
Pericardial Recesses Mimicking Mediastinal Adenopathy on CT

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Imaging Features
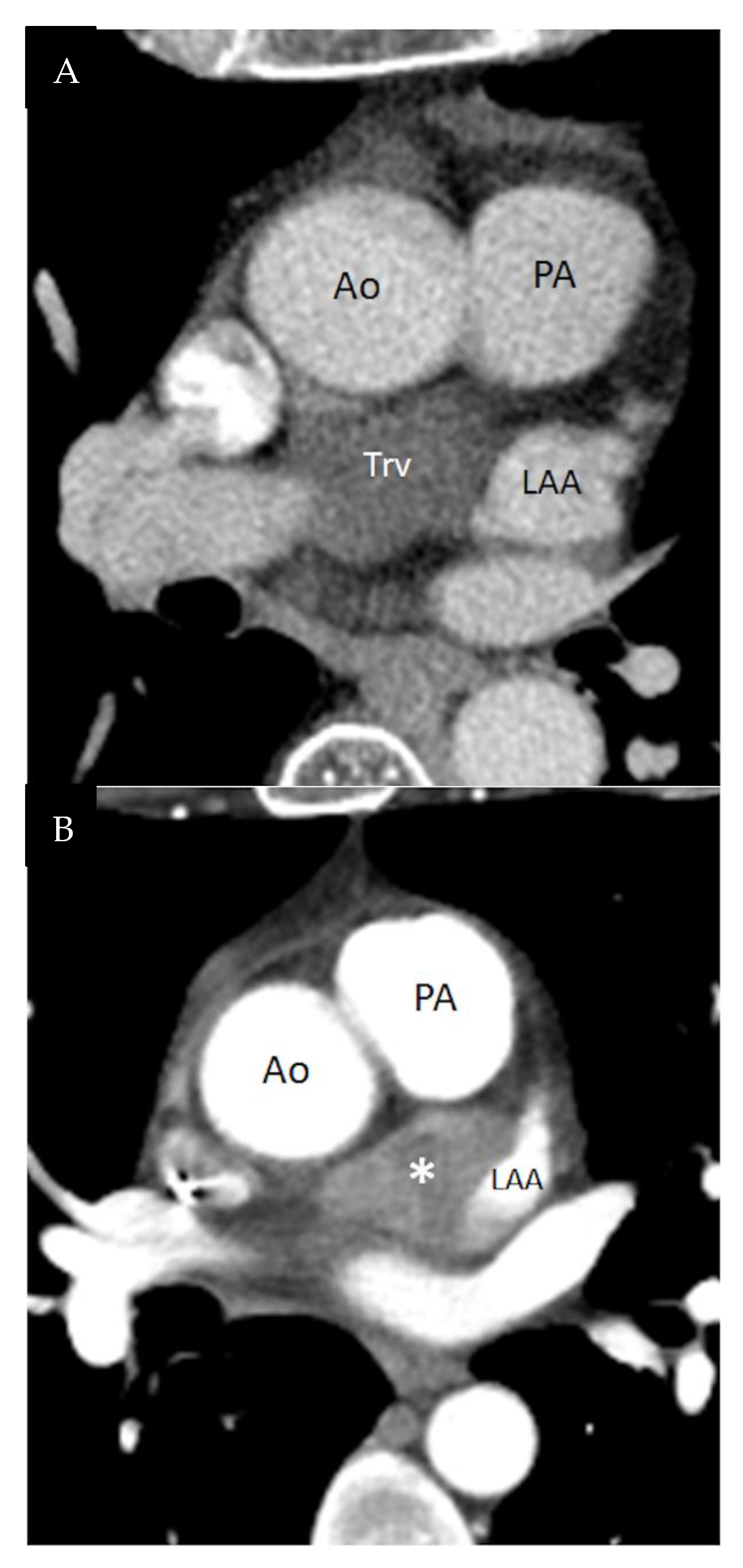
3. Transverse Sinus
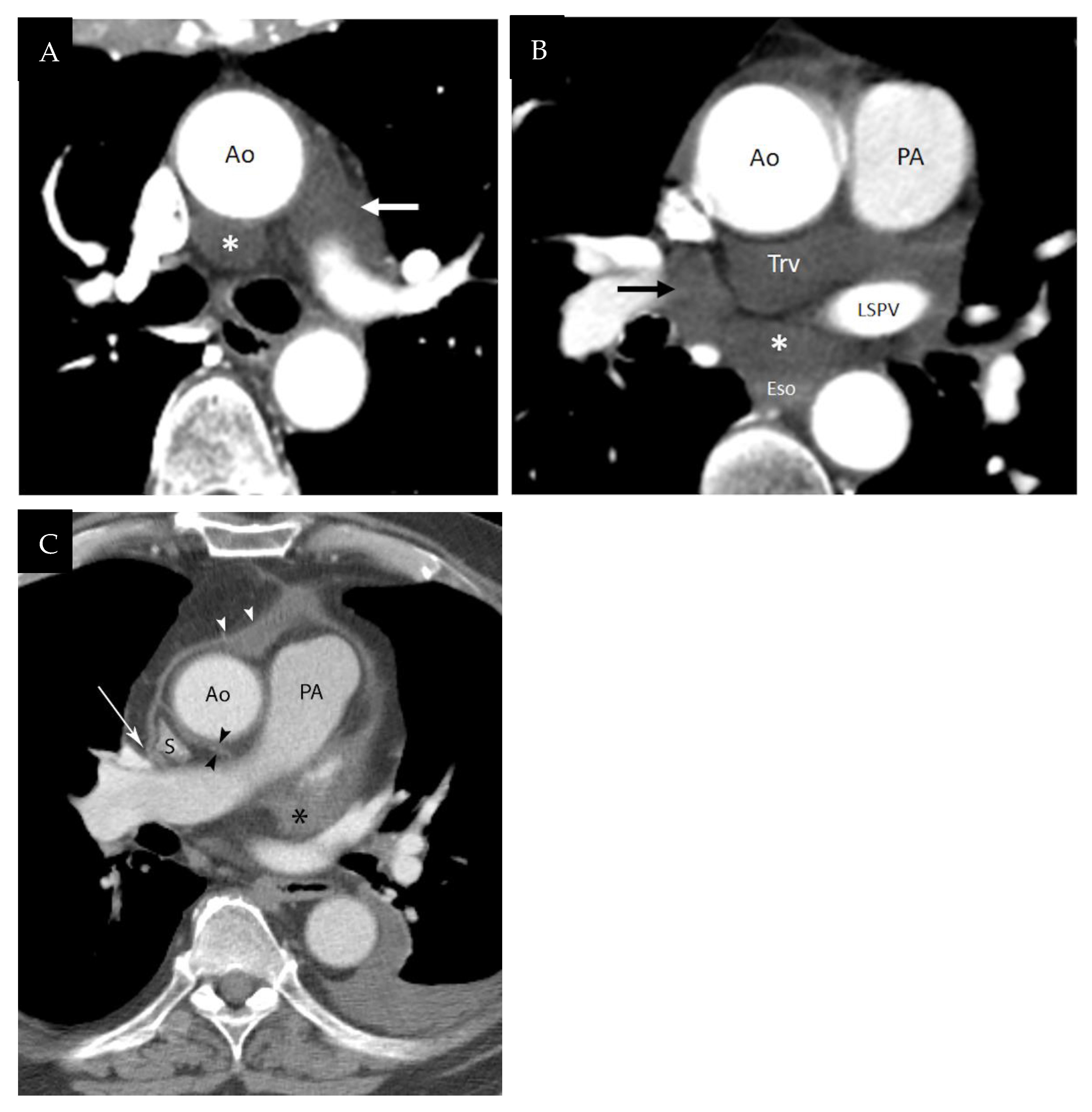
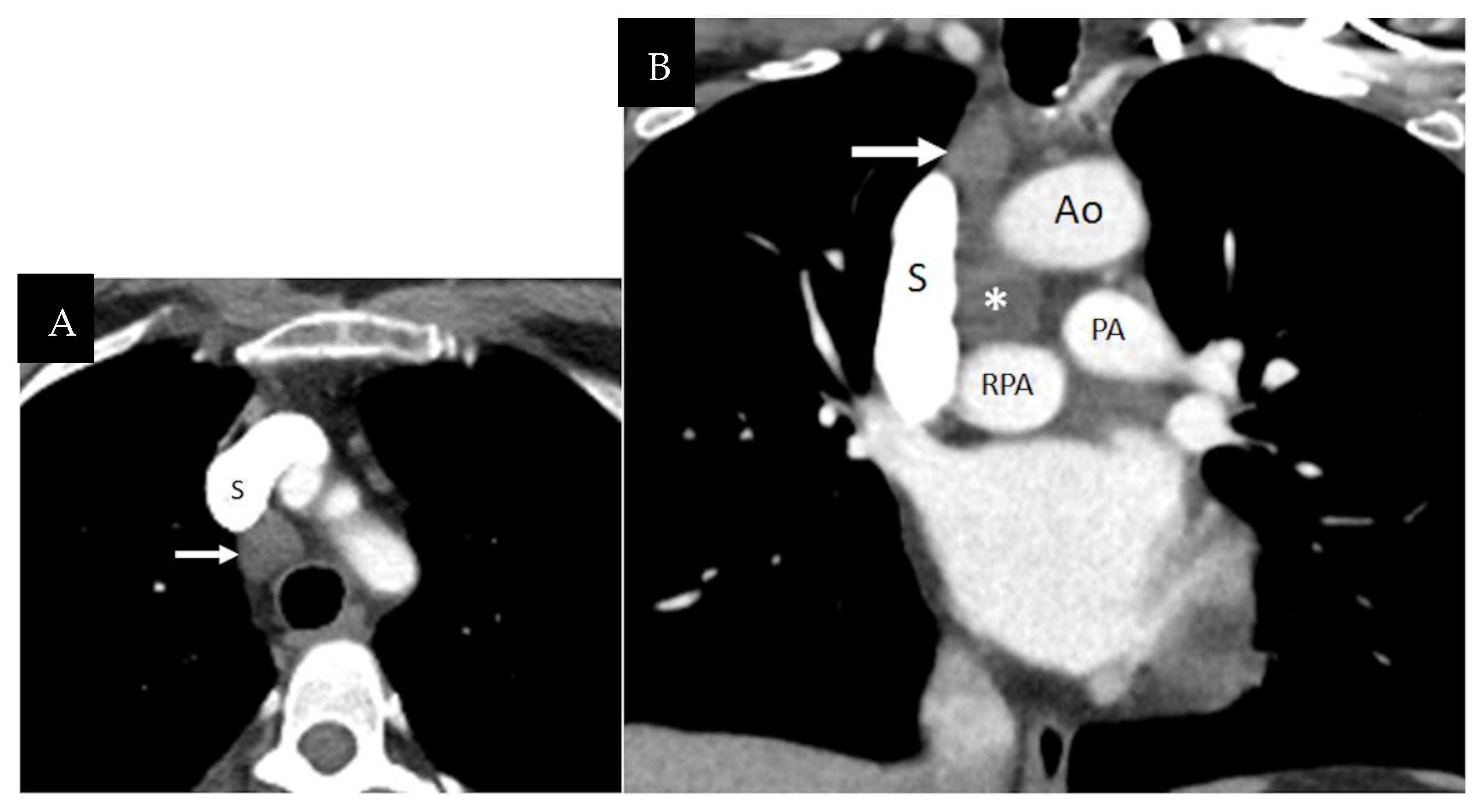
3.1. Superior Aortic Recess
3.2. Inferior Aortic Recess
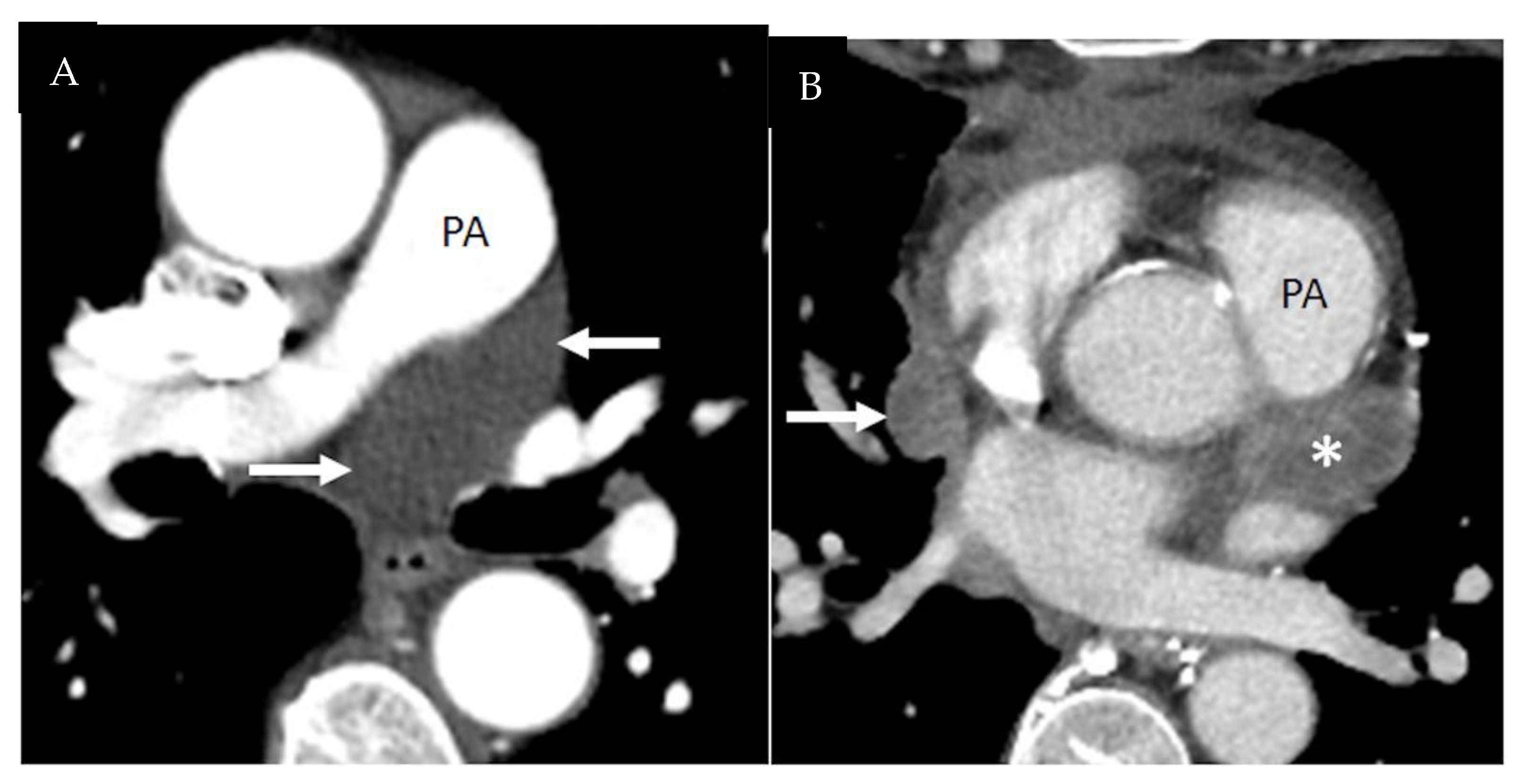
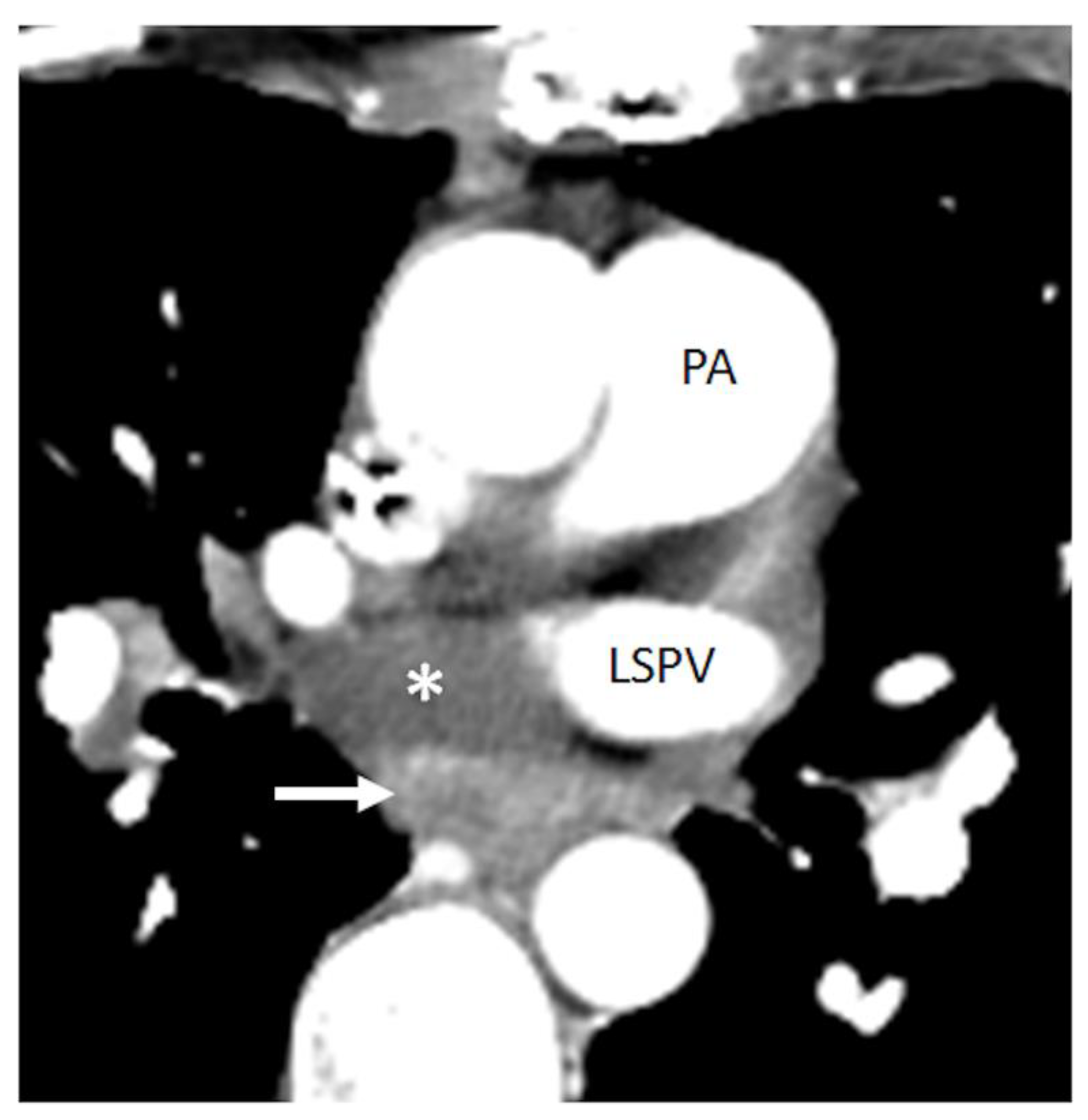
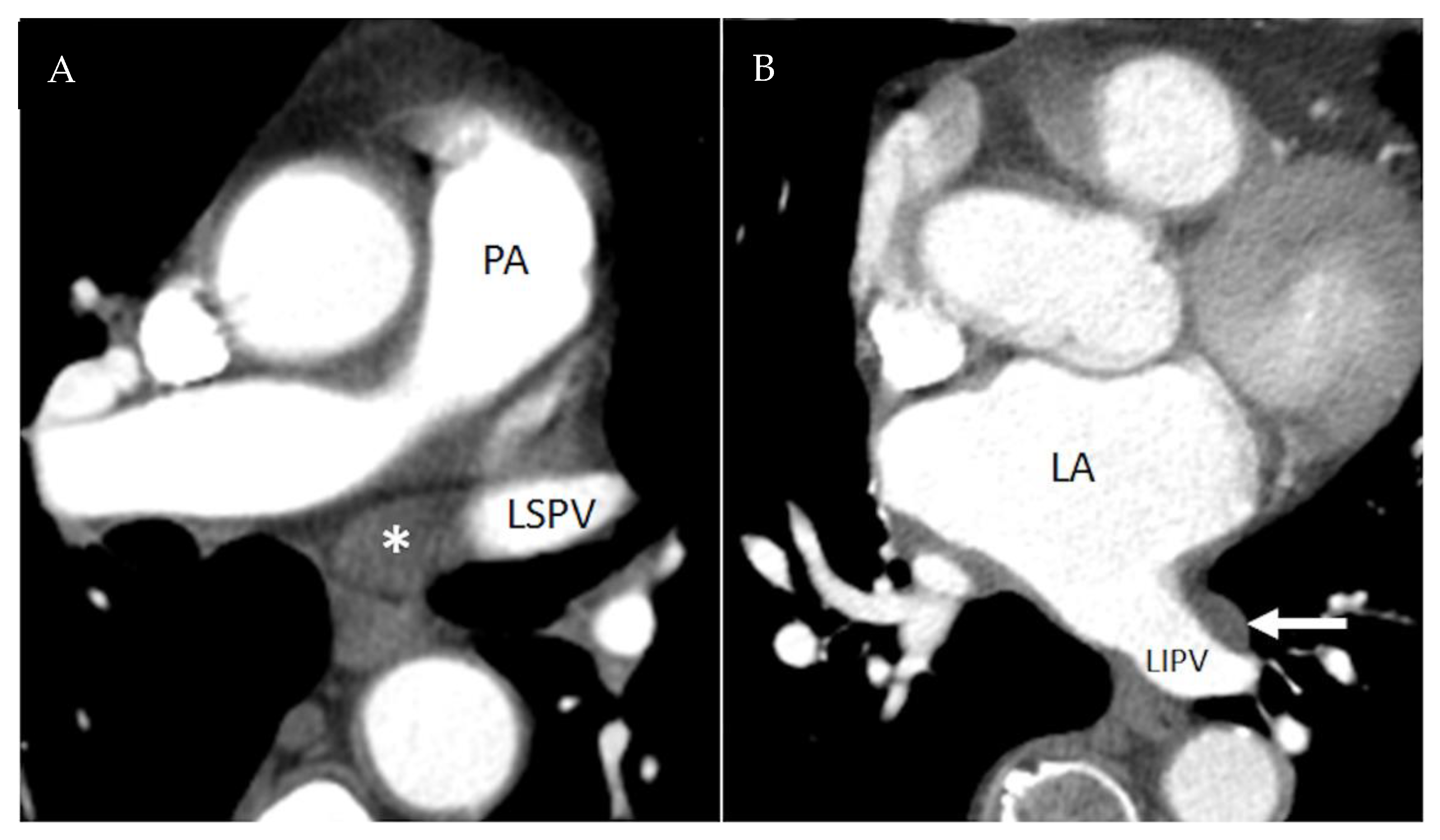
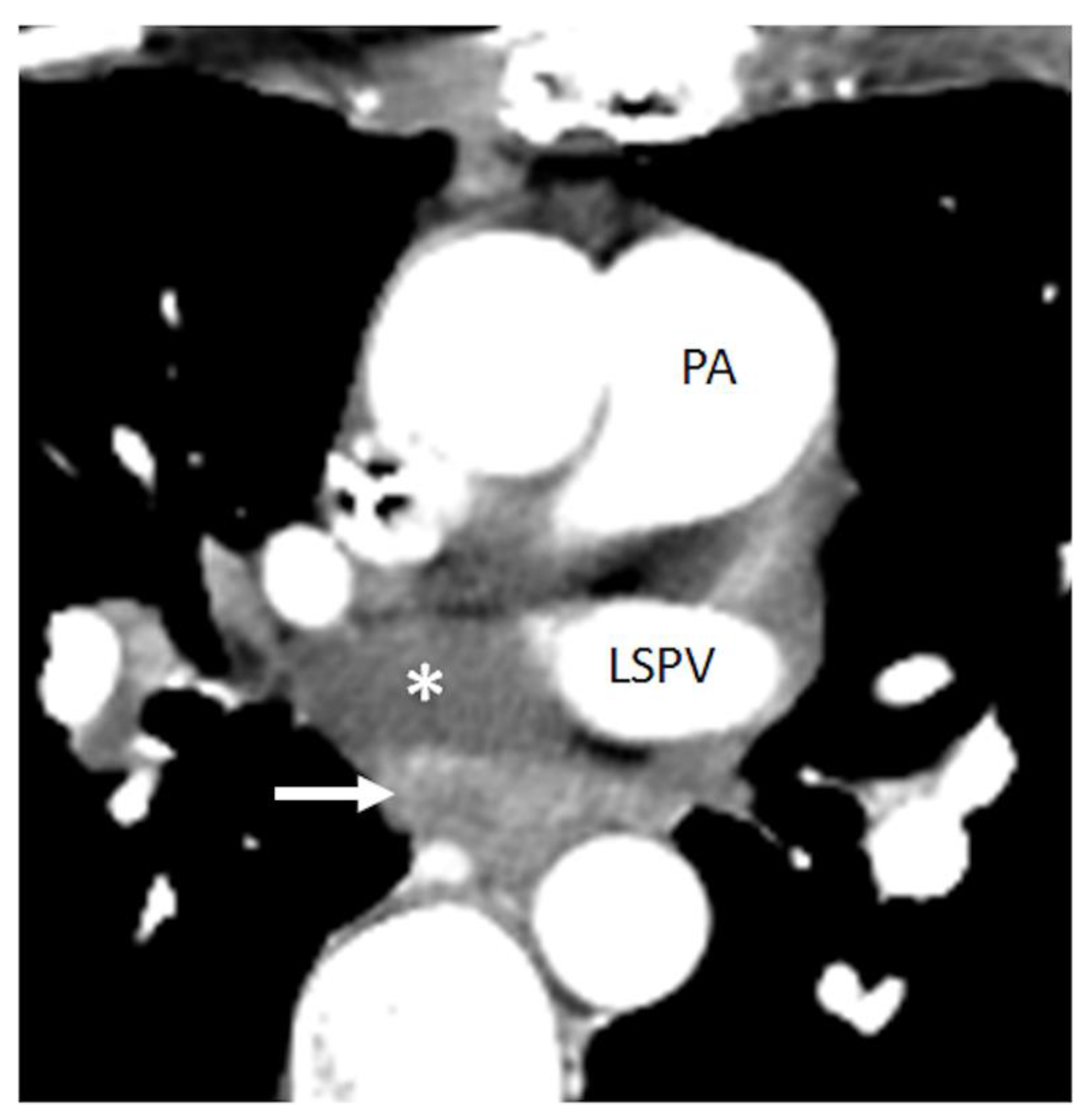
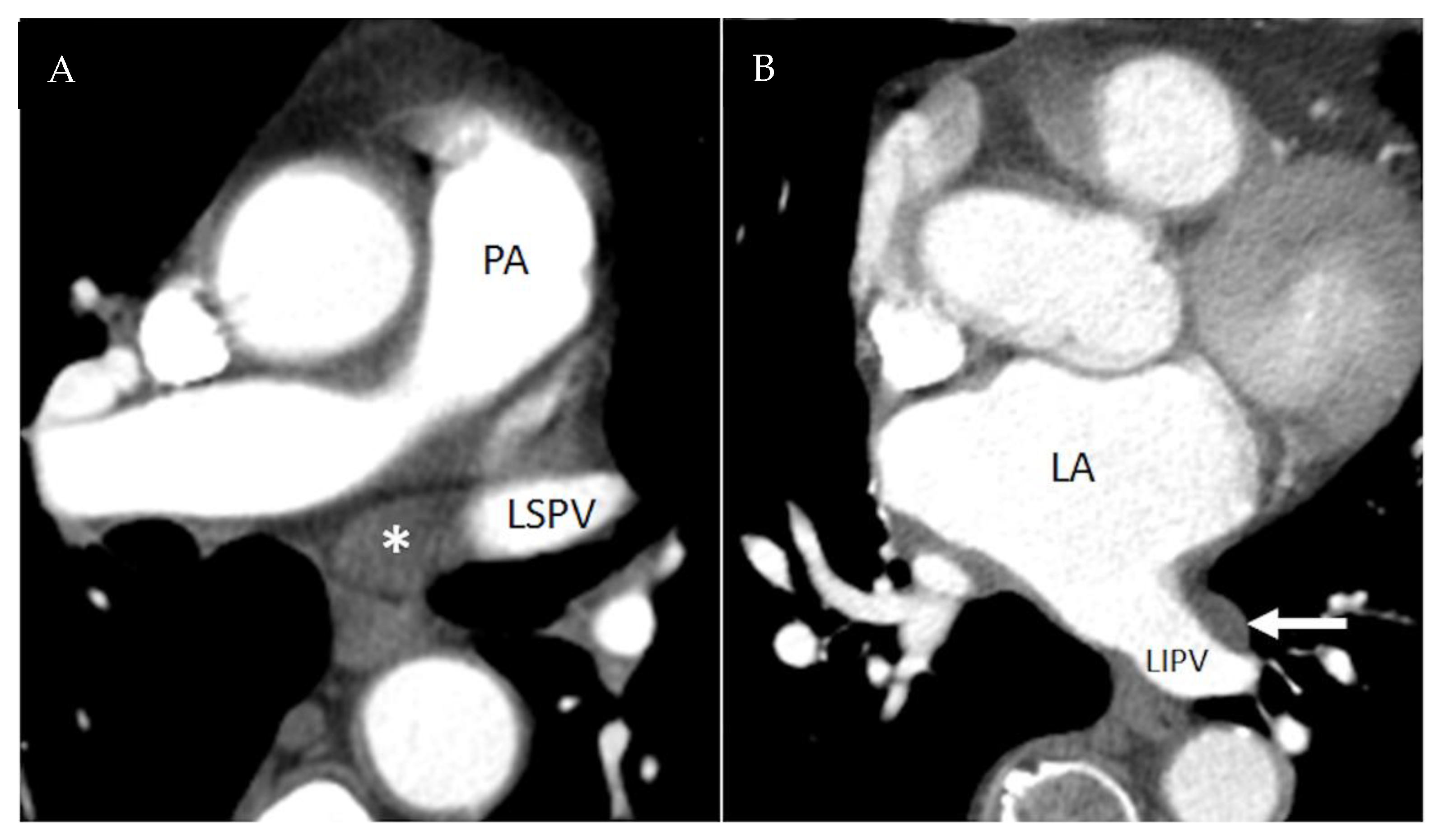
3.3. Right and Left Pulmonic Recesses
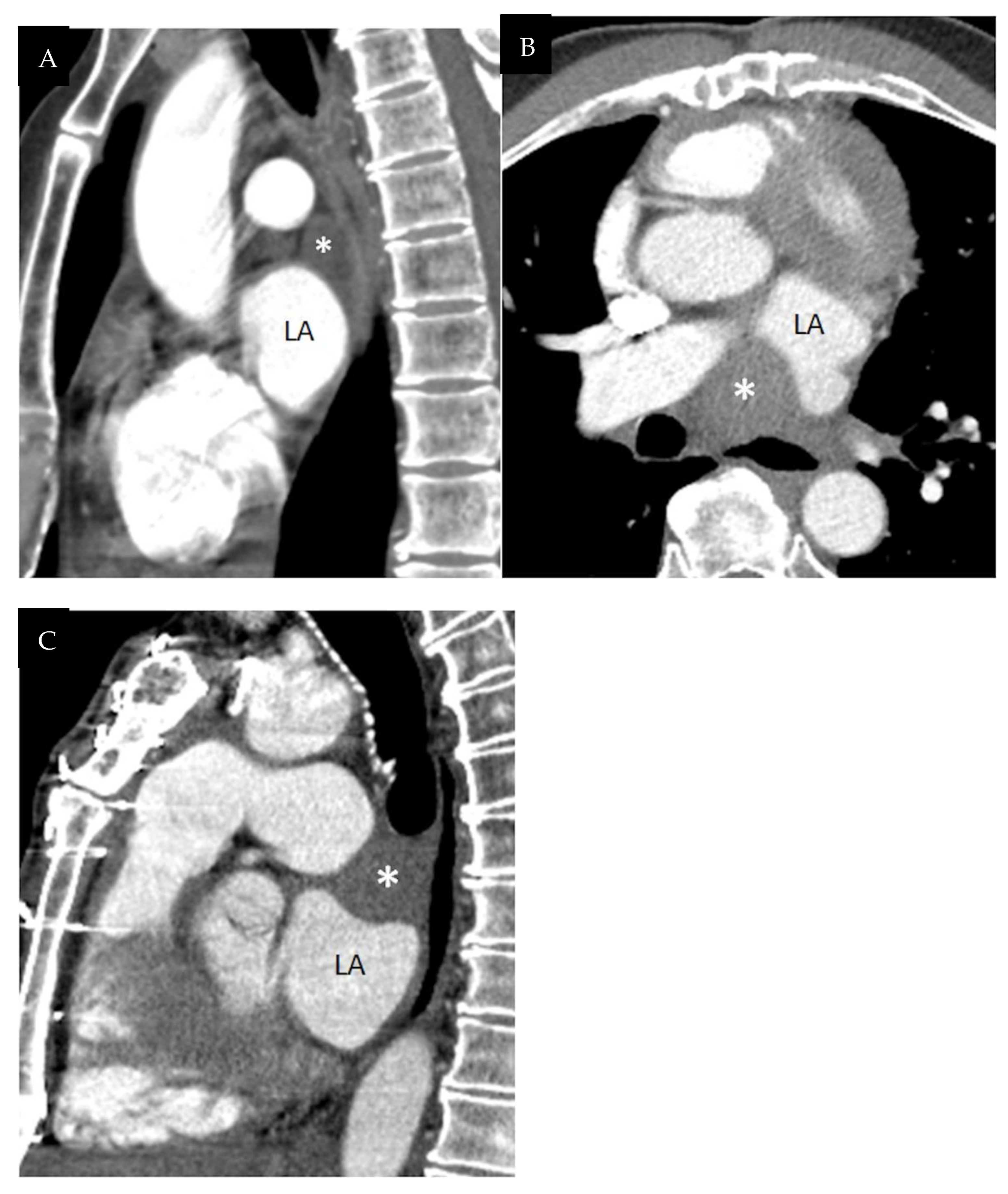
3.4. Oblique Sinus
4. Pericardial Cavity Proper
4.1. Postcaval Recess
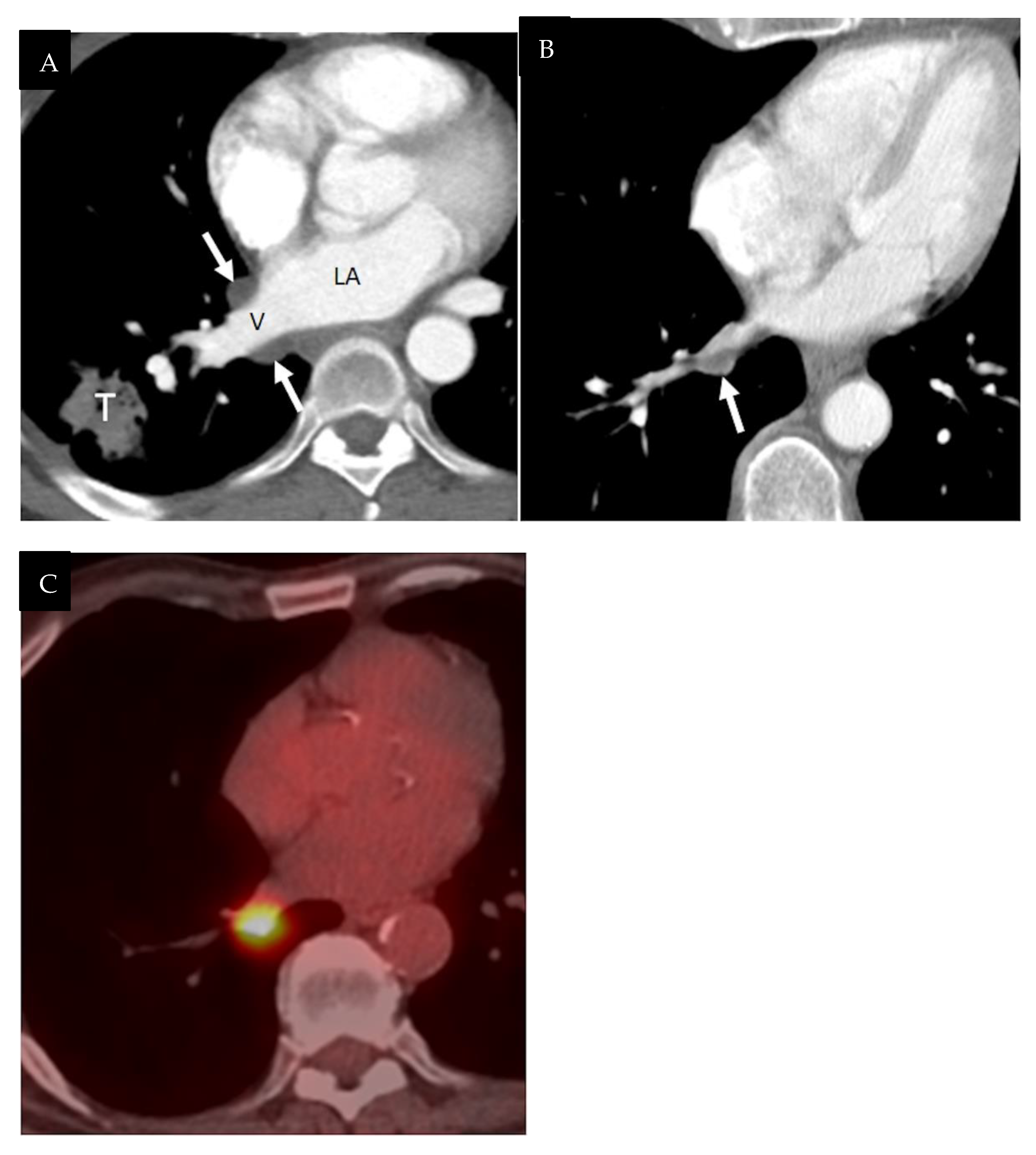
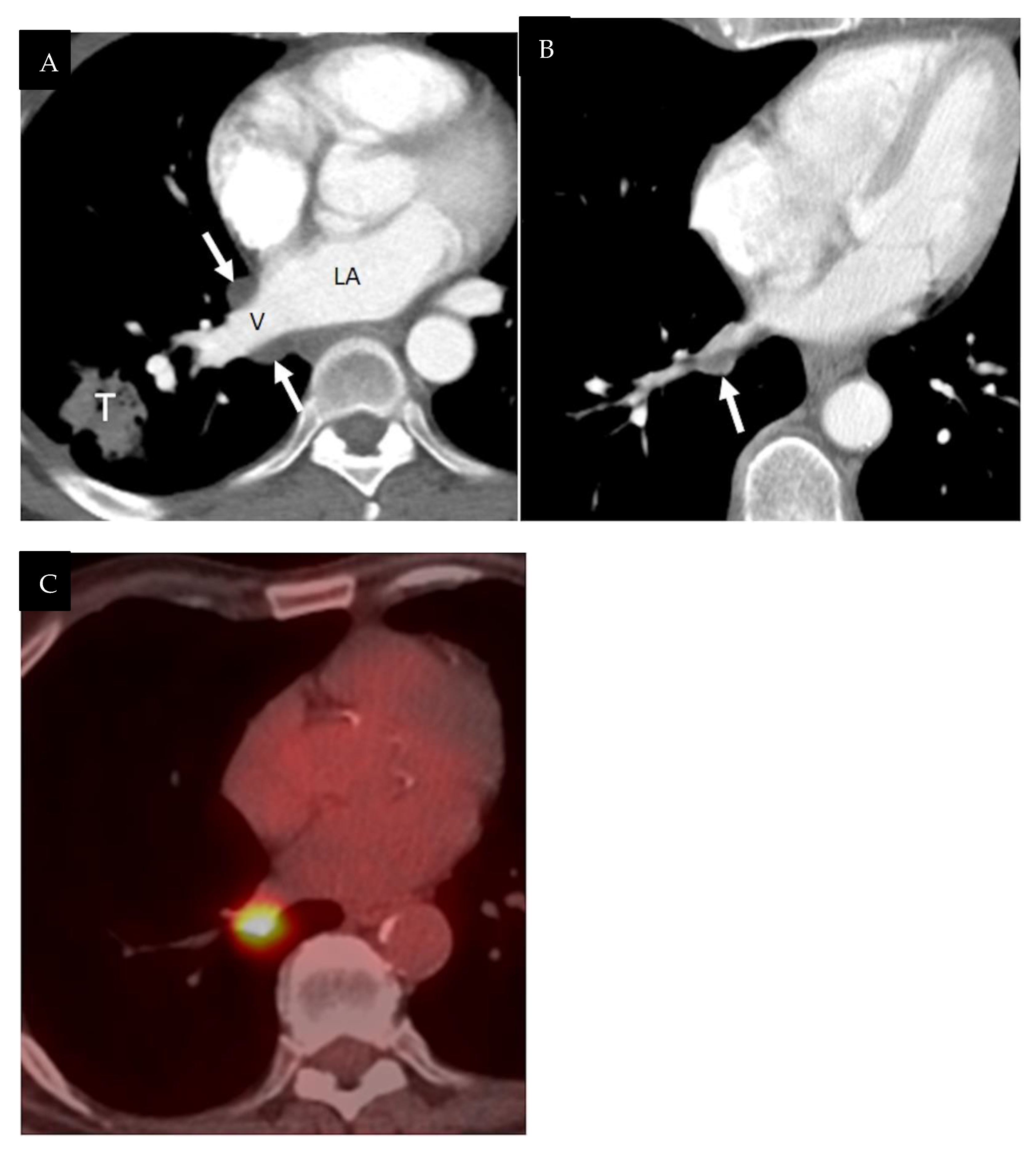
4.2. Right and Left Pulmonary Venous Recesses
5. Additional Pitfalls in Pericardial Imaging
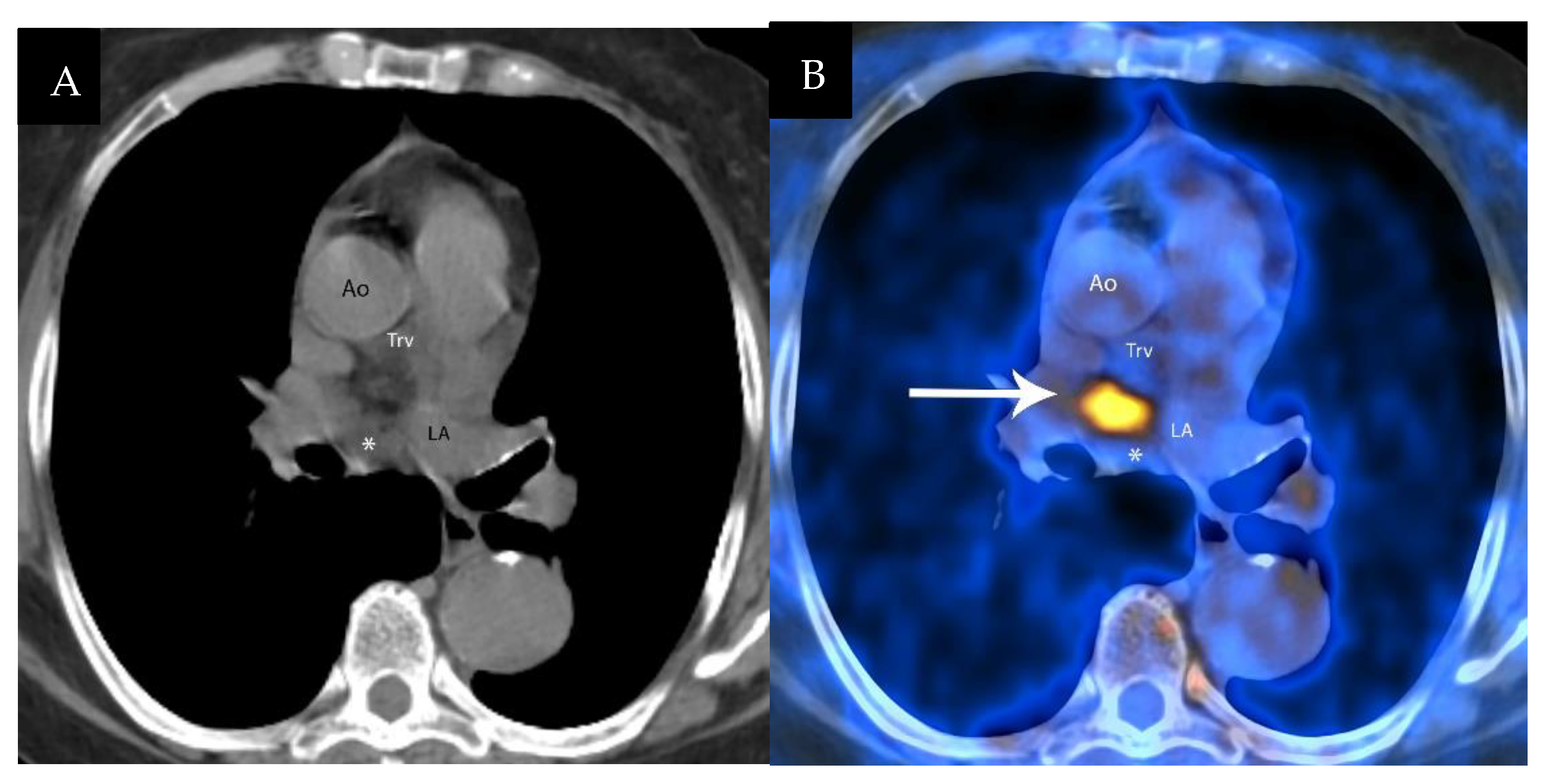
5.1. Hypermetabolic Brown Fat
5.2. Acute Pericarditis
5.3. Epipericardial Fat Necrosis
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Little, W.C.; Freeman, G.L. Pericardial disease. Circulation 2006, 113, 1622–1632. [Google Scholar] [CrossRef] [PubMed]
- Shroff, G.S.; Viswanathan, C.; Godoy, M.C.; Marom, E.M.; Sabloff, B.S.; Truong, M.T. Pitfalls in oncologic imaging: Pericardial recesses mimicking adenopathy. Semin. Roentgenol. 2015, 50, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Bogaert, J.; Francone, M. Pericardial disease: Value of CT and MR imaging. Radiology 2013, 267, 340–356. [Google Scholar] [CrossRef] [PubMed]
- Shroff, G.S.; Ahuja, J.; Strange, C.D.; Gayer, G.; Jo, N.; Archer, J.M.; Truong, M.T. Pitfalls in oncologic imaging of the pericardium on CT and PET/CT. Semin. Ultrasound CT MRI 2022. [Google Scholar] [CrossRef]
- Kodama, F.; Fultz, P.J.; Wandtke, J.C. Comparing thin-section and thick-section CT of pericardial sinuses and recesses. AJR Am. J. Roentgenol. 2003, 181, 1101–1108. [Google Scholar] [CrossRef]
- Basile, A.; Bisceglie, P.; Giulietti, G.; Calcara, G.; Figuera, M.; Mundo, E.; Granata, A.; Runza, G.; Privitera, C.; Privitera, G.; et al. Prevalence of “high-riding” superior pericardial recesses on thin-section 16-MDCT scans. Eur. J. Radiol. 2006, 59, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Axel, L. Assessment of pericardial disease by magnetic resonance and computed tomography. J. Magn. Reson. Imaging 2004, 19, 816–826. [Google Scholar] [CrossRef] [PubMed]
- Vesely, T.M.; Cahill, D.R. Cross-sectional anatomy of the pericardial sinuses, recesses, and adjacent structures. Surg. Radiol. Anat. 1986, 8, 221–227. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, S.M.; Williams, P.L.; Williams, M.P.; Edwards, A.J.; Roobottom, C.A.; Morgan-Hughes, G.J.; Manghat, N.E. Imaging the pericardium: Appearances on ECG-gated 64-detector row cardiac computed tomography. Br. J. Radiol. 2010, 83, 194–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, Y.W.; McAdams, H.P.; Jeon, S.C.; Seo, H.S.; Hahm, C.K. The “High-Riding” superior pericardial recess: CT findings. AJR Am. J. Roentgenol. 2000, 175, 1025–1028. [Google Scholar] [CrossRef] [PubMed]
- Broderick, L.S.; Brooks, G.N.; Kuhlman, J.E. Anatomic pitfalls of the heart and pericardium. Radiographics 2005, 25, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Groell, R.; Schaffler, G.J.; Rienmueller, R. Pericardial sinuses and recesses: Findings at electrocardiographically triggered electron-beam CT. Radiology 1999, 212, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Truong, M.T.; Erasmus, J.J.; Gladish, G.W.; Sabloff, B.S.; Marom, E.M.; Madewell, J.E.; Chasen, M.H.; Munden, R.F. Anatomy of pericardial recesses on multidetector CT: Implications for oncologic imaging. AJR Am. J. Roentgenol. 2003, 181, 1109–1113. [Google Scholar] [CrossRef] [PubMed]
- Truong, M.T.; Erasmus, J.J.; Sabloff, B.S.; Marom, E.M.; Gladish, G.W.; Chasen, M.H.; Munden, R.F. Pericardial “sleeve” recess of right inferior pulmonary vein mimicking adenopathy: Computed tomography findings. J. Comput. Assist. Tomogr. 2004, 28, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, J.D.; Vogel, W.; Vegt, E. Factors influencing brown fat activation in FDG PET/CT: A retrospective analysis of 15,000+ cases. Br. J. Radiol. 2017, 90, 20170093. [Google Scholar] [CrossRef] [PubMed]
- Fan, C.M.; Fischman, A.J.; Kwek, B.H.; Abbara, S.; Aquino, S.L. Lipomatous hypertrophy of the interatrial septum: Increased uptake on FDG PET. AJR Am. J. Roentgenol. 2005, 184, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Kligerman, S. Imaging of Pericardial Disease. Radiol. Clin. N. Am. 2019, 57, 179–199. [Google Scholar] [CrossRef] [PubMed]
- Hyeon, C.W.; Yi, H.K.; Kim, E.K.; Park, S.J.; Lee, S.C.; Park, S.W.; Oh, J.K.; Choi, J.Y.; Chang, S.A. The role of (18)F-fluorodeoxyglucose-positron emission tomography/computed tomography in the differential diagnosis of pericardial disease. Sci. Rep. 2020, 10, 21524. [Google Scholar] [CrossRef] [PubMed]
- Fred, H.L. Pericardial fat necrosis: A review and update. Tex. Heart Inst. J. 2010, 37, 82–84. [Google Scholar] [PubMed]
- Kashyap, R.; Lau, E.; George, A.; Seymour, J.F.; Lade, S.; Hicks, R.J.; Hofman, M.S. High FDG activity in focal fat necrosis: A pitfall in interpretation of posttreatment PET/CT in patients with non-Hodgkin lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 1330–1336. [Google Scholar] [CrossRef] [PubMed]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Archer, J.M.; Ahuja, J.; Strange, C.D.; Shroff, G.S.; Unlu, E.; Truong, M.T. Pericardial Recesses Mimicking Mediastinal Adenopathy on CT. J. Respir. 2022, 2, 87-100. https://doi.org/10.3390/jor2020007
Archer JM, Ahuja J, Strange CD, Shroff GS, Unlu E, Truong MT. Pericardial Recesses Mimicking Mediastinal Adenopathy on CT. Journal of Respiration. 2022; 2(2):87-100. https://doi.org/10.3390/jor2020007
Chicago/Turabian StyleArcher, John Matthew, Jitesh Ahuja, Chad D. Strange, Girish S. Shroff, Ebru Unlu, and Mylene T. Truong. 2022. "Pericardial Recesses Mimicking Mediastinal Adenopathy on CT" Journal of Respiration 2, no. 2: 87-100. https://doi.org/10.3390/jor2020007
APA StyleArcher, J. M., Ahuja, J., Strange, C. D., Shroff, G. S., Unlu, E., & Truong, M. T. (2022). Pericardial Recesses Mimicking Mediastinal Adenopathy on CT. Journal of Respiration, 2(2), 87-100. https://doi.org/10.3390/jor2020007