
Recent Advances in Prostate Cancer (PCa) Diagnostics

 , , ,
, , ,  ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Localized PCa Diagnosis
2.1. Digital Rectal Examination (DRE)
2.2. Transrectal Ultrasound (TRUS)
2.3. Magnetic Resonance Imaging (MRI)
2.4. Computed Tomography (CT)
3. Advanced PCa Diagnosis
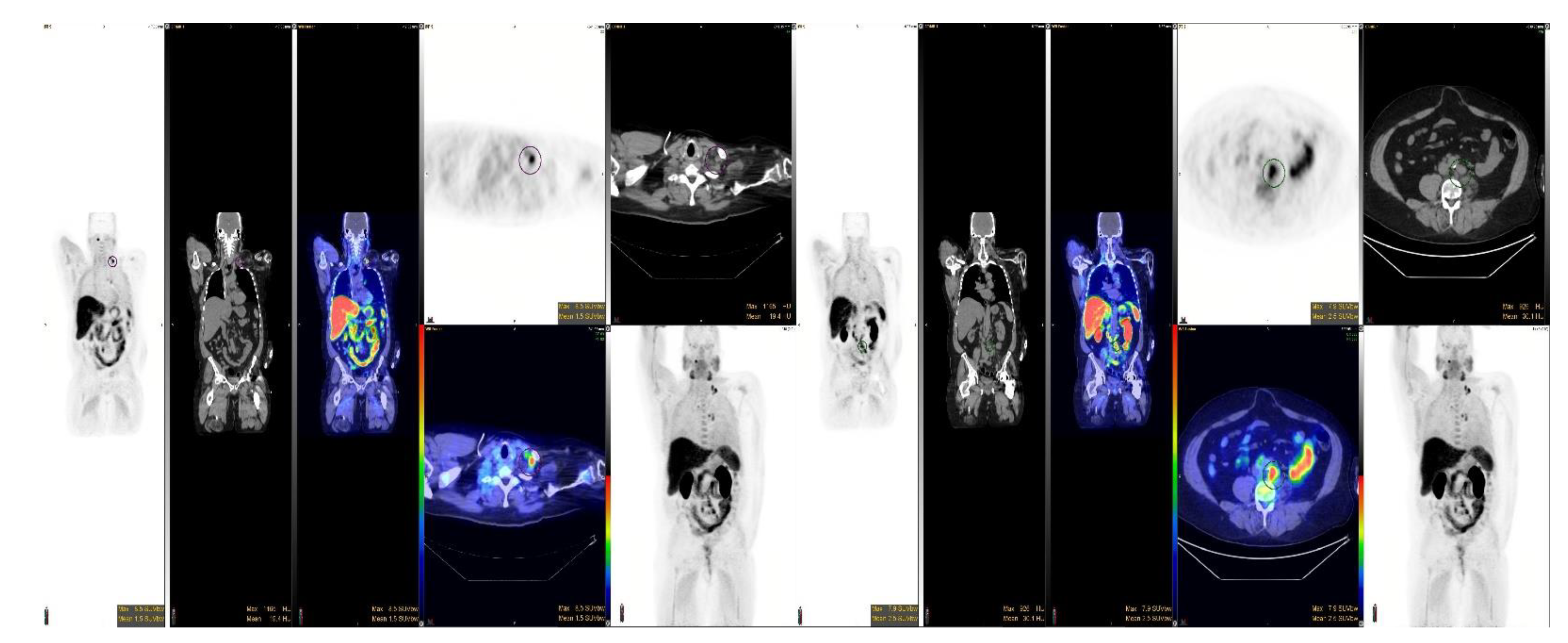
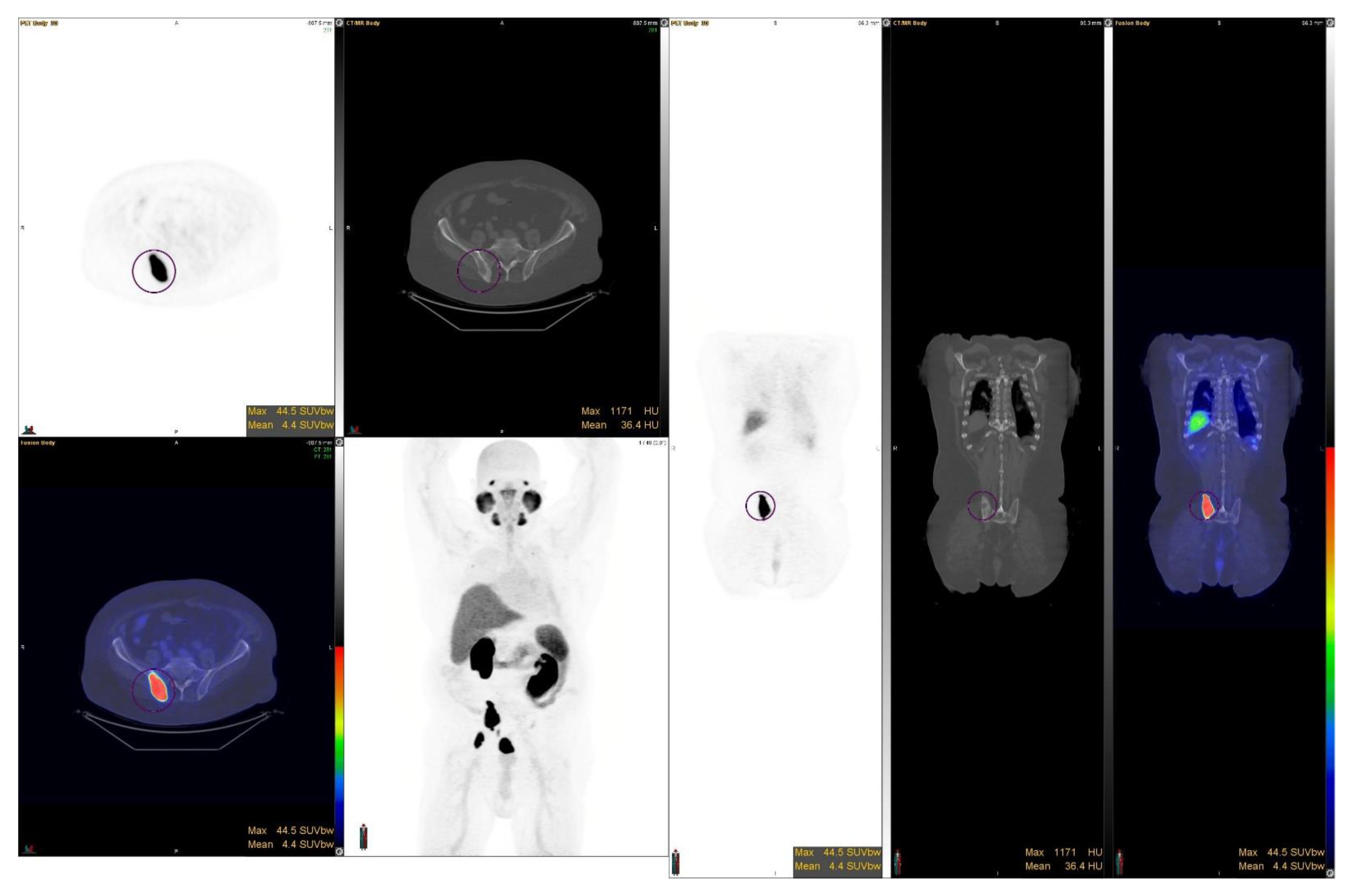
3.1. Positron Emission Tomography (PET)
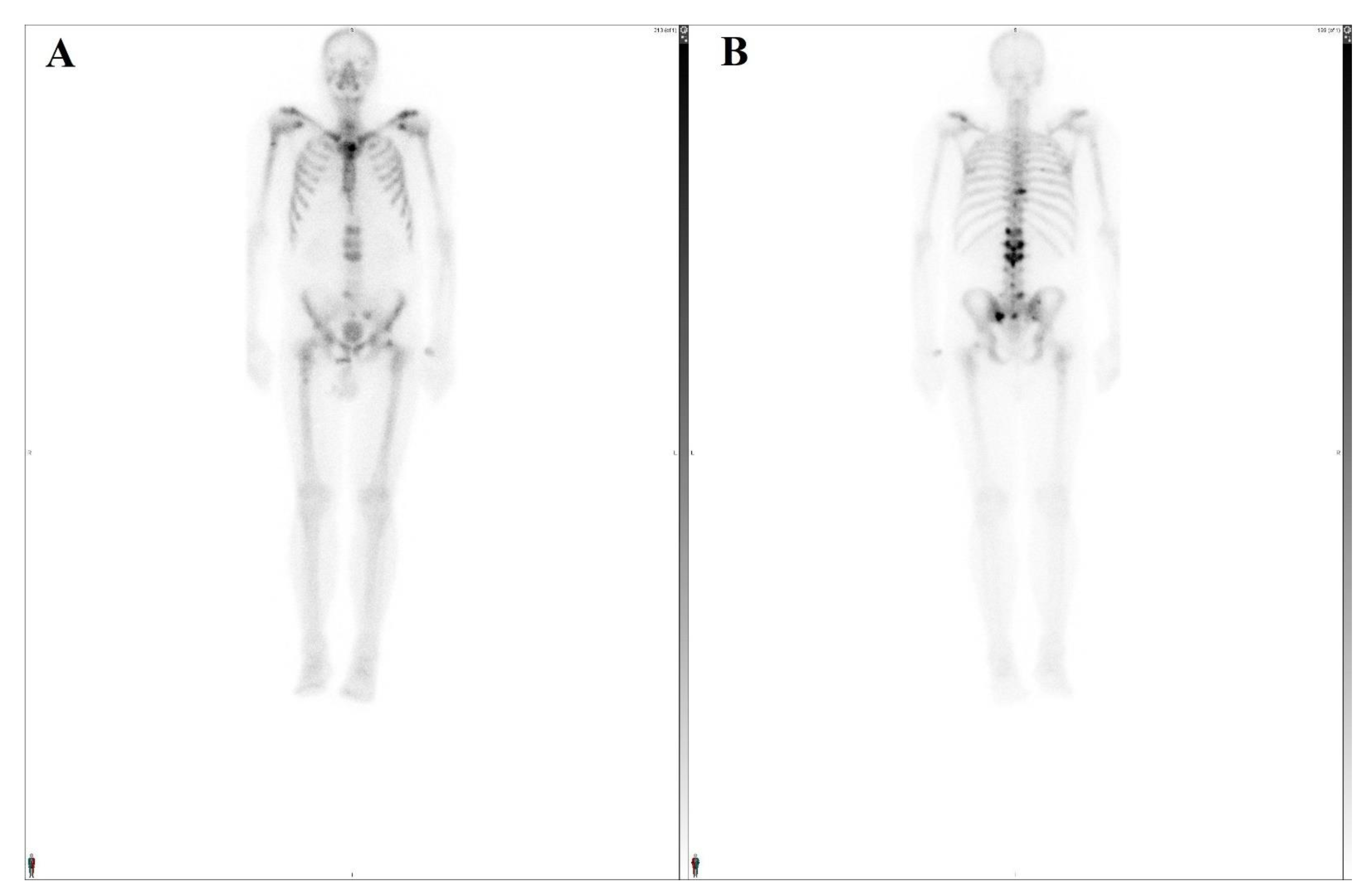
3.2. Bone Scan (BS)
3.3. Conventional CT Imaging
3.4. MRI
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Rawla, P. Epidemiology of Prostate Cancer. World J. Oncol. 2019, 10, 63–89. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31068988 (accessed on 11 April 2022). [CrossRef]
- Jadvar, H.; Alavi, A. Role of Imaging in Prostate Cancer. PET Clin. 2009, 4, 135–138. Available online: http://www.ncbi.nlm.nih.gov/pubmed/20161047 (accessed on 11 April 2022). [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. Available online: http://www.ncbi.nlm.nih.gov/pubmed/33433946. (accessed on 11 April 2022). [CrossRef]
- Giri, V.N.; Morgan, T.M.; Morris, D.S.; Berchuck, J.E.; Hyatt, C.; Taplin, M.-E. Genetic testing in prostate cancer management: Considerations informing primary care. CA Cancer J. Clin. 2022. online ahead of print. Available online: http://www.ncbi.nlm.nih.gov/pubmed/35201622 (accessed on 11 April 2022). [CrossRef]
- Desai, M.M.; Cacciamani, G.E.; Gill, K.; Zhang, J.; Liu, L.; Abreu, A.; Gill, I.S. Trends in Incidence of Metastatic Prostate Cancer in the US. JAMA Netw. Open 2022, 5, e222246. Available online: http://www.ncbi.nlm.nih.gov/pubmed/35285916 (accessed on 11 April 2022). [CrossRef]
- Cuzick, J.; Thorat, M.A.; Andriole, G.; Brawley, O.W.; Brown, P.H.; Culig, Z.; Eeles, R.A.; Ford, L.G.; Hamdy, F.C.; Holmberg, L.; et al. Prevention and early detection of prostate cancer. Lancet Oncol. 2014, 15, e484-92. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25281467 (accessed on 11 April 2022). [CrossRef]
- Turkbey, B.; Albert, P.S.; Kurdziel, K.; Choyke, P.L. Imaging localized prostate cancer: Current approaches and new developments. AJR. Am. J. Roentgenol. 2009, 192, 1471–1480. Available online: http://www.ncbi.nlm.nih.gov/pubmed/19457807 (accessed on 11 April 2022). [CrossRef]
- Ghafoor, S.; Burger, I.A.; Vargas, A.H. Multimodality Imaging of Prostate Cancer. J. Nucl. Med. 2019, 60, 1350–1358. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31481573 (accessed on 11 April 2022). [CrossRef]
- Soares, S.C.M.; de Camargo Cancela, M.; Migowski, A.; de Souza, D.L.B. Digital rectal examination and its associated factors in the early detection of prostate cancer: A cross-sectional population-based study. BMC Public Health 2019, 19, 1573. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31775710 (accessed on 11 April 2022). [CrossRef]
- Naji, L.; Randhawa, H.; Sohani, Z.; Dennis, B.; Lautenbach, D.; Kavanagh, O.; Bawor, M.; Banfield, L.; Profetto, J. Digital Rectal Examination for Prostate Cancer Screening in Primary Care: A Systematic Review and Meta-Analysis. Ann. Fam. Med. 2018, 16, 149–154. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29531107 (accessed on 11 April 2022). [CrossRef]
- Izawa, J.I.; Klotz, L.; Siemens, D.R.; Kassouf, W.; So, A.; Jordan, J.; Chetner, M.; Iansavichene, A.E. Prostate cancer screening: Canadian guidelines 2011. Can. Urol. Assoc. J. 2011, 5, 235–240. Available online: http://www.ncbi.nlm.nih.gov/pubmed/21801679 (accessed on 11 April 2022). [CrossRef]
- Koulikov, D.; Mamber, A.; Fridmans, A.; Abu Arafeh, W.; Shenfeld, O.Z. Why I cannot find the prostate? Behind the subjectivity of rectal exam. ISRN Urol. 2012, 2012, 456821. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22530153 (accessed on 11 April 2022). [CrossRef]
- Zhang, A.; Fear, T.; Ahmed, H. Digital rectal examination in prostate cancer screening. Univ. West. Ont. Med. J. 2013, 82, 10–11. Available online: https://ojs.lib.uwo.ca/index.php/uwomj/article/view/4626 (accessed on 11 April 2022). [CrossRef]
- Kawachi, M.H.; Bahnson, R.R.; Barry, M.; Busby, J.E.; Carroll, P.R.; Carter, H.B.; Catalona, W.J.; Cookson, M.S.; Epstein, J.I.; Etzioni, R.B.; et al. NCCN clinical practice guidelines in oncology: Prostate cancer early detection. J. Natl. Compr. Cancer Netw. 2010, 8, 240–262. Available online: http://www.ncbi.nlm.nih.gov/pubmed/20141680 (accessed on 11 April 2022). [CrossRef]
- Adhyam, M.; Gupta, A.K. A Review on the Clinical Utility of PSA in Cancer Prostate. Indian J. Surg. Oncol. 2012, 3, 120–129. Available online: http://www.ncbi.nlm.nih.gov/pubmed/23730101 (accessed on 11 April 2022). [CrossRef]
- Miller, D.C.; Hafez, K.S.; Stewart, A.; Montie, J.E.; Wei, J.T. Prostate carcinoma presentation, diagnosis, and staging: An update form the National Cancer Data Base. Cancer 2003, 98, 1169–1178. Available online: http://www.ncbi.nlm.nih.gov/pubmed/12973840 (accessed on 11 April 2022). [CrossRef]
- Richie, J.P.; Catalona, W.J.; Ahmann, F.R.; Hudson, M.A.; Scardino, P.T.; Flanigan, R.C.; DeKernion, J.B.; Ratliff, T.L.; Kavoussi, L.R.; Dalkin, B.L.; et al. Effect of patient age on early detection of prostate cancer with serum prostate-specific antigen and digital rectal examination. Urology 1993, 42, 365–374. Available online: http://www.ncbi.nlm.nih.gov/pubmed/7692657 (accessed on 11 April 2022). [CrossRef]
- Catalona, W.J.; Richie, J.P.; Ahmann, F.R.; Hudson, M.A.; Scardino, P.T.; Flanigan, R.C.; DeKernion, J.B.; Ratliff, T.L.; Kavoussi, L.R.; Dalkin, B.L.; et al. Comparison of Digital Rectal Examination and Serum Prostate Specific Antigen in the Early Detection of Prostate Cancer: Results of a Multicenter Clinical Trial of 6630 Men. J. Urol. 2017, 197, S200–S207. Available online: http://www.ncbi.nlm.nih.gov/pubmed/28012755 (accessed on 11 April 2022). [CrossRef]
- Anastasi, G.; Subba, E.; Pappalardo, R.; Macchione, L.; Ricotta, G.; Muscarà, G.; Lembo, F.; Magno, C. Transrectal ultrasound (TRUS) guided prostate biopsy: Three different types of local anesthesia. Arch. Ital. Urol. Androl. 2016, 88, 308–310. Available online: http://www.ncbi.nlm.nih.gov/pubmed/28073199 (accessed on 11 April 2022). [CrossRef]
- Dähnert, W.F.; Hamper, U.M.; Eggleston, J.C.; Walsh, P.C.; Sanders, R.C. Prostatic evaluation by transrectal sonography with histopathologic correlation: The echopenic appearance of early carcinoma. Radiology 1986, 158, 97–102. Available online: http://www.ncbi.nlm.nih.gov/pubmed/3510032 (accessed on 11 April 2022). [CrossRef]
- Brock, M.; von Bodman, C.; Sommerer, F.; Löppenberg, B.; Klein, T.; Deix, T.; Palisaar, J.R.; Noldus, J.; Eggert, T. Comparison of real-time elastography with grey-scale ultrasonography for detection of organ-confined prostate cancer and extra capsular extension: A prospective analysis using whole mount sections after radical prostatectomy. BJU Int. 2011, 108 Pt 2, E217–E222. Available online: http://www.ncbi.nlm.nih.gov/pubmed/21819532 (accessed on 11 April 2022). [CrossRef]
- Trevethan, R. Sensitivity, Specificity, and Predictive Values: Foundations, Pliabilities, and Pitfalls in Research and Practice. Front. Public Health 2017, 5, 307. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29209603 (accessed on 11 April 2022). [CrossRef]
- Pummer, K.; Rieken, M.; Augustin, H.; Gutschi, T.; Shariat, S.F. Innovations in diagnostic imaging of localized prostate cancer. World J. Urol. 2014, 32, 881–890. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24078105 (accessed on 11 April 2022). [CrossRef]
- Wildeboer, R.R.; Postema, A.W.; Demi, L.; Kuenen, M.P.J.; Wijkstra, H.; Mischi, M. Multiparametric dynamic contrast-enhanced ultrasound imaging of prostate cancer. Eur. Radiol. 2017, 27, 3226–3234. Available online: http://www.ncbi.nlm.nih.gov/pubmed/28004162 (accessed on 11 April 2022). [CrossRef]
- Carpagnano, F.A.; Eusebi, L.; Carriero, S.; Giannubilo, W.; Bartelli, F.; Guglielmi, G. Prostate Cancer Ultrasound: Is Still a Valid Tool? Curr. Radiol. Rep. 2021, 9, 7. Available online: https://link.springer.com/10.1007/s40134-021-00382-6 (accessed on 11 April 2022). [CrossRef]
- Mitterberger, M.J.; Aigner, F.; Horninger, W.; Ulmer, H.; Cavuto, S.; Halpern, E.J.; Frauscher, F. Comparative efficiency of contrast-enhanced colour Doppler ultrasound targeted versus systematic biopsy for prostate cancer detection. Eur. Radiol. 2010, 20, 2791–2796. Available online: http://www.ncbi.nlm.nih.gov/pubmed/20571801 (accessed on 11 April 2022). [CrossRef]
- Halpern, E.J. Contrast-enhanced ultrasound imaging of prostate cancer. Rev. Urol. 2006, 8 (Suppl. 1), S29–S37. Available online: http://www.ncbi.nlm.nih.gov/pubmed/17021624 (accessed on 11 April 2022).
- Taverna, G.; Morandi, G.; Seveso, M.; Giusti, G.; Benetti, A.; Colombo, P.; Minuti, F.; Grizzi, F.; Graziotti, P. Colour Doppler and microbubble contrast agent ultrasonography do not improve cancer detection rate in transrectal systematic prostate biopsy sampling. BJU Int. 2011, 108, 1723–1727. Available online: http://www.ncbi.nlm.nih.gov/pubmed/21756276 (accessed on 11 April 2022). [CrossRef]
- Loch, T. Computerized transrectal ultrasound (C-TRUS) of the prostate: Detection of cancer in patients with multiple negative systematic random biopsies. World J. Urol. 2007, 25, 375–380. Available online: http://www.ncbi.nlm.nih.gov/pubmed/17694312 (accessed on 11 April 2022). [CrossRef]
- van der Aa, A.A.M.A.; Mannaerts, C.K.; Gayet, M.C.W.; van der Linden, J.C.; Schrier, B.P.; Sedelaar, J.P.M.; Mischi, M.; Beerlage, H.P.; Wijkstra, H. Three-dimensional greyscale transrectal ultrasound-guidance and biopsy core preembedding for detection of prostate cancer: Dutch clinical cohort study. BMC Urol. 2019, 19, 23. Available online: https://bmcurol.biomedcentral.com/articles/10.1186/s12894-019-0455-7 (accessed on 11 April 2022). [CrossRef]
- Walz, J.; Loch, T.; Salomon, G.; Wijkstra, H. Imaging of the prostate. Die Urol. 2013, 52, 490–496. Available online: http://www.ncbi.nlm.nih.gov/pubmed/23494334 (accessed on 11 April 2022).
- Strunk, T.; Decker, G.; Willinek, W.; Mueller, S.C.; Rogenhofer, S. Combination of C-TRUS with multiparametric MRI: Potential for improving detection of prostate cancer. World J. Urol. 2014, 32, 335–339. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22885659 (accessed on 11 April 2022). [CrossRef]
- Brock, M.; Eggert, T.; Palisaar, R.J.; Roghmann, F.; Braun, K.; Löppenberg, B.; Sommerer, F.; Noldus, J.; von Bodman, C. Multiparametric ultrasound of the prostate: Adding contrast enhanced ultrasound to real-time elastography to detect histopathologically confirmed cancer. J. Urol. 2013, 189, 93–98. Available online: http://www.ncbi.nlm.nih.gov/pubmed/23164379 (accessed on 11 April 2022). [CrossRef]
- Sigrist, R.M.S.; Liau, J.; El Kaffas, A.; Chammas, M.C.; Willmann, J.K. Ultrasound Elastography: Review of Techniques and Clinical Applications. Theranostics 2017, 7, 1303–1329. Available online: http://www.ncbi.nlm.nih.gov/pubmed/28435467 (accessed on 11 April 2022). [CrossRef] [PubMed]
- Zhu, Y.; Chen, Y.; Qi, T.; Jiang, J.; Qi, J.; Yu, Y.; Yao, X.; Guan, W. Prostate cancer detection with real-time elastography using a bi-plane transducer: Comparison with step section radical prostatectomy pathology. World J. Urol. 2014, 32, 329–333. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22885658 (accessed on 11 April 2022). [CrossRef]
- Yuan, J.; Poon, D.M.C.; Lo, G.; Wong, O.L.; Cheung, K.Y.; Yu, S.K. A narrative review of MRI acquisition for MR-guided-radiotherapy in prostate cancer. Quant. Imaging Med. Surg. 2022, 12, 1585–1607. Available online: http://www.ncbi.nlm.nih.gov/pubmed/35111651 (accessed on 11 April 2022). [CrossRef]
- Hambrock, T.; Somford, D.M.; Hoeks, C.; Bouwense, S.A.W.; Huisman, H.; Yakar, D.; van Oort, I.M.; Witjes, J.A.; Fütterer, J.J.; Barentsz, J.O. Magnetic resonance imaging guided prostate biopsy in men with repeat negative biopsies and increased prostate specific antigen. J. Urol. 2010, 183, 520–527. Available online: http://www.ncbi.nlm.nih.gov/pubmed/20006859 (accessed on 11 April 2022). [CrossRef]
- Choi, M.S.; Choi, Y.S.; Yoon, B.I.; Kim, S.J.; Cho, H.J.; Hong, S.H.; Lee, J.Y.; Hwang, T.-K.; Kim, S.W. The Clinical Value of Performing an MRI before Prostate Biopsy. Korean J. Urol. 2011, 52, 572–577. Available online: http://www.ncbi.nlm.nih.gov/pubmed/21927706 (accessed on 11 April 2022). [CrossRef]
- Laurence Klotz, C.M. Can high resolution micro-ultrasound replace MRI in the diagnosis of prostate cancer? Eur. Urol. Focus 2020, 6, 419–423. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31771935 (accessed on 11 April 2022). [CrossRef]
- Schoots, I.G.; Padhani, A.R. Delivering Clinical impacts of the MRI diagnostic pathway in prostate cancer diagnosis. Abdom. Radiol. (N. Y.) 2020, 45, 4012–4022. Available online: http://www.ncbi.nlm.nih.gov/pubmed/32356003 (accessed on 11 April 2022). [CrossRef]
- Available online: https://www.ncbi.nlm.nih.gov/books/NBK544759/?report=reader (accessed on 11 April 2022).
- Bjurlin, M.A.; Carroll, P.R.; Eggener, S.; Fulgham, P.F.; Margolis, D.J.; Pinto, P.A.; Rosenkrantz, A.B.; Rubenstein, J.N.; Rukstalis, D.B.; Taneja, S.S.; et al. Update of the Standard Operating Procedure on the Use of Multiparametric Magnetic Resonance Imaging for the Diagnosis, Staging and Management of Prostate Cancer. J. Urol. 2020, 203, 706–712. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31642740 (accessed on 11 April 2022). [CrossRef] [PubMed]
- Siddiqui, M.M.; Rais-Bahrami, S.; Turkbey, B.; George, A.K.; Rothwax, J.; Shakir, N.; Okoro, C.; Raskolnikov, D.; Parnes, H.L.; Linehan, W.M.; et al. Comparison of MR/ultrasound fusion-guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer. JAMA 2015, 313, 390–397. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25626035 (accessed on 11 April 2022). [CrossRef] [PubMed]
- Penzkofer, T.; Tuncali, K.; Fedorov, A.; Song, S.-E.; Tokuda, J.; Fennessy, F.M.; Vangel, M.G.; Kibel, A.S.; Mulkern, R.V.; Wells, W.M.; et al. Transperineal in-bore 3-T MR imaging-guided prostate biopsy: A prospective clinical observational study. Radiology 2015, 274, 170–180. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25222067 (accessed on 11 April 2022). [CrossRef] [PubMed]
- Moore, C.M.; Robertson, N.L.; Arsanious, N.; Middleton, T.; Villers, A.; Klotz, L.; Taneja, S.S.; Emberton, M. Image-guided prostate biopsy using magnetic resonance imaging-derived targets: A systematic review. Eur. Urol. 2013, 63, 125–140. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22743165 (accessed on 16 April 2022). [CrossRef] [PubMed]
- Wegelin, O.; van Melick, H.H.E.; Hooft, L.; Bosch, J.L.H.R.; Reitsma, H.B.; Barentsz, J.O.; Somford, D.M. Comparing Three Different Techniques for Magnetic Resonance Imaging-targeted Prostate Biopsies: A Systematic Review of In-bore versus Magnetic Resonance Imaging-transrectal Ultrasound fusion versus Cognitive Registration. Is There a Preferred Technique? Eur. Urol. 2017, 71, 517–531. Available online: http://www.ncbi.nlm.nih.gov/pubmed/27568655 (accessed on 16 April 2022). [CrossRef]
- Drost, F.-J.H.; Osses, D.F.; Nieboer, D.; Steyerberg, E.W.; Bangma, C.H.; Roobol, M.J.; Schoots, I.G. Prostate MRI, with or without MRI-targeted biopsy, and systematic biopsy for detecting prostate cancer. Cochrane Database Syst. Rev. 2019, 4, CD012663. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31022301 (accessed on 16 April 2022). [CrossRef]
- Hövels, A.M.; Heesakkers, R.A.M.; Adang, E.M.; Jager, G.J.; Strum, S.; Hoogeveen, Y.L.; Severens, J.L.; Barentsz, J.O. The diagnostic accuracy of CT and MRI in the staging of pelvic lymph nodes in patients with prostate cancer: A meta-analysis. Clin. Radiol. 2008, 63, 387–395. Available online: http://www.ncbi.nlm.nih.gov/pubmed/18325358 (accessed on 16 April 2022). [CrossRef]
- Korevaar, S.; Tennakoon, R.; Page, M.; Brotchie, P.; Thangarajah, J.; Florescu, C.; Sutherland, T.; Kam, N.M.; Bab-Hadiashar, A. Incidental detection of prostate cancer with computed tomography scans. Sci. Rep. 2021, 11, 7956. Available online: http://www.ncbi.nlm.nih.gov/pubmed/33846450 (accessed on 16 April 2022). [CrossRef]
- Rowe, S.P.; Gorin, M.A.; Allaf, M.E.; Pienta, K.J.; Tran, P.T.; Pomper, M.G.; Ross, A.E.; Cho, S.Y. PET imaging of prostate-specific membrane antigen in prostate cancer: Current state of the art and future challenges. Prostate Cancer Prostatic Dis. 2016, 19, 223–230. Available online: http://www.ncbi.nlm.nih.gov/pubmed/27136743 (accessed on 16 April 2022). [CrossRef]
- Wang, R.; Shen, G.; Huang, M.; Tian, R. The Diagnostic Role of 18F-Choline, 18F-Fluciclovine and 18F-PSMA PET/CT in the Detection of Prostate Cancer With Biochemical Recurrence: A Meta-Analysis. Front. Oncol. 2021, 11, 684629. Available online: http://www.ncbi.nlm.nih.gov/pubmed/34222008 (accessed on 16 April 2022). [CrossRef]
- Liu, Y. Diagnostic role of fluorodeoxyglucose positron emission tomography-computed tomography in prostate cancer. Oncol. Lett. 2014, 7, 2013–2018. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24932281 (accessed on 16 April 2022). [CrossRef] [PubMed][Green Version]
- Wallitt, K.L.; Khan, S.R.; Dubash, S.; Tam, H.H.; Khan, S.; Barwick, T.D. Clinical PET Imaging in Prostate Cancer. Radiographics 2017, 37, 1512–1536. Available online: http://www.ncbi.nlm.nih.gov/pubmed/28800286 (accessed on 16 April 2022). [CrossRef]
- Chang, C.-H.; Wu, H.-C.; Tsai, J.J.P.; Shen, Y.-Y.; Changlai, S.-P.; Kao, A. Detecting metastatic pelvic lymph nodes by 18F-2-deoxyglucose positron emission tomography in patients with prostate-specific antigen relapse after treatment for localized prostate cancer. Urol. Int. 2003, 70, 311–315. Available online: http://www.ncbi.nlm.nih.gov/pubmed/12740497 (accessed on 16 April 2022). [CrossRef]
- Jadvar, H.; Desai, B.; Ji, L.; Conti, P.S.; Dorff, T.B.; Groshen, S.G.; Gross, M.E.; Pinski, J.K.; Quinn, D.I. Prospective evaluation of 18F-NaF and 18F-FDG PET/CT in detection of occult metastatic disease in biochemical recurrence of prostate cancer. Clin. Nucl. Med. 2012, 37, 637–643. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22691503 (accessed on 16 April 2022). [CrossRef] [PubMed]
- von Eyben, F.E.; Kairemo, K. Meta-analysis of (11)C-choline and (18)F-choline PET/CT for management of patients with prostate cancer. Nucl. Med. Commun. 2014, 35, 221–230. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24240194 (accessed on 16 April 2022). [CrossRef] [PubMed]
- Evangelista, L.; Guttilla, A.; Zattoni, F.; Muzzio, P.C.; Zattoni, F. Utility of choline positron emission tomography/computed tomography for lymph node involvement identification in intermediate- to high-risk prostate cancer: A systematic literature review and meta-analysis. Eur. Urol. 2013, 63, 1040–1048. Available online: http://www.ncbi.nlm.nih.gov/pubmed/23036576 (accessed on 16 April 2022). [CrossRef] [PubMed]
- Fanti, S.; Minozzi, S.; Castellucci, P.; Balduzzi, S.; Herrmann, K.; Krause, B.J.; Oyen, W.; Chiti, A. PET/CT with (11)C-choline for evaluation of prostate cancer patients with biochemical recurrence: Meta-analysis and critical review of available data. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 55–69. Available online: http://www.ncbi.nlm.nih.gov/pubmed/26450693 (accessed on 16 April 2022). [CrossRef]
- Evangelista, L.; Zattoni, F.; Guttilla, A.; Saladini, G.; Zattoni, F.; Colletti, P.M.; Rubello, D. Choline PET or PET/CT and biochemical relapse of prostate cancer: A systematic review and meta-analysis. Clin. Nucl. Med. 2013, 38, 305–314. Available online: http://www.ncbi.nlm.nih.gov/pubmed/23486334 (accessed on 16 April 2022). [CrossRef]
- Graziani, T.; Ceci, F.; Castellucci, P.; Polverari, G.; Lima, G.M.; Lodi, F.; Morganti, A.G.; Ardizzoni, A.; Schiavina, R.; Fanti, S. (11)C-Choline PET/CT for restaging prostate cancer. Results from 4426 scans in a single-centre patient series. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1971–1979. Available online: http://www.ncbi.nlm.nih.gov/pubmed/27277279 (accessed on 16 April 2022). [CrossRef]
- Jones, W.; Griffiths, K.; Barata, P.C.; Paller, C.J. PSMA Theranostics: Review of the Current Status of PSMA-Targeted Imaging and Radioligand Therapy. Cancers 2020, 12, 1367. Available online: http://www.ncbi.nlm.nih.gov/pubmed/32466595 (accessed on 16 April 2022). [CrossRef]
- Ferraro, D.A.; Garcia Schüler, H.I.; Muehlematter, U.J.; Eberli, D.; Müller, J.; Müller, A.; Gablinger, R.; Kranzbühler, H.; Omlin, A.; Kaufmann, P.A.; et al. Impact of 68Ga-PSMA-11 PET staging on clinical decision-making in patients with intermediate or high-risk prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 652–664. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31802175 (accessed on 16 April 2022). [CrossRef]
- Luiting, H.B.; van Leeuwen, P.J.; Busstra, M.B.; Brabander, T.; van der Poel, H.G.; Donswijk, M.L.; Vis, A.N.; Emmett, L.; Stricker, P.D.; Roobol, M.J. Use of gallium-68 prostate-specific membrane antigen positron-emission tomography for detecting lymph node metastases in primary and recurrent prostate cancer and location of recurrence after radical prostatectomy: An overview of the current literature. BJU Int. 2020, 125, 206–214. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31680398 (accessed on 16 April 2022). [CrossRef]
- Maurer, T.; Eiber, M.; Schwaiger, M.; Gschwend, J.E. Current use of PSMA-PET in prostate cancer management. Nat. Rev. Urol. 2016, 13, 226–235. Available online: http://www.ncbi.nlm.nih.gov/pubmed/26902337 (accessed on 16 April 2022). [CrossRef]
- Razik, A.; Das, C.J.; Sharma, S. PET-CT and PET-MR in urological cancers other than prostate cancer: An update on state of the art. Indian J. Urol. 2018, 34, 20–27. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29343908 (accessed on 16 April 2022).
- Eiber, M.; Maurer, T.; Souvatzoglou, M.; Beer, A.J.; Ruffani, A.; Haller, B.; Graner, F.-P.; Kübler, H.; Haberkorn, U.; Eisenhut, M.; et al. Evaluation of Hybrid 68Ga-PSMA Ligand PET/CT in 248 Patients with Biochemical Recurrence After Radical Prostatectomy. J. Nucl. Med. 2015, 56, 668–674. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25791990 (accessed on 16 April 2022). [CrossRef]
- Einspieler, I.; Rauscher, I.; Düwel, C.; Krönke, M.; Rischpler, C.; Habl, G.; Dewes, S.; Ott, A.; Wester, H.-J.; Schwaiger, M.; et al. Detection Efficacy of Hybrid 68Ga-PSMA Ligand PET/CT in Prostate Cancer Patients with Biochemical Recurrence After Primary Radiation Therapy Defined by Phoenix Criteria. J. Nucl. Med. 2017, 58, 1081–1087. Available online: http://www.ncbi.nlm.nih.gov/pubmed/28209912 (accessed on 16 April 2022). [CrossRef]
- Pan, K.-H.; Wang, J.-F.; Wang, C.-Y.; Nikzad, A.A.; Kong, F.Q.; Jian, L.; Zhang, Y.-Q.; Lu, X.-M.; Xu, B.; Wang, Y.-L.; et al. Evaluation of 18F-DCFPyL PSMA PET/CT for Prostate Cancer: A Meta-Analysis. Front. Oncol. 2020, 10, 597422. Available online: http://www.ncbi.nlm.nih.gov/pubmed/33680924 (accessed on 16 April 2022). [CrossRef]
- Hartrampf, P.E.; Petritsch, B.; Buck, A.K.; Serfling, S.E. Pitfalls in PSMA-PET/CT: Intensive bone marrow uptake in a case with polycythemia vera. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1669–1670. Available online: http://www.ncbi.nlm.nih.gov/pubmed/33111182 (accessed on 16 April 2022). [CrossRef]
- Cantiello, F.; Gangemi, V.; Cascini, G.L.; Calabria, F.; Moschini, M.; Ferro, M.; Musi, G.; Butticè, S.; Salonia, A.; Briganti, A.; et al. Diagnostic Accuracy of 64Copper Prostate-specific Membrane Antigen Positron Emission Tomography/Computed Tomography for Primary Lymph Node Staging of Intermediate- to High-risk Prostate Cancer: Our Preliminary Experience. Urology 2017, 106, 139–145. Available online: http://www.ncbi.nlm.nih.gov/pubmed/28438628 (accessed on 16 April 2022). [CrossRef]
- Shen, G.; Deng, H.; Hu, S.; Jia, Z. Comparison of choline-PET/CT, MRI, SPECT, and bone scintigraphy in the diagnosis of bone metastases in patients with prostate cancer: A meta-analysis. Skelet. Radiol. 2014, 43, 1503–1513. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24841276 (accessed on 16 April 2022). [CrossRef]
- Beheshti, M.; Langsteger, W.; Fogelman, I. Prostate cancer: Role of SPECT and PET in imaging bone metastases. Semin. Nucl. Med. 2009, 39, 396–407. Available online: http://www.ncbi.nlm.nih.gov/pubmed/19801219 (accessed on 16 April 2022). [CrossRef] [PubMed]
- O’Sullivan, J.M.; Norman, A.R.; Cook, G.J.; Fisher, C.; Dearnaley, D.P. Broadening the criteria for avoiding staging bone scans in prostate cancer: A retrospective study of patients at the Royal Marsden Hospital. BJU Int. 2003, 92, 685–689. Available online: http://www.ncbi.nlm.nih.gov/pubmed/14616446 (accessed on 16 April 2022). [CrossRef] [PubMed]
- Lin, K.; Szabo, Z.; Chin, B.B.; Civelek, A.C. The value of a baseline bone scan in patients with newly diagnosed prostate cancer. Clin. Nucl. Med. 1999, 24, 579–582. Available online: http://www.ncbi.nlm.nih.gov/pubmed/10439178 (accessed on 16 April 2022). [CrossRef]
- Abuzallouf, S.; Dayes, I.; Lukka, H. Baseline staging of newly diagnosed prostate cancer: A summary of the literature. J. Urol. 2004, 171 Pt 1, 2122–2127. Available online: http://www.ncbi.nlm.nih.gov/pubmed/15126770 (accessed on 16 April 2022). [CrossRef] [PubMed]
- Harisinghani, M.G.; Barentsz, J.; Hahn, P.F.; Deserno, W.M.; Tabatabaei, S.; van de Kaa, C.H.; de la Rosette, J.; Weissleder, R. Noninvasive detection of clinically occult lymph-node metastases in prostate cancer. N. Engl. J. Med. 2003, 348, 2491–2499. Available online: http://www.ncbi.nlm.nih.gov/pubmed/12815134 (accessed on 16 April 2022). [CrossRef]
- Perez-Lopez, R.; Tunariu, N.; Padhani, A.R.; Oyen, W.J.G.; Fanti, S.; Vargas, H.A.; Omlin, A.; Morris, M.J.; de Bono, J.; Koh, D.-M. Imaging Diagnosis and Follow-up of Advanced Prostate Cancer: Clinical Perspectives and State of the Art. Radiology 2019, 292, 273–286. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31237493 (accessed on 16 April 2022). [CrossRef]
- Westphalen, A.C.; Reed, G.D.; Vinh, P.P.; Sotto, C.; Vigneron, D.B.; Kurhanewicz, J. Multiparametric 3T endorectal mri after external beam radiation therapy for prostate cancer. J. Magn. Reson. Imaging 2012, 36, 430–437. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22535708 (accessed on 16 April 2022). [CrossRef]
- Pucar, D.; Shukla-Dave, A.; Hricak, H.; Moskowitz, C.S.; Kuroiwa, K.; Olgac, S.; Ebora, L.E.; Scardino, P.T.; Koutcher, J.A.; Zakian, K.L. Prostate cancer: Correlation of MR imaging and MR spectroscopy with pathologic findings after radiation therapy-initial experience. Radiology 2005, 236, 545–553. Available online: http://www.ncbi.nlm.nih.gov/pubmed/15972335 (accessed on 16 April 2022). [CrossRef]
- Thoeny, H.C.; Froehlich, J.M.; Triantafyllou, M.; Huesler, J.; Bains, L.J.; Vermathen, P.; Fleischmann, A.; Studer, U.E. Metastases in normal-sized pelvic lymph nodes: Detection with diffusion-weighted MR imaging. Radiology 2014, 273, 125–135. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24893049 (accessed on 16 April 2022). [CrossRef]
- Woo, S.; Suh, C.H.; Kim, S.Y.; Cho, J.Y.; Kim, S.H. The Diagnostic Performance of MRI for Detection of Lymph Node Metastasis in Bladder and Prostate Cancer: An Updated Systematic Review and Diagnostic Meta-Analysis. Am. J. Roentgenol. 2018, 210, W95–W109. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29381380 (accessed on 16 April 2022). [CrossRef]
- Birkhäuser, F.D.; Studer, U.E.; Froehlich, J.M.; Triantafyllou, M.; Bains, L.J.; Petralia, G.; Vermathen, P.; Fleischmann, A.; Thoeny, H.C. Combined ultrasmall superparamagnetic particles of iron oxide-enhanced and diffusion-weighted magnetic resonance imaging facilitates detection of metastases in normal-sized pelvic lymph nodes of patients with bladder and prostate cancer. Eur. Urol. 2013, 64, 953–960. Available online: http://www.ncbi.nlm.nih.gov/pubmed/23916692 (accessed on 16 April 2022). [CrossRef] [PubMed]
- Pasoglou, V.; Larbi, A.; Collette, L.; Annet, L.; Jamar, F.; Machiels, J.-P.; Michoux, N.; Vande Berg, B.C.; Tombal, B.; Lecouvet, F.E. One-step TNM staging of high-risk prostate cancer using magnetic resonance imaging (MRI): Toward an upfront simplified “all-in-one” imaging approach? Prostate 2014, 74, 469–477. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24375774 (accessed on 16 April 2022). [CrossRef] [PubMed]
- Padhani, A.R.; Lecouvet, F.E.; Tunariu, N.; Koh, D.-M.; De Keyzer, F.; Collins, D.J.; Sala, E.; Schlemmer, H.P.; Petralia, G.; Vargas, H.A.; et al. METastasis Reporting and Data System for Prostate Cancer: Practical Guidelines for Acquisition, Interpretation, and Reporting of Whole-body Magnetic Resonance Imaging-based Evaluations of Multiorgan Involvement in Advanced Prostate Cancer. Eur. Urol. 2017, 71, 81–92. Available online: http://www.ncbi.nlm.nih.gov/pubmed/27317091 (accessed on 16 April 2022). [CrossRef] [PubMed]
- Barnes, A.; Alonzi, R.; Blackledge, M.; Charles-Edwards, G.; Collins, D.J.; Cook, G.; Coutts, G.; Goh, V.; Graves, M.; Kelly, C.; et al. UK quantitative WB-DWI technical workgroup: Consensus meeting recommendations on optimisation, quality control, processing and analysis of quantitative whole-body diffusion-weighted imaging for cancer. Br. J. Radiol. 2018, 91, 20170577. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29076749 (accessed on 16 April 2022). [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdelrazek, A.; Mahmoud, A.M.; Joshi, V.B.; Habeeb, M.; Ahmed, M.E.; Ghoniem, K.; Delgado, A.; Khater, N.; Kwon, E.; Kendi, A.T. Recent Advances in Prostate Cancer (PCa) Diagnostics. Uro 2022, 2, 109-121. https://doi.org/10.3390/uro2020014
Abdelrazek A, Mahmoud AM, Joshi VB, Habeeb M, Ahmed ME, Ghoniem K, Delgado A, Khater N, Kwon E, Kendi AT. Recent Advances in Prostate Cancer (PCa) Diagnostics. Uro. 2022; 2(2):109-121. https://doi.org/10.3390/uro2020014
Chicago/Turabian StyleAbdelrazek, Ahmad, Ahmed M. Mahmoud, Vidhu B. Joshi, Mohamed Habeeb, Mohamed E. Ahmed, Khaled Ghoniem, Arleen Delgado, Nazih Khater, Eugene Kwon, and A. Tuba Kendi. 2022. "Recent Advances in Prostate Cancer (PCa) Diagnostics" Uro 2, no. 2: 109-121. https://doi.org/10.3390/uro2020014
APA StyleAbdelrazek, A., Mahmoud, A. M., Joshi, V. B., Habeeb, M., Ahmed, M. E., Ghoniem, K., Delgado, A., Khater, N., Kwon, E., & Kendi, A. T. (2022). Recent Advances in Prostate Cancer (PCa) Diagnostics. Uro, 2(2), 109-121. https://doi.org/10.3390/uro2020014