
Bimodal Active Shape Models for Cervical Vertebrae and Spinal Canal Boundary Extraction †


 and
and 
Abstract
:1. Introduction
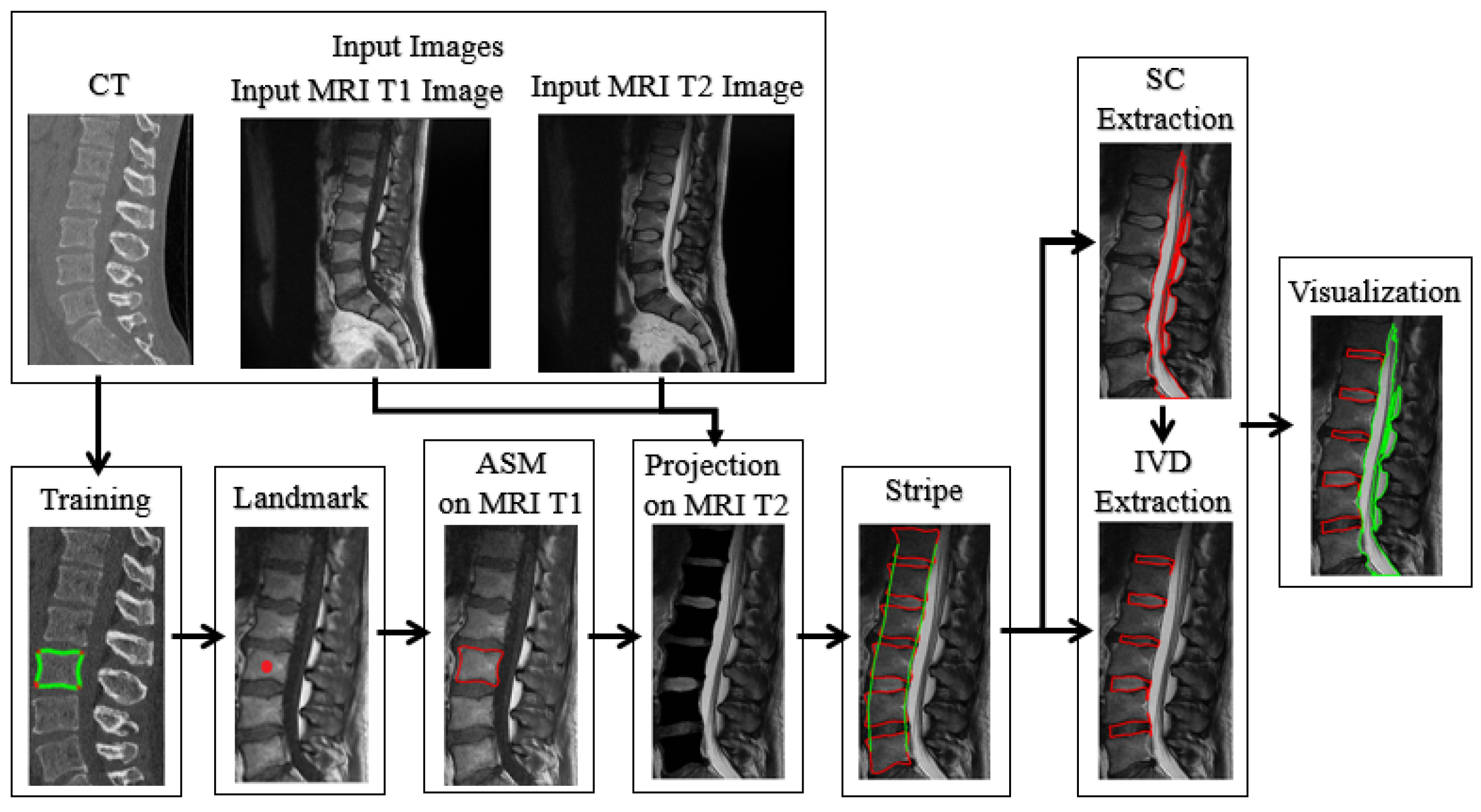
2. Material and Methods
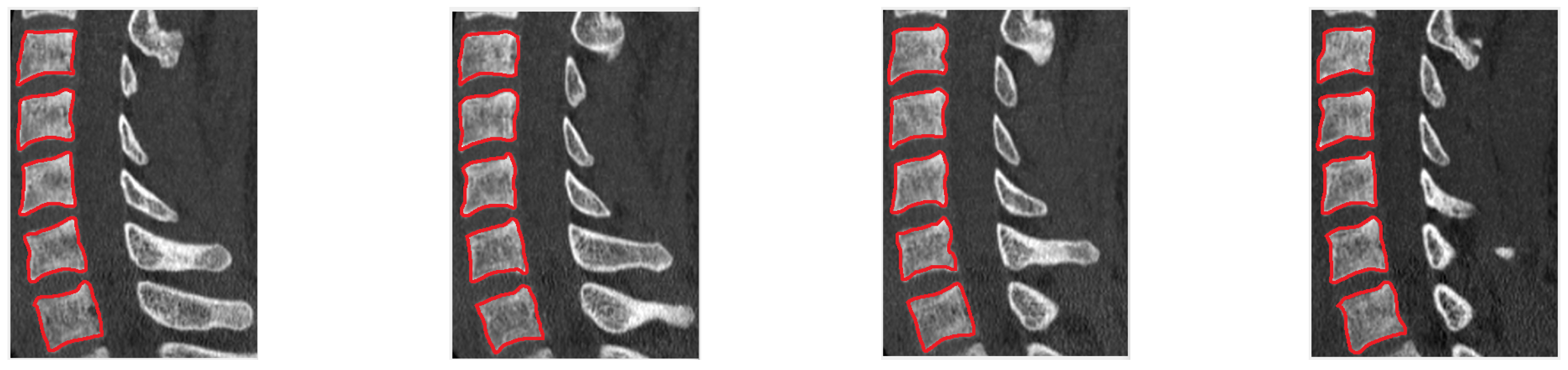
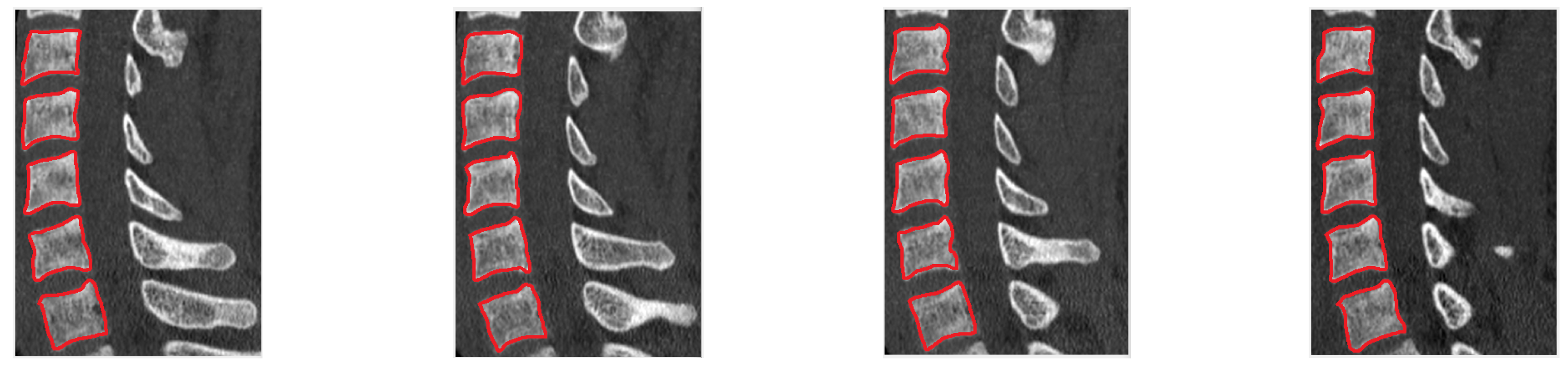
2.1. ASM Training on CT Sagittal Cervical Images
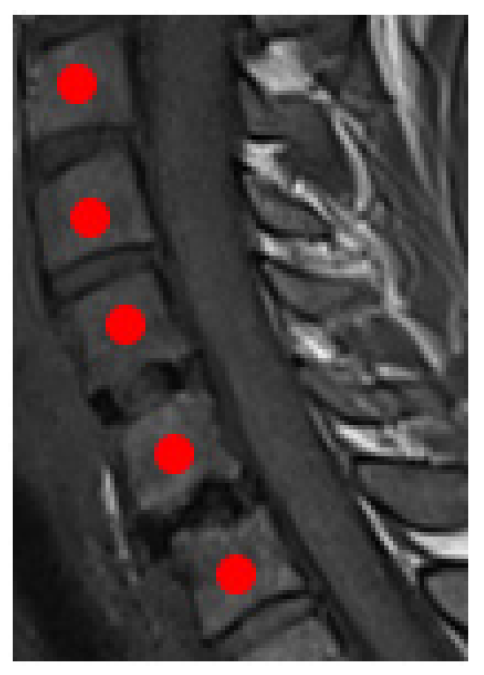
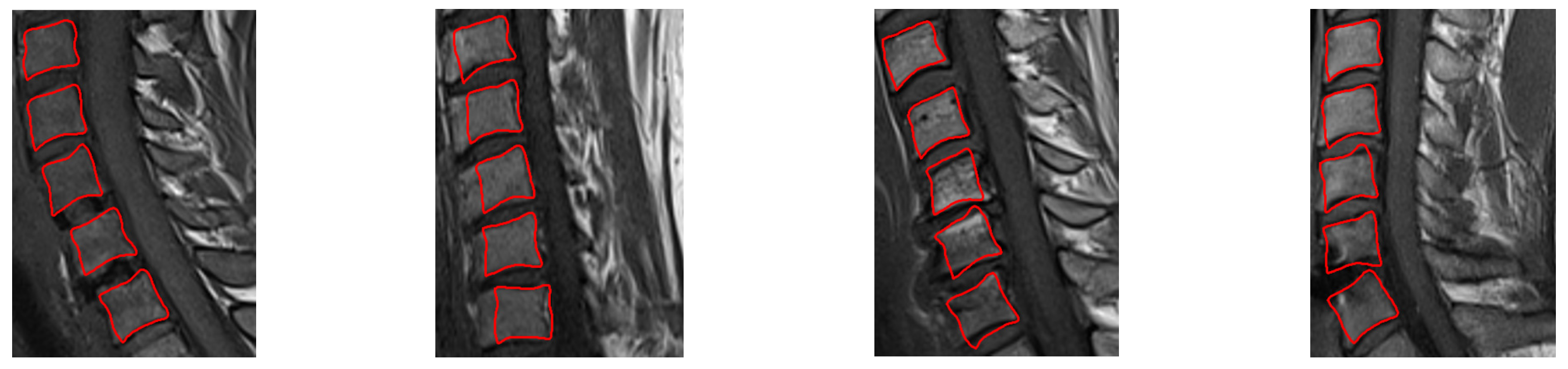
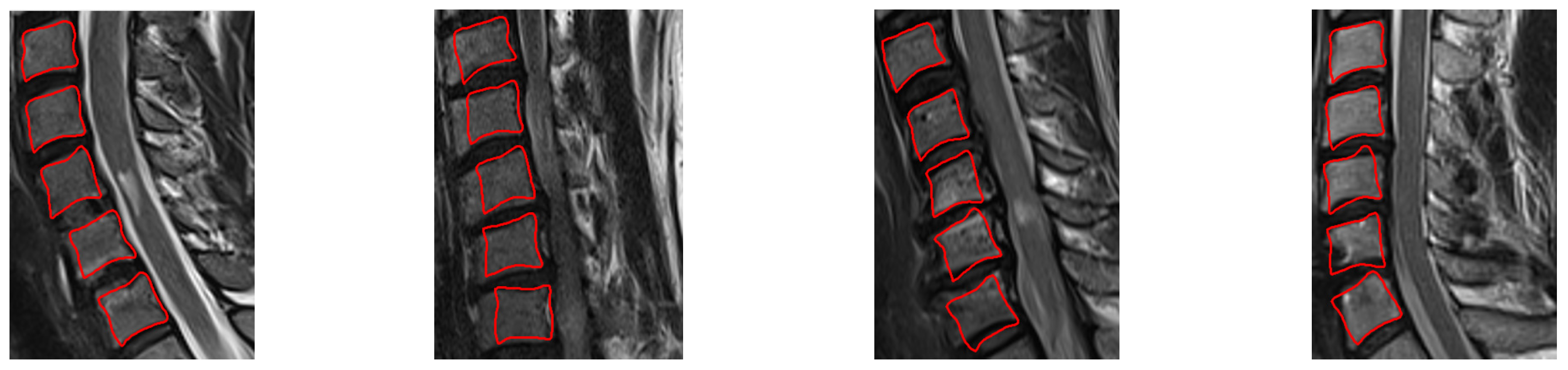
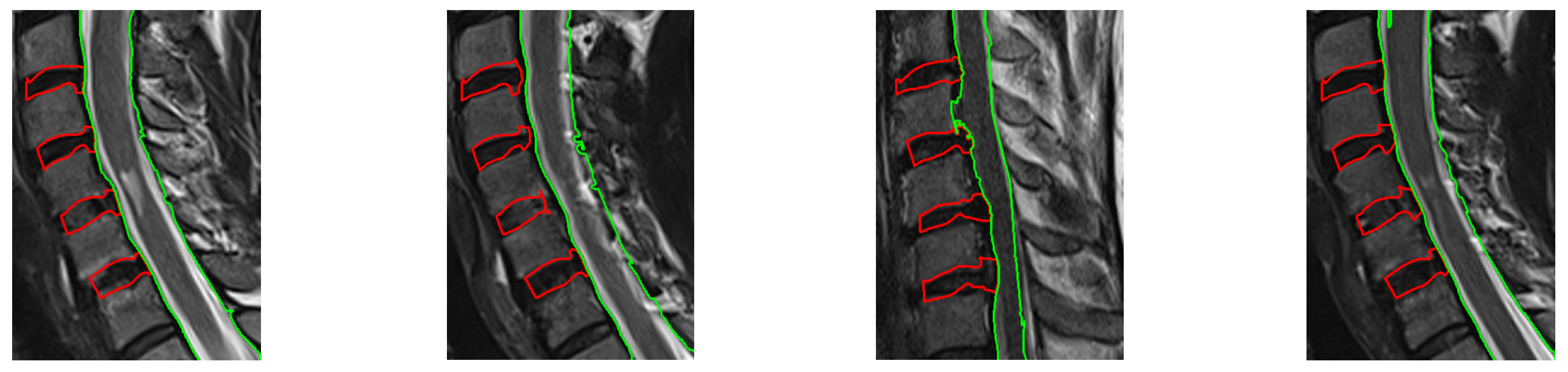
2.2. ASM Positioning on T1-Weighted MR and Transfer to T2-Weighted MR Image
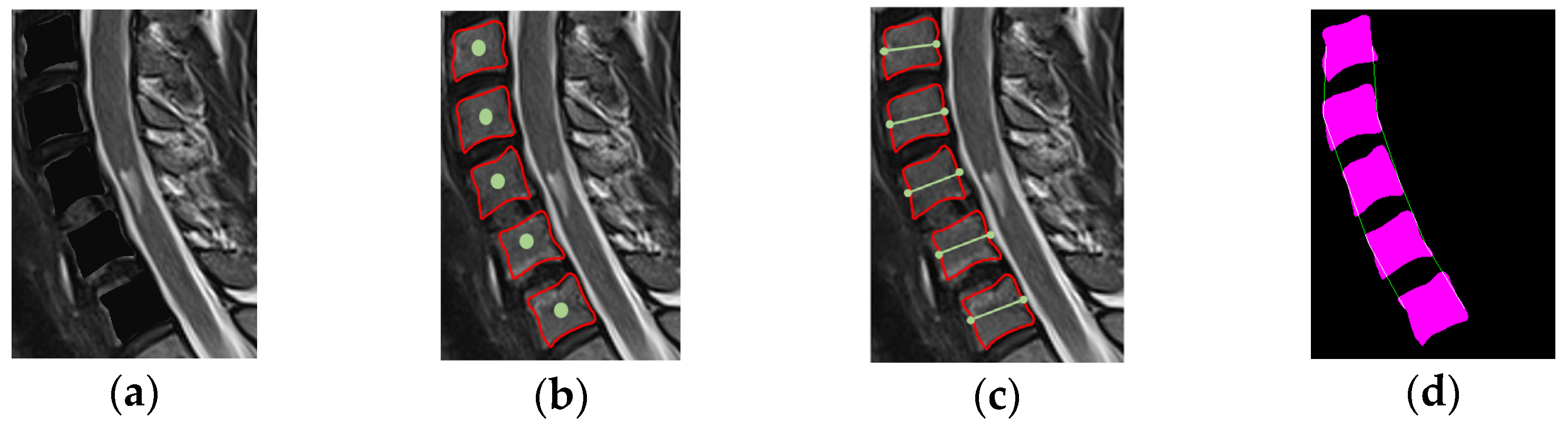
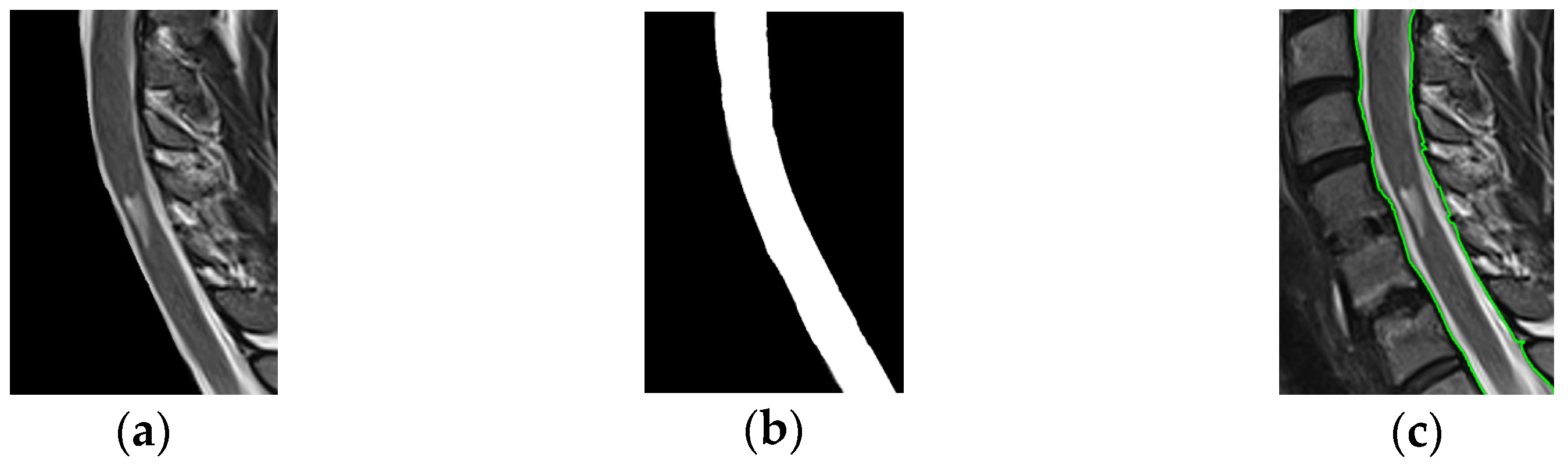
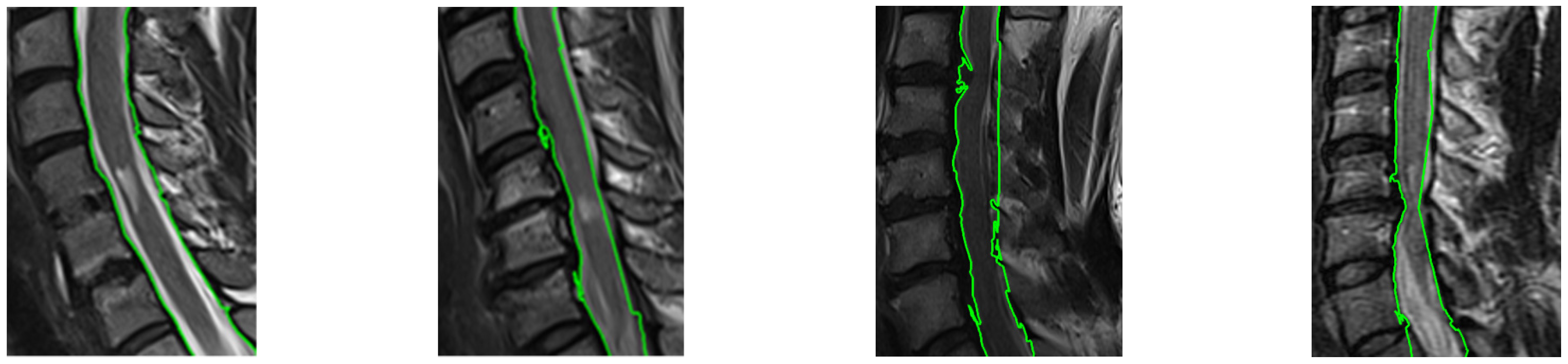
2.3. SC and IVD Boundary Extraction
3. Experimental Evaluation
3.1. Datasets
3.2. Evaluation Metrics
3.3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Emch, T.; Modic, M. Imaging of lumbar degenerative disk disease: History and current state. Skelet. Radiol. 2011, 40, 1175–1189. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Jian, F.; Wu, H.; Li, H. An improved level set method for vertebra CT image segmentation. Biomed. Eng. Online 2013, 12, 48. [Google Scholar] [CrossRef] [PubMed]
- Castro, I.M.J.; Pereañez, P.M.M.; Lekadir, K.; Lazary, A.; Frangi, A.F. Statistical interspace models (SIMs): Application to robust 3D spine segmentation. IEEE Trans. Med. Imaging 2015, 34, 1663–1675. [Google Scholar] [CrossRef] [PubMed]
- Zheng, G.; Chu, C.; Belavý, D.L.; Ibragimov, B.; Korez, R.; Vrtovec, T.; Hutt, H.; Everson, R.; Meakin, J.; Andrade, I.L. Evaluation and comparison of 3D intervertebral disc localization and segmentation methods for 3D T2 MR data: A grand challenge. Med. Image Anal. 2017, 35, 327–344. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Carassa, A.; Ohb, J.; Nairc, G.; Phamd, L.D.; Reichb, S.D.; Princea, L.J. Automatic magnetic resonance spinal cord segmentation with topology constraints for variable fields of view. Neuroimage 2013, 83, 1051–1062. [Google Scholar] [CrossRef] [PubMed]
- Yiannakas, M.C.; Mustafa, A.M.; Leener, B.; Kearney, H.; Tur, C.; Altman, D.R.; Angrlis, F.; Plantone, D.; Ciccarelli, O.; Miller, H.D.; et al. Fully automated segmentation of the cervical cord from T1-weighted MRI using PropSeg: Application to multiple sclerosis. NeuroImage Clin. 2016, 10, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Lemay, A.; Gros, C.; Zhuo, Z.; Zhang, J.; Duan, Y.; Cohen, A.J.; Liu, Y. Automatic Multiclass Intramedullary Spinal Cord Tumor Segmentation on MRI with Deep Learning. NeuroImage Clin. 2021, 31, 102766. [Google Scholar] [CrossRef]
- Koh, J.; Scott, D.P.; Chaudhary, V.; Dhillon, G. An automatic segmentation method of the spinal canal from clinical MR images based on an attention model and an active contour model. In Proceedings of the IEEE International Symposium on Biomedical Imaging (ISBI), Chicago, IL, USA, 30 March–2 April 2011. [Google Scholar]
- Asman, A.J.; Bryan, W.F.; Smith, S.A.; Reich, S.D.; Landman, A.B. Groupwise multi-atlas segmentation of the spinal cord’s internal structure. Med. Image Anal. 2014, 18, 460–471. [Google Scholar] [CrossRef]
- Zhang, X.; Yang, Y.; Shen, Y.W.; Li, P.; Zhong, Y.; Zhou, J.; Zhang, K.R.; Shen, C.Y.; Li, Y.; Zhang, M.F.; et al. SeUneter: Channel attentive U-Net for instance segmentation of the cervical spine MRI medical image. Front. Physiol. 2022, 13, 1081441. [Google Scholar] [CrossRef]
- Al Arif, S.M.M.R.; Knapp, K.; Slabaugh, G. Fully automatic cervical vertebrae segmentation framework for X-ray images. Comput. Methods Programs Biomed. 2018, 157, 95–111. [Google Scholar] [CrossRef] [PubMed]
- Sahar, S.; Hamed, D.; Seyed, A.H.B.; Ali, K.; Mohammad, A. Fully automatic 3D segmentation of the thoracolumbar spinal cord and the vertebral canal from T2-weighted MRI using K-means clustering algorithm. Spinal Cord 2020, 58, 811–820. [Google Scholar]
- Cootes, T.F.; Taylor, C.J.; Cooper, D.H.; Graham, J. Active shape models-their training and application. Comput. Vis. Image Underst. 1995, 61, 38–59. [Google Scholar] [CrossRef]
- Mohammed, B.; Saïd, M.; Fabian, L. A framework of vertebrae segmentation using the active shape model-based approach. Int. J. Biomed. Imaging 2011, 2011, 764046. [Google Scholar]
- Taha, A.A.; Hanbury, A. Metrics for Evaluation 3D Medical Image Segmentation: Analysis, Selection, and Tool. BMC Med. Imaging 2015, 15, 29. [Google Scholar] [CrossRef] [PubMed]
- Huttenlocher, D.; Klanderma, G.; Rucklidge, W. Comparing images using the Hausdorff distance. IEEE Trans. Pattern Anal. Mach. Intell. 1993, 15, 850–863. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Mean DSC (%) ± SD | Mean HD (mm) ± SD |
|---|---|---|
| Al Arif et al. [11] (Unet) | 84 ± 1.3 | 1.6 ± 2.6 |
| Al Arif et al. [11] (UNet-S) | 84 ± 1.3 | 1.6 ± 2.5 |
| Zhang et al. [10] (U-Net) | 85.09 ± 1.65 | - |
| Zhang et al. [10] (AttU-Net) | 87.68 ± 1.55 | - |
| Zhang et al. [10] (UNet++) | 85.08 ± 1.62 | - |
| Zhang et al. [10] (DeepLab-v3+) | 88.78 ± 1.78 | - |
| Zhang et al. [10] (TransUnet) | 87.9 ± 1.53 | - |
| Zhang et al. [10] (Swin-Unet) | 84.51 ± 1.55 | - |
| Proposed | 88.6 ± 5.2 | - |
| Method | Mean DSC (%) ± SD |
|---|---|
| Zhang et al. [10] (U-Net) | 85.09 ± 1.65 |
| Zhang et al. [10] (AttU-Net) | 87.68 ± 1.55 |
| Zhang et al. [10] (UNet++) | 85.08 ± 1.62 |
| Zhang et al. [10] (DeepLab-v3+) | 88.78 ± 1.78 |
| Zhang et al. [10] (TransUnet) | 87.9 ± 1.53 |
| Zhang et al. [10] (Swin-Unet) | 84.51 ± 1.55 |
| Proposed | 84.9 ± 2.4 |
| Method | Mean DSC (%) ± SD | Mean HD (mm) ± SD |
|---|---|---|
| Sahar et al. [12] | 81 ± 4 | 12.3 ± 2.4 |
| Zhang et al. [10] (U-Net) | 85.09 ± 1.65 | - |
| Zhang et al. [10] (AttU-Net) | 87.68 ± 1.55 | - |
| Zhang et al. [10] (UNet++) | 85.08 ± 1.62 | - |
| Zhang et al. [10] (DeepLab-v3+) | 88.78 ± 1.78 | - |
| Zhang et al. [10] (TransUnet) | 87.9 ± 1.53 | - |
| Zhang et al. [10] (Swin-Unet) | 84.51 ± 1.55 | - |
| Proposed | 90 ± 3.5 | 4.3 ± 2.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liaskos, M.; Savelonas, M.A.; Asvestas, P.A.; Matsopoulos, G.K. Bimodal Active Shape Models for Cervical Vertebrae and Spinal Canal Boundary Extraction. Eng. Proc. 2023, 50, 1. https://doi.org/10.3390/engproc2023050001
Liaskos M, Savelonas MA, Asvestas PA, Matsopoulos GK. Bimodal Active Shape Models for Cervical Vertebrae and Spinal Canal Boundary Extraction. Engineering Proceedings. 2023; 50(1):1. https://doi.org/10.3390/engproc2023050001
Chicago/Turabian StyleLiaskos, Meletios, Michalis A. Savelonas, Pantelis A. Asvestas, and George K. Matsopoulos. 2023. "Bimodal Active Shape Models for Cervical Vertebrae and Spinal Canal Boundary Extraction" Engineering Proceedings 50, no. 1: 1. https://doi.org/10.3390/engproc2023050001
APA StyleLiaskos, M., Savelonas, M. A., Asvestas, P. A., & Matsopoulos, G. K. (2023). Bimodal Active Shape Models for Cervical Vertebrae and Spinal Canal Boundary Extraction. Engineering Proceedings, 50(1), 1. https://doi.org/10.3390/engproc2023050001