

Spontaneous Bacterial Peritonitis in Decompensated Liver Cirrhosis—A Literature Review



Abstract
1. Introduction
2. Materials and Methods
3. Types of SBP
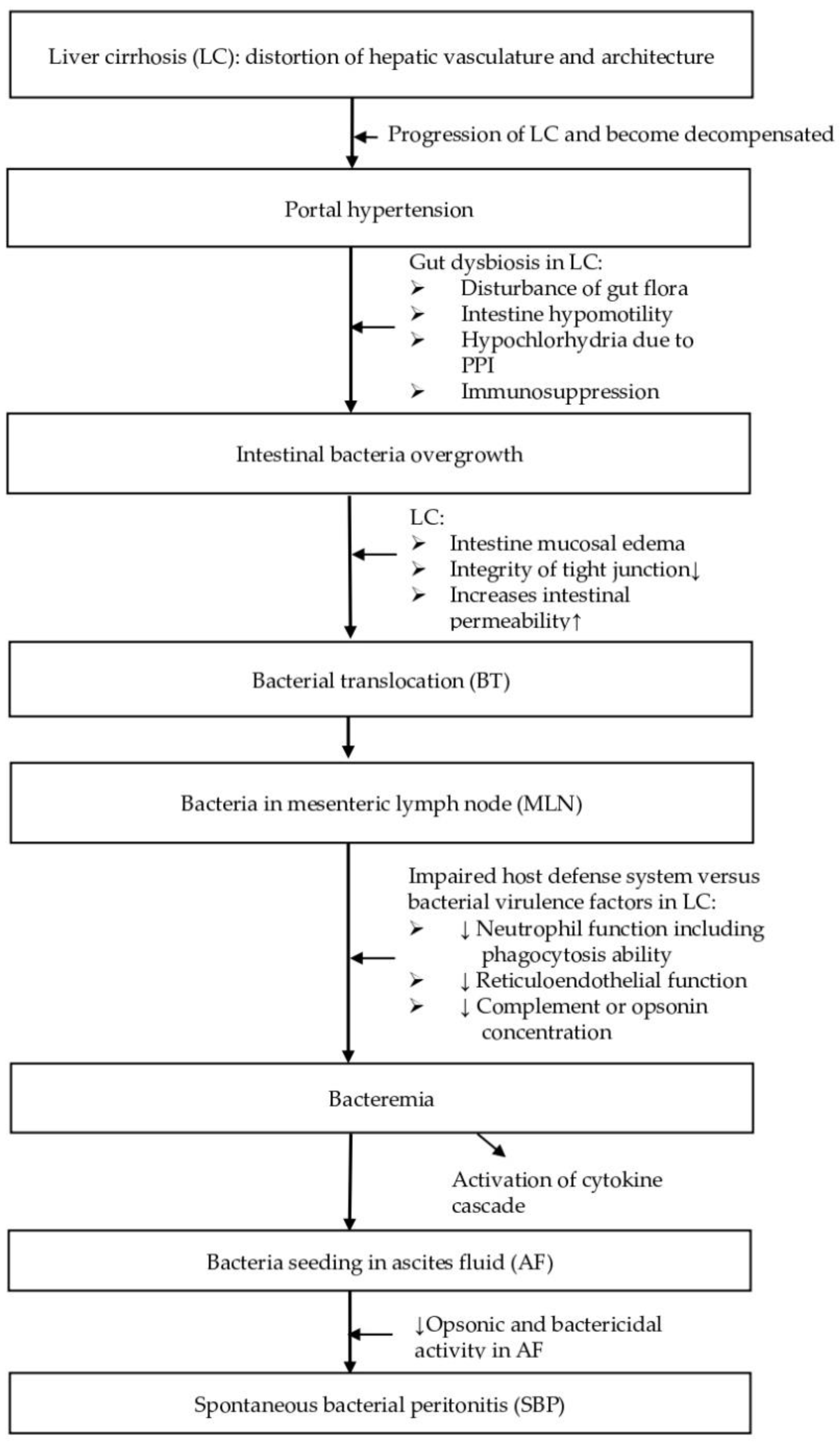
4. Pathogenesis
4.1. Gut Dysbiosis
4.2. Bacterial Translocation
4.3. Impaired Host Defense System
5. Bacteriology
5.1. Gram-Negative Bacilli
5.2. Gram-Positive Cocci
5.3. Multidrug-Resistant Microorganisms
5.4. Anaerobes
5.5. Community-Acquired SBP vs. Healthcare-Associated SBP vs. Nosocomial-Acquired SBP
6. Diagnosis
6.1. Clinical Presentations
6.2. Diagnostic Paracentesis
6.3. Handling and Interpretation of Ascites Fluid Study
6.4. Diagnostic Criteria for SBP Types, Distinguishing Secondary Bacterial Peritonitis
6.5. Other Diagnostic Markers of SBP
7. Risk Factors
7.1. First Episode
7.2. Recurrent Episodes
8. Prognosis
8.1. In-Hospital Mortality
8.2. Long-Term Mortality
9. Treatment
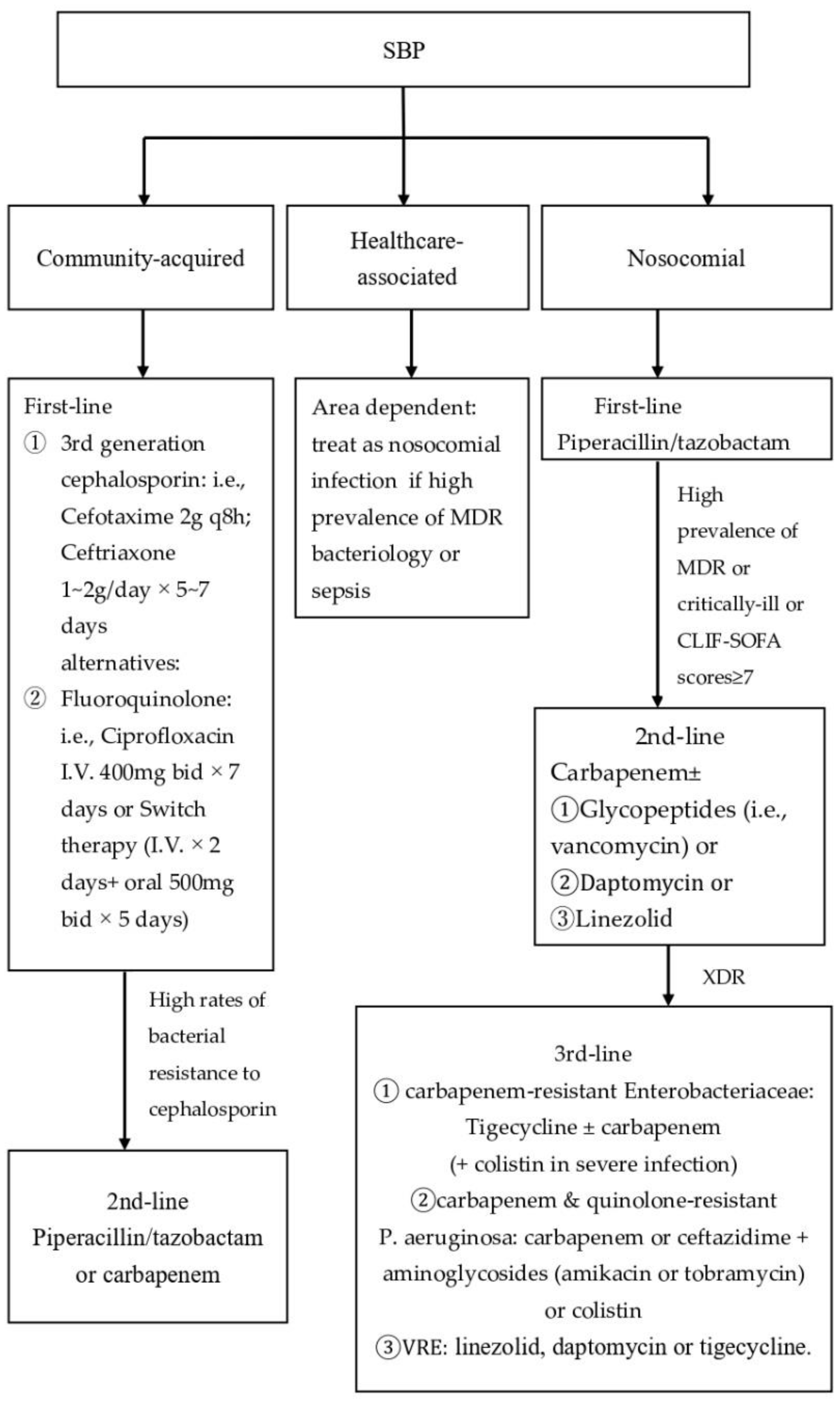
9.1. Antibiotic Therapy
9.1.1. Community-Acquired SBP
9.1.2. Nosocomial and Healthcare SBP
9.2. Indication for Repeated Paracentesis
9.3. Albumin Supplement in Patients with Renal Impairment
9.4. Discontinue NSBB in Patients with SBP
9.5. Other Novel Therapeutic Strategies
10. Prophylaxis of SBP
10.1. SBP Prophylaxis in High-Risk Groups
10.1.1. Prophylaxis in Patients with Upper Gastrointestinal Bleeding (UGIB)
10.1.2. Primary Prophylaxis in Patients with Low Ascites Total Protein and Associated Advanced Liver Failure or Renal Dysfunction without History of SBP
10.1.3. Secondary Prophylaxis in Patients with Prior SBP
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wasmuth, H.E.; Kunz, D.; Yagmur, E.; Timmer-Stranghöner, A.; Vidacek, D.; Siewert, E.; Bach, J.; Geier, A.; Purucker, E.A.; Gressner, A.M. Patients with acute on chronic liver failure display ‘sepsis-like’immune paralysis. J. Hepatol. 2005, 42, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Wiest, R.; Garcia-Tsao, G. Bacterial translocation (BT) in cirrhosis. Hepatology 2005, 41, 422–433. [Google Scholar] [CrossRef] [PubMed]
- Fernández, J.; Navasa, M.; Gómez, J.; Colmenero, J.; Vila, J.; Arroyo, V.; Rodés, J. Bacterial infections in cirrhosis: Epidemiological changes with invasive procedures and norfloxacin prophylaxis. Hepatology 2002, 35, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.H.; Lin, C.Y.; Sheen, I.S.; Chen, W.T.; Lin, T.N.; Ho, Y.P.; Chiu, C.T. Recurrence of spontaneous bacterial peritonitis in cirrhotic patients non-prophylactically treated with norfloxacin: Serum albumin as an easy but reliable predictive factor. Liver Int. 2011, 31, 184–191. [Google Scholar] [CrossRef]
- Aithal, G.P.; Palaniyappan, N.; China, L.; Harmala, S.; Macken, L.; Ryan, J.M.; Wilkes, E.A.; Moore, K.; Leithead, J.A.; Hayes, P.C.; et al. Guidelines on the management of ascites in cirrhosis. Gut 2021, 70, 9–29. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Tsao, G. Current management of the complications of cirrhosis and portal hypertension: Variceal hemorrhage, ascites, and spontaneous bacterial peritonitis. Gastroenterology 2001, 120, 726–748. [Google Scholar] [CrossRef]
- Rimola, A.; García-Tsao, G.; Navasa, M.; Piddock, L.J.; Planas, R.; Bernard, B.; Inadomi, J.M. Diagnosis, treatment and prophylaxis of spontaneous bacterial peritonitis: A consensus document. J. Hepatol. 2000, 32, 142–153. [Google Scholar] [CrossRef]
- Runyon, B.A.; AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012. Hepatology 2013, 57, 1651–1653. [Google Scholar] [CrossRef]
- Akriviadis, E.A.; Runyon, B.A. Utility of an algorithm in differentiating spontaneous from secondary bacterial peritonitis. Gastroenterology 1990, 98, 127–133. [Google Scholar] [CrossRef]
- Runyon, B.A.; Committee, A.P.G. Management of adult patients with ascites due to cirrhosis: An update. Hepatology 2009, 49, 2087–2107. [Google Scholar] [CrossRef]
- Dever, J.B.; Sheikh, M.Y. Review article: Spontaneous bacterial peritonitis--bacteriology, diagnosis, treatment, risk factors and prevention. Aliment. Pharmacol. Ther. 2015, 41, 1116–1131. [Google Scholar] [CrossRef] [PubMed]
- Pinzello, G.; Simonetti, R.G.; Craxi, A.; Di Piazza, S.; Spano, C.; Pagliaro, L. Spontaneous bacterial peritonitis: A prospective investigation in predominantly nonalcoholic cirrhotic patients. Hepatology 1983, 3, 545–549. [Google Scholar] [CrossRef]
- Fernandez, J.; Navasa, M.; Planas, R.; Montoliu, S.; Monfort, D.; Soriano, G.; Vila, C.; Pardo, A.; Quintero, E.; Vargas, V.; et al. Primary prophylaxis of spontaneous bacterial peritonitis delays hepatorenal syndrome and improves survival in cirrhosis. Gastroenterology 2007, 133, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Navasa, M.; Follo, A.; Llovet, J.M.; Clemente, G.; Vargas, V.; Rimola, A.; Marco, F.; Guarner, C.; Forne, M.; Planas, R.; et al. Randomized, comparative study of oral ofloxacin versus intravenous cefotaxime in spontaneous bacterial peritonitis. Gastroenterology 1996, 111, 1011–1017. [Google Scholar] [CrossRef]
- Navasa, M.; Follo, A.; Filella, X.; Jimenez, W.; Francitorra, A.; Planas, R.; Rimola, A.; Arroyo, V.; Rodes, J. Tumor necrosis factor and interleukin-6 in spontaneous bacterial peritonitis in cirrhosis: Relationship with the development of renal impairment and mortality. Hepatology 1998, 27, 1227–1232. [Google Scholar] [CrossRef]
- Al-Ghamdi, H.; Al-Harbi, N.; Mokhtar, H.; Daffallah, M.; Memon, Y.; Aljumah, A.A.; Sanai, F.M. Changes in the patterns and microbiology of spontaneous bacterial peritonitis: Analysis of 200 cirrhotic patients. Acta Gastro Enterol. Belg. 2019, 82, 261–266. [Google Scholar]
- Na, S.H.; Kim, E.J.; Nam, E.Y.; Song, K.H.; Choe, P.G.; Park, W.B.; Bang, J.H.; Kim, E.S.; Park, S.W.; Kim, H.B.; et al. Comparison of clinical characteristics and outcomes of spontaneous bacterial peritonitis and culture negative neutrocytic ascites. Scand. J. Gastroenterol. 2017, 52, 199–203. [Google Scholar] [CrossRef]
- Runyon, B.A.; Canawati, H.N.; Akriviadis, E.A. Optimization of ascitic fluid culture technique. Gastroenterology 1988, 95, 1351–1355. [Google Scholar] [CrossRef]
- Oladimeji, A.A.; Temi, A.P.; Adekunle, A.E.; Taiwo, R.H.; Ayokunle, D.S. Prevalence of spontaneous bacterial peritonitis in liver cirrhosis with ascites. Pan Afr. Med. J. 2013, 15, 128. [Google Scholar] [CrossRef]
- Chu, C.M.; Chang, K.Y.; Liaw, Y.F. Prevalence and prognostic significance of bacterascites in cirrhosis with ascites. Dig. Dis. Sci. 1995, 40, 561–565. [Google Scholar] [CrossRef]
- Runyon, B.A.; Squier, S.; Borzio, M. Translocation of gut bacteria in rats with cirrhosis to mesenteric lymph nodes partially explains the pathogenesis of spontaneous bacterial peritonitis. J. Hepatol. 1994, 21, 792–796. [Google Scholar] [CrossRef]
- Berg, R.D.; Garlington, A.W. Translocation of certain indigenous bacteria from the gastrointestinal tract to the mesenteric lymph nodes and other organs in a gnotobiotic mouse model. Infect. Immun. 1979, 23, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Vilela, E.G.; Thabut, D.; Rudler, M.; Bittencourt, P.L. Management of Complications of Portal Hypertension. Can. J. Gastroenterol. Hepatol. 2019, 2019, 6919284. [Google Scholar] [CrossRef] [PubMed]
- Guarner, C.; Runyon, B.A.; Young, S.; Heck, M.; Sheikh, M.Y. Intestinal bacterial overgrowth and bacterial translocation in cirrhotic rats with ascites. J. Hepatol. 1997, 26, 1372–1378. [Google Scholar] [CrossRef]
- Cirera, I.; Bauer, T.M.; Navasa, M.; Vila, J.; Grande, L.; Taura, P.; Fuster, J.; Garcia-Valdecasas, J.C.; Lacy, A.; Suarez, M.J.; et al. Bacterial translocation of enteric organisms in patients with cirrhosis. J. Hepatol. 2001, 34, 32–37. [Google Scholar] [CrossRef]
- Dunn, D.L.; Barke, R.A.; Knight, N.B.; Humphrey, E.W.; Simmons, R.L. Role of resident macrophages, peripheral neutrophils, and translymphatic absorption in bacterial clearance from the peritoneal cavity. Infect. Immun. 1985, 49, 257–264. [Google Scholar] [CrossRef]
- Ruiz-Alcaraz, A.J.; Martinez-Banaclocha, H.; Marin-Sanchez, P.; Carmona-Martinez, V.; Iniesta-Albadalejo, M.A.; Tristan-Manzano, M.; Tapia-Abellan, A.; Garcia-Penarrubia, P.; Machado-Linde, F.; Pelegrin, P.; et al. Isolation of functional mature peritoneal macrophages from healthy humans. Immunol. Cell Biol. 2020, 98, 114–126. [Google Scholar] [CrossRef]
- Charles, A.; Janeway, J.; Travers, P.; Walport, M.; Shlomchik, M.J. Immunobiology: The Immune System in Health and Disease, 5th ed.; Garland Publishing: New York, NY, USA, 2001. [Google Scholar]
- Huang, C.H.; Jeng, W.J.; Ho, Y.P.; Teng, W.; Hsieh, Y.C.; Chen, W.T.; Chen, Y.C.; Lin, H.H.; Sheen, I.S.; Lin, C.Y. Increased EMR2 expression on neutrophils correlates with disease severity and predicts overall mortality in cirrhotic patients. Sci. Rep. 2016, 6, 38250. [Google Scholar] [CrossRef]
- Rimola, A.; Soto, R.; Bory, F.; Arroyo, V.; Piera, C.; Rodes, J. Reticuloendothelial system phagocytic activity in cirrhosis and its relation to bacterial infections and prognosis. Hepatology 1984, 4, 53–58. [Google Scholar] [CrossRef]
- Runyon, B.A. Low-protein-concentration ascitic fluid is predisposed to spontaneous bacterial peritonitis. Gastroenterology 1986, 91, 1343–1346. [Google Scholar] [CrossRef]
- Hoefs, J.C.; Runyon, B.A. Spontaneous bacterial peritonitis. Dis. Mon. 1985, 31, 1–48. [Google Scholar] [CrossRef]
- Wiest, R.; Krag, A.; Gerbes, A. Spontaneous bacterial peritonitis: Recent guidelines and beyond. Gut 2012, 61, 297–310. [Google Scholar] [CrossRef] [PubMed]
- Bhuva, M.; Ganger, D.; Jensen, D. Spontaneous bacterial peritonitis: An update on evaluation, management, and prevention. Am. J. Med. 1994, 97, 169–175. [Google Scholar] [CrossRef]
- Runyon, B.A. Monomicrobial nonneutrocytic bacterascites: A variant of spontaneous bacterial peritonitis. Hepatology 1990, 12, 710–715. [Google Scholar] [CrossRef]
- Piroth, L.; Pechinot, A.; Di Martino, V.; Hansmann, Y.; Putot, A.; Patry, I.; Hadou, T.; Jaulhac, B.; Chirouze, C.; Rabaud, C.; et al. Evolving epidemiology and antimicrobial resistance in spontaneous bacterial peritonitis: A two-year observational study. BMC Infect. Dis. 2014, 14, 287. [Google Scholar] [CrossRef]
- Gines, P.; Rimola, A.; Planas, R.; Vargas, V.; Marco, F.; Almela, M.; Forne, M.; Miranda, M.L.; Llach, J.; Salmeron, J.M.; et al. Norfloxacin prevents spontaneous bacterial peritonitis recurrence in cirrhosis: Results of a double-blind, placebo-controlled trial. Hepatology 1990, 12, 716–724. [Google Scholar] [CrossRef]
- Llovet, J.M.; Rodriguez-Iglesias, P.; Moitinho, E.; Planas, R.; Bataller, R.; Navasa, M.; Menacho, M.; Pardo, A.; Castells, A.; Cabre, E.; et al. Spontaneous bacterial peritonitis in patients with cirrhosis undergoing selective intestinal decontamination. A retrospective study of 229 spontaneous bacterial peritonitis episodes. J. Hepatol. 1997, 26, 88–95. [Google Scholar] [CrossRef]
- Campillo, B.; Dupeyron, C.; Richardet, J.P.; Mangeney, N.; Leluan, G. Epidemiology of severe hospital-acquired infections in patients with liver cirrhosis: Effect of long-term administration of norfloxacin. Clin. Infect. Dis. 1998, 26, 1066–1070. [Google Scholar] [CrossRef]
- Alexopoulou, A.; Papadopoulos, N.; Eliopoulos, D.G.; Alexaki, A.; Tsiriga, A.; Toutouza, M.; Pectasides, D. Increasing frequency of gram-positive cocci and gram-negative multidrug-resistant bacteria in spontaneous bacterial peritonitis. Liver Int. 2013, 33, 975–981. [Google Scholar] [CrossRef]
- Fernandez, J.; Acevedo, J.; Castro, M.; Garcia, O.; de Lope, C.R.; Roca, D.; Pavesi, M.; Sola, E.; Moreira, L.; Silva, A.; et al. Prevalence and risk factors of infections by multiresistant bacteria in cirrhosis: A prospective study. Hepatology 2012, 55, 1551–1561. [Google Scholar] [CrossRef]
- Reuken, P.A.; Pletz, M.W.; Baier, M.; Pfister, W.; Stallmach, A.; Bruns, T. Emergence of spontaneous bacterial peritonitis due to enterococci—Risk factors and outcome in a 12-year retrospective study. Aliment Pharm. 2012, 35, 1199–1208. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulou, A.; Vasilieva, L.; Agiasotelli, D.; Siranidi, K.; Pouriki, S.; Tsiriga, A.; Toutouza, M.; Dourakis, S.P. Extensively drug-resistant bacteria are an independent predictive factor of mortality in 130 patients with spontaneous bacterial peritonitis or spontaneous bacteremia. World J. Gastroenterol. 2016, 22, 4049. [Google Scholar] [CrossRef] [PubMed]
- Dupeyron, C.; Campillo, S.B.; Mangeney, N.; Richardet, J.P.; Leluan, G. Carriage of Staphylococcus aureus and of gram-negative bacilli resistant to third-generation cephalosporins in cirrhotic patients: A prospective assessment of hospital-acquired infections. Infect. Control Hosp. Epidemiol. 2001, 22, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Campillo, B.; Richardet, J.P.; Kheo, T.; Dupeyron, C. Nosocomial spontaneous bacterial peritonitis and bacteremia in cirrhotic patients: Impact of isolate type on prognosis and characteristics of infection. Clin. Infect. Dis. 2002, 35, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Such, J.; Runyon, B.A. Spontaneous bacterial peritonitis. Clin. Infect. Dis. 1998, 27, 669–674, quiz 675–666. [Google Scholar] [CrossRef]
- Sheckman, P.; Onderdonk, A.B.; Bartlett, J.G. Anaerobes in spontaneous peritonitis. Lancet 1977, 2, 1223. [Google Scholar] [CrossRef]
- Shi, L.; Wu, D.; Wei, L.; Liu, S.; Zhao, P.; Tu, B.; Xie, Y.; Liu, Y.; Wang, X.; Liu, L.; et al. Nosocomial and Community-Acquired Spontaneous Bacterial Peritonitis in patients with liver cirrhosis in China: Comparative Microbiology and Therapeutic Implications. Sci. Rep. 2017, 7, 46025. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis. J. Hepatol. 2010, 53, 397–417. [Google Scholar] [CrossRef]
- Orman, E.S.; Hayashi, P.H.; Bataller, R.; Barritt, A.S.t. Paracentesis is associated with reduced mortality in patients hospitalized with cirrhosis and ascites. Clin. Gastroenterol. Hepatol. 2014, 12, 496–503.e1. [Google Scholar] [CrossRef]
- Kim, J.J.; Tsukamoto, M.M.; Mathur, A.K.; Ghomri, Y.M.; Hou, L.A.; Sheibani, S.; Runyon, B.A. Delayed paracentesis is associated with increased in-hospital mortality in patients with spontaneous bacterial peritonitis. Am. J. Gastroenterol. 2014, 109, 1436–1442. [Google Scholar] [CrossRef]
- Grabau, C.M.; Crago, S.F.; Hoff, L.K.; Simon, J.A.; Melton, C.A.; Ott, B.J.; Kamath, P.S. Performance standards for therapeutic abdominal paracentesis. Hepatology 2004, 40, 484–488. [Google Scholar] [CrossRef] [PubMed]
- Runyon, B.A.; Umland, E.T.; Merlin, T. Inoculation of blood culture bottles with ascitic fluid. Improved detection of spontaneous bacterial peritonitis. Arch. Intern. Med. 1987, 147, 73–75. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef] [PubMed]
- Hoefs, J.C. Increase in ascites white blood cell and protein concentrations during diuresis in patients with chronic liver disease. Hepatology 1981, 1, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Runyon, B.A.; Hoefs, J.C. Culture-negative neutrocytic ascites: A variant of spontaneous bacterial peritonitis. Hepatology 1984, 4, 1209–1211. [Google Scholar] [CrossRef] [PubMed]
- Garrison, R.N.; Cryer, H.M.; Howard, D.A.; Polk, H.C., Jr. Clarification of risk factors for abdominal operations in patients with hepatic cirrhosis. Ann. Surg. 1984, 199, 648–655. [Google Scholar] [CrossRef]
- Runyon, B.A.; Hoefs, J.C. Ascitic fluid analysis in the differentiation of spontaneous bacterial peritonitis from gastrointestinal tract perforation into ascitic fluid. Hepatology 1984, 4, 447–450. [Google Scholar] [CrossRef]
- Soriano, G.; Castellote, J.; Alvarez, C.; Girbau, A.; Gordillo, J.; Baliellas, C.; Casas, M.; Pons, C.; Roman, E.M.; Maisterra, S.; et al. Secondary bacterial peritonitis in cirrhosis: A retrospective study of clinical and analytical characteristics, diagnosis and management. J. Hepatol. 2010, 52, 39–44. [Google Scholar] [CrossRef]
- Weil, D.; Heurgue-Berlot, A.; Monnet, E.; Chassagne, S.; Cervoni, J.P.; Feron, T.; Grandvallet, C.; Muel, E.; Bronowicki, J.P.; Thiefin, G.; et al. Accuracy of calprotectin using the Quantum Blue Reader for the diagnosis of spontaneous bacterial peritonitis in liver cirrhosis. Hepatol. Res. 2019, 49, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Lutz, P.; Pfarr, K.; Nischalke, H.D.; Kramer, B.; Goeser, F.; Glassner, A.; Wolter, F.; Kokordelis, P.; Nattermann, J.; Sauerbruch, T.; et al. The ratio of calprotectin to total protein as a diagnostic and prognostic marker for spontaneous bacterial peritonitis in patients with liver cirrhosis and ascites. Clin. Chem. Lab. Med. 2015, 53, 2031–2039. [Google Scholar] [CrossRef]
- Gundling, F.; Schmidtler, F.; Hapfelmeier, A.; Schulte, B.; Schmidt, T.; Pehl, C.; Schepp, W.; Seidl, H. Fecal calprotectin is a useful screening parameter for hepatic encephalopathy and spontaneous bacterial peritonitis in cirrhosis. Liver Int. 2011, 31, 1406–1415. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.H.; Tseng, H.J.; Amodio, P.; Chen, Y.L.; Wang, S.F.; Chang, S.H.; Hsieh, S.Y.; Lin, C.Y. Hepatic Encephalopathy and Spontaneous Bacterial Peritonitis Improve Cirrhosis Outcome Prediction: A Modified Seven-Stage Model as a Clinical Alternative to MELD. J. Pers. Med. 2020, 10, 186. [Google Scholar] [CrossRef] [PubMed]
- Andreu, M.; Sola, R.; Sitges-Serra, A.; Alia, C.; Gallen, M.; Vila, M.C.; Coll, S.; Oliver, M.I. Risk factors for spontaneous bacterial peritonitis in cirrhotic patients with ascites. Gastroenterology 1993, 104, 1133–1138. [Google Scholar] [CrossRef]
- Runyon, B.A.; Morrissey, R.L.; Hoefs, J.C.; Wyle, F.A. Opsonic activity of human ascitic fluid: A potentially important protective mechanism against spontaneous bacterial peritonitis. Hepatology 1985, 5, 634–637. [Google Scholar] [CrossRef] [PubMed]
- Bernard, B.; Cadranel, J.F.; Valla, D.; Escolano, S.; Jarlier, V.; Opolon, P. Prognostic significance of bacterial infection in bleeding cirrhotic patients: A prospective study. Gastroenterology 1995, 108, 1828–1834. [Google Scholar] [CrossRef]
- Bernard, B.; Grange, J.D.; Khac, E.N.; Amiot, X.; Opolon, P.; Poynard, T. Antibiotic prophylaxis for the prevention of bacterial infections in cirrhotic patients with gastrointestinal bleeding: A meta-analysis. Hepatology 1999, 29, 1655–1661. [Google Scholar] [CrossRef]
- Martinez, J.; Hernandez-Gea, V.; Rodriguez-de-Santiago, E.; Tellez, L.; Procopet, B.; Giraldez, A.; Amitrano, L.; Villanueva, C.; Thabut, D.; Ibanez-Samaniego, L.; et al. Bacterial infections in patients with acute variceal bleeding in the era of antibiotic prophylaxis. J. Hepatol. 2021, 75, 342–350. [Google Scholar] [CrossRef]
- Deshpande, A.; Pasupuleti, V.; Thota, P.; Pant, C.; Mapara, S.; Hassan, S.; Rolston, D.D.; Sferra, T.J.; Hernandez, A.V. Acid-suppressive therapy is associated with spontaneous bacterial peritonitis in cirrhotic patients: A meta-analysis. J. Gastroenterol. Hepatol. 2013, 28, 235–242. [Google Scholar] [CrossRef]
- Trikudanathan, G.; Israel, J.; Cappa, J.; O’Sullivan, D.M. Association between proton pump inhibitors and spontaneous bacterial peritonitis in cirrhotic patients—A systematic review and meta-analysis. Int. J. Clin. Pract. 2011, 65, 674–678. [Google Scholar] [CrossRef]
- O’Leary, J.G.; Reddy, K.R.; Wong, F.; Kamath, P.S.; Patton, H.M.; Biggins, S.W.; Fallon, M.B.; Garcia-Tsao, G.; Subramanian, R.M.; Malik, R.; et al. Long-term use of antibiotics and proton pump inhibitors predict development of infections in patients with cirrhosis. Clin. Gastroenterol. Hepatol. 2015, 13, 753–759.e1-2. [Google Scholar] [CrossRef]
- Alaniz, C.; Regal, R.E. Spontaneous bacterial peritonitis: A review of treatment options. P T 2009, 34, 204–210. [Google Scholar] [PubMed]
- Senzolo, M.; Cholongitas, E.; Burra, P.; Leandro, G.; Thalheimer, U.; Patch, D.; Burroughs, A.K. beta-Blockers protect against spontaneous bacterial peritonitis in cirrhotic patients: A meta-analysis. Liver Int. 2009, 29, 1189–1193. [Google Scholar] [CrossRef] [PubMed]
- Senkerikova, R.; de Mare-Bredemeijer, E.; Frankova, S.; Roelen, D.; Visseren, T.; Trunecka, P.; Spicak, J.; Metselaar, H.; Jirsa, M.; Kwekkeboom, J.; et al. Genetic variation in TNFA predicts protection from severe bacterial infections in patients with end-stage liver disease awaiting liver transplantation. J. Hepatol. 2014, 60, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Tito, L.; Rimola, A.; Gines, P.; Llach, J.; Arroyo, V.; Rodes, J. Recurrence of spontaneous bacterial peritonitis in cirrhosis: Frequency and predictive factors. Hepatology 1988, 8, 27–31. [Google Scholar] [CrossRef]
- Hung, T.H.; Tsai, C.C.; Hsieh, Y.H.; Tsai, C.C. The long-term mortality of spontaneous bacterial peritonitis in cirrhotic patients: A 3-year nationwide cohort study. Turk. J. Gastroenterol. 2015, 26, 159–162. [Google Scholar] [CrossRef]
- Tandon, P.; Garcia-Tsao, G. Renal dysfunction is the most important independent predictor of mortality in cirrhotic patients with spontaneous bacterial peritonitis. Clin. Gastroenterol. Hepatol. 2011, 9, 260–265. [Google Scholar] [CrossRef]
- Karvellas, C.J.; Abraldes, J.G.; Arabi, Y.M.; Kumar, A.; Cooperative Antimicrobial Therapy of Septic Shock Database Research Group. Appropriate and timely antimicrobial therapy in cirrhotic patients with spontaneous bacterial peritonitis-associated septic shock: A retrospective cohort study. Aliment. Pharmacol. Ther. 2015, 41, 747–757. [Google Scholar] [CrossRef]
- Bac, D.J. Spontaneous bacterial peritonitis: An indication for liver transplantation? Scand. J. Gastroenterol. Suppl. 1996, 218, 38–42. [Google Scholar] [CrossRef]
- Cabrera, J.; Arroyo, V.; Ballesta, A.M.; Rimola, A.; Gual, J.; Elena, M.; Rodes, J. Aminoglycoside nephrotoxicity in cirrhosis. Value of urinary beta 2-microglobulin to discriminate functional renal failure from acute tubular damage. Gastroenterology 1982, 82, 97–105. [Google Scholar] [CrossRef]
- Umgelter, A.; Reindl, W.; Miedaner, M.; Schmid, R.M.; Huber, W. Failure of current antibiotic first-line regimens and mortality in hospitalized patients with spontaneous bacterial peritonitis. Infection 2009, 37, 2–8. [Google Scholar] [CrossRef]
- Chavez-Tapia, N.C.; Soares-Weiser, K.; Brezis, M.; Leibovici, L. Antibiotics for spontaneous bacterial peritonitis in cirrhotic patients. Cochrane Database Syst. Rev. 2009, CD002232. [Google Scholar] [CrossRef] [PubMed]
- Felisart, J.; Rimola, A.; Arroyo, V.; Perez-Ayuso, R.M.; Quintero, E.; Gines, P.; Rodes, J. Cefotaxime is more effective than is ampicillin-tobramycin in cirrhotics with severe infections. Hepatology 1985, 5, 457–462. [Google Scholar] [CrossRef]
- Rimola, A.; Salmeron, J.M.; Clemente, G.; Rodrigo, L.; Obrador, A.; Miranda, M.L.; Guarner, C.; Planas, R.; Sola, R.; Vargas, V.; et al. Two different dosages of cefotaxime in the treatment of spontaneous bacterial peritonitis in cirrhosis: Results of a prospective, randomized, multicenter study. Hepatology 1995, 21, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Runyon, B.A.; McHutchison, J.G.; Antillon, M.R.; Akriviadis, E.A.; Montano, A.A. Short-course versus long-course antibiotic treatment of spontaneous bacterial peritonitis. A randomized controlled study of 100 patients. Gastroenterology 1991, 100, 1737–1742. [Google Scholar] [CrossRef]
- Fernandez, J.; Ruiz del Arbol, L.; Gomez, C.; Durandez, R.; Serradilla, R.; Guarner, C.; Planas, R.; Arroyo, V.; Navasa, M. Norfloxacin vs ceftriaxone in the prophylaxis of infections in patients with advanced cirrhosis and hemorrhage. Gastroenterology 2006, 131, 1049–1056, quiz 1285. [Google Scholar] [CrossRef] [PubMed]
- Mazer, L.; Tapper, E.B.; Piatkowski, G.; Lai, M. The need for antibiotic stewardship and treatment standardization in the care of cirrhotic patients with spontaneous bacterial peritonitis—A retrospective cohort study examining the effect of ceftriaxone dosing. F1000Research 2014, 3, 57. [Google Scholar] [CrossRef] [PubMed]
- Baskol, M.; Gursoy, S.; Baskol, G.; Ozbakir, O.; Guven, K.; Yucesoy, M. Five days of ceftriaxone to treat culture negative neutrocytic ascites in cirrhotic patients. J. Clin. Gastroenterol. 2003, 37, 403–405. [Google Scholar] [CrossRef][Green Version]
- Terg, R.; Cobas, S.; Fassio, E.; Landeira, G.; Rios, B.; Vasen, W.; Abecasis, R.; Rios, H.; Guevara, M. Oral ciprofloxacin after a short course of intravenous ciprofloxacin in the treatment of spontaneous bacterial peritonitis: Results of a multicenter, randomized study. J. Hepatol. 2000, 33, 564–569. [Google Scholar] [CrossRef]
- Angeli, P.; Guarda, S.; Fasolato, S.; Miola, E.; Craighero, R.; Piccolo, F.; Antona, C.; Brollo, L.; Franchin, M.; Cillo, U.; et al. Switch therapy with ciprofloxacin vs. intravenous ceftazidime in the treatment of spontaneous bacterial peritonitis in patients with cirrhosis: Similar efficacy at lower cost. Aliment. Pharmacol. Ther. 2006, 23, 75–84. [Google Scholar] [CrossRef]
- Ariza, X.; Castellote, J.; Lora-Tamayo, J.; Girbau, A.; Salord, S.; Rota, R.; Ariza, J.; Xiol, X. Risk factors for resistance to ceftriaxone and its impact on mortality in community, healthcare and nosocomial spontaneous bacterial peritonitis. J. Hepatol. 2012, 56, 825–832. [Google Scholar] [CrossRef]
- Piano, S.; Fasolato, S.; Salinas, F.; Romano, A.; Tonon, M.; Morando, F.; Cavallin, M.; Gola, E.; Sticca, A.; Loregian, A.; et al. The empirical antibiotic treatment of nosocomial spontaneous bacterial peritonitis: Results of a randomized, controlled clinical trial. Hepatology 2016, 63, 1299–1309. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Yoon, J.S.; Park, J.; Jung, Y.J.; Lee, J.S.; Song, J.; Lee, H.A.; Seo, Y.S.; Lee, M.; Park, J.M.; et al. Empirical Treatment With Carbapenem vs Third-generation Cephalosporin for Treatment of Spontaneous Bacterial Peritonitis. Clin. Gastroenterol. Hepatol. 2021, 19, 976–986.e5. [Google Scholar] [CrossRef] [PubMed]
- Piano, S.; Brocca, A.; Mareso, S.; Angeli, P. Infections complicating cirrhosis. Liver Int. 2018, 38 (Suppl. 1), 126–133. [Google Scholar] [CrossRef] [PubMed]
- Falcone, M.; Russo, A.; Pacini, G.; Merli, M.; Venditti, M. Spontaneous Bacterial Peritonitis Due to Methicillin-Resistant Staphylococcus Aureus in a Patient with Cirrhosis: The Potential Role for Daptomycin and Review of the Literature. Infect. Dis. Rep. 2015, 7, 6127. [Google Scholar] [CrossRef]
- Koulenti, D.; Xu, E.; Mok, I.Y.S.; Song, A.; Karageorgopoulos, D.E.; Armaganidis, A.; Lipman, J.; Tsiodras, S. Novel Antibiotics for Multidrug-Resistant Gram-Positive Microorganisms. Microorganisms 2019, 7, 270. [Google Scholar] [CrossRef]
- Sort, P.; Navasa, M.; Arroyo, V.; Aldeguer, X.; Planas, R.; Ruiz-del-Arbol, L.; Castells, L.; Vargas, V.; Soriano, G.; Guevara, M.; et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. N. Engl. J. Med. 1999, 341, 403–409. [Google Scholar] [CrossRef]
- Sigal, S.H.; Stanca, C.M.; Fernandez, J.; Arroyo, V.; Navasa, M. Restricted use of albumin for spontaneous bacterial peritonitis. Gut 2007, 56, 597–599. [Google Scholar] [CrossRef][Green Version]
- Salerno, F.; Navickis, R.J.; Wilkes, M.M. Albumin infusion improves outcomes of patients with spontaneous bacterial peritonitis: A meta-analysis of randomized trials. Clin. Gastroenterol. Hepatol. 2013, 11, 123–130.e1. [Google Scholar] [CrossRef]
- Mandorfer, M.; Bota, S.; Schwabl, P.; Bucsics, T.; Pfisterer, N.; Kruzik, M.; Hagmann, M.; Blacky, A.; Ferlitsch, A.; Sieghart, W.; et al. Nonselective beta blockers increase risk for hepatorenal syndrome and death in patients with cirrhosis and spontaneous bacterial peritonitis. Gastroenterology 2014, 146, 1680–1690.e1. [Google Scholar] [CrossRef]
- Pampalone, M.; Vitale, G.; Gruttadauria, S.; Amico, G.; Iannolo, G.; Douradinha, B.; Mularoni, A.; Conaldi, P.G.; Pietrosi, G. Human Amnion-Derived Mesenchymal Stromal Cells: A New Potential Treatment for Carbapenem-Resistant Enterobacterales in Decompensated Cirrhosis. Int. J. Mol. Sci. 2022, 23, 857. [Google Scholar] [CrossRef]
- Soriano, G.; Guarner, C.; Teixido, M.; Such, J.; Barrios, J.; Enriquez, J.; Vilardell, F. Selective intestinal decontamination prevents spontaneous bacterial peritonitis. Gastroenterology 1991, 100, 477–481. [Google Scholar] [CrossRef]
- Soriano, G.; Guarner, C.; Tomas, A.; Villanueva, C.; Torras, X.; Gonzalez, D.; Sainz, S.; Anguera, A.; Cusso, X.; Balanzo, J.; et al. Norfloxacin prevents bacterial infection in cirrhotics with gastrointestinal hemorrhage. Gastroenterology 1992, 103, 1267–1272. [Google Scholar] [CrossRef]
- Grange, J.D.; Roulot, D.; Pelletier, G.; Pariente, E.A.; Denis, J.; Ink, O.; Blanc, P.; Richardet, J.P.; Vinel, J.P.; Delisle, F.; et al. Norfloxacin primary prophylaxis of bacterial infections in cirrhotic patients with ascites: A double-blind randomized trial. J. Hepatol. 1998, 29, 430–436. [Google Scholar] [CrossRef]
- Soares-Weiser, K.; Brezis, M.; Tur-Kaspa, R.; Paul, M.; Yahav, J.; Leibovici, L. Antibiotic prophylaxis of bacterial infections in cirrhotic inpatients: A meta-analysis of randomized controlled trials. Scand. J. Gastroenterol. 2003, 38, 193–200. [Google Scholar] [CrossRef]
- Terg, R.; Fassio, E.; Guevara, M.; Cartier, M.; Longo, C.; Lucero, R.; Landeira, C.; Romero, G.; Dominguez, N.; Munoz, A.; et al. Ciprofloxacin in primary prophylaxis of spontaneous bacterial peritonitis: A randomized, placebo-controlled study. J. Hepatol. 2008, 48, 774–779. [Google Scholar] [CrossRef]
- Ortiz, J.; Vila, M.C.; Soriano, G.; Minana, J.; Gana, J.; Mirelis, B.; Novella, M.T.; Coll, S.; Sabat, M.; Andreu, M.; et al. Infections caused by Escherichia coli resistant to norfloxacin in hospitalized cirrhotic patients. Hepatology 1999, 29, 1064–1069. [Google Scholar] [CrossRef] [PubMed]
- Tandon, P.; Delisle, A.; Topal, J.E.; Garcia-Tsao, G. High prevalence of antibiotic-resistant bacterial infections among patients with cirrhosis at a US liver center. Clin. Gastroenterol. Hepatol. 2012, 10, 1291–1298. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, J.; Prado, V.; Trebicka, J.; Amoros, A.; Gustot, T.; Wiest, R.; Deulofeu, C.; Garcia, E.; Acevedo, J.; Fuhrmann, V.; et al. Multidrug-resistant bacterial infections in patients with decompensated cirrhosis and with acute-on-chronic liver failure in Europe. J. Hepatol. 2019, 70, 398–411. [Google Scholar] [CrossRef]
- Loomba, R.; Wesley, R.; Bain, A.; Csako, G.; Pucino, F. Role of fluoroquinolones in the primary prophylaxis of spontaneous bacterial peritonitis: Meta-analysis. Clin. Gastroenterol. Hepatol. 2009, 7, 487–493. [Google Scholar] [CrossRef]
- Saab, S.; Hernandez, J.C.; Chi, A.C.; Tong, M.J. Oral antibiotic prophylaxis reduces spontaneous bacterial peritonitis occurrence and improves short-term survival in cirrhosis: A meta-analysis. Am. J. Gastroenterol. 2009, 104, 993–1001. [Google Scholar] [CrossRef]
- Komolafe, O.; Roberts, D.; Freeman, S.C.; Wilson, P.; Sutton, A.J.; Cooper, N.J.; Pavlov, C.S.; Milne, E.J.; Hawkins, N.; Cowlin, M.; et al. Antibiotic prophylaxis to prevent spontaneous bacterial peritonitis in people with liver cirrhosis: A network meta-analysis. Cochrane Database Syst. Rev. 2020, 1, CD013125. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, J.; Tandon, P.; Mensa, J.; Garcia-Tsao, G. Antibiotic prophylaxis in cirrhosis: Good and bad. Hepatology 2016, 63, 2019–2031. [Google Scholar] [CrossRef] [PubMed]
- Jalan, R.; Fernandez, J.; Wiest, R.; Schnabl, B.; Moreau, R.; Angeli, P.; Stadlbauer, V.; Gustot, T.; Bernardi, M.; Canton, R.; et al. Bacterial infections in cirrhosis: A position statement based on the EASL Special Conference 2013. J. Hepatol. 2014, 60, 1310–1324. [Google Scholar] [CrossRef]
- Hou, M.C.; Lin, H.C.; Liu, T.T.; Kuo, B.I.; Lee, F.Y.; Chang, F.Y.; Lee, S.D. Antibiotic prophylaxis after endoscopic therapy prevents rebleeding in acute variceal hemorrhage: A randomized trial. Hepatology 2004, 39, 746–753. [Google Scholar] [CrossRef] [PubMed]
- Chavez-Tapia, N.C.; Barrientos-Gutierrez, T.; Tellez-Avila, F.; Soares-Weiser, K.; Mendez-Sanchez, N.; Gluud, C.; Uribe, M. Meta-analysis: Antibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleeding—An updated Cochrane review. Aliment. Pharm. 2011, 34, 509–518. [Google Scholar] [CrossRef]
- de Franchis, R.; Bosch, J.; Garcia-Tsao, G.; Reiberger, T.; Ripoll, C.; Baveno, V.I.I.F. Baveno VII—Renewing consensus in portal hypertension. J. Hepatol. 2022, 76, 959–974. [Google Scholar] [CrossRef]
- Garcia-Tsao, G.; Abraldes, J.G.; Berzigotti, A.; Bosch, J. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology 2017, 65, 310–335. [Google Scholar] [CrossRef]
- Bauer, T.M.; Follo, A.; Navasa, M.; Vila, J.; Planas, R.; Clemente, G.; Vargas, V.; Bory, F.; Vaquer, P.; Rodes, J. Daily norfloxacin is more effective than weekly rufloxacin in prevention of spontaneous bacterial peritonitis recurrence. Dig. Dis. Sci. 2002, 47, 1356–1361. [Google Scholar] [CrossRef]
- Goel, A.; Rahim, U.; Nguyen, L.H.; Stave, C.; Nguyen, M.H. Systematic review with meta-analysis: Rifaximin for the prophylaxis of spontaneous bacterial peritonitis. Aliment. Pharmacol. Ther. 2017, 46, 1029–1036. [Google Scholar] [CrossRef]
- Terg, R.; Llano, K.; Cobas, S.M.; Brotto, C.; Barrios, A.; Levi, D.; Wasen, W.; Bartellini, M.A. Effects of oral ciprofloxacin on aerobic gram-negative fecal flora in patients with cirrhosis: Results of short- and long-term administration, with daily and weekly dosages. J. Hepatol. 1998, 29, 437–442. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Ascites Fluid | Classic SBP | CNNA 1 | MNB 2 |
|---|---|---|---|
| PMN count (cells/mm3) | ≥250 | ≥250 | <250 |
| Ascites culture | positive | negative | positive |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.-H.; Lee, C.-H.; Chang, C. Spontaneous Bacterial Peritonitis in Decompensated Liver Cirrhosis—A Literature Review. Livers 2022, 2, 214-232. https://doi.org/10.3390/livers2030018
Huang C-H, Lee C-H, Chang C. Spontaneous Bacterial Peritonitis in Decompensated Liver Cirrhosis—A Literature Review. Livers. 2022; 2(3):214-232. https://doi.org/10.3390/livers2030018
Chicago/Turabian StyleHuang, Chien-Hao, Chen-Hung Lee, and Ching Chang. 2022. "Spontaneous Bacterial Peritonitis in Decompensated Liver Cirrhosis—A Literature Review" Livers 2, no. 3: 214-232. https://doi.org/10.3390/livers2030018
APA StyleHuang, C.-H., Lee, C.-H., & Chang, C. (2022). Spontaneous Bacterial Peritonitis in Decompensated Liver Cirrhosis—A Literature Review. Livers, 2(3), 214-232. https://doi.org/10.3390/livers2030018