

Knowledge of Diabetes among Adults at High Risk for Type 2 Diabetes in the Trivandrum District of Kerala, India

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
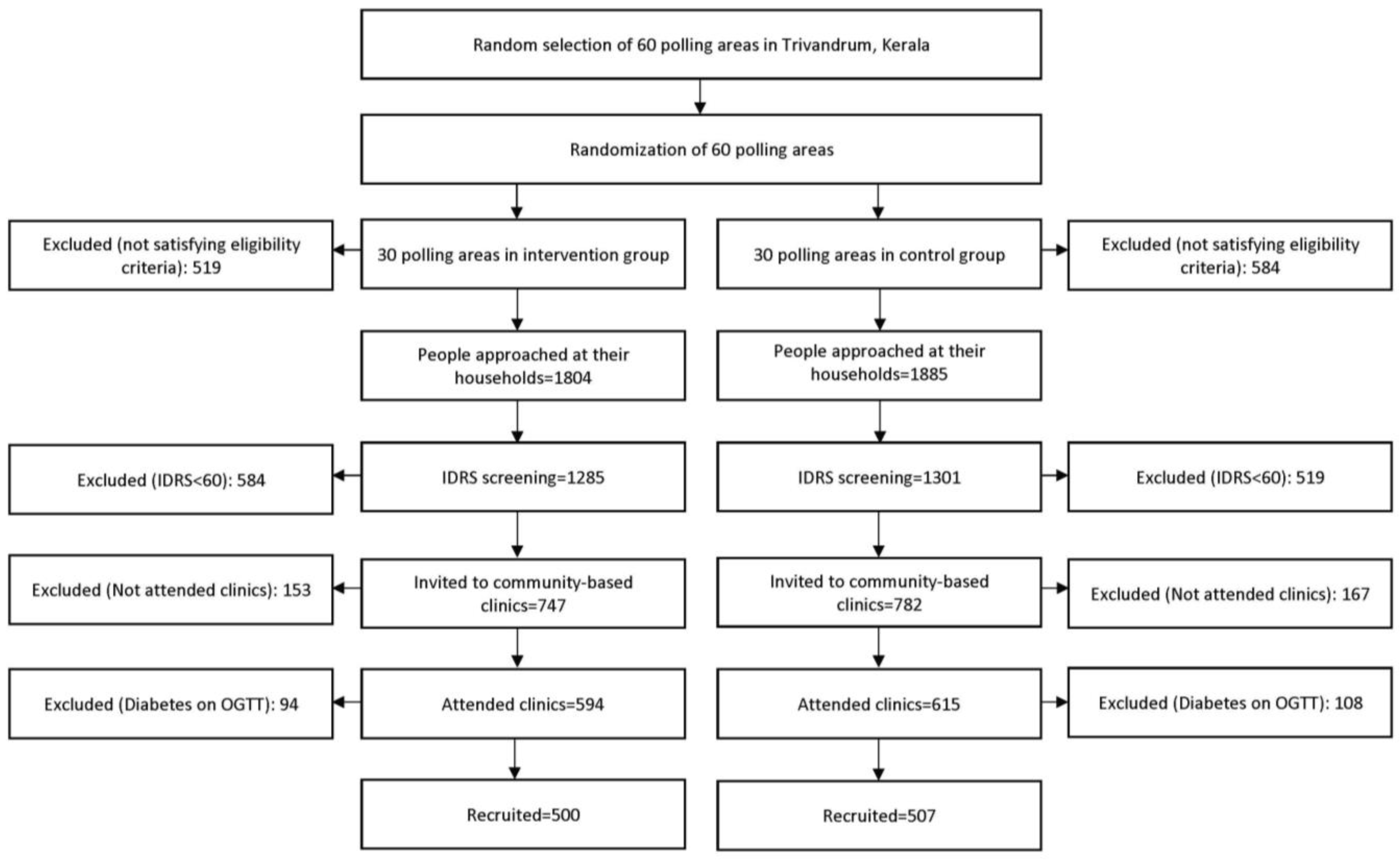
2.1. Study Design and Study Population
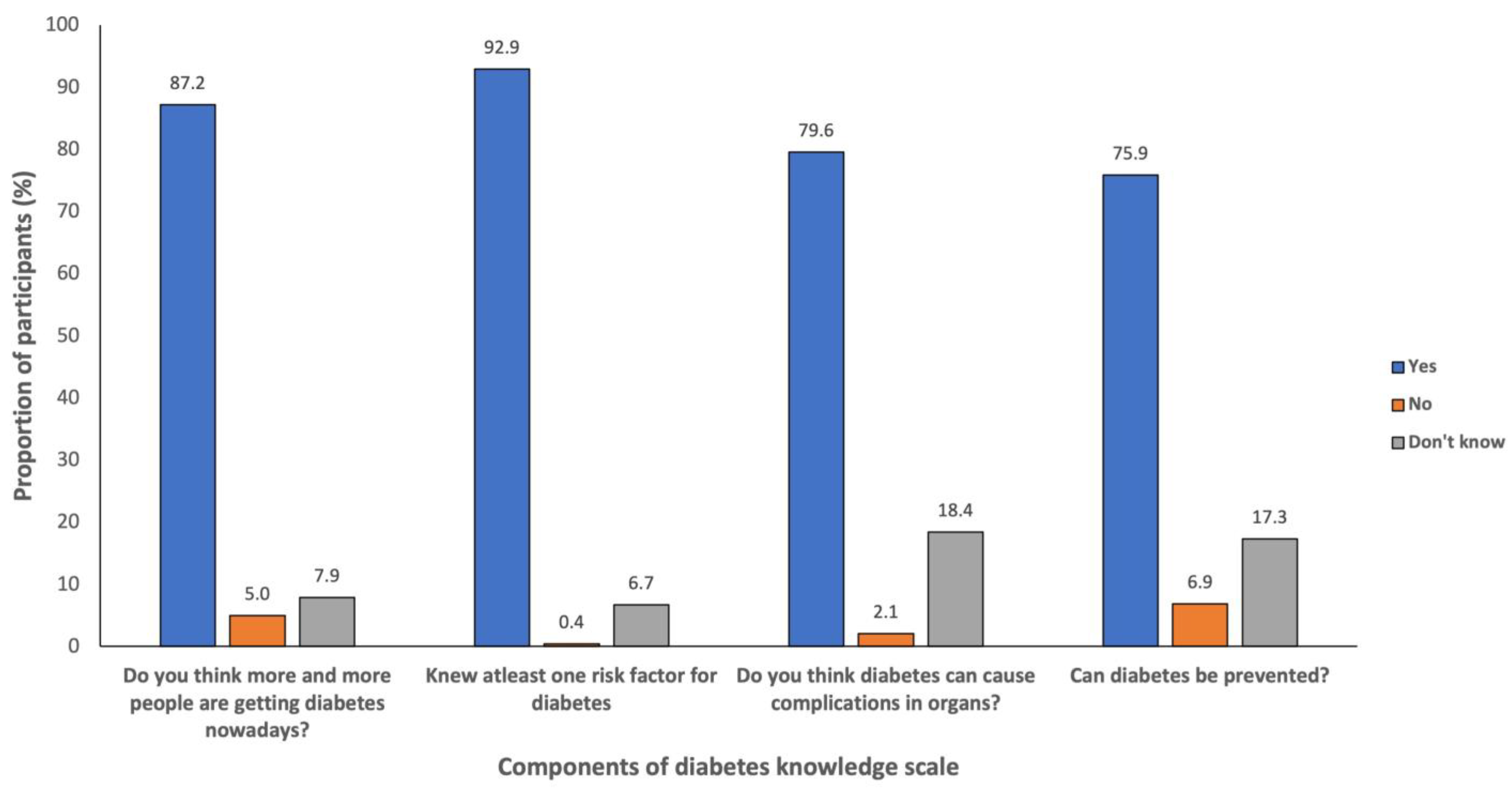
2.2. Diabetes Knowledge Scale
- Have you heard of the term diabetes? Yes/No
- If yes, do you think, in general, more and more people are getting affected with diabetes nowadays? Yes/No/Don’t know
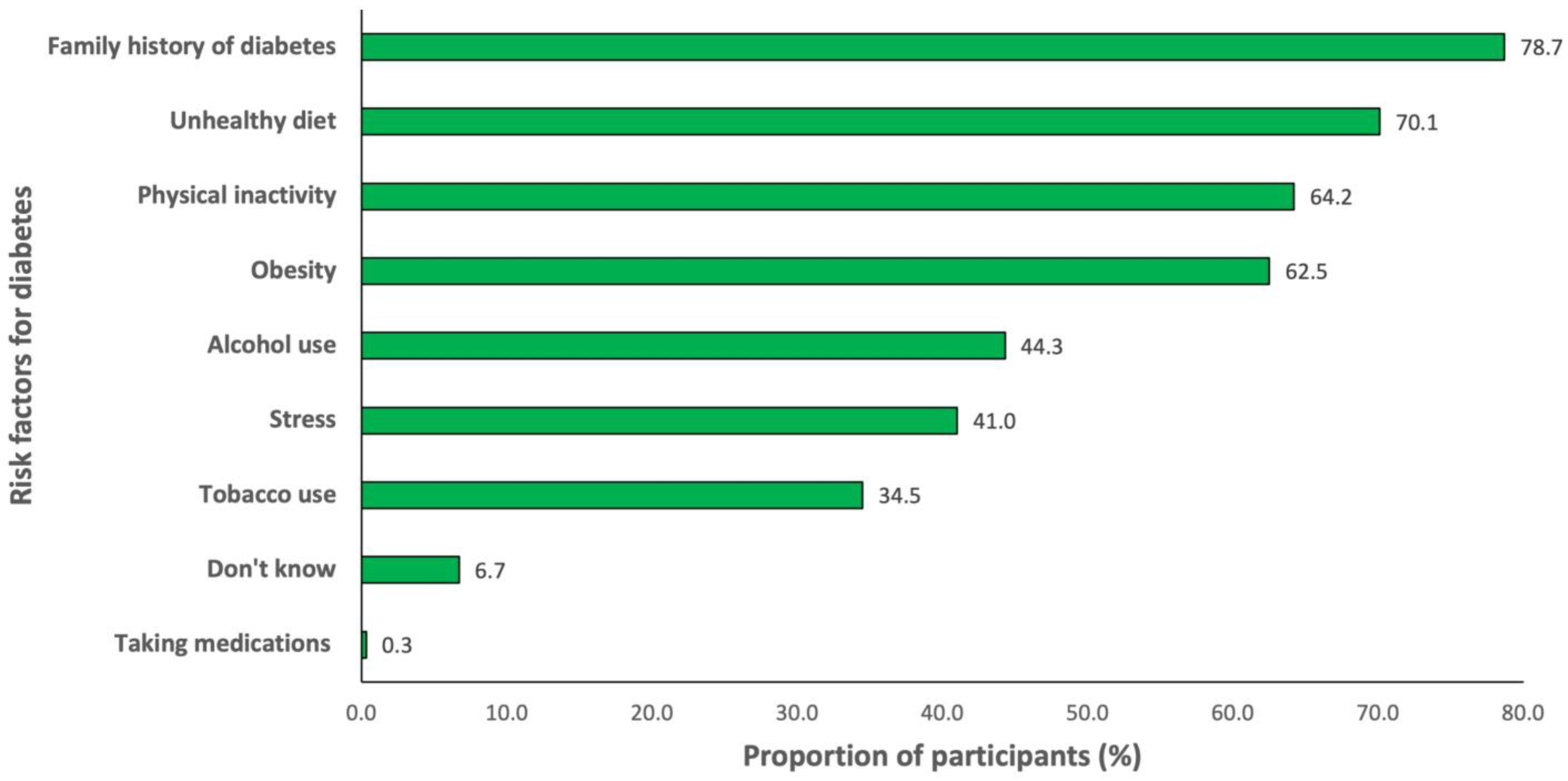
- What are the factors you think contribute to diabetes? (please circle as many as appropriate)
- Obesity
- Decreased physical activity
- Family history of diabetes
- Mental stress
- Unhealthy diet
- Tobacco use
- Alcohol use
- Others (specify)
- Don’t know
- Do you know that diabetes can cause complications in organs? Yes/No/Don’t know
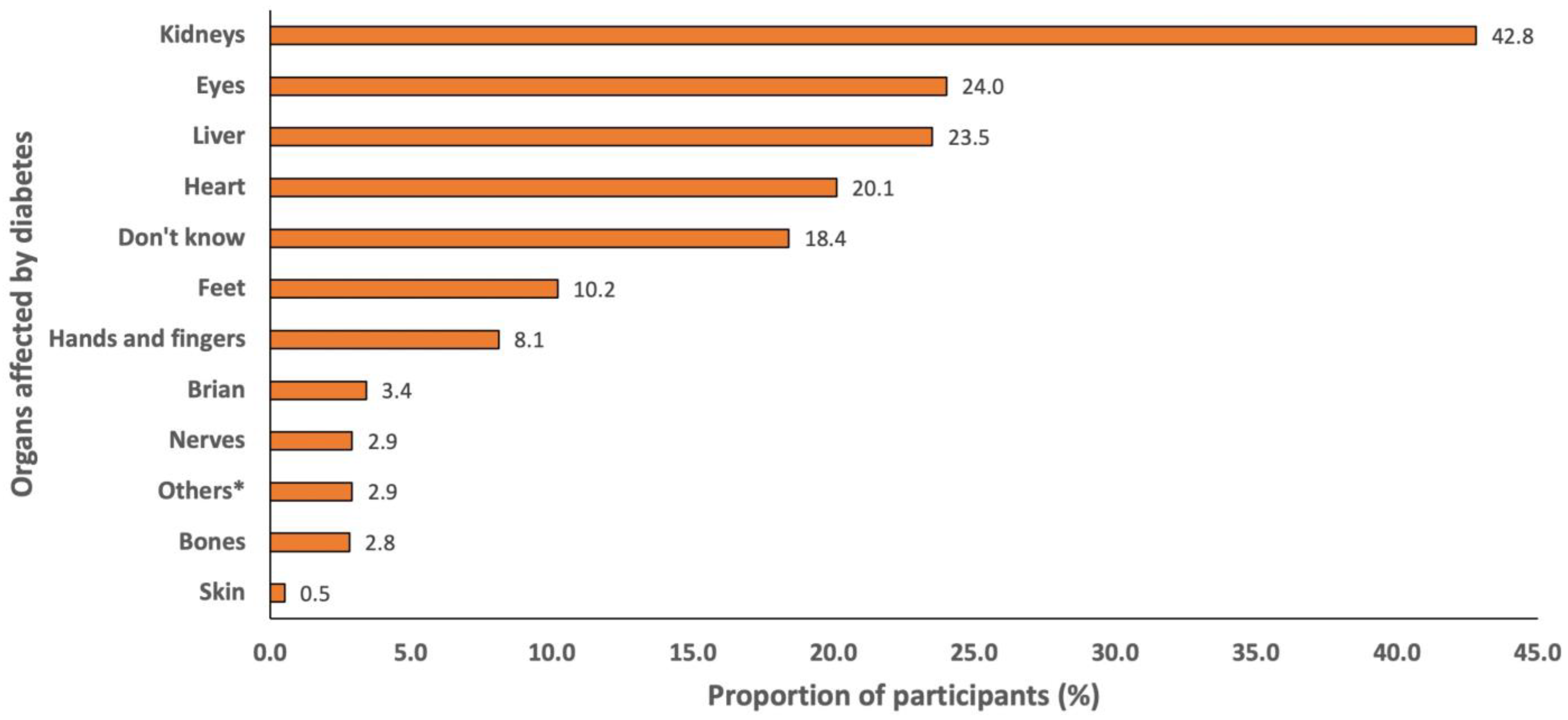
- If yes, which organs are they?
- Eyes
- Heart
- Nerves
- Feet
- Kidneys
- Hands and Fingers
- Bones
- Brain
- Liver
- Skin
- Others (specify)
- Don’t know
- Can diabetes be prevented? Yes/No/Don’t know
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Components of Diabetes Knowledge Scale and Diabetes Knowledge Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar]
- Oberoi, S.; Kansra, P. Economic menace of diabetes in India: A systematic review. Int. J. Diabetes Dev. Ctries 2020, 40, 464–475. [Google Scholar] [CrossRef] [PubMed]
- Weber, M.B.; Gujral, U.P.; Jagannathan, R.; Shah, M. Lifestyle Interventions for Diabetes Prevention in South Asians: Current Evidence and Opportunities. Curr. Diab. Rep. 2021, 21, 23. [Google Scholar] [CrossRef]
- Aziz, Z.; Absetz, P.; Oldroyd, J.; Pronk, N.P.; Oldenburg, B. A systematic review of real-world diabetes prevention programs: Learnings from the last 15 years. Implement. Sci. 2015, 10, 172. [Google Scholar] [CrossRef]
- Rani, P.K.; Raman, R.; Subramani, S.; Perumal, G.; Kumaramanickavel, G.; Sharma, T. Knowledge of diabetes and diabetic retinopathy among rural populations in India, and the influence of knowledge of diabetic retinopathy on attitude and practice. Rural Remote Health 2008, 8, 838. [Google Scholar] [CrossRef]
- Visser, A.; Snoek, F. Perspectives on education and counseling for diabetes patients. Patient Educ. Couns. 2004, 53, 251–255. [Google Scholar] [CrossRef]
- Deepa, M.; Bhansali, A.; Anjana, R.M.; Pradeepa, R.; Joshi, S.R.; Joshi, P.P.; Dhandhania, V.K.; Rao, P.V.; Subashini, R.; Unnikrishnan, R.; et al. Knowledge and awareness of diabetes in urban and rural India: The Indian Council of Medical Research India Diabetes Study (Phase I): Indian Council of Medical Research India Diabetes 4. Indian J. Endocrinol. Metab. 2014, 18, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Mohan, D.; Raj, D.; Shanthirani, C.S.; Datta, M.; Unwin, N.C.; Kapur, A.; Mohan, V. Awareness and knowledge of diabetes in Chennai--the Chennai Urban Rural Epidemiology Study [CURES-9]. J. Assoc. Physicians India 2005, 53, 283–287. [Google Scholar]
- Muninarayana, C.; Balachandra, G.; Hiremath, S.G.; Iyengar, K.; Anil, N.S. Prevalence and awareness regarding diabetes mellitus in rural Tamaka, Kolar. Int. J. Diabetes Dev. Ctries 2010, 30, 18–21. [Google Scholar] [CrossRef]
- Murugesan, N.; Snehalatha, C.; Shobhana, R.; Roglic, G.; Ramachandran, A. Awareness about diabetes and its complications in the general and diabetic population in a city in southern India. Diabetes Res. Clin. Pract. 2007, 77, 433–437. [Google Scholar] [CrossRef]
- Singh, A.; Milton, P.E.; Nanaiah, A.; Samuel, P.; Thomas, N. Awareness and attitude toward diabetes in the rural population of Arunachal Pradesh, Northeast India. Indian J. Endocrinol. Metab. 2012, 16 (Suppl. S1), S83–S86. [Google Scholar] [CrossRef]
- Kurian, B.; Qurieshi, M.; Ganesh, R.; Leelamoni, K. A community-based study on knowledge of diabetes mellitus among adults in a rural population of Kerala. Int. J. Noncommun. Dis. 2016, 1, 59–64. [Google Scholar] [CrossRef]
- Basu, S.; Khobragade, M.; Raut, D.; Garg, S. Knowledge of diabetes among diabetic patients in government hospitals of Delhi. Int. J. Non-Commun. Dis. 2017, 2, 8–10. [Google Scholar] [CrossRef]
- Sathish, T.; Williams, E.D.; Pasricha, N.; Absetz, P.; Lorgelly, P.; Wolfe, R.; Mathews, E.; Aziz, Z.; Thankappan, K.R.; Zimmet, P.; et al. Cluster randomised controlled trial of a peer-led lifestyle intervention program: Study protocol for the Kerala diabetes prevention program. BMC Public Health 2013, 13, 1035. [Google Scholar] [CrossRef] [PubMed]
- Sathish, T.; Aziz, Z.; Absetz, P.; Thankappan, K.R.; Tapp, R.J.; Balachandran, S.; Shetty, S.S.; Oldenburg, B. Participant recruitment into a community-based diabetes prevention trial in India: Learnings from the Kerala Diabetes Prevention Program. Contemp. Clin. Trials. Commun. 2019, 15, 100382. [Google Scholar] [CrossRef]
- Sathish, T.; Shaw, J.E.; Tapp, R.J.; Wolfe, R.; Thankappan, K.R.; Balachandran, S.; Oldenburg, B. Targeted screening for prediabetes and undiagnosed diabetes in a community setting in India. Diabetes Metab. Syndr. 2019, 13, 1785–1790. [Google Scholar] [CrossRef]
- Mohan, V.; Deepa, R.; Deepa, M.; Somannavar, S.; Datta, M. A simplified Indian Diabetes Risk Score for screening for undiagnosed diabetic subjects. J. Assoc. Physicians India 2005, 53, 759–763. [Google Scholar]
- Mohan, V.; Anbalagan, V.P. Expanding role of the Madras Diabetes Research Foundation—Indian Diabetes Risk Score in clinical practice. Indian J. Endocrinol. Metab. 2013, 17, 31–36. [Google Scholar] [CrossRef]
- Mohan, V.; Deepa, M.; Anjana, R.M.; Lanthorn, H.; Deepa, R. Incidence of diabetes and pre-diabetes in a selected urban south Indian population (CUPS-19). J. Assoc. Physicians India 2008, 56, 152–157. [Google Scholar]
- Nag, T.; Ghosh, A. Indian diabetes risk score and clustering of metabolic syndrome phenotype in a rural community of Asian Indian origin. Diabetes Res. Clin. Pract. 2016, 112, 44–49. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Commitee. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45 (Suppl. S1), S17–S38. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Census 2011. Kerala Literacy Rate 2011. Available online: https://www.census2011.co.in/census/state/kerala.html (accessed on 22 November 2022).
- Sathish, T.; Kannan, S.; Sarma, P.S.; Razum, O.; Thankappan, K.R. Incidence of hypertension and its risk factors in rural Kerala, India: A community-based cohort study. Public Health 2012, 126, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Sathish, T.; Kannan, S.; Sarma, S.P.; Razum, O.; Sauzet, O.; Thankappan, K.R. Seven-year longitudinal change in risk factors for non-communicable diseases in rural Kerala, India: The WHO STEPS approach. PLoS ONE 2017, 12, e0178949. [Google Scholar] [CrossRef] [PubMed]
- Sathish, T.; Oldenburg, B.; Tapp, R.J.; Shaw, J.E.; Wolfe, R.; Sajitha, B.; D’Esposito, F.; Absetz, P.; Mathews, E.; Zimmet, P.Z.; et al. Baseline characteristics of participants in the Kerala Diabetes Prevention Program: A cluster randomized controlled trial of lifestyle intervention in Asian Indians. Diabet Med. 2017, 34, 647–653. [Google Scholar] [CrossRef]
- International Institute for Population Sciences (IIPS) and ICF. National Family Health Survey (NFHS-5), 2019–2021: India. Available online: http://rchiips.org/nfhs/NFHS-5Reports/NFHS-5_INDIA_REPORT.pdf (accessed on 9 February 2023).
- Knott, C.; Bell, S.; Britton, A. Alcohol Consumption and the Risk of Type 2 Diabetes: A Systematic Review and Dose-Response Meta-analysis of More than 1.9 Million Individuals from 38 Observational Studies. Diabetes Care 2015, 38, 1804–1812. [Google Scholar] [CrossRef]
- Pan, A.; Wang, Y.; Talaei, M.; Hu, F.B.; Wu, T. Relation of active, passive, and quitting smoking with incident type 2 diabetes: A systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2015, 3, 958–967. [Google Scholar] [CrossRef]
- Fowler, M.J. Microvascular and Macrovascular Complications of Diabetes. Clin. Diabetes 2008, 26, 77–82. [Google Scholar] [CrossRef]
- Crawford, F.; Nicolson, D.J.; Amanna, A.E.; Martin, A.; Gupta, S.; Leese, G.P.; Heggie, R.; Chappell, F.M.; McIntosh, H.H. Preventing foot ulceration in diabetes: Systematic review and meta-analyses of RCT data. Diabetologia 2020, 63, 49–64. [Google Scholar] [CrossRef]
- Sarma, P.S.; Sadanandan, R.; Thulaseedharan, J.V.; Soman, B.; Srinivasan, K.; Varma, R.P.; Nair, M.R.; Pradeepkumar, A.S.; Jeemon, P.; Thankappan, K.R.; et al. Prevalence of risk factors of non-communicable diseases in Kerala, India: Results of a cross-sectional study. BMJ Open 2019, 9, e027880. [Google Scholar] [CrossRef]
- India State-Level Disease Burden Initiative Collaborators. Nations within a nation: Variations in epidemiological transition across the states of India, 1990–2016 in the Global Burden of Disease Study. Lancet 2017, 390, 2437–2460. [Google Scholar] [CrossRef]
- Thankappan, K.R.; Shah, B.; Mathur, P.; Sarma, P.S.; Srinivas, G.; Mini, G.K.; Daivadanam, M.; Soman, B.; Vasan, R.S. Risk factor profile for chronic non-communicable diseases: Results of a community-based study in Kerala, India. Indian J. Med. Res. 2010, 131, 53–63. [Google Scholar] [PubMed]
- India State-Level Disease Burden Initiative Diabetes Collaborators. The increasing burden of diabetes and variations among the states of India: The Global Burden of Disease Study 1990–2016. Lancet Glob. Health 2018, 6, e1352–e1362. [Google Scholar] [CrossRef] [PubMed]
- Anjana, R.M.; Deepa, M.; Pradeepa, R.; Mahanta, J.; Narain, K.; Das, H.K.; Adhikari, P.; Rao, P.V.; Saboo, B.; Kumar, A.; et al. Prevalence of diabetes and prediabetes in 15 states of India: Results from the ICMR-INDIAB population-based cross-sectional study. Lancet Diabetes Endocrinol. 2017, 5, 585–596. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | N = 1007 |
|---|---|
| Age (years), mean (SD) | 46.0 (7.5) |
| Sex, n (%) | |
| Men | 532 (52.8) |
| Women | 475 (47.2) |
| Education, n (%) | |
| Up to primary | 253 (25.1) |
| Above primary to higher secondary school | 653 (64.9) |
| College or above | 101 (10.0) |
| Occupation, n (%) | |
| Skilled/unskilled | 728 (72.3) |
| Homemaker | 268 (26.6) |
| Unemployed/retired | 11 (1.1) |
| Marital status, n (%) | |
| Single | 11 (1.1) |
| Married | 958 (95.1) |
| Divorced/separated/widowed | 38 (3.8) |
| Monthly household expenditure (INR), median (IQR) | 7000 (5000–10,000) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sathish, T.; Thankappan, K.R.; Panniyammakal, J.; Oldenburg, B. Knowledge of Diabetes among Adults at High Risk for Type 2 Diabetes in the Trivandrum District of Kerala, India. Diabetology 2023, 4, 76-85. https://doi.org/10.3390/diabetology4010009
Sathish T, Thankappan KR, Panniyammakal J, Oldenburg B. Knowledge of Diabetes among Adults at High Risk for Type 2 Diabetes in the Trivandrum District of Kerala, India. Diabetology. 2023; 4(1):76-85. https://doi.org/10.3390/diabetology4010009
Chicago/Turabian StyleSathish, Thirunavukkarasu, Kavumpurathu Raman Thankappan, Jeemon Panniyammakal, and Brian Oldenburg. 2023. "Knowledge of Diabetes among Adults at High Risk for Type 2 Diabetes in the Trivandrum District of Kerala, India" Diabetology 4, no. 1: 76-85. https://doi.org/10.3390/diabetology4010009
APA StyleSathish, T., Thankappan, K. R., Panniyammakal, J., & Oldenburg, B. (2023). Knowledge of Diabetes among Adults at High Risk for Type 2 Diabetes in the Trivandrum District of Kerala, India. Diabetology, 4(1), 76-85. https://doi.org/10.3390/diabetology4010009