Abstract
At the starting point of this case study, a garrison hospital performed an assessment of the need for treatment when the number of conscripts queuing at reception is at its highest level. The research aims to find out the reasons for conscripts’ perceived long waiting times, which causes absence from the conscripts’ training. According to the predictions made by the queuing simulation, the hospital’s staff are able to receive patients arriving at reception in the morning without the queue time causing undue harm to training. However, during large congestion peaks, the waiting times may become unreasonable, which would require an increase in human resources. Peaks of congestion usually occur at the beginning of the week, as well as on days with heavy military training.
1. Introduction
The modelling of health care resources is especially important after a time of crisis, which is the case for example after a pandemic. Indeed, COVID-19 has had a significant impact on health care in Finland. According to the Finnish Institute for Health and Welfare (THL), the number of hospital visits due to COVID-19 increased a lot between March and April 2020 [1]. In addition, there was an increase in waiting times for specialized health care ([2], Figure 7). The pandemic also put a strain on personnel resources within the health care system, with many of the staff reallocated from other departments or working long hours to cope with demand.
In the defense forces, the general service regulations (YLPALVO) define the following for those performing health care services: “The defense forces are responsible for organizing the health care of conscripts in service, women performing voluntary military service and students being trained for military service, as well as those participating in voluntary exercises and supervised shootings of the defense forces and training ordered from the National Defense Training Association. The health care of the Defense Forces is open health care by nature. Nurse and doctor appointments are arranged according to local special conditions, needs, and resources. The goal is to use health care methods to secure the service safety of the persons under the care of the Defense Forces. A conscript in service has the right to medical examination by a healthcare professional without unnecessary delay. Dental care is organized in accordance with local needs and conditions, either as the Defense Forces’ own activity or as a purchased service.” ([3], pp. 42–43).
Here, we use a simulation to show the effects of alternating queuing conditions for health center operational status. In order to establish our simulation model, we used queueing theory, which is the mathematical study of queues [4]. This study is also part of operations research since we use the simulation results to make decisions about the resources needed to provide a service.
Queueing theory is important because it helps to identify and analyze the queues that form in many different systems. It provides insights into how to manage queues, as well as how to allocate resources so that serving customers is effective with minimal waiting times. Queueing theory has applications in many areas such as healthcare, telecommunications networks, airport check-in, computer processing, traffic control systems, manufacturing processes, etc. If one understands the principles of queueing theory, one can make better decisions when it comes to resource allocation and customer service management. Earlier, we used queueing theory in the Finnish Defence Forces (FDF), for example, in the modelling of custom inspections in [5] and in the tactical warfare simulator SANDIS, which uses Markov chains [6].
The main factors of queueing theory are [7]:
- Arrival rate—the rate at which customers or jobs enter the system.
- Number of service channels—the number of servers or machines available to process requests from customers in the queue.
- Queue discipline—the serving order of customers, such as first come, first served (FIFO) or last in, first out (LIFO).
- Service rate—the service rate of customers or jobs.
- Queue length—the number of customers waiting in line to be served by the service facility.
- Utilization—a measure of how busy a resource is, typically expressed as a percentage of its capacity (e.g., 80% utilization).
- Waiting time—the amount of time that elapses between when a customer arrives and when he/she is served by the service facility.
- Throughput—the average number of customers or jobs processed per unit of time (e.g., per hour).
In medical services, we use queue theory to help optimize the efficiency of patient care. To achieve this, we manage waiting times, prioritize patients based on their need for treatment, and analyze how changes in staffing or scheduling affect the overall efficiency of a facility [8]. Queue theory helps healthcare providers balance demand with resources by helping them understand how many beds they need, when they should schedule staff shifts, and where they should allocate additional resources. Queue theory can also forecast future patient loads so that facilities can plan accordingly.
This work deals with the use of the health care services of a garrison health center by those performing their military service from the point of view of the time spent waiting in line. We investigate the capacity of the health center and the effect of “peak congestion” on service times. We find out what would be the optimal number of reception points, without the need for resources changing significantly. The aim is to model the current situation as accurately as possible, from the perspective of how long a conscript waits for access to receive treatment in normal situations and during peak traffic.
2. Problem Description
We investigated the ability of the Finnish garrison hospital of the Kainuu brigade to perform an assessment of the need for medical treatment when the number of conscripts (max. 600) queuing at reception is at its highest level and the ratio of patients to nurses is at its maximum level. The aim of the study is to illustrate with which nurse capacity the duration of treatment queues could be at such a level that all conscripts queuing at reception in the morning would be able to return to their basic unit service during the morning. The starting point of the review is how to serve conscripts registered for the morning health check-up within the 120-min time window. The purpose of the work is to investigate the capacity of the health center’s queuing services and the effect of “traffic peaks” on service times. We are looking for an answer to the question of what the optimal number of reception points would be without the need for resources changing significantly. We model how long a conscript waits for access to the evaluation of the need for treatment in normal situations and during peak traffic.
Here, we studied patients from the moment they sign up for the morning reception. The observed queue begins to form from the moment when the conscript reports their need for treatment and reaches the nurse’s preliminary check-up and the doctor’s check-up if it is necessary. The reviewed queue ends when a medical professional has assessed the person’s state of health. The research aims to find ways to reduce the time spent in the queue. The morning reception starts at 07:00. In terms of the smooth running of conscript training, persons capable of service must return to service within two hours. We are investigating whether it is possible to serve all conscripts within 120 min: how many conscripts can we examine and what number of nursing staff does this require?
3. Model and Results
The queuing mechanics of the garrison hospital can be thought of as a single queue with several servants and stages. The behavior of the queue can be described using certain expectation values. The parameters needed for the calculation are the number of customers joining the queue per time unit and the average number of customers served per time unit. The subject under review is the Kainuu brigade and the healthcare services provided by its health center. The service regulations of the Kainuu brigade dictate the following when registering for the morning reception of basic units:
- To register for the morning reception, the conscript reports to the unit’s duty officer after waking up.
- The health center calls through the units and collects the preliminary strengths of those who come to the reception by unit.
- Conscripts registered for the morning reception do not take part in the day’s service and wait in their rooms until the unit’s personnel are ordered to the health center for their turn.
- Those who have signed up for the reception of the first three basic units of the breakfast shift of the Kainuu brigade will go directly from breakfast to the reception.
- Other units are called to the reception systematically, and the health center schedules their arrival.
The queue model is defined here by the following five rules:
- A:
- How to join the queue? Since all conscripts aiming for the morning reception start queuing when they report to the duty officer of their unit immediately after being woken up, in queue modeling, everyone starts queuing at the same moment. The method of joining the queue does not involve a statistical distribution and therefore does not affect the modeling values. In the modeling, it has been assumed that the customers are in a queue together and they are served at the next free service point in order of arrival. There is therefore no queue for each service point.
- B:
- How to exit the queue? You leave the queue after the treatment time is over. In the modeling of the queue, the treatment duration is normally distributed so that the average is 2.0 min and the standard deviation is 0.5 min.
- C:
- Number of service channels. This study examines the garrison hospital’s ability to process patients in a given time, where the analysis involves changing the number of service places to achieve the most optimal outcome.
- D:
- Maximum queue length. The maximum length of the queue has been defined as 600 people because according to experts, this is the longest queue formed at the KAIPR garrison hospital.
- E:
- Queuing principle. The queue at the garrison hospital works with the first in, first out (FIFO) method, i.e., the first customer in the queue is also the first to leave the service point. The model does not take into account the fact that the customer could leave the queue in the middle of queuing, as this is practically not possible for on-duty personnel. It is also not possible to skip the queue, and acute cases do not even enter this queue.
Here, it is not meaningful to calculate the load factor of the queue because every customer starts queuing at the same time. After the customer joins the queue, they are taken care of anyway. The purpose of the modeling is to find out by what means the total duration of the queue can be made as short as possible.
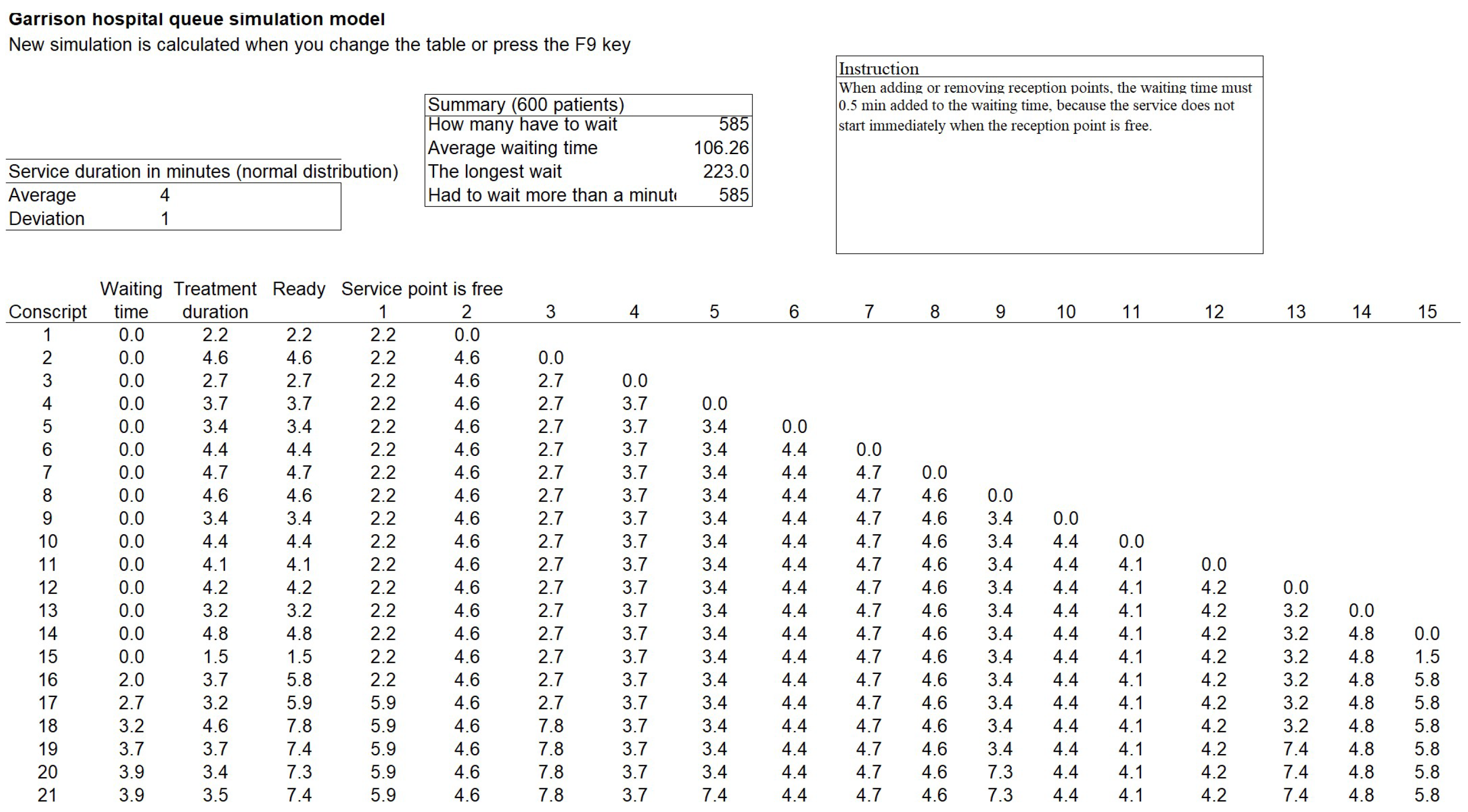
In the simulation model in Figure 1, the “waiting time” column shows when the conscript can get to reception. The model takes into account the fact that the first conscripts get to the nurse immediately, without queuing. Half a minute has been added to the waiting time after each person on duty so that the nurse has time to invite a new patient in before the start of the treatment period. In addition, the breaks taken by the nurses have been taken into account by adding 15 min at 60, 120, and 180 min for each service point. At present, a maximum of 15 nurses can be provided to the health center, and in the worst case, all 500 conscripts would feel sick.
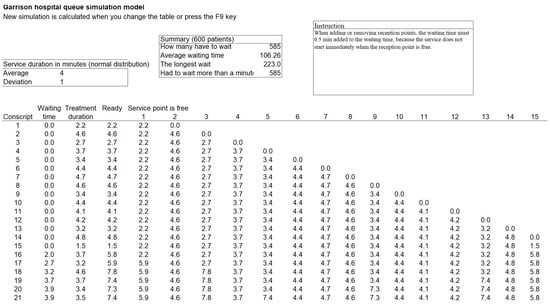
Figure 1.
An Illustration of the simulation model of the garrison hospital.
4. Results
Table 1 reflects the current efficiency and personnel situation of the garrison hospital. The research wanted to examine the actual maximum strengths, so field nurses have also been included in the nurse strength from the enhanced strength onwards.

Table 1.
The largest possible number of patients with the current nursing staff.
Table 2 shows the number of nurses needed at different times. If the need for treatment is assessed in two hours, the conscript still has time to participate in afternoon training. If the assessment takes more than four hours, the conscript does not have time to participate in training for the whole day.
Table 2.
The required number of nurses in different situations.
5. Discussion and Future
Most of the garrisons in Finland, like the Kajaani brigade considered here, are large entities comprising several basic units centrally served by the garrison health station. Thus, we can conclude that the modeling carried out here gives a sufficiently accurate overview for identifying problem points. According to the results of the research, the hospital’s staff are able to receive patients arriving for the morning reception without the waiting time causing undue harm to training. This means an absence of less than two hours from training due to queuing. This is realized when the total number of arriving patients is a maximum of approximately 250 patients. At peaks of congestion, where the number of patients can rise to more than 500 patients, the capacity of the garrison health center is not sufficient to keep the waiting times reasonable. This would require an increase in human resources. Congestion peaks occur especially after returning from holidays and on days with heavy outdoor training. The research aimed to observe the reasons for conscripts’ perceived long waiting times, which partly cause unnecessary absences from training. Based on the research, it is possible to examine the current system and evaluate its ability to cope with the number of customers. However, the research does not provide practical answers as to how to correct the observed problems. This is because health care is very carefully regulated both by law and by the Defence Forces’ own regulations. Consequently, the effects of all changes must be evaluated from the perspective of the patient’s legal protection, for example. This modeling clearly supports the existence of the problem. Solutions to the problem should be explored with further research. This new research should focus on how congestion peaks in particular could be smoothed out by referring non-urgent patients to other days based on advance reservations.
Author Contributions
Conceptualization, K.S.; methodology, K.S.; software, K.S.; validation, J.S., J.H., P.P. and A.L.; formal analysis, J.S., J.H., P.P. and A.L.; investigation, J.S., J.H., P.P. and A.L.; resources, J.S., J.H., P.P. and A.L.; data curation, J.S., J.H., P.P. and A.L.; writing—original draft preparation, K.S.; writing—review and editing, K.S. and A.R.; visualization, K.S:; supervision, K.S.; project administration, K.S.; funding acquisition, K.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
We have used only anonymous data during this research.
Data Availability Statement
Data is available through Kalle Saastamoinen, kalle.saastamoinen@mil.fi.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Open Data-THL. Finnish Institute for Health and Welfare. Available online: https://thl.fi/en/web/thlfi-en/statistics-and-data/data-and-services/open-data (accessed on 9 February 2023).
- Tiirinki, H.; Tynkkynen, L.K.; Sovala, M.; Atkins, S.; Koivusalo, M.; Rautiainen, P.; Jormanainen, V.; Keskimäki, I. COVID-19 pandemic in Finland–Preliminary analysis on health sys-tem response and economic consequences. Health Policy Technol. 2020, 9, 649–662. [Google Scholar] [CrossRef] [PubMed]
- Finnish Defence Forces. Yleinen Palvelusohjesääntö (YLPALVO); Halonen, P., Karvinen, I., Eds.; Puolustusvoimat; 2017; Available online: https://puolustusvoimat.fi/documents/1948673/2258487/PEVIESTOS_YLPALVO+2017/3684dac2-c7ac-4d93-b792-34649f6e2f5d/PEVIESTOS_YLPALVO+2017.pdf (accessed on 13 February 2023).
- Sundarapandian, V. Probability, Statistics and Queuing Theory; PHI Learning Pvt. Ltd.: New Delhi, India, 2009. [Google Scholar]
- Saastamoinen, K.; Mattila, P.; Rissanen, A. A Simulation of a Custom Inspection in the Airport. In Theory and Applications of Time Series Analysis: Selected Contributions from ITISE 2018; Springer International Publishing: Berlin/Heidelberg, Germany, 2019; Volume 5, pp. 319–330. [Google Scholar] [CrossRef]
- Lappi, E. Computational methods for tactical simulations. Ph.D. Thesis, Maanpuolustuskorkeakoulu, Helsinki, Finland, 2012. [Google Scholar]
- Gross, D. Fundamentals of Queueing Theory; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- Fomundam, S.; Herrmann, J.W. A Survey of Queuing Theory Applications in Healthcare. In Institute for Systems Research Technical Reports; A. James Clark School of Engineering at the University of Maryland: College Park, MD, USA, 2007. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).