
The Emotional Resources Group: A Mixed Methods Practice-Based Study of a Transdiagnostic Emotion Regulation Group Intervention


Abstract
1. Introduction
1.1. Emotion Regulation Group Interventions
1.2. The Need for Trauma-Informed Interventions
1.3. The Emotional Resources Group
1.4. The Current Research
2. Method
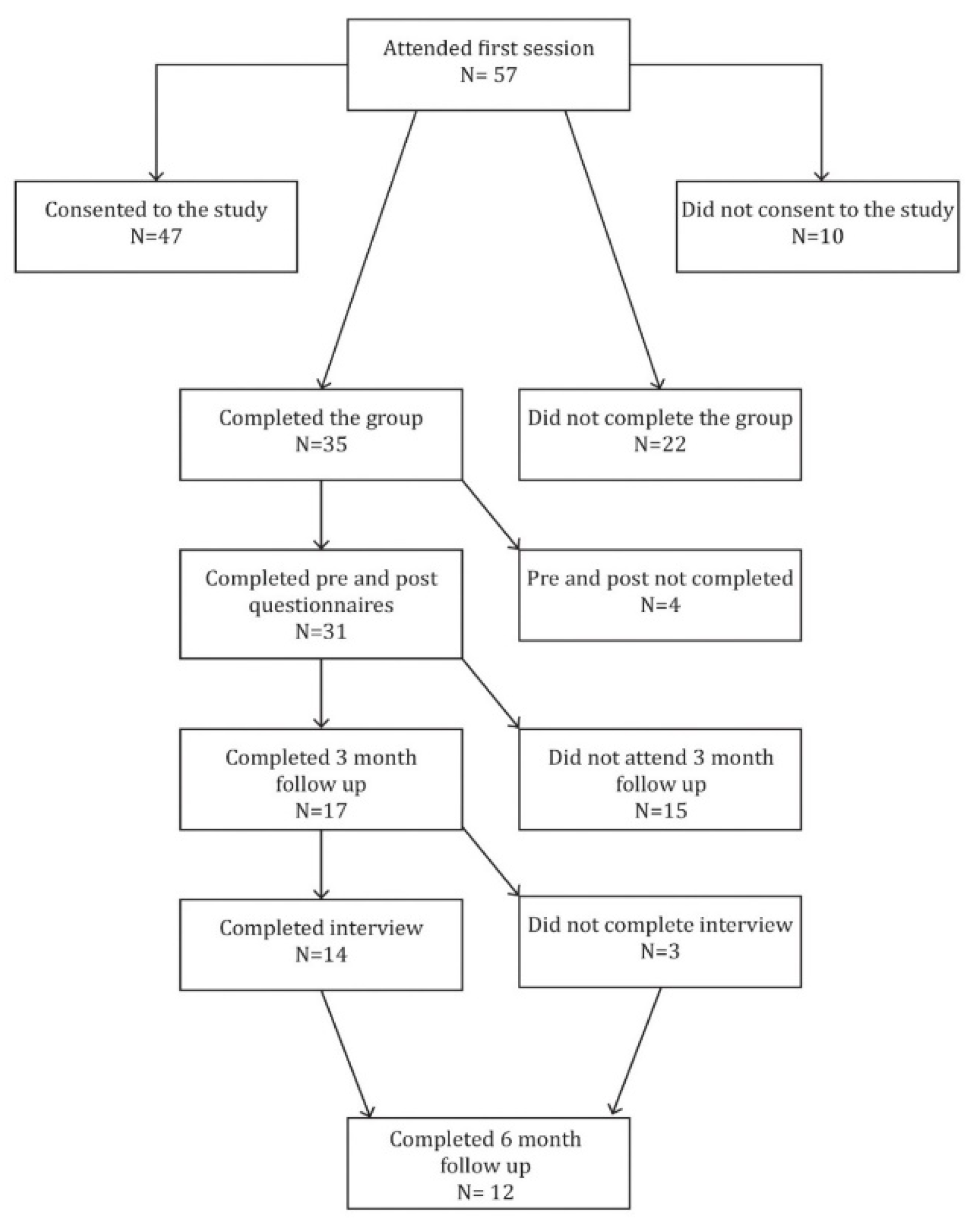
2.1. Design
2.2. Measures
2.2.1. Treatment Fidelity
2.2.2. Participants
2.3. Procedure
2.4. Qualitative Interview
2.5. Ethics
2.6. Analysis
2.6.1. Quantitative Measures
2.6.2. Qualitative Interviews
3. Results
3.1. Quantitative Results
3.2. Qualitative Results
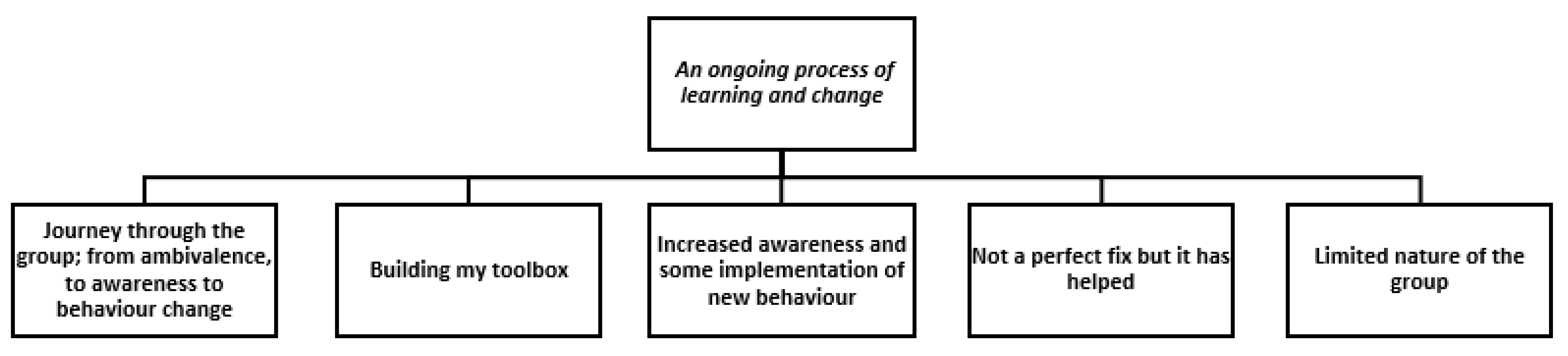
3.3. Themes
3.3.1. An Ongoing Process of Learning and Change
3.3.2. Journey through the Group; from Ambivalence, to Awareness, to Behaviour Change
3.3.3. Building My Toolbox
3.4. Increased Awareness and Some Implementation of New Behaviour
3.5. Not a Perfect Fix but It Has Helped
3.6. Limited Nature of the Group
4. Discussion
4.1. Limitations and Considerations for Further Research
4.2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blackledge, J.T.; Hayes, S.C. Emotion regulation in acceptance and commitment therapy. J. Clin. Psychol. 2001, 57, 243–255. [Google Scholar] [CrossRef]
- Fosha, D. Transforming Power of Affect: A Model for Accelerated Change; Basic Books: New York, NY, USA, 2000. [Google Scholar]
- Greenberg, L.S. Coaching Clients to Work Through Their Feelings. In Emotion-Focused Therapy, 2nd ed.; American Psychological Association: Washington, DC, USA, 2015. [Google Scholar]
- Linehan, M.M. DBT? Skills Training Handouts and Worksheets, 2nd ed.; Guilford Publications: New York, NY, USA, 2014. [Google Scholar]
- Linehan, M.M.; Bohus, M.; Lynch, T.R. Dialectical Behavior Therapy for Pervasive Emotion Dysregulation: Theoretical and Practical Underpinnings. In Handbook of Emotion Regulation; Gross, J.J., Ed.; Guilford Press: New York, NY, USA, 2007; pp. 581–605. Available online: https://eprints.soton.ac.uk/194405/ (accessed on 13 February 2020).
- Papa, A.; Boland, M.; Sewell, M.T. Emotion regulation and CBT. In Cognitive Behavior Therapy: Core Principles for Practice; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2012; pp. 273–323. [Google Scholar] [CrossRef]
- Gross, J.J. Emotion Regulation: Current Status and Future Prospects. Psychol. Inq. 2015, 26, 1–26. [Google Scholar] [CrossRef]
- Gross, J.J. Emotion regulation: Affective, cognitive, and social consequences. Psychophysiology 2002, 39, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Barrett, L.F. How Emotions Are Made: The Secret Life of the Brain; Picador: London, UK, 2017. [Google Scholar]
- Giner-Sorolla, R. The past thirty years of emotion research: Appraisal and beyond. Cogn. Emot. 2019, 33, 48–54. [Google Scholar] [CrossRef]
- Yih, J.; Uusberg, A.; Taxer, J.; Gross, J. Better together: A unified perspective on appraisal and emotion regulation. Cogn. Emot. 2018, 33, 1–7. [Google Scholar] [CrossRef]
- Ochsner, K.; Bunge, S.; Gross, J.; Gabrieli, J. Rethinking Feelings: An fMRI Study of the Cognitive Regulation of Emotion. J. Cogn. Neurosci. 2002, 14, 1215–1229. [Google Scholar] [CrossRef]
- Siemer, M.; Mauss, I.; Gross, J. Same Situation-Different Emotions: How Appraisals Shape Our Emotions. Emotion 2007, 7, 592–600. [Google Scholar] [CrossRef]
- Gross, J.J. The Emerging Field of Emotion Regulation: An Integrative Review. Rev. Gen. Psychol. 1998, 2, 271–299. [Google Scholar] [CrossRef]
- Gross, J.J.; Feldman Barrett, L. Emotion generation and emotion regulation: One or two depends on your point of view. Emot. Rev. 2011, 3, 8–16. [Google Scholar] [CrossRef]
- Kellett, S.; Clarke, S.; Matthews, L. Delivering group psychoeducational CBT in Primary Care: Comparing outcomes with individual CBT and individual psychodynamic-interpersonal psychotherapy. Br. J. Clin. Psychol. 2007, 46, 211–222. [Google Scholar] [CrossRef]
- Morrison, N. Group cognitive therapy: Treatment of choice or sub-optimal option? Behav. Cogn. Psychother. 2001, 29, 311–332. [Google Scholar] [CrossRef]
- Tucker, M.; Oei, T.P.S. Is Group More Cost Effective than Individual Cognitive Behaviour Therapy? The Evidence is not Solid Yet. Behav. Cogn. Psychother. 2007, 35, 77–91. [Google Scholar] [CrossRef]
- Gratz, K.L.; Gunderson, J.G. Preliminary Data on an Acceptance-Based Emotion Regulation Group Intervention for Deliberate Self-Harm Among Women with Borderline Personality Disorder. Behav. Ther. 2006, 37, 25–35. [Google Scholar] [CrossRef]
- Harvey, R.; Black, D.W.; Blum, N. Systems Training for Emotional Predictability and Problem Solving (STEPPS) in the United Kingdom: A Preliminary Report. J. Contemp. Psychother. 2010, 40, 225–232. [Google Scholar] [CrossRef]
- Blum, N.; St. John, D.; Pfohl, B.; Stuart, S.; McCormick, B.; Allen, J.; Arndt, S.; Black, D.W. Systems Training for Emotional Predictability and Problem Solving (STEPPS) for Outpatients with Borderline Personality Disorder: A Randomized Controlled Trial and 1-Year Follow-Up. Am. J. Psychiatry 2008, 165, 468–478. [Google Scholar] [CrossRef]
- Dixon-Gordon, K.L.; Chapman, A.L.; Turner, B.J. A Preliminary Pilot Study Comparing Dialectical Behavior Therapy Emotion Regulation Skills with Interpersonal Effectiveness Skills and a Control Group Treatment. J. Exp. Psychopathol. 2015, 6, 369–388. [Google Scholar] [CrossRef]
- Rizvi, S.L.; Steffel, L.M. A Pilot Study of 2 Brief Forms of Dialectical Behavior Therapy Skills Training for Emotion Dysregulation in College Students. J. Am. Coll. Health 2014, 62, 434–439. [Google Scholar] [CrossRef]
- Gratz, K.L.; Roemer, L. Multidimensional Assessment of Emotion Regulation and Dysregulation: Development, Factor Structure, and Initial Validation of the Difficulties in Emotion Regulation Scale. J. Psychopathol. Behav. Assess. 2008, 30, 315. [Google Scholar] [CrossRef]
- Bullis, J.R.; Sauer-Zavala, S.; Bentley, K.H.; Thompson-Hollands, J.; Carl, J.R.; Barlow, D.H. The unified protocol for transdiagnostic treatment of emotional disorders: Preliminary exploration of effectiveness for group delivery. Behav. Modif. 2015, 39, 295–321. [Google Scholar] [CrossRef]
- Berking, M.; Wupperman, P.; Reichardt, A.; Pejic, T.; Dippel, A.; Znoj, H. Emotion-regulation skills as a treatment target in psychotherapy. Behav. Res. Ther. 2008, 46, 1230–1237. [Google Scholar] [CrossRef]
- McKay, M.; West, A. Emotion Efficacy Therapy: A Brief, Exposure-Based Treatment for Emotion Regulation Integrating ACT and DBT, 1st ed.; Context Press: Oakland, CA, USA, 2016. [Google Scholar]
- Tehranirad, S. A Comparison of the Effectiveness of a Transdiagnostic Group Protocol (Mind & Emotions) Versus Three Modules of Dialectical Behavior Therapy for Mild to Severe Emotional Dysregulation; Psy.D., The Wright Institute: Berkeley, CA, USA, 2016; Available online: http://search.proquest.com/docview/1901459507/abstract/FA622560CF044084PQ/1 (accessed on 13 February 2020).
- Bacon, T.; Doughty, C.; Summers, A.; Wiffen, B.; Stanley, Z.; McAlpine, S. The Emotional Resources Group: Provisional outcome data for a pilot six-session emotion regulation programme for secondary care. Br. J. Clin. Psychol. 2018, 57, 223–239. [Google Scholar] [CrossRef] [PubMed]
- Álvarez, M.-J.; Roura, P.; Osés, A.; Foguet, Q.; Solà, J.; Arrufat, F.-X. Prevalence and Clinical Impact of Childhood Trauma in Patients with Severe Mental Disorders. J. Nerv. Ment. Dis. 2011, 199, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Dillon, J.; Johnstone, L.C.; Longden, E. Trauma, dissociation, attachment and neuroscience: A new paradigm for understanding severe mental distress. In De-Medicalizing Misery II; Palgrave Macmillan: London, UK, 2014; pp. 226–234. [Google Scholar] [CrossRef]
- Rossiter, A.; Byrne, F.; Wota, A.P.; Nisar, Z.; Ofuafor, T.; Murray, I.; Byrne, C.; Hallahan, B. Childhood trauma levels in individuals attending adult mental health services: An evaluation of clinical records and structured measurement of childhood trauma. Child Abus. Negl. 2015, 44, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Wu, N.S.; Schairer, L.C.; Dellor, E.; Grella, C. Childhood trauma and health outcomes in adults with comorbid substance abuse and mental health disorders. Addict. Behav. 2010, 35, 68–71. [Google Scholar] [CrossRef] [PubMed]
- Cloitre, M.; Khan, C.; Mackintosh, M.-A.; Garvert, D.; Henn-Haase, C.; Falvey, E.; Saito, J. Emotion Regulation Mediates the Relationship Between ACES and Physical and Mental Health. Psychol. Trauma: Theory Res. Pract. Policy 2019, 11, 82–89. [Google Scholar] [CrossRef]
- Bacon, T.; Stanley, Z.; Manual for the Emotional Resources Group. Unpublished Manuscript. 2016.
- Koole, S.L. The psychology of emotion regulation: An integrative review. Cogn. Emot. 2009, 23, 4–41. [Google Scholar] [CrossRef]
- Ogles, B.M.; Lambert, M.J.; Fields, S.A. Essentials of Outcome Assessment, 1st ed.; Wiley: Hoboken, NJ, USA, 2002. [Google Scholar]
- Langkaas, T.F.; Wampold, B.E.; Hoffart, A. Five types of clinical difference to monitor in practice. Psychotherapy 2018, 55, 241–254. [Google Scholar] [CrossRef]
- Carpinello, S.E.; Knight, E.L.; Markowitz, F.E.; Pease, E.A. The development of the Mental Health Confidence Scale: A measure of self-efficacy in individuals diagnosed with mental disorders. Psychiatr. Rehabil. J. 2000, 23, 236–243. [Google Scholar] [CrossRef]
- Stewart-Brown, S.L.; Platt, S.; Tennant, A.; Maheswaran, H.; Parkinson, J.; Weich, S.; Tennant, R.; Taggart, F.; Clarke, A. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): A valid and reliable tool for measuring mental well-being in diverse populations and projects. J. Epidemiol. Comm, Health 2011, 65 (Suppl. S2), A38–A39. [Google Scholar] [CrossRef]
- Mundt, J.C.; Marks, I.M.; Shear, M.K.; Greist, J.M. The Work and Social Adjustment Scale: A simple measure of impairment in functioning. Br. J. Psychiatry 2002, 180, 461–464. [Google Scholar] [CrossRef]
- Zahra, D.; Qureshi, A.; Henley, W.; Taylor, R.; Quinn, C.; Pooler, J.; Hardy, G.; Newbold, A.; Byng, R. The work and social adjustment scale: Reliability, sensitivity and value. Int. J. Psychiatry Clin. Pract. 2014, 18, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.; Rief, W.; Klaiberg, A.; Braehler, E. Validity of the Brief Patient Health Questionnaire Mood Scale (PHQ-9) in the general population. Gen. Hosp. Psychiatry 2006, 28, 71–77. [Google Scholar] [CrossRef] [PubMed]
- CORE Outcome Measurement Tools. (n.d.). Available online: http://www.coreims.co.uk/About_Measurement_CORE_Tools.html (accessed on 14 April 2020).
- Barkham, M.; Bewick, B.; Mullin, T.; Gilbody, S.; Connell, J.; Cahill, J.; Mellor-Clark, J.; Richards, D.; Unsworth, G.; Evans, C. The CORE-10: A short measure of psychological distress for routine use in the psychological therapies. Couns. Psychother. Res. 2013, 13, 3–13. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Successful Qualitative Research: A Practical Guide for Beginners; SAGE: Newbury Park, CA, USA, 2013. [Google Scholar]
- Field, A.P. Discovering Statistics Using IBM SPSS Statistics, 5th ed.; SAGE: Newbury Park, CA, USA, 2018. [Google Scholar]
- Hayes, S.C. Acceptance and commitment therapy, relational frame theory, and the third wave of behavioral and cognitive therapies. Behav. Ther. 2004, 35, 639–665. [Google Scholar] [CrossRef]
- Bouton, M.E.; Westbrook, R.F.; Corcoran, K.A.; Maren, S. Contextual and Temporal Modulation of Extinction: Behavioral and Biological Mechanisms. Biol. Psychiatry 2006, 60, 352–360. [Google Scholar] [CrossRef]
- Nilsen, P.; Roback, K.; Broström, A.; Ellström, P.-E. Creatures of habit: Accounting for the role of habit in implementation research on clinical behaviour change. Implement. Sci. 2012, 7, 53. [Google Scholar] [CrossRef]
- Lyng, J.; Swales, M.A.; Hastings, R.P.; Millar, T.; Duffy, D.J.; Booth, R. Standalone DBT Group Skills Training Versus Standard (i.e. All Modes) DBT for Borderline Personality Disorder: A Natural Quasi-experiment in Routine Clinical Practice. Commun. Ment. Health J. 2020, 56, 238–250. [Google Scholar] [CrossRef]
- Neacsiu, A.D.; Eberle, J.W.; Kramer, R.; Wiesmann, T.; Linehan, M.M. Dialectical behavior therapy skills for transdiagnostic emotion dysregulation: A pilot randomized controlled trial. Behav. Res. Ther. 2014, 59, 40–51. [Google Scholar] [CrossRef]
- Daly, M.; Sutin, A.R.; Robinson, E. Longitudinal changes in mental health and the COVID-19 pandemic: Evidence from the UK Household Longitudinal Study. Psychol. Med. 2020, 13, 1–10. [Google Scholar] [CrossRef]
- Serafini, G.; Parmigiani, B.; Amerio, A.; Aguglia, A.; Sher, L.; Amore, M. The psychological impact of COVID-19 on the mental health in the general population. QJM Int. J. Med. 2020, 113, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Ford, J.D.; Chang, R.; Levine, J.; Zhang, W. Randomized Clinical Trial Comparing Affect Regulation and Supportive Group Therapies for Victimization-Related PTSD With Incarcerated Women. Behav. Ther. 2013, 44, 262–276. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.; Gillanders, D.; Stuart, S. The impact of group emotion regulation interventions on emotion regulation ability: A systematic review. J. Clin. Med. 2022, 11, 2519. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Measure | Baseline n = 31 | End of ERG n = 31 | T (30) T (27) | Cohen’s d | 3 Month n = 12 | 6 Month n = 12 | Within F F(3,33) F(1.657,18.232) ε | Partial ω2 | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||||||
| Difficulties in Emotion Regulation Scale (DERS) ‡ | |||||||||||||
| 128.94 a | 21.97 | 114.06 b | 26.79 | 4.23 ** | 0.76 | 118.33 a | 24.74 | 113.08 a | 29.28 | 2.60 | § p = 0.69 ns | 0.11 | |
| Subscales: NONACCEPT | n = 28 | n = 28 | |||||||||||
| 20.75 a | 5.69 | 19.36 a | 6.32 | 1.75 ns ¶ | 0.33 | ||||||||
| GOALS | |||||||||||||
| 20.21 a | 4.10 | 18.71 b | 4.45 | 2.25 ns ¶ | 0.43 | ||||||||
| CLARITY | |||||||||||||
| 15.52 a | 3.62 | 14.82 b | 3.23 | 2.43 ns ¶ | 0.46 | ||||||||
| AWARENESS | |||||||||||||
| 19.71 a | 3.63 | 18.75 a | 3.79 | 1.48 ns ¶ | 0.28 | ||||||||
| IMPULSE | |||||||||||||
| 21.71 a | 5.21 | 18.86 b | 5.10 | 4.18 * ¶ | 0.84 | ||||||||
| STRATEGIES | |||||||||||||
| 29.68 a | 6.33 | 26.21 b | 6.26 | 3.91 * ¶ | 0.74 | ||||||||
| CORE-10 ‡ | 24.71 a | 6.70 | 19.87 b | 8.18 | 3.62 ** | 0.65 | 22.25 a | 8.25 | 20.42 a | 8.93 | 1.88 | p = 0.19 ns | 0.05 |
| Work and Social Adjustment Scale (WSAS) ‡ | 28.02 a | 7.94 | 25.39 b | 8.31 | 2.28 * | 0.41 | 25.58 a | 7.79 | 25.58 a | 8.70 | 1.05 | p = 0.70 ns | <0.00 |
| Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS) † | 32.53 a | 8.68 | 39.50 b | 9.78 | 4.48 ** | 0.81 | 37.75 a | 7.46 | 38.50 a | 7.65 | 2.90 * | 0.11 | |
| Mental Health Confidence scale (MHCS) † | 46.35 a | 12.19 | 53.87 b | 15.62 | 3.93 * | 0.61 | 55.75 a | 12.26 | 56.42 a | 10.82 | 2.38 | p = 0.09 ns | 0.08 |
| Participant Pseudonym | Gender | Age Range | Self-Described Difficulty | Previous Use of Mental Health Services | Individually Therapy Arranged after ERG |
|---|---|---|---|---|---|
| David | Male | 36–45 | OCD | No | Yes |
| Stacey | Female | 46–55 | Anxiety and depression | Yes | Yes |
| Sally | Female | 16–25 | EUPD/BPD | Yes | Yes |
| Nicola | Female | 26–35 | Trauma | Yes | No |
| Yvonne | Female | 16–25 | Not stated | Yes | Yes |
| Florence | Female | 56–65 | Depression | Yes | No |
| Phoebe | Female | 26–35 | Trauma | Yes | No |
| Eilidh | Female | 16–25 | Not stated | Yes | No |
| Danielle | Female | 46–55 | Trauma | Yes | No |
| Mary | Female | 36–45 | Anxiety and depression | Yes | Yes |
| Andrea | Female | 46–55 | Anxiety and depression | No | Yes |
| Charlotte | Female | 26–35 | Depression | Yes | Yes |
| Gabby | Female | 16–25 | Not stated | No | Yes |
| Heather | Female | 26–35 | EUPD/BPD | Yes | Yes |
| Theme Participant | An Ongoing Process of Learning and Change | Journey through the Group; from Ambivalence, to Awareness to Behaviour Change | Building My Toolbox | Increased Awareness and Some Implementation of New Behaviour | Not a Perfect Fix but It Has Helped | Limited Nature of the Group |
|---|---|---|---|---|---|---|
| David | √ | √ | √ | √ | √ | |
| Stacey | √ | √ | √ | |||
| Sally | √ | √ | √ | √ | ||
| Nicola | √ | √ | √ | √ | √ | √ |
| Yvonne | √ | √ | √ | √ | √ | √ |
| Florence | √ | √ | ||||
| Phoebe | √ | √ | √ | √ | √ | √ |
| Eilidh | √ | √ | √ | √ | √ | √ |
| Danielle | √ | √ | √ | √ | √ | |
| Mary | √ | √ | √ | √ | √ | √ |
| Andrea | √ | √ | √ | √ | √ | √ |
| Charlotte | √ | √ | √ | √ | √ | √ |
| Gabby | √ | √ | √ | √ | √ | √ |
| Heather | √ | √ | √ | √ | √ | √ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moore, R.; Gillanders, D.; Stuart, S. The Emotional Resources Group: A Mixed Methods Practice-Based Study of a Transdiagnostic Emotion Regulation Group Intervention. Psychiatry Int. 2022, 3, 297-312. https://doi.org/10.3390/psychiatryint3040024
Moore R, Gillanders D, Stuart S. The Emotional Resources Group: A Mixed Methods Practice-Based Study of a Transdiagnostic Emotion Regulation Group Intervention. Psychiatry International. 2022; 3(4):297-312. https://doi.org/10.3390/psychiatryint3040024
Chicago/Turabian StyleMoore, Rebekah, David Gillanders, and Simon Stuart. 2022. "The Emotional Resources Group: A Mixed Methods Practice-Based Study of a Transdiagnostic Emotion Regulation Group Intervention" Psychiatry International 3, no. 4: 297-312. https://doi.org/10.3390/psychiatryint3040024
APA StyleMoore, R., Gillanders, D., & Stuart, S. (2022). The Emotional Resources Group: A Mixed Methods Practice-Based Study of a Transdiagnostic Emotion Regulation Group Intervention. Psychiatry International, 3(4), 297-312. https://doi.org/10.3390/psychiatryint3040024