Abstract
Nursing students often experience high levels of anxiety compared to students in other disciplines due to academic and clinical demands. Some of the important factors believed to influence psychological well-being are nomophobia, emotional regulation, self-efficacy and loneliness. Therefore, the current study aimed to explore the relationships between nomophobia, emotional regulation, loneliness, self-efficacy and anxiety among nursing students using structural equation modeling (SEM). A cross-sectional study was conducted among 121 nursing students. Data were collected using validated tools, including the Nomophobia Questionnaire (NMP-Q), Emotion Regulation Questionnaire (ERQ), UCLA Loneliness Scale, General Self-Efficacy scale and Generalized Anxiety Disorder (GAD-7) scale. Structural Equation Modeling (SEM) was used to explore the relationship between study variables. The findings revealed that nomophobia and loneliness were positively associated with anxiety, with standardized path coefficients of β = 0.35 (p < 0.001) and β = 0.25 (p < 0.001), respectively. Conversely, emotional regulation (β = −0.20, p < 0.001) and self-efficacy (β = −0.30, p < 0.001) showed significant protective effects by reducing anxiety. Additionally, emotional regulation negatively influenced nomophobia (β = −0.21, p < 0.001) and loneliness (β = −0.15, p < 0.05), highlighting its role in mitigating adverse psychological outcomes. Self-efficacy exhibited a negative but non-significant association with loneliness (β = −0.09, p = 0.10) and demonstrated a significant negative effect on nomophobia (β = −0.13, p < 0.05). Nomophobia and loneliness significantly contribute to heightened anxiety levels among nursing students, while emotional regulation and self-efficacy serve as protective factors. Given the high-stress nature of nursing education and clinical practice, interventions aimed at enhancing emotional regulation skills and fostering social support networks could be particularly beneficial in mitigating nomophobia, reducing loneliness, and ultimately lowering anxiety levels. Integrating such strategies into nursing curricula may not only support students’ mental well-being but also enhance their academic performance.
1. Introduction
Nursing education is inherently stressful, often placing students in acute situations of psychological distress due to the demanding nature of academic and clinical training. Studies have indicated that nursing students exhibit anxiety levels that are higher compared to their counterparts specializing in different fields. This has been associated with intensive course loads, tight assessment schedules, and the psychological burden placed on a student of caring for needy patients [1,2,3].
Nomophobia is defined as a type of fear, which refers to not having one’s mobile phone nearby or not having access to the internet. This has become more common in recent times, as technology develops and evolves. According to Valenti et al. [4], nomophobia is related not only to technological issues but also to emotional and social problems; hence, loneliness can be a mediator in the relationship between those conditions and nomophobia. Another systematic review by Rodríguez-García et al. [5] further underscores the fact that nomophobia is related to anxiety and psychological distress and therefore is relevant for understanding mental health issues among students. On the other hand, there are studies in support of the positive impact of high levels of nomophobia on anxiety levels among students. Such findings corroborate another view that too much reliance on mobile technology is closely linked to deteriorating situations regarding mental health [6]. Emotional regulation refers to the approaches that an individual employs in an attempt to influence their own feelings and the ways in which individuals experience and then express those emotions. With respect to mental health, emotional regulation tends to be considered crucial, particularly in terms of mitigating the influences of loneliness and nomophobia on anxiety. According to one recent study, poor emotional regulation skills may predispose an individual to loneliness and anxiety [7]. Moreover, Lee et al. [8] found that, through proper emotional regulation or management, even the negative impacts on learning created by mobile phone addiction could be surmounted, pointing again to the crucial role of emotional management in maintaining psychological well-being amidst technological pressures. In addition, it has also been established that emotional regulation is a valid predictor of anxiety; therefore, individuals with more disorders regarding the management of their emotions have shown a predisposition to increased anxiety symptoms [7].
Loneliness can be defined as a subjective feeling of social isolation that is capable of having serious impacts on mental health, even if it may not be objectively verifiable. A study showed that loneliness mediates the relationship between nomophobia and anxiety; lonely individuals tend to use smartphones to interact socially, thereby increasing their nomophobic tendencies [4]. Gezgin and Ümmet [9] reported that, among university students, there is a positive relationship between nomophobia and social and emotional loneliness. Loneliness is also found to increase anxiety levels where, in several studies, feelings of loneliness have been associated with increased developments of higher anxiety and depressive symptoms [10]. This is considered a cause for alarm, especially among nursing students, who may encounter certain stressors that add to the feelings of loneliness and anxiety.
Anxiety is one of the most common mental health issues among students, and includes a great deal of worrying and a severe form of fear that might lead to severe disabilities in daily functioning. Anxiety is notably prevalent among nursing students globally. A systematic review and meta-analysis reported that most nursing students experienced moderate stress (42.1%) and mild to moderate anxiety (19.4–25.1%) [11]. A study conducted in the Middle East among clinical training students at the University of Sharjah found that 63% of the sample population had a high state anxiety and 62% had high trait anxiety [12]. In Saudi Arabia, recent studies have highlighted significant levels of anxiety among nursing students. For instance, a study conducted at Jazan University found that 85.3% of nursing students experienced minimal anxiety symptoms, while 6.3% reported mild anxiety, 6.1% severe anxiety, and 2.4% moderate anxiety Another study found that 18.5% of female university nursing students experienced anxiety during the COVID-19 pandemic [13]. The interaction between nomophobia, emotional regulation and loneliness contributes towards this anxiety among students. Another study revealed that students with high levels of nomophobia have more chances of developing the symptoms of anxiety, and explores the concept that fear of technology disconnection may amplify overall anxiety [14]. Furthermore, emotional regulation turned out to be a protective agent amidst anxiety conditions, because effective strategies in regulating one’s emotions had a therapeutic effect in instances of loneliness and nomophobia [7].
Loneliness might be further exacerbated by nomophobia, as students increasingly use smartphones even for academic and social support; thus, feelings of isolation arise when they cannot access these [15,16]. Moreover, emotional regulation is one of the most important issues in influencing how students manage the stressors occurring in the nursing educational process. In other words, if the regulation of emotions is effective, then negative feelings of anxiety and loneliness will be significantly decreased, and students will successfully cope with all the complexities of their education [17,18]. On the other hand, poor emotional regulation develops the burden of loneliness, as emotionally distressed individuals retreat into social solitude, which further enhances their anxiety [17,19]. Current problems have been made even more relevant by the COVID-19 pandemic and, in this regard, several nursing students reported that, because of social distancing and the increase in online learning modes, they felt lonelier and more anxious [13,19,20,21,22]. This relationship is intricate and multi-dimensional in nature. For example, loneliness might mediate the association between nomophobia and anxiety. Such findings hint at the fact that students who are feeling lonely are more predisposed to develop anxiety because of not being able to connect with peers through technology. Moreover, this stress leads to maladaptive coping among students during nursing education and possibly furthers the levels of loneliness and anxiety. This has been proven in such works as those by Savitsky, Findling, Ereli and Hendel [1] and Kupcewicz et al. [16] Hence, the dynamics of nomophobia, emotional regulation, loneliness, and anxiety suggest the need for focused and appropriate interventions to provide support in terms of students’ mental health and well-being.
Study of the impact of nomophobia, emotional regulation, self-efficacy and loneliness on anxiety among nursing students in Saudi Arabia becomes relevant as part of an increasing number of studies that detail the psychological condition among nursing students due to their hard work. Previous studies have indicated that Saudi Arabian nursing students have high levels of anxiety, which is caused by such factors as academic pressure and poor emotional regulation skills [23,24,25]. For example, a study found that generalized anxiety disorder among university students and nursing students was widespread, showing the urgent need for addressing their mental health [23]. In addition, Alharthi estimated the significant contribution of nomophobia to one of the key mental health issues among nursing students, i.e., anxiety and stress conditions.
In this regard, research has evidenced that emotional regulation significantly helps manage stress and anxiety, while deficiencies in it increase psychological distress among nursing students [26,27]. While the high prevalence level of anxiety among Saudi Arabian nursing students and its association with other variables, such as nomophobia and emotion regulation, have been established by earlier research, few have investigated the complex interaction of such psychological variables simultaneously. Unlike earlier studies that are primarily reliant on correlation analyses, the present study employs Structural Equation Modeling (SEM), a more sophisticated statistical technique that allows a full assessment of the relationships among nomophobia, emotion regulation, self-efficacy, loneliness, and anxiety. By using SEM, this research offers a better understanding of the way these factors lead to anxiety, with insights that could guide precise interventions to enhance the mental health of nursing students. Therefore, the current study aimed to explore the relationships between nomophobia, emotional regulation, self-efficacy, loneliness, and anxiety among nursing students using SEM.
2. Materials and Methods
2.1. Design
A cross-sectional design employing structural equation modeling (SEM) was used in this study to evaluate the relationship between nomophobia, emotional regulation, self-efficacy, loneliness, and anxiety in nursing students. SEM was chosen for its ability to analyze multiple relationships simultaneously, providing a holistic insight into the interrelationship between these psychological factors. As the study is cross-sectional, however, it is not possible to make causal inferences, and the findings have to be interpreted as associative rather than causal.
2.2. Sample and Settings
A sample size of 100 nursing students was computed based on SEM guidelines, where at least 5 to 10 persons per estimated parameter is required [28]. Since there are five variables in this study, i.e., nomophobia, emotional regulation, self-efficacy, loneliness, and anxiety, 100 research subjects were considered enough to provide model stability and sufficient statistical power. According to their recommendations, a threshold of 100–200 subjects is regarded as appropriate for effective and applicable findings [29]. To tackle the problem of low response rate, the researcher chose to go beyond the minimum number of participants required during recruitment. Usually, it is prudent to add 20% to 30% of the estimated sample size [30]. Consequently, the researchers in the current study determined that the sample size would include 130 students. The study included students of varying age, gender, and academic year level. The mean age was 20.66 ± 1.76 years for males and 20.23 ± 1.68 years for females. In terms of gender distribution, 57.02% (n = 69) of the student s were male, while 42.98% (n = 52) were female. Regarding the academic level, 8.26% (n = 10) of students were in their first year, 19.01% (n = 23) in their second year, 29.75% (n = 36) in their third year, and 42.98% (n = 52) in their fourth year. Out of the total sample of 130 students, 121 students participated in the survey, resulting in a response rate of 93.08%.
2.3. Data Collection
In this study, a convenience sampling strategy was used to recruit the participants from a nursing college in the southern region of Saudi Arabia. Data were collected between May and July 2023. Participants were invited via official university emails, ensuring that students across different academic years were informed. A total of 130 students were invited, with 121 completing the survey, yielding a response rate of 93.08%. The questionnaire was self-reported and completed independently by participants. Participation was entirely voluntary, and no rewards or incentives were provided, thereby eliminating the risk of external or self-selection bias in the responses. Participants electronically selected a permission option indicating that they fully understood and were willing to participate in the study before proceeding to answer the questionnaires. The online survey was divided into six distinct sections. In view of the demographic profile, data were collected on age, gender, and education. The rationale for including these parameters reflects related conclusions drawn from prior studies fulfilling the goal of the present work. The UCLA scale on Loneliness; Nomophobia (NMP-Q); The ERQ-Emotion Regulation Questionnaire. Generalized Self-Efficacy Scale, and GAD-7 for generalized anxiety disorder were employed.
To avoid repetition and maintain data integrity, the Google Forms settings were adjusted to disallow multiple responses submitted by the same email address. The items were set as required responses to ensure completeness before submitting. Regarding data privacy and anonymity, no personally identifiable information was collected, and responses were kept anonymous. Data was stored on a secure computer, collected on a weekly basis, and later aggregated into a single Excel file.
To be eligible for participation in this study, individuals were required to be enrolled nursing students at a college in the southern region of Saudi Arabia with the ability to read and comprehend English, as the survey was administered in English. Students with a diagnosed psychiatric disorder were excluded to minimize potential confounding effects on the study’s psychological variables.
The UCLA Loneliness Scale (Version 3) is a 20-item psychometric unidimensional scale developed to explore subjective feelings of loneliness in an individual. Each individual participant has to rate a specific item using a scale of 1–4 where 1 implies ‘Never’, 2 implies ‘Seldom’, 3 implies ‘Occasionally’ and 4 implies ‘Often’. This is a new version of the scale, which combines both the original scale and the revised one, including both editions. The two versions were blended in the process of development. As an initial measure, 10 of the original wp items were modified. This revision was carried out to be able to cater to less educated people. In the original validation of the scale, Confirmatory Factor Analysis (CFA) was conducted to assess its structure. The results supported a unidimensional model, with excellent fit indices (CFI = 0.93, TLI = 0.91, RMSEA = 0.05), confirming its validity. Internal consistency was also high, with Cronbach’s alpha values ranging from 0.89 to 0.94 [31]. In this study, the UCLA Cronbach’s alpha of 0.92 confirms its strong reliability for assessing loneliness.
Nomophobia Questionnaire (NMP-Q): This scale consists of 20 statements that have been designed and tested for validity and reliability. The original scale showed excellent internal consistency, with a total Cronbach’s alpha of 0.94. Additionally, Principal Component Analysis (PCA) was conducted to examine its factor structure [32]. The statements are evaluated on a 7-point Likert-type scale, where 1 represents strong disagreement and 7 such strong agreement. Examining a score of 1, there is a huge difference in perspectives. The NMP-Q assessment tool provides a score between 20 and 140, zero being the least nomophobic, and clearly 140 is the most nomophobic. In such a case, 20 implies that no nomophobia is present, but 21 to 59 suggests a slight nomophobia. Similarly, a score between 60 and 99 suggests a degree of discomfort, while a score between 100 and 140 indicates severe discomfort. In the current study, the reliability coefficients for the subscales were as follows: Not Being Able to Communicate (0.91), Losing Connectedness (0.87), Not Being Able to Access Information (0.89), and Forgoing Convenience (0.80), with a total Cronbach’s alpha of 0.93, confirming the Nomophobia Questionnaire’s reliability.
Emotion Regulation Questionnaire (ERQ): This includes measures developed primarily to assess how people are prepared to control their emotions using two subscales: (1) cognitive reframing, which involves evoking the positive side of a given situation; and (2) expressive inhibition, which refers to withholding the display of any inner emotion. All participants also rated the extent to which they agreed with each statement by using a 7-point Likert scale, from 1 (strongly disagree) to 7 (strongly agree). The ERQ was validated through Exploratory Factor Analysis (EFA) and CFA, confirming a two-factor structure: Cognitive Reappraisal and Expressive Suppression, which accounted for over 50% of the variance. CFA results from a combined sample (N = 1483) showed that the independence model provided the best fit, indicating that the two factors are uncorrelated, with Cronbach’s alpha ranging from 0.68 to 0.82 across samples [33]. The scale demonstrated good internal consistency, with a total Cronbach’s alpha of 0.81, indicating high reliability. The Cognitive Reappraisal subscale (6 items) had an alpha of 0.85, while the Expressive Suppression subscale (4 items) had an alpha of 0.75.
General Self-efficacy scale: Schwarzer and Jerusalem [34] have suggested that the self-efficacy scale can provide social comparison information. The unidimensional psychometric scale has ten items, and the scoring is via a four-level Likert scale. For the item ‘not at all true’, one point was given whereas. for ‘moderately true’, two points were scored. Likewise, in ‘Moderately true’, three points were given and, for ‘Exactly true’, four points were given. Examining the results, increases in the students’ self-efficacy were positively related to the scores. It has demonstrated high internal consistency, with Cronbach’s alpha ranging from 0.76 to 0.90 across various populations. The scale also exhibits strong construct validity. The General Self Efficacy Scale is assessed out of 40 and has a coefficient alpha of 0.89 in the current study.
Generalized Anxiety Disorder (GAD–7) Scale: This is a unidimensional scale and has seven questions, and the responses are scored from 0 to 21. The cumulative total scores may vary between these figures. Depending on the intensity of their symptoms, the participants rated themselves as follows: no anxiety (0–4), mild anxiety (5–9), moderate anxiety (10–14), and severe anxiety (15–21). Thus, anxiety symptoms become more severe along the scale [35]. It shows high internal consistency (Cronbach’s alpha = 0.92) and good test–retest reliability (ICC = 0.83), while its criterion validity is supported by a sensitivity of 89% and specificity of 82% at a cutoff score of 10, making it a robust tool for both clinical and research applications. The Cronbach’s alpha of 0.91 in this study confirms its strong reliability in assessing generalized anxiety symptoms.
2.4. Ethical Considerations
This study has been reviewed and approved with a certificate by the Institutional Review Board. The participants were assured that all information provided would remain confidential and anonymous throughout the research. Responses were anonymized, and no personally identifiable information was required from the respondents.
2.5. Data Analysis
All responses collected from the self-administered questionnaires were processed for preliminary descriptive statistics using IBM SPSS Statistics (Version 25.0, IBM Corp., Armonk, NY, USA) and for structural equation modeling (SEM) using AMOS software(Version 25.0, IBM Corp., Armonk, NY, USA). Such descriptive statistics as means, standard deviations and frequencies were computed for all the variables: nomophobia, emotional regulation, self-efficacy, loneliness, and anxiety. Before the application of SEM, the data were screened to assess if there were any missing values and outliers and/or if the normality assumption was violated. Missing values were corrected utilizing the expectation maximization (EM) algorithm to form whole datasets. Skewness and kurtosis statistics were utilized to evaluate normality and extreme outliers where present were controlled according to the research standards. Pearson correlation coefficients were also utilized to identify any bivariate relationship among the variables and to find out if there was a relationship between any of the suggested correlates of anxiety: nomophobia, emotional regulation, self-efficacy, and loneliness. These analyses, being of a preliminary nature, were succeeded by structural equation modeling, which was used to validate the model proposed in the hypothesis. The fit of the structural model was estimated by a number of fit indices; these included the Chi-square test (χ2), the comparative fit index (CFI), the root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR). A p-value greater than 0.05 in the Chi-square test, a CFI value for the model above 0.90 and RMSEA and SRMR below 0.08 were interpreted as fit indices of a good and acceptable model [26]. Using SEM path analysis, the mediating and moderating roles of nomophobia, emotional regulation, self-efficacy, and loneliness on anxiety were explained. Standardized regression coefficients (β) were used to detect the quantifiers’ direct and indirect effects.
3. Results
3.1. Descriptive Statistics
The average age of males was 20.66 ± 1.76 years while that of females was 20.23 ± 1.68 years. Out of a total sample of 130 students, 121 students, or 93.08% of the sample population, responded to the survey questions as presented in Table 1.

Table 1.
Profile of Participants’ Demographics (N = 121).
Table 2 presents the levels of loneliness, emotional regulation, nomophobia, self-efficacy, and anxiety. In relation to loneliness, the highest level among participants was moderate, at 39.67%, followed by mild, 28.93%, and severe levels, 23.14%, while 8.26% had no loneliness. The mean score for emotional regulation levels was 2.45 (SD ± 1.05), which reflects that there is variation in emotional control among the participants. There is also a prevalence of nomophobia: 45.45% of the students experience this in moderation, while 25.62% have severe-level nomophobia and 24.79% a mild level; only 4.13% said they have no nomophobia. High self-efficacy predominates among the students who took part, at 57.58%. Nevertheless, the low evaluation of self-efficacy was presented by as many as 42.15%.
Table 2.
Levels of Study Variables (N = 121).
Anxiety levels ranged from 33.06%, 16.53% for moderate anxiety and 13.22% for serious anxiety, while 37.19% were not anxious at all. These findings suggested that the nursing students tended to present significant variation psychologically and emotionally. This means that 33.06% of the students suffer from mild anxiety, 16.53% from moderate anxiety, and 13.22% from serious anxiety, while 37.19% have reported no anxiety.
3.2. Correlation Analysis
The correlation analysis revealed significant relationships among the variables. Table 3 summarizes the Pearson correlation coefficients. Notably, higher levels of nomophobia were significantly correlated with increased anxiety (r = 0.50, p < 0.01) and loneliness (r = 0.45, p < 0.01). This suggests that individuals who feel more reliant on their mobile phones may also feel more anxious and lonelier, potentially due to an excessive reliance on digital connectivity as a way of receiving emotional support.
Table 3.
Correlation Matrix of Study Variables.
Emotional regulation showed a moderate negative correlation with anxiety (r = −0.35, p < 0.01), suggesting that better emotional regulation was associated with lower anxiety levels. Similarly, self-efficacy exhibited a moderate negative correlation with anxiety (r = −0.30, p < 0.01), suggesting that individuals with greater confidence in their abilities may be better equipped to manage stress and anxiety.
Additionally, loneliness demonstrated a positive correlation with anxiety (r = 0.50, p < 0.01), reinforcing previous research that socially isolated individuals are more susceptible to anxiety-related symptoms. To check for the absence of multicollinearity among the study variables, we considered Pearson correlation coefficients, the highest being 0.50, between nomophobia with anxiety and loneliness with anxiety; these are moderate correlations, that are well below the critical threshold of 0.7 [26] and hence are unlikely to create multicollinearity distortion in the results. Thus, the five variables of nomophobia, emotional regulation, self-efficacy, loneliness and anxiety awaited further analysis in the structural equation model.
3.3. SEM Results and Fit Indices
The fit indices derived from the structural equation modeling (SEM) analysis demonstrate a satisfactory model fit for the relationships explored in this study. The Chi-square test produced a value of 105.32 and a p-value of 0.09. The model does not differ significantly from the observed data. The Comparative Fit Index (CFI) was recorded at 0.96, exceeding the acceptable threshold of 0.90 and affirming the model’s goodness of fit. Additionally, the Root Mean Square Error of Approximation (RMSEA) was determined to be 0.04, suggesting a strong alignment between the model and the observed data, since values under 0.08 are regarded as satisfactory. Finally, the Standardized Root Mean Square Residual (SRMR) value of 0.03 further indicates a good fit, as it is significantly below the 0.08 threshold. The fit indices collectively indicate that the SEM effectively captures the intricate relationships between nomophobia, emotional regulation, self-efficacy, loneliness, and anxiety in nursing students, as seen in Table 4.
Table 4.
SEM Results and Fit Indices.
The structural equation modeling (SEM) results yielded substantial insights into the interrelationships among the examined variables as seen in Table 5 and Figure 1. Nomophobia demonstrated a significant positive correlation with anxiety (β = 0.35, p < 0.001), suggesting that elevated levels of nomophobia are linked to heightened anxiety in nursing students. This highlights the importance of addressing mobile phone dependency to mitigate anxiety in high-stress nursing environments. In contrast, emotional regulation and self-efficacy exhibited substantial negative impacts on anxiety (β = −0.20, p < 0.001 and β = −0.30, p < 0.001, respectively), Emphasizing their protective roles in psychological well-being, these findings suggest that enhancing self-efficacy and emotional regulation through targeted interventions may help nursing students manage stress and anxiety more effectively in both academic and clinical settings. Strengthening emotional regulation skills can enable students to cope better with high-pressure situations, maintaining emotional stability during patient care. Loneliness had a positive correlation with anxiety (β = 0.25, p < 0.001), underscoring the importance of fostering strong peer support networks in nursing programs to help reduce loneliness and improve student resilience.
Table 5.
Standardized Regression Coefficients for Path Analysis.
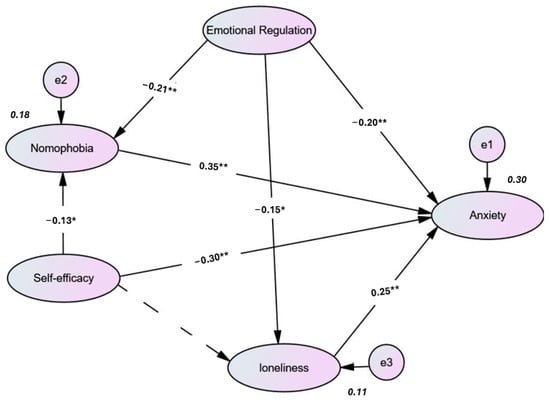
Figure 1.
Path Diagram of Structural Equation Model Examining Relationships Among Nomophobia, Emotional Regulation, Self-Efficacy, Loneliness, and Anxiety. Dotted lines show statistically insignificant paths. All estimates are standardized B coefficients. ** p < 0.001, * p < 0.05.
Emotional regulation exhibited substantial negative impacts on both nomophobia (β = −0.21, p < 0.001) and loneliness (β = −0.15, p < 0.05), underscoring its significance in mitigating these adverse consequences. Despite the lack of statistical significance in the association between self-efficacy and loneliness (β = −0.15, p = 0.10), a negative trend was seen, indicating that increased self-efficacy may correlate with diminished loneliness. Furthermore, self-efficacy exhibited a strong negative correlation with nomophobia (p < 0.05), indicating that students with greater self-confidence are less likely to experience excessive mobile phone dependence. The findings elucidate the intricate interactions among the variables, highlighting that nomophobia and loneliness significantly contribute to anxiety, whereas emotional control and self-efficacy function as protective factors.
4. Discussion
The present study has provided significant insights into the intricate relationships between nomophobia, emotional regulation, self-efficacy, loneliness, and anxiety among nursing students. The data indicate that loneliness levels ranged from moderate (39.67%) to severe (23.14%), with 8.26% having no loneliness. These rates are relatively similar to some studies conducted among nursing university students, such as a study conducted during the time of the COVID-19 pandemic documenting 49.7% of nursing students who experienced loneliness, which was associated with significant levels of depression, anxiety, and stress [36]. In addition, the prevalence of loneliness among university students was 60.2% as reported in Turkey [37]. The mean score for emotional regulation was low, at 2.45 ± 1.05. This finding confirms previous studies indicating that nursing students have difficulties in managing their feelings and emotions, which can further enhance feelings of loneliness and anxiety [38]. Nursing students are often exposed to high levels of academic and clinical stress, which can lead to difficulties in managing emotions [39].
In this study, the reported prevalence of nomophobia among nursing students was 45.45% moderate, 25.62% severe, and 24.79% mild. This figure is consistent with findings from other studies that have explored nomophobia in similar populations. For instance, one multi-site study by Molu et al. [40] found that nursing students report varied levels of nomophobia, with a considerable proportion of 68.9% reporting at moderate to severe level. This agrees with the findings of Anand [41], who assessed the prevalence of nomophobia among nursing students in Kollam, revealing that 87% of nursing students reported mild to moderate level of nomophobia. In contrast, a study conducted by Ferchichi et al. [42] found 84.2% of Tunisian university students reported having moderate to severe nomophobia, which is higher than the findings of this study. The nursing students with low self-efficacy in this study (42.15%) align with previous research on healthcare students. Labrague et al. [43] studied stress perceptions and coping strategies among Saudi nursing students and highlighted the important role that self-efficacy plays in managing academic and clinical stress. They found that students with high self-efficacy could handle challenges more effectively, which resulted in lower anxiety and improved academic performance. A study by Purwandari et al. [44] estimated the self-efficacy of nursing students. The mean self-efficacy score was 60.75, indicating that there is a moderate level of confidence among students in handling their educational responsibilities. In addition, a study conducted by Xu [38] on nursing undergraduates reported a moderate level of academic self-efficacy, influenced by factors such as psychological distress, social support, and mindfulness.
The current study showed that 33.06% of students had mild anxiety, while 16.53% and 13.22% had moderate and severe anxiety, respectively. These findings are consistent with the Saudi studies by Alhashim [23], which reported that high a prevalence among nursing students. Similarly, a study involving 6348 nursing students in China reported that 43.3% experienced moderate to severe anxiety, as assessed by the Generalized Anxiety Disorder 7-Item Scale (GAD-7) [45]. In contrast, in another cross-sectional study conducted in South Africa, it was found that 74.7% of nursing students exhibited anxiety symptoms, indicating a widespread issue that transcends geographical boundaries [46]. Results obtained from the structural equation modeling analysis provided insight into the nomophobia, emotional regulation, self-efficacy, loneliness, and anxiety that nursing students experience. A significant positive effect of nomophobia on anxiety, β = 0.35, p < 0.001, also aligns with earlier established literature, which stated that nomophobia is a crucial element, which influences the mental health conditions of any given individual. For instance, Gnardellis [47] found that individuals affected by nomophobic behaviors could achieve a higher disposition towards anxieties and stress. Participants who suffer from severe anxiety frequently use their phones in all aspects of their daily lives. In the same vein, a systematic review indicated that severe nomophobia is related to a higher risk of anxiety and depression, especially in students on health-related courses [5,48].
Furthermore, in contrast, emotional regulation and self-efficacy became significant negative predictors of anxiety with coefficients of −0.20 (p < 0.001) and −0.30 (p < 0.001), respectively. This finding is in line with the literature showing that effective emotional regulation strategies reduce anxiety symptoms [49,50]. It has also been found that self-efficacy plays a vital role in managing anxiety, since individuals with high self-efficacy are more likely to use adaptive coping strategies than their low self-efficacy counterparts. The negative relation of emotional regulation with nomophobia scored at β = −0.21, p < 0.001, suggesting that the development of emotional regulation skills may reduce nomophobic tendencies and thus alleviate anxiety.
On the other hand, loneliness significantly contributed to anxiety, with a positive coefficient of 0.25 (p < 0.001), confirming the fact that loneliness is an essential risk factor for anxiety, especially during the implementation of social distancing in the COVID-19 pandemic [51,52]. Indeed, research findings have shown how loneliness increases feelings of anxiety, creating a circle in which increased loneliness leads to heightened anxiety, which in turn may further isolate a person [53]. The negative effect of emotional regulation on loneliness scored at β = −0.15, p < 0.05, which evidenced the importance of emotional skills in fighting off feelings of loneliness and suggested that interventions aimed at improving emotional regulation could also help in reducing loneliness among nursing students. Although the relationship between self-efficacy and loneliness was not significant (β = −0.15, p = 0.10), the negative trend suggests a possible area for further exploration. Previous research has suggested that higher self-efficacy may lead to better social interactions and reduced feelings of loneliness, although evidence is mixed.
4.1. Implications
The findings of this study have important implications for nursing education, mental health interventions, and policy development. Addressing nomophobia, emotional regulation, loneliness, and self-efficacy may lead to a significant improvement in the psychological well-being and academic performance of nursing students. To achieve this, educational programs should integrate evidence-based strategies for enhancing emotional regulation capacity and self-efficacy, since such capacities serve as protective factors for anxiety and stress. For instance, incorporating mindfulness training, cognitive–behavioral techniques, and exercises to enhance resilience must be included in the nursing curricula to equip students with effective coping mechanisms. Additionally, the establishment of supportive social networks in academic settings can reduce loneliness and its accompanying mental health effects.
Nursing colleges should encourage peer-mentoring programs, group learning activities, and faculty support programs to enhance a sense of belonging among students. Furthermore, policymakers and institutional decision-makers should consider the implementation of structured interventions, such as digital well-being workshops, stress management, and responsible technology use, to offset the negative effects of nomophobia. In addition, integrating digital literacy training into nursing curricula can help students develop healthier relationships with technology, so that the use of smartphones will not interfere with mental health, academic focus, or clinical practice. Equally important, mental health services and counseling programs must also be available to nursing students, with targeted intervention for those struggling with anxiety, loneliness, or poor emotional regulation. Ultimately, by adopting these practical strategies, nursing educators and policymakers can promote a more positive learning culture, better equipping students to deal with academic and clinical stresses and guarding their mental health.
4.2. Limitations
This present study has several limitations that need to be acknowledged: the cross-sectional design may prevent any causal relationship being drawn between such variables as nomophobia, emotional regulation, loneliness, self-efficacy, and anxiety, as it captures data at a single point in time. Thus, it is not possible to ascertain the direction of effects and if relationships exist over time. Longitudinal or experimental designs should be employed in future studies to track causal paths and draw a more complete understanding of these psychological factors. Second, this study relies solely on self-reported data, which may be subject to response bias, as participants could have underreported or overstated their experiences. Third, the generalization of these findings is limited by the convenience sampling, since the sample was drawn from one nursing college in Saudi Arabia, which may not be representative of different regions or educational settings where nursing students are found. Finally, the small sample size limits the ability to conduct subgroup analyses based on gender, age, or academic progress, preventing an exploration of potential variations or interaction effects within the model. Future research should consider reconducting the study with a larger and more diverse sample.
5. Conclusions
The present study has provided important insights into the complex associations between nomophobia, emotional regulation, self-efficacy, loneliness, and anxiety among nursing students. The findings in this regard have shown that nomophobia and loneliness increase levels of anxiety, whereas emotional regulation and self-efficacy offer a protective role in lessening anxiety. Curiously, emotional regulation decreases nomophobia and loneliness, indicating that emotional regulation is highly crucial in addressing psychological well-being. While these factors are relevant to students in general, they hold particular significance in nursing education due to the profession’s unique academic and clinical demands. Specifically, nursing students frequently encounter high-stress situations, emotional distress from patient care, and severe academic pressure. As a result, emotional regulation and self-efficacy are essential to their well-being. Additionally, the clinical nature of nursing programs may heighten loneliness and reliance on mobile technology, potentially exacerbating nomophobia and anxiety.
The interplay of these factors within nursing education necessitates a discipline-specific approach to addressing mental health challenges. Therefore, targeted interventions should focus on integrating emotional regulation training, enhancing self-efficacy, and reducing loneliness and nomophobia within a nursing-specific framework. To achieve this, the nursing curriculum must foster a facilitative learning environment that equips students with appropriate coping skills for their professional roles. Incorporating coping strategies into nursing education enables institutions to better address students’ mental well-being, thereby improving both their academic performance and practice readiness. Longitudinal research needs to be the priority of future studies to identify the long-term consequences of such interventions and develop evidence-based approaches to enhance the resilience and mental well-being of nursing students.
Author Contributions
Conceptualization, Z.F.A. and M.A.; methodology, Z.F.A. and M.A.; software, Z.F.A. and M.A.; validation, Z.F.A. and M.A.; formal analysis, Z.F.A. and M.A.; investigation, Z.F.A. and M.A.; resources, Z.F.A. and M.A.; data curation, Z.F.A. and M.A.; writing—original draft preparation, Z.F.A. and M.A.; writing—review and editing, Z.F.A. and M.A.; visualization, Z.F.A. and M.A.; supervision, Z.F.A. and M.A.; project administration, Z.F.A. and M.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Research Ethics Committee of the King Khalid University (ECM#2023-1804) on September 2023. All patients signed an informed consent form to participate in this study, following all the necessary ethical recommendations inherent to a project developed with humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets that were utilized in this work will be made available to the authors upon receiving a reasonable request.
Acknowledgments
We would like to thank all participants in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Savitsky, B.; Findling, Y.; Ereli, A.; Hendel, T. Anxiety and coping strategies among nursing students during the COVID-19 pandemic. Nurse Educ. Pract. 2020, 46, 102809. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.E.P. Psychological Distress in Student Nurses Undertaking an Educational Programme With Professional Registration as a Nurse: Their Perceived Barriers and Facilitators in Seeking Psychological Support. J. Psychiatr. Ment. Health Nurs. 2018, 25, 258–269. [Google Scholar] [CrossRef]
- Santoso, A.; Dwidiyanti, M.; Wijayanti, D.Y.; Ulliya, S.; Munif, B.; Karota, E.; Tanjung, D. Online Nurse: Incorporating Islamic Spiritual Mindfulness to Decrease Anxiety during Online Learning among Nursing Students. J. Aisyah J. Ilmu Kesehat. 2022, 7, 883–888. [Google Scholar] [CrossRef]
- Valenti, G.D.; Bottaro, R.; Faraci, P. Effects of Difficulty in Handling Emotions and Social Interactions on Nomophobia: Examining the Mediating Role of Feelings of Loneliness. Int. J. Ment. Health Addict. 2022, 22, 528–542. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-García, A.-M.; Moreno-Guerrero, A.-J.; Belmonte, J.L. Nomophobia: An Individual’s Growing Fear of Being Without a Smartphone—A Systematic Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 580. [Google Scholar] [CrossRef]
- Kupcewicz, E.; Mikla, M.; Kadučáková, H.; Grochans, E. Loneliness and Satisfaction With Life Among Nursing Students in Poland, Spain and Slovakia During the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 2929. [Google Scholar] [CrossRef]
- Santl, L.; Brajković, L.; Kopilaš, V. Relationship Between Nomophobia, Various Emotional Difficulties, and Distress Factors Among Students. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 716–730. [Google Scholar] [CrossRef]
- Lee, S.-y.; Kim, M.W.; McDonough, I.M.; Mendoza, J.S.; Kim, M.S. The Effects of Cell Phone Use and Emotion-regulation Style on College Students’ Learning. Appl. Cogn. Psychol. 2017, 31, 360–366. [Google Scholar] [CrossRef]
- Gezgin, D.M.; Ümmet, D. An Investigation of the Relationship Between Nomophobia and Social and Emotional Loneliness of Turkish University Students. Int. J. Psychol. Educ. Stud. 2021, 8, 14–26. [Google Scholar] [CrossRef]
- Tárrega-Piquer, I. Nomophobia and Its Relationship With Social Anxiety and Procrastination in Nursing Students: An Observational Study. Nurs. Rep. 2023, 13, 1695–1705. [Google Scholar] [CrossRef]
- Vo, T.N.; Chiu, H.-Y.; Chuang, Y.-H.; Huang, H.-C. Prevalence of stress and anxiety among nursing students: A systematic review and meta-analysis. Nurse Educ. 2023, 48, E90–E95. [Google Scholar] [CrossRef] [PubMed]
- Otim, M.; Al Marzouqi, A.M.; Subu, M.; Damaj, N.; Al-Harbawi, S. Prevalence of generalised anxiety disorders among clinical training students at the university of sharjah. J. Multidiscip. Healthc. 2021, 14, 1863–1872. [Google Scholar] [CrossRef] [PubMed]
- Albikawi, Z.F. Predictors of anxiety, depression, and stress among female university nursing students during the COVID-19 pandemic: A cross-sectional study in Saudi Arabia. J. Pers. Med. 2022, 12, 1887. [Google Scholar] [CrossRef] [PubMed]
- Karakurt, N.; Durmaz, H.; Oral, M. Investigation of the Relationship Between Nomophobia and Anxiety Among Undergraduate Health Sciences Students. Samsun Sağlık Bilim. Derg. 2020, 5, 157–165. [Google Scholar] [CrossRef]
- McCloughen, A.; Levy, D.; Johnson, A.; Nguyen, H.; McKenzie, H. Nursing students’ socialisation to emotion management during early clinical placement experiences: A qualitative study. J. Clin. Nurs. 2020, 29, 2508–2520. [Google Scholar] [CrossRef]
- Kupcewicz, E.; Grochans, E.; Kadučáková, H.; Mikla, M.; Jóźwik, M. Analysis of the Relationship Between Stress Intensity and Coping Strategy and the Quality of Life of Nursing Students in Poland, Spain and Slovakia. Int. J. Environ. Res. Public Health 2020, 17, 4536. [Google Scholar] [CrossRef]
- Córdova, A.; Caballero-García, A.; Drobnic, F.; Roche, E.; Noriega, D.C. Influence of Stress and Emotions in the Learning Process: The Example of COVID-19 on University Students: A Narrative Review. Healthcare 2023, 11, 1787. [Google Scholar] [CrossRef]
- Kim, S.H.; Park, S. Influence of Learning Flow and Distance E-Learning Satisfaction on Learning Outcomes and the Moderated Mediation Effect of Social-Evaluative Anxiety in Nursing College Students During the COVID-19 Pandemic: A Cross-Sectional Study. Nurse Educ. Pract. 2021, 56, 103197. [Google Scholar] [CrossRef]
- Çopur, E.Ö. Anxiety and Fear of COVID-19 Among Nursing Students During the COVID-19 Pandemic: A Descriptive Correlation Study. Perspect. Psychiatr. Care 2021, 58, 141–148. [Google Scholar] [CrossRef]
- García-González, J.; Wei, R.; Alarcón, R.; Requena, M.; Ding, C.; Ventura-Miranda, M.I. Analysis of Anxiety Levels of Nursing Students Because of E-Learning During the COVID-19 Pandemic. Healthcare 2021, 9, 252. [Google Scholar] [CrossRef]
- Fitzgerald, A.; Konrad, S. Transition in Learning During COVID-19: Student Nurse Anxiety, Stress, and Resource Support. Nurs. Forum 2021, 56, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Albikawi, Z.F. Fear related to COVID-19, mental health issues, and predictors of insomnia among female nursing college students during the pandemic. Healthcare 2023, 11, 174. [Google Scholar] [CrossRef] [PubMed]
- Alhashim, A.A.A. Prevalence of Generalized Anxiety Disorder Among University Students in Saudi Arabia. Saudi J. Med. Pharm. Sci. 2024, 10, 261–266. [Google Scholar] [CrossRef]
- Andargeery, S.Y. Psychological Distress, Academic Stress, and Burnout Among Saudi Undergraduate Nursing Students. J. Clin. Med. 2024, 13, 3357. [Google Scholar] [CrossRef]
- Albikawi, Z.F. Anxiety, depression, self-esteem, internet addiction and predictors of cyberbullying and cybervictimization among female nursing university students: A cross sectional study. Int. J. Environ. Res. Public Health 2023, 20, 4293. [Google Scholar] [CrossRef]
- Shdaifat, E. Personality Traits, Emotional Regulation, and Happiness in Nursing Students: A Cross-Sectional Study. Sage Open 2024, 14, 21582440241293550. [Google Scholar] [CrossRef]
- Alkharj, S. Stress and Academic Engagement Among Saudi Undergraduate Nursing Students: The Mediating Role of Emotion Regulation and Emotional Intelligence. Nurs. Open 2024, 11, e2167. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; Guilford Publications: New York, NY, USA, 2023. [Google Scholar]
- Westland, J.C. Lower bounds on sample size in structural equation modeling. Electron. Commer. Res. Appl. 2010, 9, 476–487. [Google Scholar] [CrossRef]
- Bujang, M.A. A step-by-step process on sample size determination for medical research. Malays. J. Med. Sci. MJMS 2021, 28, 15. [Google Scholar] [CrossRef]
- Russell, D.W. UCLA Loneliness Scale (Version 3): Reliability, validity, and factor structure. J. Personal. Assess. 1996, 66, 20–40. [Google Scholar] [CrossRef]
- Yildirim, C.; Correia, A.-P. Exploring the dimensions of nomophobia: Development and validation of a self-reported questionnaire. Comput. Hum. Behav. 2015, 49, 130–137. [Google Scholar] [CrossRef]
- Gross, J.J.; John, O.P. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. J. Personal. Soc. Psychol. 2003, 85, 348. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, R.; Jerusalem, M. Generalized self-efficacy scale. Causal Control Beliefs 1995, 35, 82-003. [Google Scholar]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Jantara, R.; Abreu, D.; Santana, L.; Piexak, D.; Ribeiro, J.; Barlem, J.G.T. Social isolation and loneliness in nursing students in the context of the COVID-19 pandemic. Rev. Enferm. Uerj 2022, 29, e63609. [Google Scholar] [CrossRef]
- Özdemir, U.; Tuncay, T. Correlates of loneliness among university students. Child Adolesc. Psychiatry Ment. Health 2008, 2, 29. [Google Scholar] [CrossRef]
- Rafati, F.; Nouhi, E.; Sabzevari, S.; Dehghan-Nayeri, N. Coping strategies of nursing students for dealing with stress in clinical setting: A qualitative study. Electron. Physician 2017, 9, 6120. [Google Scholar] [CrossRef]
- Albikawi, Z.F.; Abuadas, M.H. How dialectical behavioral-based intervention affects nursing college students’ hope, somatic symptoms, and negative thoughts during COVID-19. J. Infect. Dev. Ctries. 2023, 17, 1690–1699. [Google Scholar] [CrossRef]
- Molu, N.G.; İçel, S.; Aydoğan, A. Relationship Between Nomophobia Levels and Personality Traits of Nursing Students: A Multicenter Study. Mod. Care J. 2023, 20, 132269. [Google Scholar] [CrossRef]
- Anand, S. A Study to Assess the Prevalence of Nomophobia Among Nursing Students in Kollam. Indian J. Psychiatr. Nurs. 2022, 19, 147–151. [Google Scholar] [CrossRef]
- Ferchichi, M.A.; Aouadi, K.; Aouadi, I.; Sendi, I. Nomophobia in Tunisian nursing students: Prevalence, associated factors, and comorbidity with generalized anxiety disorder. J. Public Health 2023. [Google Scholar] [CrossRef]
- Labrague, L.J.; McEnroe–Petitte, D.M.; De Los Santos, J.A.A.; Edet, O.B. Examining stress perceptions and coping strategies among Saudi nursing students: A systematic review. Nurse Educ. Today 2018, 65, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Purwandari, R.; Afandi, A.T.; Amini, D.A.; Ardiana, A.; Kurniawan, D.E. The overview of self-efficacy among nursing students. Babali Nurs. Res. 2023, 4, 100–108. [Google Scholar] [CrossRef]
- Li, M.; Eschenauer, R.; Persaud, V. Between Avoidance and Problem Solving: Resilience, Self-Efficacy, and Social Support Seeking. J. Couns. Dev. 2018, 96, 132–143. [Google Scholar] [CrossRef]
- Manana, M. Prevalence and Risk Factors for Anxiety Symptoms Among Student Nurses in Gauteng Province of South Africa. Behav. Sci. 2023, 13, 630. [Google Scholar] [CrossRef]
- Gnardellis, C. Nomophobia and Its Association With Depression, Anxiety and Stress (DASS Scale), Among Young Adults in Greece. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 2765–2778. [Google Scholar] [CrossRef]
- Humood, A.; Altooq, N.; Altamimi, A.; Almoosawi, H.; Alzafiri, M.; Bragazzi, N.L.; Husni, M.; Jahrami, H. The Prevalence of Nomophobia by Population and by Research Tool: A Systematic Review, Meta-Analysis, and Meta-Regression. Psych 2021, 3, 249–258. [Google Scholar] [CrossRef]
- O’Day, E.; Morrison, A.S.; Goldin, P.R.; Gross, J.J.; Heimberg, R.G. Social Anxiety, Loneliness, and the Moderating Role of Emotion Regulation. J. Soc. Clin. Psychol. 2019, 38, 751–773. [Google Scholar] [CrossRef]
- Ju, W.; Wu, Y.; Yu, T. Temporal Associations Among Loneliness, Anxiety, and Depression During the COVID-19 Pandemic Period. Stress Health 2021, 38, 90–101. [Google Scholar] [CrossRef]
- Okruszek, Ł.; Aniszewska-Stańczuk, A.; Piejka, A.; Wiśniewska, M.; Żurek, K. Safe but Lonely? Loneliness, Anxiety, and Depression Symptoms and COVID-19. Front. Psychol. 2020, 11, 579181. [Google Scholar] [CrossRef]
- Palgi, Y.; Shrira, A.; Ring, L.; Bodner, E.; Avidor, S.; Bergman, Y.S.; Cohen-Fridel, S.; Keisari, S.; Hoffman, Y. The Loneliness Pandemic: Loneliness and Other Concomitants of Depression, Anxiety and Their Comorbidity During the COVID-19 Outbreak. J. Affect. Disord. 2020, 275, 109–111. [Google Scholar] [CrossRef]
- Ebesutani, C.; Fierstein, M.; Viana, A.G.; Trent, L.R.; Young, J.; Sprung, M. The Role of Loneliness in the Relationship Between Anxiety and Depression in Clinical and School-Based Youth. Psychol. Sch. 2015, 52, 223–234. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).