
Biliary hCGβ Is a Potential Novel Marker for Prediction of Biliary Neoplasia in Primary Sclerosing Cholangitis Patients

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Immunofluorometric Assays
2.3. Data Analyses
3. Results
3.1. Patients
3.2. Detection of Markers in Bile
3.3. Biliary hCGβ Levels Are Higher in Patients with Biliary Neoplasia
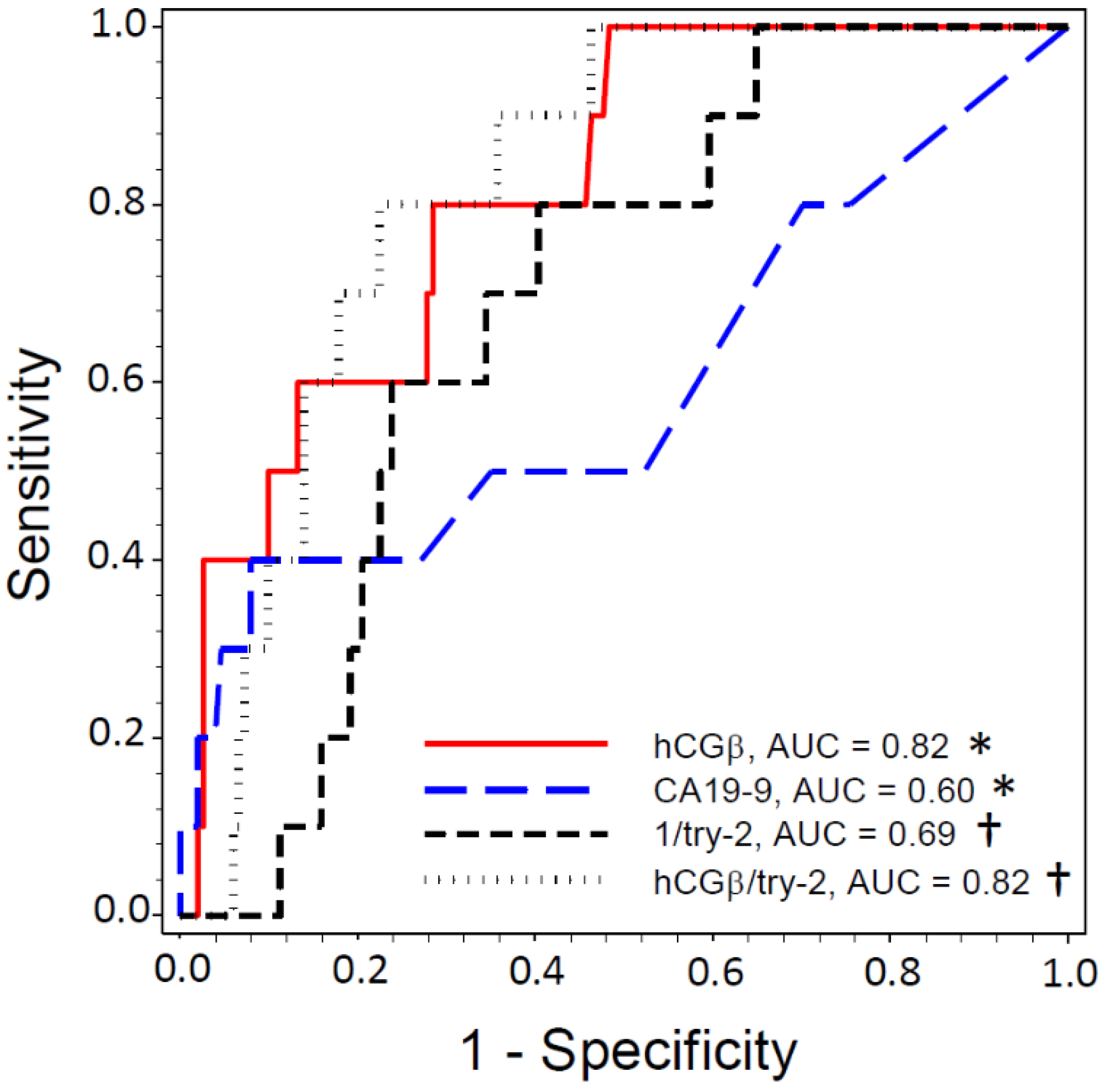
3.4. Biliary hCGβ Has Better Diagnostic Accuracy Than Serum CA19-9 for Detecting Biliary Neoplasia
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dyson, J.K.; Beuers, U.; Jones, D.E.J.; Lohse, A.W.; Hudson, M. Primary sclerosing cholangitis. Lancet 2018, 391, 2547–2559. [Google Scholar] [CrossRef]
- Fung, B.M.; Tabibian, J.H. Cholangiocarcinoma in patients with primary sclerosing cholangitis. Curr. Opin. Gastroenterol. 2020, 36, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.T.; Talwalkar, J.A.; Rosen, C.B.; Smyrk, T.C.; Abraham, S.C. Precancerous bile duct pathology in end-stage primary sclerosing cholangitis, with and without cholangiocarcinoma. Am. J. Surg. Pathol. 2010, 34, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Boonstra, K.; Weersma, R.K.; van Erpecum, K.J.; Rauws, E.A.; Spanier, B.W.M.; Poen, A.C.; van Nieuwkerk, K.M.; Drenth, J.P.; Witteman, B.J.; Tuynman, H.A.; et al. Population-based epidemiology, malignancy risk, and outcome of primary sclerosing cholangitis. Hepatology 2013, 58, 2045–2055. [Google Scholar] [CrossRef]
- Weismüller, T.J.; Trivedi, P.J.; Bergquist, A.; Imam, M.; Lenzen, H.; Ponsioen, C.Y.; Holm, K.; Gotthardt, D.; Färkkilä, M.A.; Marschall, H.U.; et al. Patient Age, Sex, and Inflammatory Bowel Disease Phenotype Associate with Course of Primary Sclerosing Cholangitis. Gastroenterology 2017, 152, 1975–1984.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedström, J.; Haglund, C.; Haapiainen, R.; Stenman, U.-H. Serum trypsinogen-2 and trypsin-2-alpha(1)-antitrypsin complex in malignant and benign digestive-tract diseases. Preferential elevation in patients with cholangiocarcinomas. Int. J. Cancer 1996, 66, 326–331. [Google Scholar] [CrossRef]
- Lempinen, M.; Isoniemi, H.; Mäkisalo, H.; Nordin, A.; Halme, L.; Arola, J.; Höckerstedt, K.; Stenman, U.-H. Enhanced detection of cholangiocarcinoma with serum trypsinogen-2 in patients with severe bile duct strictures. J. Hepatol. 2007, 47, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Paju, A.; Stenman, U.H. Biochemistry and clinical role of trypsinogens and pancreatic secretory trypsin inhibitor. Crit. Rev. Clin. Lab. Sci. 2006, 43, 103–142. [Google Scholar] [CrossRef] [PubMed]
- Räsänen, K.; Itkonen, O.; Koistinen, H.; Stenman, U.-H. Emerging Roles of SPINK1 in Cancer. Clin. Chem. 2016, 62, 449–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stenman, U.H. Biomarker development, from bench to bedside. Crit. Rev. Clin. Lab. Sci. 2016, 53, 69–86. [Google Scholar] [CrossRef]
- Oiva, J.; Itkonen, O.; Koistinen, R.; Hotakainen, K.; Zhang, W.-M.; Kemppainen, E.; Puolakkainen, P.; Kylänpää, L.; Stenman, U.-H.; Koistinen, H. Specific Immunoassay Reveals Increased Serum Trypsinogen 3 in Acute Pancreatitis. Clin. Chem. 2011, 57, 1506–1513. [Google Scholar] [CrossRef] [PubMed]
- Hedström, J.; Haglund, C.; Leinonen, J.; Nordling, S.; Stenman, U.-H.; Hedström, J. Trypsinogen-1, -2 and tumour-associated trypsin-inhibitor in bile and biliary tract tissues from patients with biliary tract diseases and pancreatic carcinomas. Scand. J. Clin. Lab. Investig. 2001, 61, 111–118. [Google Scholar] [PubMed]
- Koistinen, H.; Stenman, U.-H. LH/hCG-receptor independent activities of hCG and hCGβ. In 100 Years of Human Chorionic Gonadotropin: Reviews and New Perspectives, 1st ed.; Cole, L., Butler, S., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 261–268. [Google Scholar]
- Boyd, S.; Tenca, A.; Jokelainen, K.; Mustonen, H.; Krogerus, L.; Arola, J.; Färkkilä, M.A. Screening primary sclerosing cholangitis and biliary dysplasia with endoscopic retrograde cholangiography and brush cytology: Risk factors for biliary neoplasia. Endoscopy 2016, 48, 432–439. [Google Scholar] [CrossRef]
- Itkonen, O.; Kylänpää, L.; Zhang, W.-M.; Stenman, U.-H. Reference intervals for and validation of recalibrated immunoassays for trypsinogen-1 and trypsinogen-2. Clin. Chem. 2012, 58, 1494–1496. [Google Scholar] [CrossRef] [PubMed]
- Janeiro, E.; Guimarães, J.; Stenman, U.-H.; Catarino, M.; Itkonen, O. Validation and comparison of tumor-associated trypsin inhibitor (TATI) immunoassays. Clin. Chim. Acta 2012, 413, 1244–1248. [Google Scholar] [CrossRef] [PubMed]
- Lempiäinen, A.; Stenman, U.-H.; Blomqvist, C.; Hotakainen, K. Free beta-subunit of human chorionic gonadotropin in serum is a diagnostically sensitive marker of seminomatous testicular cancer. Clin. Chem. 2008, 54, 1840–1843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alfthan, H.; Haglund, C.; Dabek, J.; Stenman, U.-H. Concentrations of human chorionic gonadotropin, its β-subunit and the core fragment of the β-subunit in serum and urine of men and nonpregnant women. Clin. Chem. 1992, 38, 1981–1987. [Google Scholar] [CrossRef] [PubMed]
- Louhimo, J.; Nordling, S.; Alfthan, H.; von Boguslawski, K.; Stenman, U.-H.; Haglund, C. Specific staining of human chorionic gonadotropin beta in benign and malignant gastrointestinal tissues with monoclonal antibodies. Histopathology 2001, 38, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, T.; Ushio, M.; Takahashi, S.; Yamagata, W.; Takasaki, Y.; Suzuki, A.; Okawa, Y.; Ochiai, K.; Tomishima, K.; Ishii, S.; et al. Role of Peroral Cholangioscopy in the Diagnosis of Primary Sclerosing Cholangitis. Diagnostics 2020, 10, 268. [Google Scholar] [CrossRef] [PubMed]
- Arnelo, U.; von Seth, E.; Bergquist, A. Prospective Evaluation of the Clinical Utility of Single-Operator Peroral Cholangioscopy in Patients with Primary Sclerosing Cholangitis. Endoscopy 2015, 47, 696–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Vries, A.B.; van der Heide, F.; Ter Steege, R.W.F.; Koornstra, J.J.; Buddingh, K.T.; Gouw, A.S.H.; Weersma, R.K. Limited Diagnostic Accuracy and Clinical Impact of Single-Operator Peroral Cholangioscopy for Indeterminate Biliary Strictures. Endoscopy 2020, 52, 107–114. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| All | PSC a | Biliary Neoplasia b | |||||
|---|---|---|---|---|---|---|---|
| Variables c | No | Yes | p | No | Yes | p | |
| n (%) | 214 (100) | 32 (15) | 182 (85) | 171 (94) | 11 (6.0) | ||
| Categorical data (values represent number (%) of patients. p-values, Fisher’s Exact test, exact 2-sided) | |||||||
| Females (n = 214) d | 91 (43) | 14 (44) | 77 (42) | 1.0 | 75 (44) | 2 (18) | 0.12 |
| Smoking (n = 176) d | 20 (11) | 0 (0) | 20 (12) | 1.0 | 19 (12) | 1 (10) | 1.0 |
| Alcohol (n = 175) d | 124 (71) | 3 (75) | 121 (71) | 1.0 | 116 (72) | 5 (50) | 0.16 |
| IBD (n = 214) d | 141 (66) | 8 (25) | 133 (73) | <0.001 | 122 (71) | 11 (100) | 0.038 |
| Colectomy (n = 197) d | 30 (15) | 3 (18) | 27 (15) | 0.73 | 22 (13) | 5 (45) | 0.013 |
| Continuous data (values represent median (IQR). p-values, Mann–Whitney U test) | |||||||
| Age (years) (n = 214) | 40 (22) | 46 (22) | 39 (22) | 0.062 | 40 (22) | 32 (22) | 0.17 |
| BMI (n = 184) | 25.0 (5.9) | 27.8 (4.5) | 24.6 (5.0) | 0.021 | 25.0 (5.6) | 22.7 (3.4) | 0.008 |
| PSC duration (years) (n = 182) | 4 (7) | - | 4 (7) | 4 (6) | 3 (9) | 0.97 | |
| ERC score (n = 213) | 4 (5) | 2 (3) | 5 (6) | <0.001 | 4 (5) | 10 (4) | <0.001 |
| Laboratory data (median (IQR). p-values, Mann–Whitney U test) | |||||||
| B-Hemoglobin (g/L) (n = 213) | 138 (22) | 137 (29) | 138 (22) | 0.91 | 138 (22) | 135 (20) | 0.27 |
| B-Thrombocytes (109/L) (n = 213) | 248 (104) | 238 (73) | 251 (112) | 0.40 | 244 (103) | 316 (291) | 0.16 |
| P-ALT (U/L) (n = 210) | 31 (36) | 33 (26) | 30 (38) | 0.73 | 30 (36) | 34 (117) | 0.44 |
| P-AST (U/L) (n = 207) | 32 (18) | 29 (13) | 32 (20) | 0.48 | 32 (18) | 34 (98) | 0.16 |
| P-ALP (U/L) (n = 208) | 98 (75) | 80 (46) | 102 (75) | 0.013 | 102 (70) | 203 (430) | 0.15 |
| S-Bilirubin, tot (µmol/L) (n = 209) | 11 (9) | 11 (12) | 11 (9) | 0.46 | 11 (9) | 16 (9) | 0.074 |
| P-Albumin (g/L) (n = 207) | 38.7 (5.5) | 39 (4.9) | 39 (5.5) | 0.71 | 38.7 (5.4) | 37.2 (11.5) | 0.45 |
| fP-Cholesterol (mmol/L) (n = 202) | 4.8 (1.5) | 5.2 (1.7) | 4.6 (1.4) | 0.016 | 4.6 (1.4) | 4.6 (1.3) | 0.63 |
| S-CA19-9 (kU/L) (n = 188) | 6 (9) | 5 (5) | 6 (8) | 0.11 | 6 (8) | 7 (27) | 0.31 |
| Novel biliary markers (median (IQR). p-values, Mann–Whitney U test) | |||||||
| SPINK1 (µg/L) (n = 214) | 26.8 (57.1) | 18.4 (34.5) | 28.4 (62.0) | 0.050 | 27.6 (60.9) | 49.3 (81.4) | 0.10 |
| Trypsin(ogen)-2 (µg/L) (n = 214) | 223 (655) | 177 (441) | 240 (770) | 0.67 | 248 (851) | 55.6 (133) | 0.027 |
| Trypsin(ogen)-3 (µg/L) (n = 212) | 1.02 (11.3) | 0.57 (9.55) | 1.83 (12.2) | 0.53 | 2.70 (12.3) | 0.20 (5.80) | 0.18 |
| hCGβ (pmol/L) (n = 214) | 1.54 (2.68) | 1.49 (2.60) | 1.56 (2.71) | 0.84 | 1.41 (2.48) | 5.51 (11.7) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koistinen, H.; Boyd, S.; Arola, J.; Jokelainen, K.; Koistinen, R.; Lempiäinen, A.; Hotakainen, K.; Stenman, U.-H.; Färkkilä, M. Biliary hCGβ Is a Potential Novel Marker for Prediction of Biliary Neoplasia in Primary Sclerosing Cholangitis Patients. Livers 2021, 1, 322-329. https://doi.org/10.3390/livers1040025
Koistinen H, Boyd S, Arola J, Jokelainen K, Koistinen R, Lempiäinen A, Hotakainen K, Stenman U-H, Färkkilä M. Biliary hCGβ Is a Potential Novel Marker for Prediction of Biliary Neoplasia in Primary Sclerosing Cholangitis Patients. Livers. 2021; 1(4):322-329. https://doi.org/10.3390/livers1040025
Chicago/Turabian StyleKoistinen, Hannu, Sonja Boyd, Johanna Arola, Kalle Jokelainen, Riitta Koistinen, Anna Lempiäinen, Kristina Hotakainen, Ulf-Håkan Stenman, and Martti Färkkilä. 2021. "Biliary hCGβ Is a Potential Novel Marker for Prediction of Biliary Neoplasia in Primary Sclerosing Cholangitis Patients" Livers 1, no. 4: 322-329. https://doi.org/10.3390/livers1040025
APA StyleKoistinen, H., Boyd, S., Arola, J., Jokelainen, K., Koistinen, R., Lempiäinen, A., Hotakainen, K., Stenman, U.-H., & Färkkilä, M. (2021). Biliary hCGβ Is a Potential Novel Marker for Prediction of Biliary Neoplasia in Primary Sclerosing Cholangitis Patients. Livers, 1(4), 322-329. https://doi.org/10.3390/livers1040025