
Progression of Well-Differentiated Papillary Mesothelial Tumour to Mesothelioma in a Patient with Ehlers Danlos Syndrome



{kind=link}
{kind=link}
Abstract
:1. Introduction
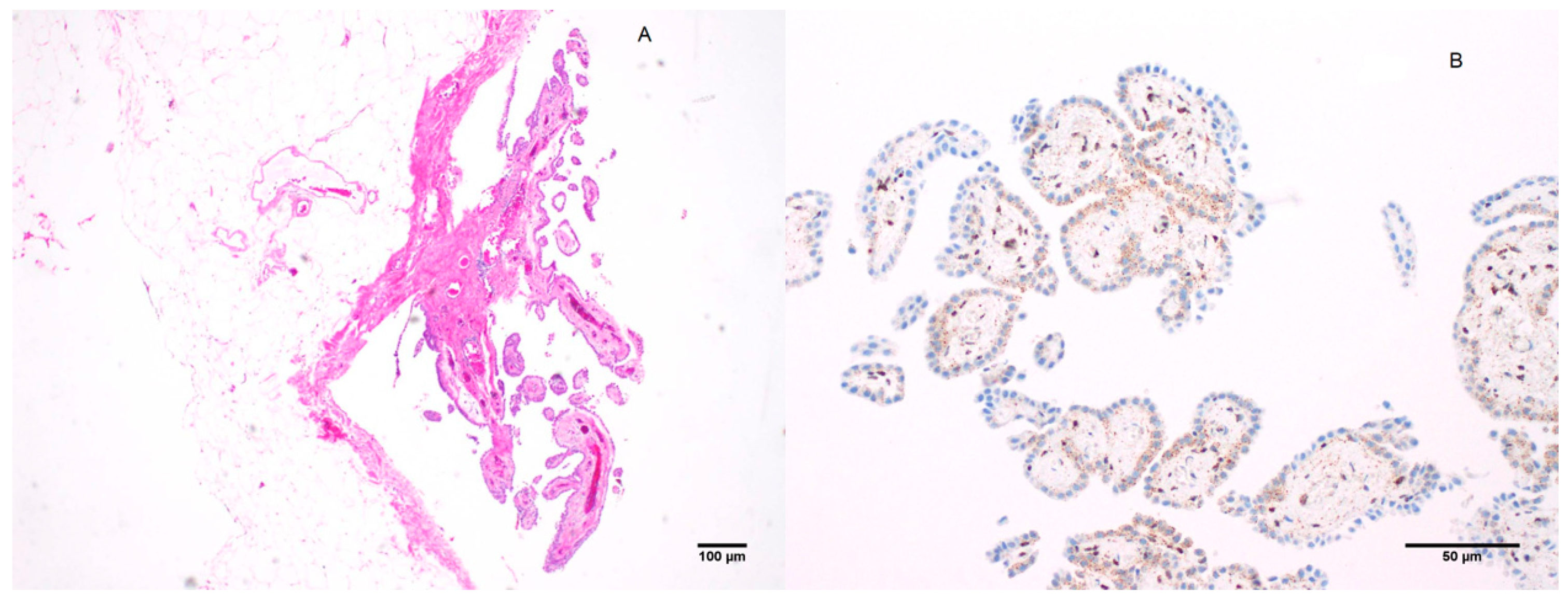
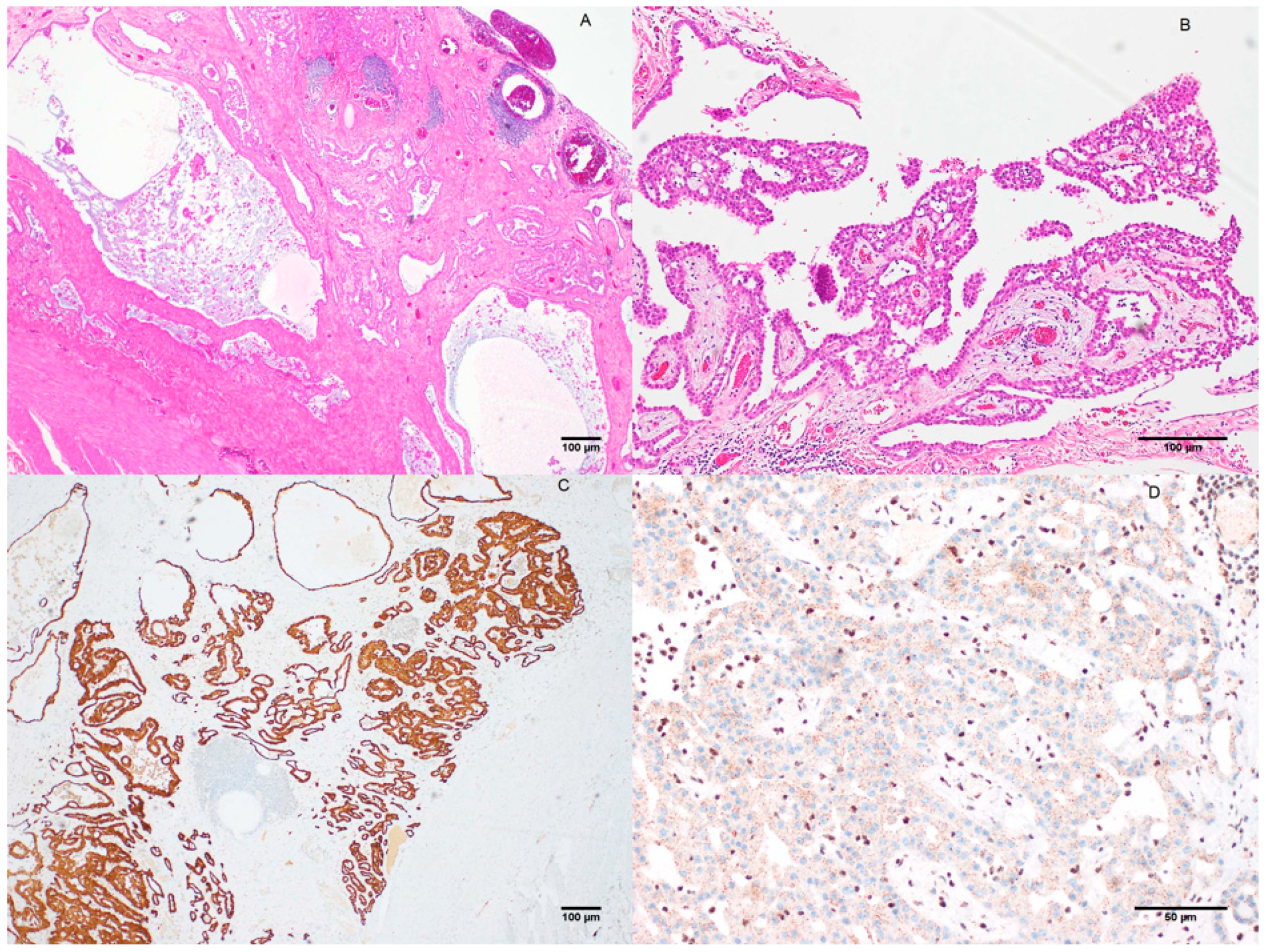
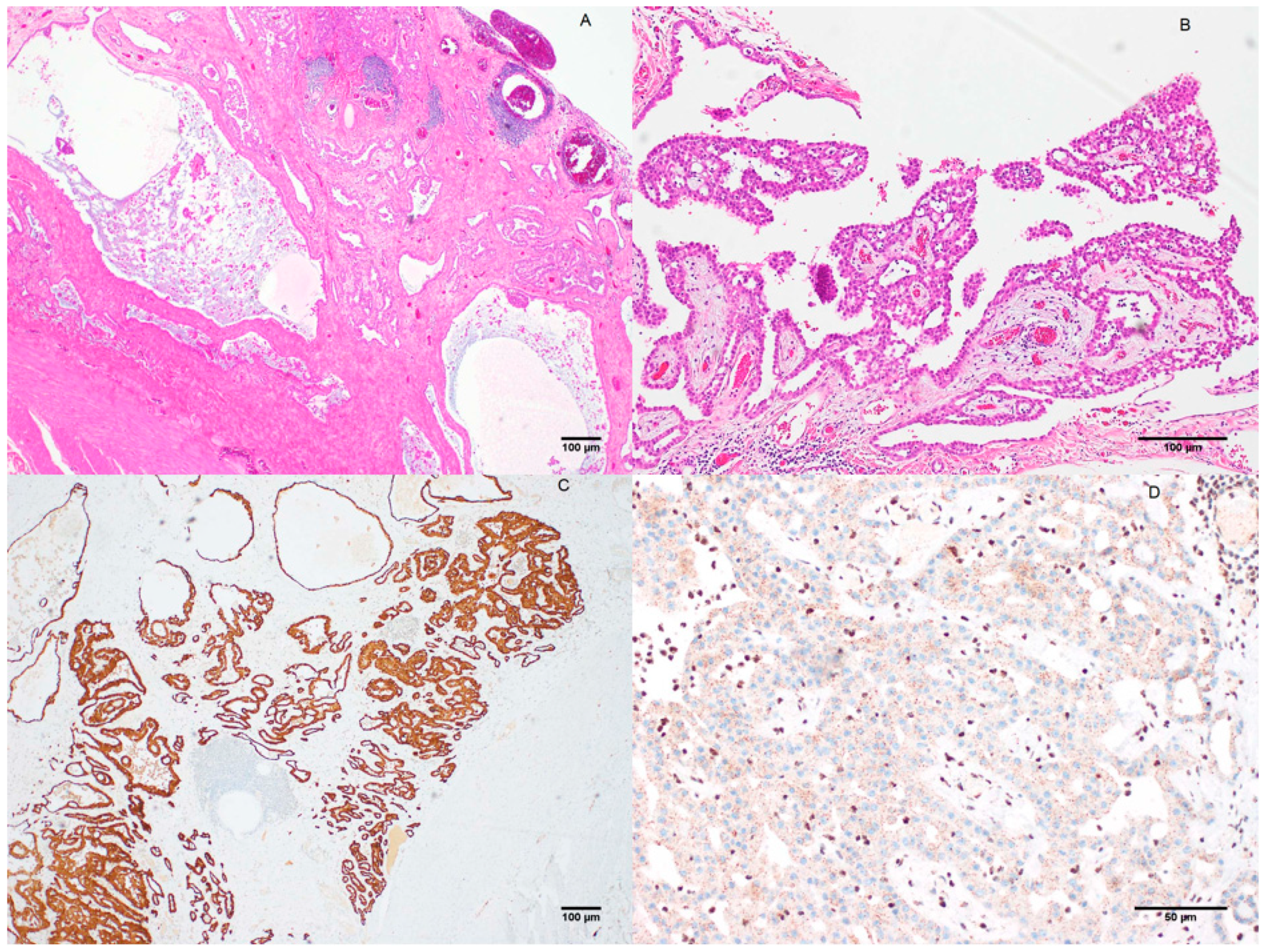
2. Case Presentation
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Malpica, A.; Sant’Ambrogio, S.; Deavers, M.T.; Silva, E.G. Well-differentiated papillary mesothelioma of the female peritoneum: A clinicopathologic study of 26 cases. Am. J. Surg. Pathol. 2012, 36, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Daya, D.; Elliott McCaughey, W. Well-differentiated papillary mesothelioma of the peritoneum. A clinicopathologic study of 22 cases. Cancer 1990, 65, 292–296. [Google Scholar] [CrossRef]
- Sun, M.; Zhao, L.; Lao, I.W.; Yu, L.; Wang, J. Well-differentiated papillary mesothelioma: A 17-year single institution experience with a series of 75 cases. Ann. Diagn. Pathol. 2019, 38, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Bürrig, K.-F.; Pfitzer, P.; Hort, W. Well-differentiated papillary mesothelioma of the peritoneum: A borderline mesothelioma. Virchows Arch. A 1990, 417, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Kim, H.-S. Clinicopathological characteristics of well-differentiated papillary mesothelioma of the peritoneum: A single-institutional experience of 12 cases. In Vivo 2019, 33, 633–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization Classification of Tumours. Pathology & Genetics. Tumours of the Lung, Pleura, Thymus and Heart; Travis, W.D., Brambilla, E., Müller-Hermelink, H.K., Harris, C.C., Eds.; IARC Press: Lyon, France, 2004; pp. 135–136. [Google Scholar]
- Butnor, K.J.; Sporn, T.A.; Hammar, S.P.; Roggli, V.L. Well-differentiated papillary mesothelioma. Am. J. Surg. Pathol. 2001, 25, 1304–1309. [Google Scholar] [CrossRef] [PubMed]
- Galateau-Sallé, F.; Vignaud, J.M.; Burke, L.; Gibbs, A.; Brambilla, E.; Attanoos, R.; Goldberg, M.; Launoy, G. Well-differentiated papillary mesothelioma of the pleura: A series of 24 cases. Am. J. Surg. Pathol. 2004, 28, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Churg, A.; Allen, T.; Borczuk, A.C.; Cagle, P.T.; Galateau-Sallé, F.; Hwang, H.; Murer, B.; Murty, V.V.; Ordonez, N.; Tazelaar, H.D. Well-differentiated papillary mesothelioma with invasive foci. Am. J. Surg. Pathol. 2014, 38, 990–998. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Thoracic Tumours, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2021; Volume 5. [Google Scholar]
- Hoekman, K.; Tognon, G.; Risse, E.; Bloemsma, C.; Vermorken, J. Well-differentiated papillary mesothelioma of the peritoneum: A separate entity. Eur. J. Cancer 1996, 32, 255–258. [Google Scholar] [CrossRef]
- Jones, M.A.; Young, R.H.; Scully, R.E. Malignant mesothelioma of the tunica vaginalis. A clinicopathologic analysis of 11 cases with review of the literature. Am. J. Surg. Pathol. 1995, 19, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, C.; Campelos, S.; Moura, C.; Machado, J.; Justino, A.; Parente, B. Well-differentiated papillary mesothelioma: Clustering in a Portuguese family with a germline BAP1 mutation. Ann. Oncol. 2013, 24, 2147–2150. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.E.; Molina, J.R.; Sukov, W.R.; Roden, A.C.; Eunhee, S.Y. BAP1 loss is unusual in well-differentiated papillary mesothelioma and may predict development of malignant mesothelioma. Hum. Pathol. 2018, 79, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Churg, A.; Galateau-Salle, F.; Roden, A.C.; Attanoos, R.; von der Thusen, J.H.; Tsao, M.S.; Chang, N.; De Perrot, M.; Dacic, S. Malignant mesothelioma in situ: Morphologic features and clinical outcome. Mod. Pathol. 2020, 33, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Dacic, S.; Roy, S.; Lyons, M.A.; von der Thusen, J.H.; Galateau-Salle, F.; Churg, A. Whole exome sequencing reveals BAP1 somatic abnormalities in mesothelioma in situ. Lung Cancer 2020, 149, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Pulford, E.; Henderson, D.W.; Klebe, S. Malignant mesothelioma in situ: Diagnostic and clinical considerations. Pathology 2020, 52, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Zauderer, M.G.; Bott, M.; McMillan, R.; Sima, C.S.; Rusch, V.; Krug, L.M.; Ladanyi, M. Clinical characteristics of patients with malignant pleural mesothelioma harboring somatic BAP1 mutations. J. Thorac. Oncol. 2013, 8, 1430–1433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bisconti, M.; Bisetti, A.; Bidoli, P. Malignant mesothelioma in subjects with Marfan’s syndrome and Ehlers-Danlos syndrome: Only an apparent association? Respiration 2000, 67, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Fikree, A.; Chelimsky, G.; Collins, H.; Kovacic, K.; Aziz, Q. Gastrointestinal involvement in the Ehlers–Danlos syndromes. Am. J. Med. Genet. Part C Semin. Med. Genet. 2017, 175C, 181–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrestha, R.; Nabavi, N.; Volik, S.; Anderson, S.; Haegert, A.; McConeghy, B.; Sar, F.; Brahmbhatt, S.; Bell, R.; Le Bihan, S. Well-Differentiated Papillary Mesothelioma of the Peritoneum is Genetically Distinct from Malignant Mesothelioma. Cancers 2020, 12, 1568. [Google Scholar] [CrossRef] [PubMed]
- Stevers, M.; Rabban, J.T.; Garg, K.; Van Ziffle, J.; Onodera, C.; Grenert, J.P.; Yeh, I.; Bastian, B.C.; Zaloudek, C.; Solomon, D.A. Well-differentiated papillary mesothelioma of the peritoneum is genetically defined by mutually exclusive mutations in TRAF7 and CDC42. Mod. Pathol. 2019, 32, 88–99. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prabhakaran, S.; Hussey, M.; O’Byrne, K.J.; Klebe, S. Progression of Well-Differentiated Papillary Mesothelial Tumour to Mesothelioma in a Patient with Ehlers Danlos Syndrome. J. Mol. Pathol. 2021, 2, 306-311. https://doi.org/10.3390/jmp2040026
Prabhakaran S, Hussey M, O’Byrne KJ, Klebe S. Progression of Well-Differentiated Papillary Mesothelial Tumour to Mesothelioma in a Patient with Ehlers Danlos Syndrome. Journal of Molecular Pathology. 2021; 2(4):306-311. https://doi.org/10.3390/jmp2040026
Chicago/Turabian StylePrabhakaran, Sarita, Matthew Hussey, Kenneth J. O’Byrne, and Sonja Klebe. 2021. "Progression of Well-Differentiated Papillary Mesothelial Tumour to Mesothelioma in a Patient with Ehlers Danlos Syndrome" Journal of Molecular Pathology 2, no. 4: 306-311. https://doi.org/10.3390/jmp2040026
APA StylePrabhakaran, S., Hussey, M., O’Byrne, K. J., & Klebe, S. (2021). Progression of Well-Differentiated Papillary Mesothelial Tumour to Mesothelioma in a Patient with Ehlers Danlos Syndrome. Journal of Molecular Pathology, 2(4), 306-311. https://doi.org/10.3390/jmp2040026