
Pregnancy Labor Prediction Using Magnetomyography Sensing and a Self-Sorting Cybernetic Model †


 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
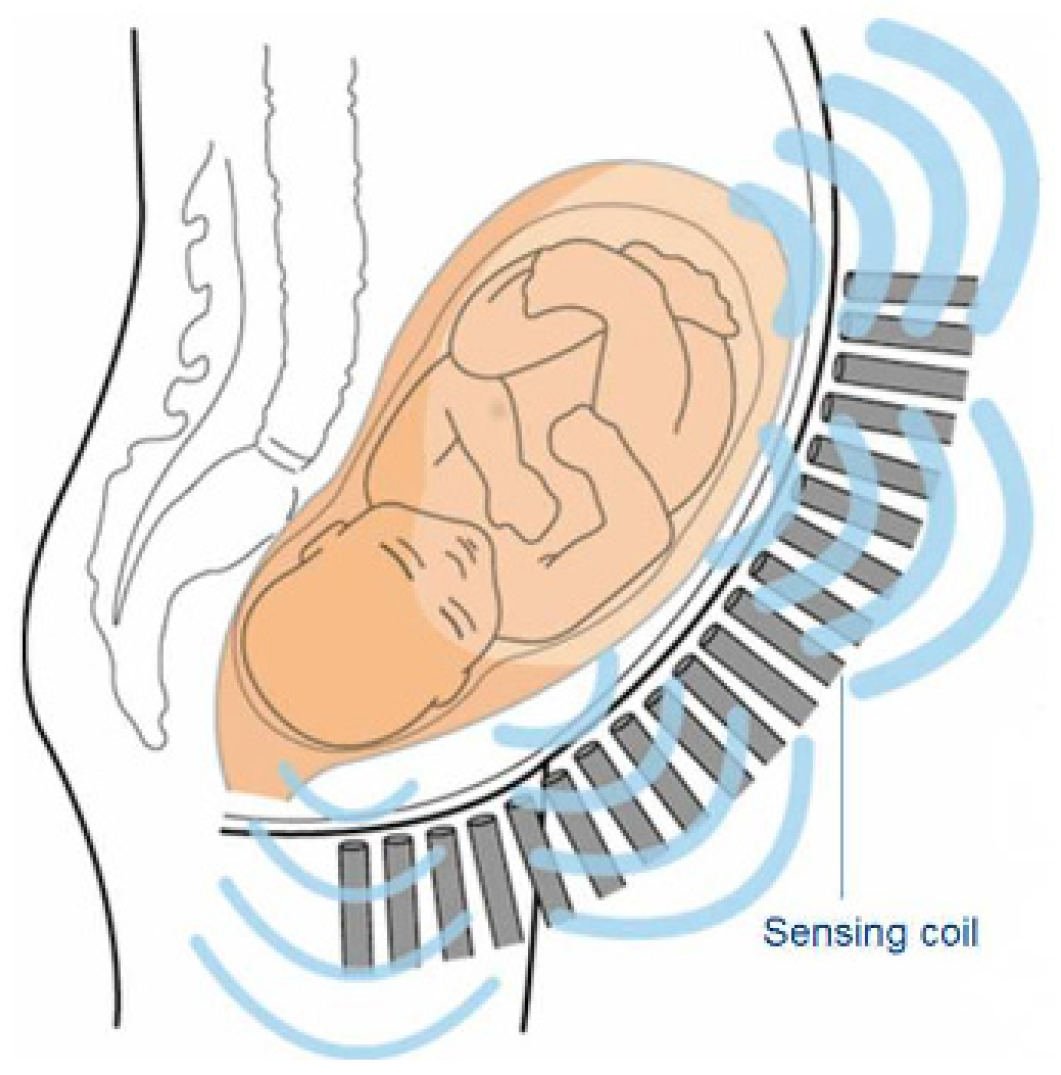
2.1. Magnetic Field
2.2. MMG Dataset
2.3. Cybernetic Model
2.3.1. Signal Decomposition
2.3.2. Feature Extraction
2.3.3. Dimensionality Reduction
2.3.4. Unsupervised Learning and Labor Prediction
3. Results and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Offiah, I.; Odonoghue, K.; Kenny, L. Clinical Risk Factors for Preterm Birth. In Preterm Birth—Mother and Child; Morrison, J., Ed.; InTech: Vienna, Austria, 2012; ISBN 978-953-307-828-1. [Google Scholar]
- Oskovi Kaplan, Z.A.; Ozgu-Erdinc, A.S. Prediction of Preterm Birth: Maternal Characteristics, Ultrasound Markers, and Biomarkers: An Updated Overview. J. Pregnancy 2018, 2018, 8367571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
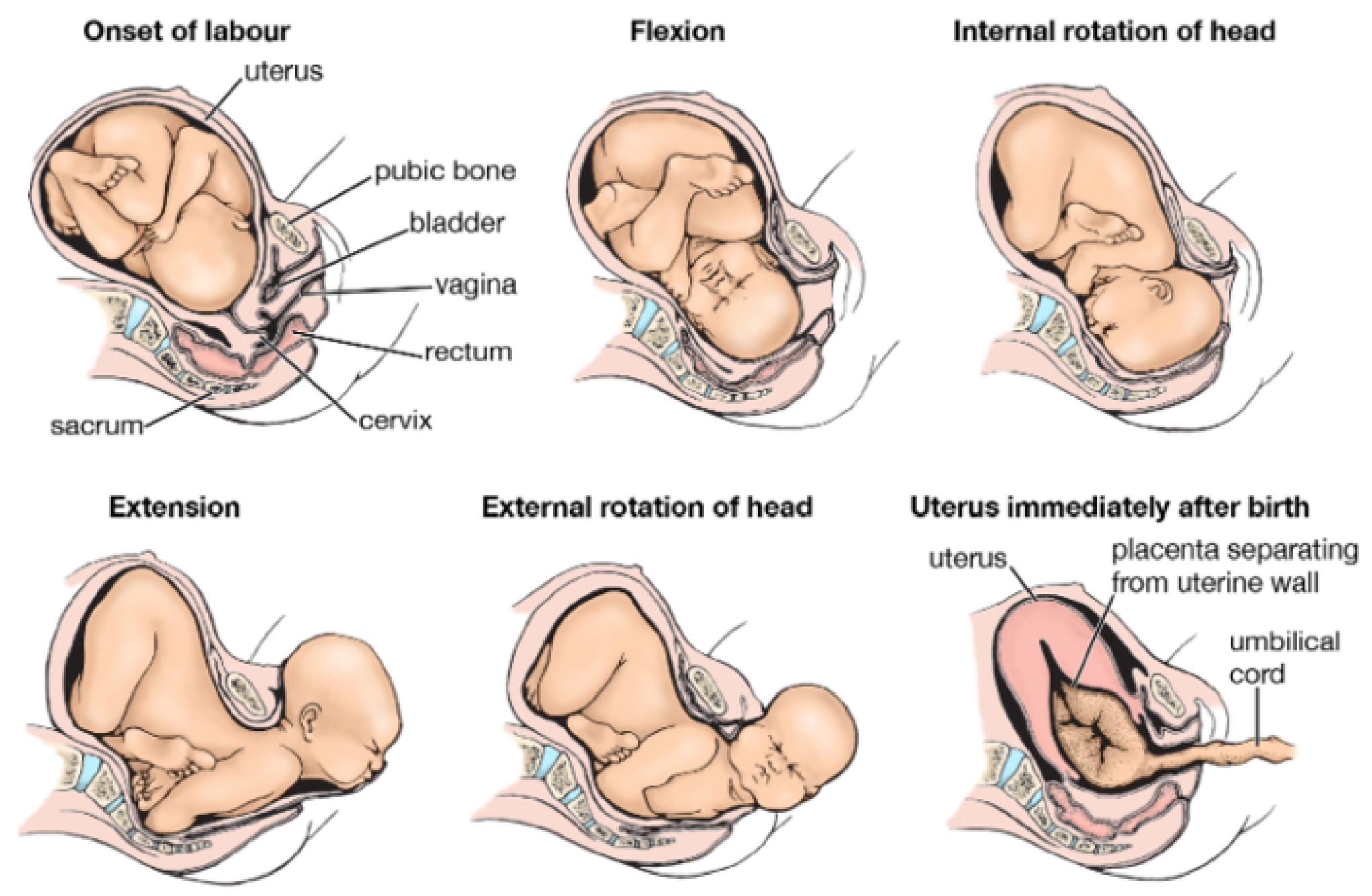
- Birth—Fetal Presentation and Passage through the Birth Canal. Available online: https://www.britannica.com/science/birth (accessed on 1 May 2021).
- Alberola-Rubio, J.; Garcia-Casado, J.; Prats-Boluda, G.; Ye-Lin, Y.; Desantes, D.; Valero, J.; Perales, A. Prediction of Labor Onset Type: Spontaneous vs. Induced; Role of Electrohysterography? Comput. Methods Programs Biomed. 2017, 144, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Moslem, B.; Hassan, M.; Khalil, M.; Marque, C.; Diab, M.O. Monitoring the Progress of Pregnancy and Detecting Labor Using Uterine Electromyography. In Proceedings of the 2009 International Symposium on Bioelectronics & Bioinformatics, Melbourne, Australia, 9–11 December 2009. [Google Scholar]
- Nsugbe, E.; Samuel, O.W.; Sanusi, I.; Asogbon, M.G.; Li, G. A Study on Preterm Predictions Using Physiological Signals, Medical Health Record Information and Low Dimensional Embedding Methods. IET Cyber-Syst. Robot. 2021, 3, 228–244. [Google Scholar] [CrossRef]
- Nsugbe, E.; Obajemu, O.; Samuel, O.W.; Sanusi, I. Enhancing Care Strategies for Preterm Pregnancies by Using a Prediction Machine to Aid Clinical Care Decisions. Mach. Learn. Appl. 2021, 6, 100110. [Google Scholar] [CrossRef]
- Nsugbe, E.; Obajemu, O.; Samuel, O.W.; Sanusi, I. Application of non-invasive magnetomyography in labor imminency prediction for term and preterm pregnancies and ethnicity specific labor imminency prediction. Mach. Learn. Appl. 2021, 5, 100066. [Google Scholar]
- Soni, D. Supervised vs. Unsupervised Learning. Available online: https://towardsdatascience.com/supervised-vs-unsupervised-learning-14f68e32ea8d (accessed on 1 May 2021).
- Wiener, N. Cybernetics: Or, Control and Communication in the Animal and the Machine, 2nd ed.; The MIT Press: Cambridge, MA, USA, 2019; ISBN 978-0-262-53784-1. [Google Scholar]
- Escalona-Vargas, D.; Govindan, R.B.; Furdea, A.; Murphy, P.; Lowery, C.L.; Eswaran, H. MMG Database. PhysioNet, 4 March 2016. [Google Scholar]
- Escalona-Vargas, D.; Govindan, R.B.; Furdea, A.; Murphy, P.; Lowery, C.L.; Eswaran, H. Characterizing the Propagation of Uterine Electrophysiological Signals Recorded with a Multi-Sensor Abdominal Array in Term Pregnancies. PLoS ONE 2015, 10, e0140894. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a New Research Resource for Complex Physiologic Signals. Circulation 2000, 101, E215–E220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Rosa, P.S.; Eswaran, H.; Preissl, H.; Nehorai, A. Multiscale Forward Electromagnetic Model of Uterine Contractions during Pregnancy. BMC Med. Phys. 2012, 12, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.; La Rosa, P.S.; Eswaran, H.; Nehorai, A. Estimating Uterine Source Current during Contractions Using Magnetomyography Measurements. PLoS ONE 2018, 13, e0202184. [Google Scholar] [CrossRef] [PubMed]
- Nsugbe, E.; Sanusi, I. Towards an Affordable Magnetomyography Instrumentation and Low Model Complexity Approach for Labour Imminency Prediction Using a Novel Multiresolution Analysis. Appl. AI Lett. 2021. [Google Scholar] [CrossRef]
- Nsugbe, E.; Samuel, O.W.; Asogbon, M.G.; Li, G. Contrast of multi-resolution analysis approach to transhumeral phantom motion decoding. CAAI Trans. Intell. Technol. 2021, 6, 360–375. [Google Scholar] [CrossRef]
- Nsugbe, E.; Ruiz-Carcel, C.; Starr, A.; Jennions, I. Estimation of Fine and Oversize Particle Ratio in a Heterogeneous Compound with Acoustic Emissions. Sensors 2018, 18, 851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nsugbe, E.; Starr, A.; Ruiz Carcel, C. Monitoring the Particle Size Distribution of a Powder Mixing Process with Acoustic Emissions: A Review. Eng. Technol. Ref. 2012, 1–12. [Google Scholar] [CrossRef]
- Nsugbe, E.; Starr, A.; Foote, P.; Ruiz-Carcel, C.; Jennions, I. Size Differentiation of a Continuous Stream of Particles Using Acoustic Emissions. IOP Conf. Ser. Mater. Sci. Eng. 2016, 161, 012090. [Google Scholar] [CrossRef] [Green Version]
- Phinyomark, A.; Limsakul, C.; Phukpattaranont, P. Application of Wavelet Analysis in EMG Feature Extraction for Pattern Classification. Meas. Sci. Rev. 2011, 11, 45. [Google Scholar] [CrossRef]
- Jolliffe, I.T.; Cadima, J. Principal Component Analysis: A Review and Recent Developments. Philos. Trans. R. Soc. A 2016, 374, 20150202. [Google Scholar] [CrossRef] [PubMed]
- Nsugbe, E.; Samuel, O.W.; Asogbon, M.G.; Li, G. A Self-Learning and Adaptive Control Scheme for Phantom Prosthesis Control Using Combined Neuromuscular and Brain-Wave Bio-Signals. Eng. Proc. 2020, 2, 59. [Google Scholar] [CrossRef]
- Carrasco, O.C. Gaussian Mixture Models Explained. Available online: https://towardsdatascience.com/gaussian-mixture-models-explained-6986aaf5a95 (accessed on 4 May 2021).
- Samuel, O.W.; Asogbon, G.M.; Sangaiah, A.K.; Fang, P.; Li, G. An Integrated Decision Support System Based on ANN and Fuzzy_AHP for Heart Failure Risk Prediction. Expert Syst. Appl. 2017, 68, 163–172. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nsugbe, E.; Samuel, O.W.; Sanusi, I.; Vishwakarma, S.; Adams, D. Pregnancy Labor Prediction Using Magnetomyography Sensing and a Self-Sorting Cybernetic Model. Eng. Proc. 2021, 10, 60. https://doi.org/10.3390/ecsa-8-11312
Nsugbe E, Samuel OW, Sanusi I, Vishwakarma S, Adams D. Pregnancy Labor Prediction Using Magnetomyography Sensing and a Self-Sorting Cybernetic Model. Engineering Proceedings. 2021; 10(1):60. https://doi.org/10.3390/ecsa-8-11312
Chicago/Turabian StyleNsugbe, Ejay, Oluwarotimi Williams Samuel, Ibrahim Sanusi, Suresh Vishwakarma, and Dawn Adams. 2021. "Pregnancy Labor Prediction Using Magnetomyography Sensing and a Self-Sorting Cybernetic Model" Engineering Proceedings 10, no. 1: 60. https://doi.org/10.3390/ecsa-8-11312
APA StyleNsugbe, E., Samuel, O. W., Sanusi, I., Vishwakarma, S., & Adams, D. (2021). Pregnancy Labor Prediction Using Magnetomyography Sensing and a Self-Sorting Cybernetic Model. Engineering Proceedings, 10(1), 60. https://doi.org/10.3390/ecsa-8-11312