sandplay Ther. 2013, 4, 45–50. [Google Scholar] [CrossRef]
- Zheng, X.; Hu, Y. The Effect of Group Sandplay Therapy on Interpersonal Trust of Adolescents. Adv. Psychol. 2019, 9, 1899–1906. [Google Scholar]
- Kazemi, E.; Ashrafi, M.; Maryam Sadat Hosseinzadeh, M.S.H.; Andalibipour, Z.; Rajab Ali, S.; Mehran Mohebian Far, M.M.F. The Effectiveness of Sand Play Therapy on Social Skills and Adaptation of Children with Separation Anxiety. Iran. J. Educ. Res. 2024, 3, 145–156. [Google Scholar]
- Ghadampour, E.; Shahbazirad, A.; Haghighi Kermanshahi, M.; Mohammadi, F.; Naseri, N. The Effects of Sand Play Therapy in Reduction of Impulsivity and Attention Deficit in Boys with ADHD. Q. J. Child Ment. Health 2018, 5, 36–46. [Google Scholar]
- Li, S.; Lu, Y.; Wu, J. Sandplay Therapy as a Complementary Treatment for Children with ADHD: A Scoping Review. Issues Ment. Health Nurs. 2023, 44, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.-M.; Hang, G.; Zhang, X.-L.; He, X.-L.; Wang, D.-D. Effects of Sandplay Therapy in Children with Attention Deficit Hyperactivity Disorders. Chin. Ment. Health J. 2010, 24, 691–695. [Google Scholar]
- Park, S.G.; Kim, H.W.; Park, B.J. The Effect of Group Sandplay Therapy on Self-Expression and School Adjustment of School Violence Victims. Korean J. Youth Stud. 2013, 20, 175–202. [Google Scholar]

{kind=link}
{kind=link}
| Directives | Session | Progress of Sandplay Therapy |
|---|---|---|
| Departure | 1 | Freely express the emotions and sensations that come from touching the sand. |
| Self-emotional contact and expression | 2 | Close your eyes and touch the sand. Feel free to experience any emotions, including sadness, pain, happiness, and worry, and express them in the sand tray. |
| 3 | Reflect on past events and situations you’ve experienced and freely express your inner emotions. | |
| Conflict and struggle | 4 | Feel free to experience and express any negative emotions, such as conflict and struggles. |
| 5 | Envision a hero confronting pain and hardship, and recreate that scene in the sand. | |
| Relationships (family, friends, school) | 6 | Freely express the emotions that arise when you think about your family. |
| 7 | Freely express the emotions that arise when you think of your friends and school. | |
| Self-understanding and acceptance | 8 | Express yourself in the sand tray (including your negative self, positive self, past, present, and future self). |
| 9 | Recall the sand creations you have made so far and express what lies at the core of your heart. | |
| Rebirth (integration) | 10 | Imagine a new version of yourself, the future you, and express how you’ve grown. |
| Variables | Intervention Group (n = 59) | Control Group (n = 60) | t/x2 | p Value |
|---|---|---|---|---|
| Age | 11.39 ± 0.49 | 11.32 ± 0.47 | 0.697 | 0.404 |
| 11 years old | 36 (61.0) | 41 (68.3) | ||
| 12 years old | 23 (39.0) | 19 (31.7) | ||
| Sex | 0.014 | 0.906 | ||
| Male | 22 (37.3) | 23 (38.3) | ||
| Female | 37 (62.7) | 37 (61.7) |
| Variables | Group (N) | Mean ± SD | Group F (P) | Time F (P) | Group × Time F (P) | Cohen’s d | |
|---|---|---|---|---|---|---|---|
| Pre | Post | ||||||
| Total problem behavior score | Intervention (59) | 53.14 ± 10.66 | 49.07 ± 9.24 | 1.466 (0.228) | 4.171 * (0.043) | 4.755 * (0.031) | 0.40 |
| Control (60) | 53.23 ± 10.95 | 53.37 ± 13.52 | |||||
| Anxiety /depression | Intervention (59) | 56.61 ± 6.59 | 52.93 ± 4.61 | 1.351 (0.248) | 9.313 ** (0.003) | 7.093 ** (0.009) | 0.49 |
| Control (60) | 56.33 ± 9.29 | 56.08 ± 8.91 | |||||
| Withdrawal /depression | Intervention (59) | 56.39 ± 7.71 | 54.32 ± 6.32 | 0.066 (0.798) | 2.962 (0.088) | 3.712 (0.056) | 0.35 |
| Control (60) | 54.98 ± 7.89 | 55.10 ± 7.45 | |||||
| Somatic symptoms | Intervention (59) | 54.47 ± 5.16 | 52.53 ± 4.17 | 1.519 (0.220) | 0.479 (0.490) | 10.023 ** (0.002) | 0.58 |
| Control (60) | 54.05 ± 6.49 | 55.30 ± 7.20 | |||||
| Rule-breaking | Intervention (59) | 53.86 ± 5.71 | 53.12 ± 4.57 | 1.460 (0.229) | 0.119 (0.731) | 3.487 (0.064) | 0.34 |
| Control (60) | 53.95 ± 4.72 | 55.03 ± 5.86 | |||||
| Aggressive behavior | Intervention (59) | 55.61 ± 6.71 | 53.51 ± 6.34 | 2.773 (0.099) | 3.056 (0.083) | 3.940 * (0.049) | 0.36 |
| Control (60) | 56.37 ± 6.83 | 56.50 ± 7.51 | |||||
| Social immaturity | Intervention (59) | 57.15 ± 6.78 | 54.51 ± 5.94 | 0.012 (0.912) | 1.042 (0.309) | 10.632 *** (0.001) | 0.60 |
| Control (60) | 55.27 ± 7.34 | 56.65 ± 8.24 | |||||
| Cognitive issues | Intervention (59) | 56.76 ± 7.23 | 55.14 ± 6.59 | 0.003 (0.958) | 1.636 (0.203) | 1.178 (0.280) | 0.20 |
| Control (60) | 55.95 ± 8.03 | 55.82 ± 8.89 | |||||
| Attention problems | Intervention (59) | 54.27 ± 7.87 | 51.83 ± 3.71 | 0.075 (0.784) | 2.354 (0.128) | 4.079 * (0.046) | 0.37 |
| Control (60) | 53.12 ± 5.24 | 53.45 ± 6.21 | |||||
| Other problems | Intervention (59) | 53.42 ± 4.60 | 53.39 ± 5.96 | 5.004 * (0.027) | 0.022 (0.881) | 0.044 (0.834) | 0.04 |
| Control (60) | 55.33 ± 5.85 | 55.53 ± 6.59 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.-A.; Lee, M.-B.; Lee, Y.; Lee, C.M.; Kim, D.H.; Kim, M.; Lee, Y.L.; Lim, M.H. The Effects of Group Sandplay Therapy (GST) on Child Victims of Cyberbullying: Focusing on Internalizing and Externalizing Problems. Psychiatry Int. 2025, 6, 80. https://doi.org/10.3390/psychiatryint6030080
Kim H-A, Lee M-B, Lee Y, Lee CM, Kim DH, Kim M, Lee YL, Lim MH. The Effects of Group Sandplay Therapy (GST) on Child Victims of Cyberbullying: Focusing on Internalizing and Externalizing Problems. Psychiatry International. 2025; 6(3):80. https://doi.org/10.3390/psychiatryint6030080
Chicago/Turabian StyleKim, Hyun-A, Myeong-Bok Lee, Youngil Lee, Chang Min Lee, Do Hyun Kim, Minsun Kim, Young Lim Lee, and Myung Ho Lim. 2025. "The Effects of Group Sandplay Therapy (GST) on Child Victims of Cyberbullying: Focusing on Internalizing and Externalizing Problems" Psychiatry International 6, no. 3: 80. https://doi.org/10.3390/psychiatryint6030080
APA StyleKim, H.-A., Lee, M.-B., Lee, Y., Lee, C. M., Kim, D. H., Kim, M., Lee, Y. L., & Lim, M. H. (2025). The Effects of Group Sandplay Therapy (GST) on Child Victims of Cyberbullying: Focusing on Internalizing and Externalizing Problems. Psychiatry International, 6(3), 80. https://doi.org/10.3390/psychiatryint6030080