
Psychopathology Present in Women after Miscarriage or Perinatal Loss: A Systematic Review



Abstract
1. Introduction
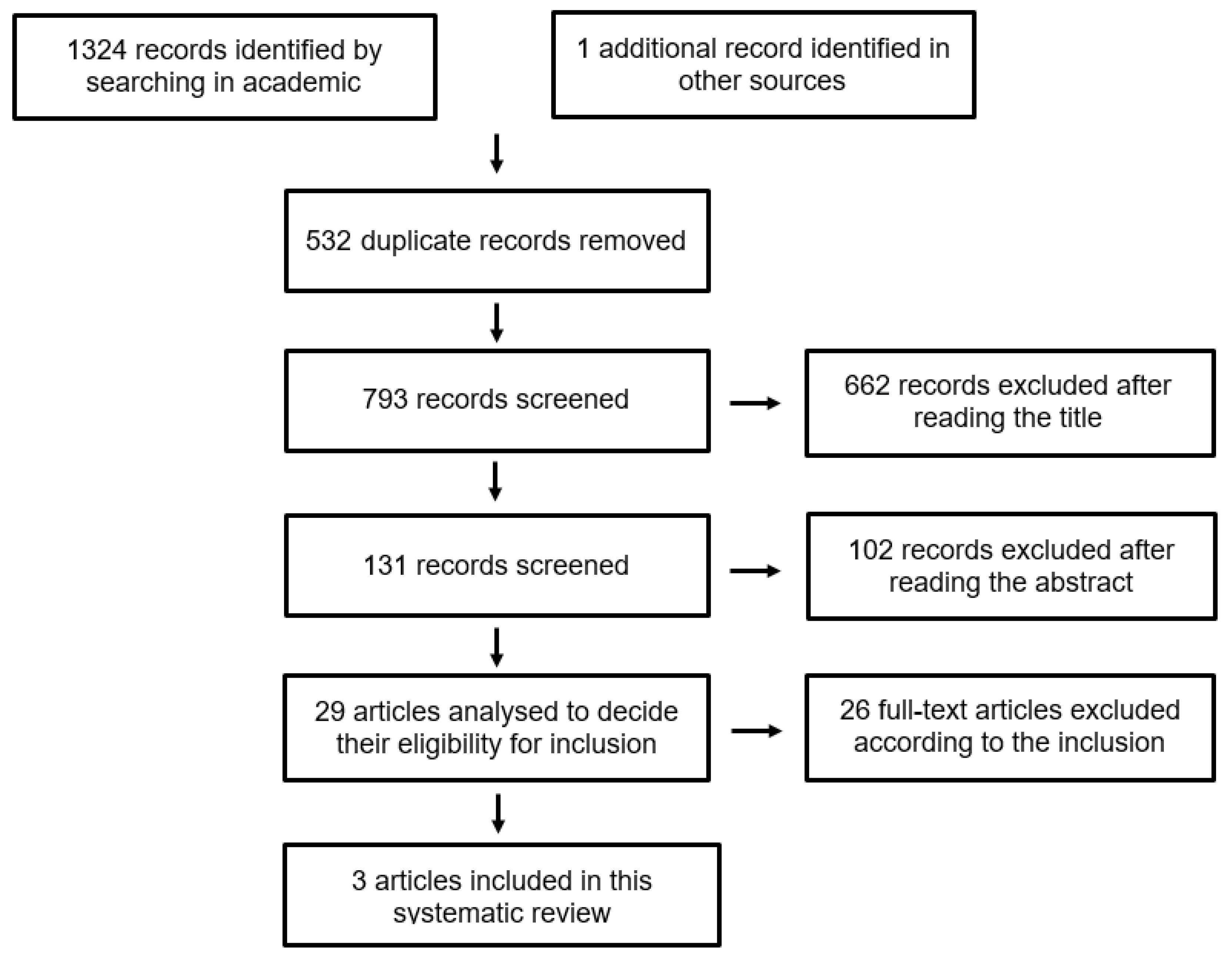
2. Materials and Methods
- -
- Studies that included women of any age who had had a miscarriage or perinatal loss in the last year;
- -
- Studies with a longitudinal cohort design with a comparison group comprising women who had not had a miscarriage or perinatal loss.
- -
- Studies focused on women who had had a recurrent miscarriage, recurrent perinatal loss, or an abortion;
- -
- Studies that included women who had had a miscarriage or perinatal loss more than one year ago;
- -
- Studies that referred to psychopathology present in the non-pregnant partner;
- -
- Studies published in a language other than English or Spanish;
- -
- Book chapters, conference communications, opinion articles, or documents other than scientific articles;
- -
- Meta-analyses, case-controlled studies, studies with qualitative designs, or design types other than longitudinal cohorts.
3. Results
3.1. Characteristics of the Studies Included
- -
- Jacob, et al., 2017 [14], analyzed 24,316 German women aged 19–54 years and the impact of miscarriage on the occurrence of anxiety and depression over 12 months;
- -
- Farren, et al., 2019 [15], analyzed 908 British women aged 16–45 years and the impact of miscarriage on the occurrence of anxiety, depression and PTSD over 9 months;
- -
- Lewkowitz, et al., 2019 [16], analyzed 1,206,050 US women aged 13–54 years and the impact of perinatal loss on the occurrence of anxiety, depression, and PTSD over 12 months.
3.2. Presence of Psychopathology
3.2.1. Anxiety
3.2.2. Depression
3.2.3. Post-Traumatic Stress Disorder
3.2.4. Psychopathology, Age and Psychiatric History
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leisher, S.H.; Teoh, Z.; Reinebrant, H.; Allanson, J.J.E.; Blencowe, H.; Erwich, J.J.; Frøen, J.F.; Gardosi, J.; Gordijn, S.; Gülmezoglu, A.M.; et al. Classification systems for causes of stillbirth and neonatal death, 2009–2014: An assessment of alignment with characteristics for an effective global system. BMC Pregnancy Childbirth 2016, 16, 269. [Google Scholar] [CrossRef] [PubMed]
- Lawn, J.E.; Blencowe, H.; Pattinson, R.; Cousens, S.; Kumar, R.; Ibiebele, I.; Gardosi, J.; Day, L.T.; Stanton, C. Stillbirths: Where? When? Why? How to make the data count? Lancet 2011, 377, 1448–1463. [Google Scholar] [CrossRef] [PubMed]
- Quenby, S.; Gallos, I.D.; Dhillon-Smith, R.K.; Podesek, M.; Stephenson, M.D.; Fisher, J.; Brosens, J.J.; Brewin, J.; Ramhorst, R.; Lucas, E.S.; et al. Miscarriage matters: The epidemiological, physical, psychological, and economic costs of early pregnancy loss. Lancet 2021, 397, 1658–1667. [Google Scholar] [CrossRef] [PubMed]
- Linnakaari, R.; Helle, N.; Mentula, M.; Bloigu, A.; Gissler, M.; Heikinheimo, O.; Niinimäki, M. Trends in the incidence, rate and treatment of miscarriage—Nationwide register-study in Finland, 1998–2016. Hum. Reprod. 2019, 34, 2120–2128. [Google Scholar] [CrossRef]
- Oiberman, A. Nacer y Después…: Aportes a la Psicología Perinatal; JCE: Buenos Aires, Argentina, 2005. [Google Scholar]
- Soifer, R. Psicología del Embarazo, Parto y Puerperio; Kargieman: Buenos Aires, Argentina, 1977. [Google Scholar]
- Bydlowski, M. La Deuda de la Vida: Itinerario Psicoanalítico de la Maternidad; Biblioteca Nueva: Madrid, Spain, 2007. [Google Scholar]
- Guclu, O.; Senormanci, G.; Tuten, A.; Gok, K.; Senormanci, O. Perinatal Grief and Related Factors After Termination of Pregnancy for Fetal Anomaly: One-Year Follow-up Study. Arch. Neuropsychiatry 2021, 58, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Moscarello, R. Perinatal Bereavement Support Service: Three-Year Review. J. Palliat. Care 1989, 5, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Parkes, C.M. Coping with Loss: Bereavement in Adult Life. BMJ 1998, 316, 856–859. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1112778/ (accessed on 21 May 2022). [CrossRef]
- Gravensteen, I.K.; Jacobsen, E.-M.; Sandset, P.M.; Helgadottir, L.B.; Rådestad, I.; Sandvik, L.; Ekeberg, Ø. Anxiety, Depression and Relationship Satisfaction in the Pregnancy Following Stillbirth and after the Birth of a Live-Born Baby: A Prospective Study. BMC Pregnancy Childbirth 2018, 18, 41. Available online: https://bmcpregnancychildbirth.biomedcentral.com/articles/10.1186/s12884-018-1666-8 (accessed on 21 May 2022). [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Instrumentos Para la Lectura Crítica. Redcaspe.org. CASPe. 2020. Available online: https://redcaspe.org/materiales/ (accessed on 30 May 2022).
- Jacob, L.; Polly, I.; Kalder, M.; Kostev, K. Prevalence of depression, anxiety, and adjustment disorders in women with spontaneous abortion in Germany—A retrospective cohort study. Psychiatry Res. 2017, 258, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Farren, J.; Jalmbrant, M.; Falconieri, N.; Mitchell-Jones, N.; Bobdiwala, S.; Al-Memar, M.; Bourne, T. Posttraumatic stress, anxiety and depression following miscarriage and ectopic pregnancy: A multicenter, prospective, cohort study. Am. J. Obstet. Gynecol. 2019, 222, 367.e1–367.e22. [Google Scholar] [CrossRef] [PubMed]
- Lewkowitz, A.K.; Rosenbloom, J.I.; Keller, M.; López, J.D.; Macones, G.A.; Olsen, M.A.; Cahill, A.G. Association between stillbirth ≥ 23 weeks gestation and acute psychiatric illness within 1 year of delivery. Am. J. Obstet. Gynecol. 2019, 221, 491.e1–491.e22. [Google Scholar] [CrossRef]
- Hughes, P.M.; Turton, P.; Evans, C.D.H. Stillbirth as risk factor for depression and anxiety in the subsequent pregnancy: Cohort study. BMJ 1999, 318, 1721–1724. [Google Scholar] [CrossRef]
- Volgsten, H.; Jansson, C.; Svanberg, A.S.; Darj, E.; Stavreus-Evers, A. Longitudinal study of emotional experiences, grief and depressive symptoms in women and men after miscarriage. Midwifery 2018, 64, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Ridaura, I. Depressive symptomatology and grief in Spanish women who have suffered a perinatal loss. Psicothema 2017, 29, 43–48. [Google Scholar]
- Bennett, S.M.; Litz, B.T.; Maguen, S.; Ehrenreich, J.T. An Exploratory Study of the Psychological Impact and Clinical Care of Perinatal Loss. J. Loss Trauma 2008, 13, 485–510. [Google Scholar] [CrossRef]
- Cacciatore, J. The Unique Experiences of Women and Their Families after the Death of a Baby. Soc. Work. Health Care 2010, 49, 134–148. [Google Scholar] [CrossRef]
- Urie, B. La Ecología del Desarrollo Humano; Ediciones Paidos Ibérica S.A.: Barcelona, Spain, 1987; ISBN 84-7509-444-9. [Google Scholar]
- Martos-López, I.M.; del Sánchez-Guisado, M.; Guedes-Arbelo, C. Duelo por muerte perinatal, un duelo desautorizado = Bereavement for perinatal death, unauthorized bereavement. Rev. Española De Comun. En Salud 2016, 7, 300–309. [Google Scholar] [CrossRef]
- Sánchez, I.; Universidad de Alicante. Duelo Desautorizado: Todo lo Que Rodea a un Duelo Tabú. 2019. Available online: https://rua.ua.es/dspace/bitstream/10045/92853/1/DUELO_DESAUTORIZADO_TODO_LO_QUE_RODEA_A_UN_DUELO_TABU_Sanchez_Perez_Ines.pdf (accessed on 20 June 2022).
- Ridaura, I. Estudio del Duelo Perinatal: Interrupciones Médicas del Embarazo, Muertes Prenatales y Muertes Postnatales. 2015. Available online: https://ddd.uab.cat/pub/tesis/2015/hdl_10803_295973/irp1de1.pdf (accessed on 20 June 2022).
- Parkes, C.M. Determinants of Outcome following Bereavement. OMEGA J. Death Dying 1976, 6, 303–323. [Google Scholar] [CrossRef]
- Sutan, R.; Miskham, H.M. Psychosocial impact of perinatal loss among Muslim women. BMC Women’s Health 2012, 12, 15. [Google Scholar] [CrossRef] [PubMed]
- Leinweber, J.; Fontein-Kuipers, Y.; Thomson, G.; Karlsdottir, S.I.; Nilsson, C.; Ekström-Bergström, A.; Olza, I.; Hadjigeorgiou, E.; Stramrood, C. Developing a woman-centered, inclusive definition of traumatic childbirth experiences: A discussion paper. Birth 2022, 49, 687–696. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Almagro, J.; Hernández-Martínez, A.; Rodríguez-Almagro, D.; Quirós-García, J.M.; Martínez-Galiano, J.M.; Gómez-Salgado, J. Women’s Perceptions of Living a Traumatic Childbirth Experience and Factors Related to a Birth Experience. Int. J. Environ. Res. Public Health 2019, 16, 1654. [Google Scholar] [CrossRef] [PubMed]
- Gálvez Toro, A.; Amezcua, M.; Salido Moreno, M.P. La construcción social de los sentimientos. La muerte del sujeto que nace. Index De Enfermería 2002, 11, 29–34. [Google Scholar]
- Bowlby, J. El Apego y la Pérdida; Ediciones Paidos Ibérica S.A.: Barcelona, Spain, 1993. [Google Scholar]
- Boyle, F.M.; Vance, J.C.; Najman, J.M.; Thearle, M.J. The mental health impact of stillbirth, neonatal death or SIDS: Prevalence and patterns of distress among mothers. Soc. Sci. Med. 1996, 43, 1273–1282. [Google Scholar] [CrossRef] [PubMed]
- Lok, I.H.; Yip, A.S.-K.; Lee, D.T.-S.; Sahota, D.; Chung, T.K.-H. A 1-year longitudinal study of psychological morbidity after miscarriage. Fertil. Steril. 2010, 93, 1966–1975. [Google Scholar] [CrossRef] [PubMed]
- Kulathilaka, S.; Hanwella, R.; de Silva, V.A. Depressive Disorder and Grief Following Spontaneous Abortion. BMC Psychiatry 2016, 16, 100. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4830021/pdf/12888_2016_Article_812.pdf (accessed on 25 June 2022). [CrossRef]
- Adane, A.A.; Bailey, H.D.; Morgan, V.A.; Galbally, M.; Farrant, B.M.; Marriott, R.; White, S.W.; Shepherd, C.C. The impact of maternal prenatal mental health disorders on stillbirth and infant mortality: A systematic review and meta-analysis. Arch. Women’s Ment. Health 2021, 24, 543–555. [Google Scholar] [CrossRef]
- Farren, J.; Jalmbrant, M.; Falconieri, N.; Mitchell-Jones, N.; Bobdiwala, S.; Al-Memar, M.; Parker, N.; Van Calster, B.; Timmerman, D.; Bourne, T. Prognostic factors for post-traumatic stress, anxiety and depression in women after early pregnancy loss: A multi-centre prospective cohort study. BMJ Open 2022, 12, e054490. [Google Scholar] [CrossRef]
- San Lazaro Campillo, I.; Meaney, S.; McNamara, K.; O’Donoghue, K. Psychological and support interventions to reduce levels of stress, anxiety or depression on women’s subsequent pregnancy with a history of miscarriage: An empty systematic review. BMJ Open 2017, 7, e017802. [Google Scholar] [CrossRef]
- Gold, K.J.; Johnson, T.R.B. Mothers at Risk. Obstet. Gynecol. 2014, 123, 6S. [Google Scholar] [CrossRef]
- Martínez Miguel, E. Propuesta de un Programa de Apoyo Y Seguimiento Para Padres en Proceso de Duelo Perinatal. Universidad de Lleida, Editor. 2016. Available online: https://repositori.udl.cat/bitstream/handle/10459.1/57605/emartinezm.pdf?sequence=1 (accessed on 21 July 2022).


{kind=link}
| Physical | Empty stomach; chest and throat tightness; shortness of breath; weakness; fatigue; and sweating. |
| Behavioral | Difficulty sleeping; nightmares; poor appetite; social withdrawal; substance use and abuse; avoidance of health situations, pregnant women and children; and limited social and occupational functioning. |
| Emotional | Shock; guilt; emptiness; anger; anxiety; sadness; reproach; confusion; disbelief; derealization; depersonalization; and loneliness. |
| Cognitive | Re-experiencing the trauma with intrusive ideas and fantasies about the fetus; ‘‘phantom’’ fetal movements; auditory and/or visual hallucinations with the fetus; difficulties concentrating and making decisions. |
| Author | Year | Country | Age | Type of Loss | Psychopathology | Miscarriage/Perinatal Loss Sample Size | Control Sample | Monitoring |
|---|---|---|---|---|---|---|---|---|
| Jacob, et al. [14] | 2017 | Germany | 16–45 | Miscarriage | Anxiety, depression | 12,158 | 12,158 | 12 months |
| Farren, et al. [15] | 2019 | United Kingdom | 19–54 | Miscarriage | Anxiety, depression, PTSD | 737 | 171 | 9 months |
| Lewkowitz, et al. [16] | 2019 | United States | 13–54 | Perinatal loss | Anxiety, depression, PTSD | 8292 | 1,194,758 | 12 months |
| Study | Psychopathology | Miscarriage/Perinatal Loss Group | Control Group | Odds Ratio |
|---|---|---|---|---|
| Jacob, et al., 2017 [14] | Anxiety | 2.4% | 2.1% | OR = 1.49; 95% CI [1.30, 1.70] |
| Depression | 3.1% | 1.2% | OR = 1.66; 95% CI [1.46, 1.89] | |
| Farren, et al., 2019 [15] | Anxiety | 24% (1 month) | 13% | aOR = 2.14; 95% CI [1.14, 4.36] |
| 22% (6 months) | ||||
| 17% (9 months) | ||||
| Depression | 12% (1 month) | 2% | aOR = 3.88; 95% CI [1.27, 19.2] | |
| 8% (6 months) | ||||
| 6% (9 months) | ||||
| PTSD | 29% (1 month) | |||
| 21% (6 months) | ||||
| 18% (9 months) | ||||
| Lewkowitz et al., 2019 [16] | Anxiety | 2.1% | 0.8% | aOR = 2.29; 95% CI [1.93, 2.70] |
| Depression | 1.7% | 0.6% | aOR = 2.75; 95% CI [2.31, 3.26] | |
| PTSD | 0.03% | aOR = 4.23; 95% CI [1.98, 9.04] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Díaz-Pérez, E.; Haro, G.; Echeverria, I. Psychopathology Present in Women after Miscarriage or Perinatal Loss: A Systematic Review. Psychiatry Int. 2023, 4, 126-135. https://doi.org/10.3390/psychiatryint4020015
Díaz-Pérez E, Haro G, Echeverria I. Psychopathology Present in Women after Miscarriage or Perinatal Loss: A Systematic Review. Psychiatry International. 2023; 4(2):126-135. https://doi.org/10.3390/psychiatryint4020015
Chicago/Turabian StyleDíaz-Pérez, Elisa, Gonzalo Haro, and Iván Echeverria. 2023. "Psychopathology Present in Women after Miscarriage or Perinatal Loss: A Systematic Review" Psychiatry International 4, no. 2: 126-135. https://doi.org/10.3390/psychiatryint4020015
APA StyleDíaz-Pérez, E., Haro, G., & Echeverria, I. (2023). Psychopathology Present in Women after Miscarriage or Perinatal Loss: A Systematic Review. Psychiatry International, 4(2), 126-135. https://doi.org/10.3390/psychiatryint4020015