Abstract
Physical inactivity is a significant global health challenge, contributing to increased morbidity and mortality rates. Regular physical activity (PA) improves both physical and mental health, particularly for women, who are at higher risk of chronic conditions associated with inactivity. This study examines barriers and enablers to PA participation among women aged 18–65 in port and coastal communities in East England, a population disproportionately affected by socioeconomic and logistical challenges. Using a mixed-methods convergent parallel design, data were collected from 112 women recruited through local PA and weight loss programmes. Quantitative data were gathered using the International Physical Activity Questionnaire (IPAQ) and the Exercise Benefits and Barriers Scale (EBBS) and analysed using descriptive statistics and logistic regression in SPSS. Qualitative data obtained through scenario-based and open-ended questions were thematically analysed in NVivo. Key findings indicate that healthcare professionals were the primary source of PA information (40%), while health benefits (36%) were the most frequently cited motivator for participation. Barriers to engagement included family responsibilities (45%), low self-confidence (31%), and limited access to facilities (27%). Women with caregiving roles or chronic health conditions were significantly less likely to engage in PA. Qualitative analysis highlighted additional psychological and environmental barriers but also identified motivators such as social support, medical advice, and personal goals. The study concludes that addressing socioenvironmental and psychological barriers to PA requires community-based, multilevel interventions. Leveraging support networks and culturally relevant programming can play a crucial role in sustaining PA engagement among women in these underserved port and coastal communities.
1. Introduction
Physical inactivity remains a critical global health concern, significantly contributing to morbidity and mortality rates worldwide [1,2,3]. Regular physical activity (PA) is vital for both physical and mental well-being, with particular importance for women who face heightened risks for chronic conditions associated with inactivity [4,5]. Engaging in PA reduces the likelihood of obesity, cardiovascular disease, and type 2 diabetes while benefiting mental health by alleviating anxiety and depression [2,6]. For adults aged 18–65, engaging in 30 min of aerobic activity five days weekly to maintain overall health is recommended [7].
In the United Kingdom, communities located in the port and coastal region, such as parts of East England, exhibit notably low PA levels influenced by geographic, socioeconomic, and environmental challenges [8]. Reports from the Northeast Coast Active Partnership (NECAP) reveal barriers such as limited recreational facilities, poverty, and environmental constraints that restrict PA access in these regions [9]. These communities often experience resource limitations, weaker infrastructure, and higher poverty rates than inland areas, disproportionately affecting women, who also contend with cultural and social barriers to PA [9,10]. Specifically, women in the port and coastal communities of East England report lower PA participation rates compared to national averages, with many engaging in less than the recommended weekly PA levels [6,11].
The Together an Active Future (TAAF) programme has emphasised the importance of tailored, community-focused PA interventions, especially for these underserved regions [12]. Integrating cultural and logistical considerations demonstrates the effectiveness of partnerships with local stakeholders to address multilevel PA barriers [13]. Community-led walking programmes, improved infrastructure, and accessible indoor spaces are among the recommended strategies to foster an active lifestyle in these areas [14]. Despite such initiatives, PA participation among women remains low, particularly in rural and coastal regions, due to the unique challenges these settings pose [11]. The intersecting effects of geographic isolation, environmental safety concerns, and limited transportation disproportionately affect women in these communities, contributing to cycles of inactivity and related health inequities [14,15]. Additionally, societal norms and caregiving responsibilities further limit women’s opportunities for PA, necessitating interventions that consider these multifaceted barriers [16].
Evidence indicates that face-to-face interventions can effectively promote PA [17,18]. Nonetheless, social, physical, and cultural contexts profoundly shape PA behaviours, suggesting that multilevel, context-aware approaches may outperform single-strategy interventions [15,16]. For example, ecological frameworks can help address various barriers by creating supportive, accessible environments and actively involving local communities, authorities, and stakeholders to sustain these initiatives [15,16]. The inclusion of gender-specific factors, such as caregiving roles, societal expectations, and perceptions of self-confidence, is essential to designing effective PA interventions for women in such contexts [19,20]. Moreover, addressing practical barriers like lack of childcare and safe exercise environments can enhance participation rates among women [21].
Specifically, women in these communities encounter unique PA challenges, including geographic isolation, unsafe facilities, and inadequate public transportation options [11,22]. These challenges are compounded by urban planning decisions that deprioritise rural areas, contributing to cycles of inactivity and related health issues [9,15]. Although research on PA barriers has been conducted, specific challenges faced by women in coastal communities remain underexplored, with most studies focused on urban or demographic-specific groups, thus overlooking the unique sociocultural and environmental factors in coastal areas [14,23].
Predominantly quantitative research on PA barriers, while informative on participation rates, often overlooks the nuanced social and cultural influences impacting PA. This study employs a mixed-methods approach that integrates quantitative PA behaviour data with qualitative insights into the lived experiences of women in these communities. Variables such as family responsibilities, access to resources, and perceived barriers and motivators are examined to provide a comprehensive understanding of the interplay between socioeconomic, environmental, and cultural factors affecting PA participation.
Research Questions
This study aims to examine the barriers to and enablers of PA participation among women aged 18–65 in the underserved port and coastal communities of East England. Specifically, this study addresses the following research questions. (1) What are the specific barriers to PA participation for women in these communities, and how can these be categorised into actionable themes? (2) What psychological, cultural, and logistical factors enable women to engage in PA despite these barriers? (3) How do healthcare professionals and community stakeholders influence PA behaviours in this population? (4) How do caregiving roles and environmental constraints impact women’s opportunities to participate in PA?
2. Materials and Methods
2.1. Research Design
The study utilises a mixed-methods convergent parallel design, following a pragmatist approach that integrates qualitative and quantitative methods [21]. This design was chosen for its ability to provide a comprehensive understanding of complex behaviours, such as PA, by combining the strengths of qualitative and quantitative approaches. The pragmatist paradigm allowed for flexibility in addressing the research objectives, ensuring practical and contextually relevant insights [24]. This design enabled the simultaneous collection of data from online surveys and structured interviews, capturing a balanced view of divergent and convergent insights from both data types [25]. The mixed-methods approach strengthened the exploration of participants’ experiences and enabled researchers to quantify key trends and relationships, creating a comprehensive analysis framework for validation through larger-scale quantitative measures [26].
2.2. Setting, Recruitment, and Sample Composition
A purposive sampling method was used to recruit 112 adult women aged 18–65 years (mean = 41.3 years, SD = 11.6 years), ensuring that participants met specific inclusion criteria relevant to the study objectives. Participants were required to demonstrate proficiency in written and spoken English and provide written informed consent to participate. The inclusion criteria focused on women who were currently enrolled in a local PA or weight loss programme or those who intended to engage with such initiatives, ensuring that the sample comprised individuals with direct or prospective experience in PA engagement. Exclusion criteria included individuals unable to provide informed consent, those lacking proficiency in English, and those with medical conditions that contraindicated participation in PA, as determined by programme facilitators.
To achieve a representative and contextually relevant sample, the study employed a combination of purposive, convenience, and outreach sampling strategies, ensuring both practical feasibility and diversity in participant characteristics. Convenience sampling [27] was utilised to recruit women already participating in structured PA or weight loss programmes, allowing for efficient and targeted engagement with individuals actively involved in PA activities. This approach enabled access to a readily available participant pool, facilitating recruitment within existing community-based PA networks.
To broaden sample diversity and ensure the inclusion of individuals at varying stages of PA engagement, an outreach dissemination strategy was implemented. Recruitment materials were distributed through partnerships with local health centres, community organisations, and digital platforms such as social media, ensuring that women who were not yet engaged in structured PA programmes but were considering participation had the opportunity to be included. This dual recruitment strategy enhanced the study’s ability to capture insights from both regular participants and potential new adopters of PA, allowing for a more comprehensive understanding of the barriers and enablers influencing PA engagement.
A maximum variation sampling strategy was applied to ensure that the sample reflected a broad spectrum of participant characteristics, particularly in relation to age, socioeconomic status, and cultural background [24,28]. Targeted outreach efforts were tailored to engage individuals from different socioeconomic strata, recognising that factors such as employment status, educational attainment, and access to PA facilities significantly influence participation in health-promoting behaviours. This approach strengthened the study’s external validity [29], ensuring that the findings were applicable to a diverse range of women with varying lived experiences and challenges related to PA engagement.
The final sample composition, as summarised in Table 1, reflects this diversity. Participants’ age distribution, ethnicity, and socioeconomic factors highlight the inclusion of women from varied demographic backgrounds, enhancing the study’s capacity to generate meaningful, context-sensitive insights into the determinants of PA participation. The integration of multiple sampling techniques ensured that the study was methodologically rigorous, balancing pragmatic recruitment approaches [30] with the need for representative diversity, ultimately supporting the study’s broader aim of informing culturally relevant and accessible PA interventions.
Justification for Sample Size
A total sample size of 112 participants was determined based on power analysis for quantitative analyses and data saturation principles for qualitative insights, ensuring methodological rigour while maintaining feasibility. The sample size was carefully selected to balance statistical robustness, practical feasibility, and the need for diverse representation across demographic and socioeconomic groups.
For the quantitative component, power analysis was conducted using G*Power 3.1, ensuring that the study met the standard threshold of 80% power (1 − β = 0.80) at a 5% significance level (α = 0.05) to detect a moderate effect size (d = 0.5) [29,31]. An a priori power analysis for independent t-tests (comparing PA levels between subgroups) and multiple logistic regression models (examining predictors of PA engagement) determined that a minimum of 102 participants was required to detect statistically significant differences while accounting for confounders [30,32]. To mitigate the risk of data loss due to missing responses, a 10% buffer was added, bringing the final target sample size to 112 participants. This sample size allowed for reliable subgroup analyses, ensuring sufficient statistical power to compare active vs. inactive participants and assess barriers across different socioeconomic and ethnic groups [21,27]. Furthermore, multiple regression analyses controlled for key demographic and health-related variables, with an R2 value of 0.31 in Model 1a, demonstrating that 31% of the variance in PA engagement was explained by the selected predictors. This ensured that the study was statistically robust while providing meaningful insights into the relationships between participant characteristics and PA behaviours.
For the qualitative component, the sample size was guided by thematic saturation principles, which suggest that 30–50 interviews are typically sufficient for achieving saturation in health-related qualitative research [21,24]. Saturation was defined as the point at which no new themes emerged from participant narratives. In mixed-methods research, a qualitative sample of 30–40 participants is often sufficient to complement quantitative findings while ensuring rich, contextually grounded insights [21]. To enhance the diversity of perspectives, a maximum variation sampling strategy was applied, ensuring representation across different age groups, socioeconomic strata, and ethnic backgrounds [24]. This strategy ensured that themes related to PA engagement, barriers, and enablers were comprehensively explored across a broad participant base, adding depth to the study’s findings.
2.3. Data Collection and Instruments
Data collection involved the use of validated instruments and integrated qualitative prompts to capture measurable data and participants’ experiences, attitudes, and motivations. The self-administered questionnaires were completed online to enhance accessibility and ensure participant convenience. Data were collected over a four-month period between September and December 2024, accounting for potential seasonal influences on PA levels.
Validity and Reliability of Instruments: This study utilised the adapted International Physical Activity Questionnaire (IPAQ), which has been widely validated for assessing PA levels in diverse populations, demonstrating strong reliability and validity [33]. In addition, we used the Exercise Benefits and Barriers Scale (EBBS), a well-established tool with validated reliability coefficients ranging from 0.86 to 0.96, indicating high internal consistency [34].
Scenario-based and open-ended reflective prompts were embedded after key quantitative items. The development of these scenarios was informed by the participants’ lived environments and existing literature on PA behaviours in similar populations [15,21]. In addition, formative interviews conducted with facilitators of PA programmes to identify common challenges and motivators contributed to the development of these scenarios. These insights were used to create realistic, relatable scenarios. For example, one scenario asked: ‘Imagine you are considering joining a new exercise group in your community. What factors would encourage or discourage you from participating?’.
2.4. Ethical Considerations
Ethical approval for this study was granted by the University of Suffolk Research Ethics Committee (reference ID: RETH24/018), adhering to the Declaration of Helsinki and the General Data Protection Regulation to protect participant rights, privacy, and welfare [35]. Participants were provided with detailed information on their rights, including the ability to withdraw at any stage without penalty. All responses were anonymised, and identifying information was stored separately on encrypted servers accessible only to authorised researchers.
Participants were initially approached electronically through platforms such as email and social media to maximise accessibility. Detailed participant information sheets and consent forms were emailed to participants, outlining the study’s purpose, potential risks, and benefits, enabling informed consent. Participants reviewed, signed, and returned consent forms electronically before beginning the questionnaire or interview.
Sensitive sections, such as barriers to PA, included available support resources to address potential discomfort. These measures ensured ethical integrity, transparency, and participant protection throughout the study [36].
2.5. Rigour
To ensure rigour, several strategies were employed to enhance credibility, validity, and transparency. Triangulation was achieved by integrating quantitative and qualitative findings, validating insights through multiple sources, and enhancing the study’s overall validity [37]. An audit trail documented every step of the research process, including methodological choices, coding decisions, and data analysis, ensuring transparency and enabling external reviewers to independently trace and evaluate findings [38].
Bias mitigation strategies included (1) triangulation of data sources, combining multiple methods and perspectives to reduce bias; (2) pilot testing of instruments with a small subset of participants to identify and address potential biases in the phrasing of questions or scenarios; (3) blind coding of qualitative responses by the two researchers to ensure impartiality and consistency in thematic analysis.
2.6. Data Analysis
Data analysis involved both quantitative and qualitative methods to provide a comprehensive understanding of participants’ PA behaviours. Quantitative data were analysed to identify trends, relationships, and predictors of PA levels, while qualitative data were thematically analysed to explore participants’ experiences, barriers, and motivators. The findings from both data types were then integrated to achieve a holistic interpretation [28].
2.7. Quantitative Data Analysis
Quantitative data were analysed using SPSS and R, selected for their user-friendliness and flexibility with complex datasets [31]. Descriptive statistics summarised PA levels, barriers, and socioeconomic status (Figure 1a,b). Inferential tests, including logistic regression, explored associations between variables, such as the relationships between PA barriers and demographic characteristics [32]. Effect sizes (R2 values) were reported alongside regression analyses to indicate the proportion of variance explained by the independent variables. These values provide an understanding of the strength and practical significance of the relationships observed. For example, in the regression model assessing predictors of PA levels, the R-squared value was 0.28, indicating that 28% of the variance in PA levels could be explained by the included predictors.
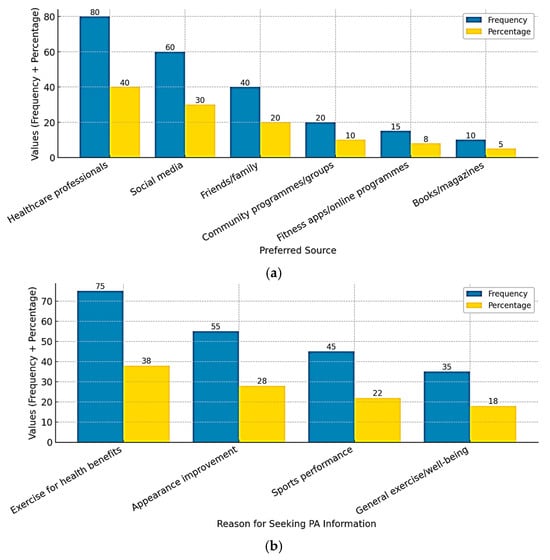
Figure 1.
(a) Preferred Sources for PA Information. (b) Reasons for Seeking PA information.
Visualisations in R, such as bubble charts, presented trends, making complex results more accessible for interpretation and linking them to research objectives [32]. Regression analysis further investigated the predictors of PA levels and barriers while controlling for confounders identified in the initial model (Figure 1 Statistical significance was set at p < 0.05, ensuring the reliability of the results [30]).
2.8. Qualitative Data Analysis
Qualitative data were analysed using thematic analysis in NVivo, employing an inductive approach to identify patterns within participants’ responses. This approach allowed for the systematic organisation of emerging themes, ensuring that the findings reflected participants’ lived experiences and perceptions regarding PA participation. Thematic analysis followed the six-phase framework proposed by Braun and Clarke [39], which included familiarisation with data, coding, theme development, reviewing, defining, and reporting. Coding was conducted independently by two researchers to enhance credibility and inter-coder reliability, ensuring that themes were consistently derived from the data.
2.9. Integrating Quantitative and Qualitative Findings
NVivo’s matrix coding query feature enabled the integration of qualitative insights with quantitative findings and the alignment of thematic data with quantitative metrics [40]. This mixed-methods integration allowed for a richer interpretation of PA behaviours and barriers, contextualising statistical trends with participant narratives, enhancing the study’s overall validity and providing robust, nuanced insights [15]. This approach, supported by tailored software, strengthens the study’s capacity to address complex research questions holistically, merging measurable outcomes with personal experiences in a structured manner [39,41].
3. Results
The findings are structured to address the key research questions, presenting baseline PA levels, sources and motivations for seeking PA information, barriers to PA, and the associations between these variables and PA behaviour. A detailed analysis of age-group differences in motivations, barriers, and enablers is also included, alongside logistic regression models identifying significant predictors of PA behaviour. This section integrates quantitative data from validated instruments and qualitative insights to provide a nuanced perspective on the interplay of psychological, social, and environmental factors influencing PA participation.
3.1. Quantitative
The quantitative analysis provides an overview of participant characteristics, PA behaviours, and associated barriers. Table 1 summarises the demographic characteristics of the participants, providing context for the subsequent analyses of PA levels, motivators, and barriers.

Table 1.
Participant demographic characteristics (n = 112).
These demographic insights are crucial for understanding the variability in PA participation, as factors such as age, socioeconomic status, and chronic health conditions influence engagement in PA programmes. For instance, 62% of participants reported having a chronic health condition, which may impact PA participation, while only 30% had limited access to PA facilities, suggesting that environmental barriers play a role for a subset of the population. The subsequent sections explore how these demographic variables relate to PA engagement, sources of information, and perceived barriers.
3.1.1. Baseline IPAQ and EBBS Scores
Baseline scores from the IPAQ and EBBS provided insight into participants’ activity levels and perceived barriers. The mean total IPAQ score was 1250 MET-minutes/week (SD = 342), with 58% of participants reporting more than 150 min of weekly PA. The EBBS revealed a mean benefit score of 3.8 (SD = 0.4) and a mean barrier score of 2.6 (SD = 0.5), indicating moderate perceptions of benefits and barriers to PA.
Participants were divided into two groups: those meeting the recommended 150 min of weekly PA (n = 65, 58%) and those who did not (n = 47, 42%). Participants in the active group reported higher IPAQ scores (1572 MET-minutes/week) and lower EBBS barrier scores (2.4 vs. 2.9, p < 0.05), suggesting that perceived barriers were inversely related to PA engagement. Conversely, participants in the inactive group reported significantly higher barriers related to time constraints and low self-confidence.
3.1.2. Sources and Motivations for PA Information
As shown in Figure 1a, healthcare professionals were the most cited source of PA information (40%), followed by social media (25%) and friends/family (16%). Participants reported various motivations for seeking PA information, with health benefits being the most common (36%), followed by appearance improvement (27%) and sports performance enhancement (22%) (Figure 1b).
3.1.3. Barriers to PA Participation
Participants reported multiple barriers to PA participation, with time constraints emerging as a predominant challenge. Family responsibilities (45%) and work commitments (34%) were the most frequently cited barriers, followed by environmental challenges such as limited access to facilities (27%) and poor weather conditions (22%). Psychological barriers, including low self-confidence (31%) and fear of injury (22%), further impeded PA engagement. Additionally, financial constraints, such as the cost of gym memberships (24%) and activewear (17%), were notable (Figure 2 and Table 2).
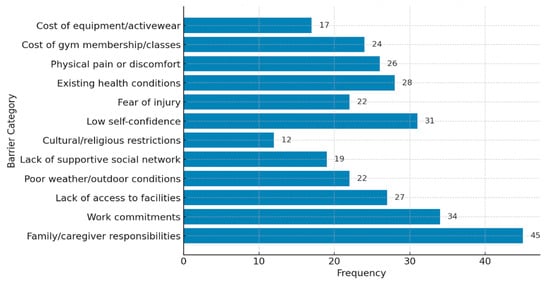
Figure 2.
Barriers to Physical Activity (PA).
Table 2.
Logistic regression analysis of PA-seeking behaviour, barriers to PA, and PA levels.
A deeper examination of the data reveals a noteworthy distinction: although 39% of the participants identified as single, 45% reported family responsibilities as a barrier to PA participation. This distinction suggests that caregiving responsibilities extend beyond traditional family roles, such as parenting, to include broader caregiving duties. For example, single participants frequently reported obligations such as supporting ageing parents, siblings, or extended family members.
Conversely, married participants often cited caregiving for children or dependent family members as their primary responsibility. These findings highlight the complex interplay of family dynamics, caregiving expectations, and cultural norms that influence time availability for PA. For single participants, these caregiving roles may overlap with work-related demands, further compounding the perception of insufficient time for PA.
3.1.4. Associations with PA Behaviour
Logistic regression analysis identified key predictors of PA behaviour using two distinct models. Model 1a focused on specific barriers to PA participation, such as time constraints, environmental factors, social and cultural barriers, psychological barriers, physical health constraints, and financial barriers. On the other hand, Model b examined overall barriers to PA (low vs. high), PA levels (low, moderate, and high), and programme participation (yes or no) as predictors of PA-seeking behaviour.
Both models controlled for participant age and health status to account for their influence on PA participation. As seen in Table 2, family responsibilities significantly reduced the likelihood of engaging in PA (B = −0.567, p = 0.045). Low self-confidence negatively influenced PA behaviour (B = −0.704, p = 0.022). Existing health conditions were a significant physical constraint, decreasing the likelihood of PA participation (B = −0.692, p = 0.012). Financial barriers, such as the cost of gym memberships, also reduced participation (B = −0.523, p = 0.034). The R-squared value for Model 1a was 0.31, indicating that 31% of the variance in PA participation was explained by the included predictors.
Model b shows that participants with low PA levels were significantly less likely to seek PA information compared to those with high PA levels (B = −0.839, p = 0.008; odds ratio = 0.43). Furthermore, participation in PA programmes positively influenced PA-seeking behaviour, with participants more than twice as likely to seek PA information (B = 0.793, p = 0.001; odds ratio = 2.21). Ethnicity was significant, with Black African participants more likely to seek PA information than other ethnic groups (B = 0.472, p = 0.030). The R-squared value for Model b was 0.29, indicating that 29% of the variance in PA-seeking behaviour was explained by the predictors.
Table 2 further presents the odds ratios for two variables—PA-seeking behaviour and barriers to PA (low) across three ethnic groups: Black African, South Asian, and other minority ethnicities, along with their corresponding confidence intervals.
Black African participants had the highest odds ratio (2.2) for PA-seeking behaviour compared to the other groups, indicating they were more than twice as likely to seek PA-related information and participate in PA programmes. The confidence interval (1.5–3.0) confirms statistical significance and highlights the strength of this association.
South Asian participants had an odds ratio of 1.8, slightly lower than Black African participants. The confidence interval (1.2–2.6) suggests a moderately strong association with PA-seeking behaviour.
Other Minority Ethnicities showed an odds ratio of 1.9, with a confidence interval (1.3–2.8). This group also demonstrated a significant tendency to engage in PA-seeking activities, although slightly lower than Black African participants.
For barriers to PA, Black African participants had an odds ratio of 1.5, suggesting a moderate likelihood of experiencing fewer barriers to PA participation. The confidence interval (1.0–2.1) indicates a meaningful, yet less robust, association compared to PA-seeking behaviour. South Asian participants had an odds ratio of 1.2, with a confidence interval (0.9–1.8). The wider confidence interval reflects greater variability in this group, and the association is weaker compared to Black African participants. Other minority ethnicities showed an odds ratio of 1.3, with a confidence interval (0.8–2.0). This group exhibited a similar trend of reduced barriers but with a broader confidence interval, suggesting more variability in experiences.
3.2. Qualitative Findings
The qualitative findings from this study highlight key factors influencing participation in physical activity programmes (Table 3). The participants identified various motivators, including health recommendations from medical professionals, personal weight loss goals, and social influences from friends and family. However, challenges such as time constraints, environmental factors, and psychological barriers also emerged. The importance of support systems was evident, with family, peers, and professionals playing crucial roles in fostering engagement. The participants recognised the benefits of PA, including improvements in physical health, mental well-being, and a sense of community. They also provided recommendations for enhancing participation, such as flexible scheduling, increased access to facilities, integrated mental health support, cultural sensitivity, and the need for enjoyable exercise activities.
Table 3.
Superordinate and subordinate themes with illustrative participant quotes.
3.2.1. Motivators for Participations
The findings reveal diverse motivators that drove women to engage in PA programmes, highlighting a complex interplay of health-related, social, and personal factors.
Health Recommendations
Health recommendations from medical professionals emerged as a significant motivator, with participants viewing PA as a prescribed remedy for managing health conditions. The trust in medical advice acted as a catalyst for initiating lifestyle changes.
“…my doctor recommended I start exercising regularly because of my high blood pressure, and I took that seriously”.(Participant 12)
“After my cholesterol levels went up, my GP advised me to join an exercise class, which I did immediately…”.(Participant 35)
The reliance on healthcare professionals suggests the need for closer collaboration between medical services and community PA programmes. However, the sustainability of these changes may depend on continued support beyond initial recommendations, highlighting an opportunity for integrated follow-ups to maintain engagement.
Weight Loss Goals
Personal milestones, such as weddings or social events, were significant drivers for weight loss and subsequent engagement in PA. These goals provided a sense of urgency and purpose.
“…I wanted to lose weight for my wedding, and this programme appeared to be the perfect opportunity”.(Participant 27)
“…losing weight has always been my goal, but I finally decided to act when I struggled to fit into my old clothes”.(Participant 43)
Weight loss goals are time-sensitive, often tied to specific events, suggesting that programmes can use such moments to recruit and retain participants. However, sustaining motivation post-event requires framing PA as a long-term lifestyle choice rather than a short-term fix.
Social Influences
Social networks played a pivotal role in encouraging participation, with peer success stories and family encouragement acting as strong motivators.
“…my friend had great results from this programme, so I decided to give it a try”.(Participant 19)
“…my sister joined first and convinced me to tag along. We keep each other motivated”.(Participant 8)
Social proof reinforces the ripple effect of one individual’s success inspiring others, underlining the importance of creating visible success stories. Group activities foster accountability, camaraderie, and shared experiences, amplifying motivation and commitment.
3.2.2. Challenges and Barriers
Participants reported a range of challenges that often hindered their ability to sustain consistent PA engagement.
Time Constraints
Juggling multiple responsibilities emerged as a dominant barrier, reflecting the tension between professional, personal, and fitness commitments.
“…balancing work, family, and exercise is truly tough. There’s just not enough time in the day”.(Participant 31)
“…by the time I finish cooking dinner and helping my kids with homework, I have no energy left for exercise”.(Participant 6)
Time constraints reflect the need for flexible programme scheduling, such as early morning or late evening sessions. Digital or at-home workout options could also address these challenges, enabling participants to integrate PA into their routines more seamlessly.
Environmental Factors
Participants highlighted barriers related to weather conditions and inadequate facilities, which disrupted regular exercise routines.
“…it’s hard to stay motivated when it’s raining all the time, and there aren’t many indoor options”.(Participant 21)
“The lack of safe parks or walking tracks in my area makes it difficult to stay active”.(Participant 49)
Environmental barriers emphasise the need for investments in community infrastructure, such as affordable indoor facilities and well-maintained outdoor spaces. Designing weather-resilient spaces can mitigate seasonal disruptions.
Psychological Barriers
Low self-esteem and fear of judgment were pervasive, creating additional emotional hurdles for participants.
“…I always feel like people are judging me when I exercise in public”.(Participant 18)
“I worry about looking silly or out of shape compared to others in the class”.(Participant 44)
These findings highlight the importance of fostering inclusive environments. Programmes should consider introducing beginner-friendly sessions, mentoring systems, or private workout spaces to alleviate anxiety and encourage participation.
3.2.3. Support Systems
Support systems played a crucial role in sustaining participants’ commitment to PA.
Family Support
Family members provided both emotional and practical support, creating a conducive environment for exercise.
“…my husband is very supportive; he even joins me for some of the workouts…”.(Participant 2)
“My teenage daughter keeps reminding me to attend my exercise class, which really helps…”.(Participant 40)
Family involvement enhances accountability and motivation. Programmes could engage family members in joint activities or provide resources to encourage collective participation.
Peer Support
The camaraderie of working out with friends or peers created a sense of belonging and mutual encouragement.
“…working out with friends makes it more fun and less of a chore”.(Participant 29)
“I love the group energy; it keeps me going even on days when I don’t feel like exercising…”.(Participant 11)
Peer-driven motivation is invaluable in fostering adherence. Group-based activities and social networks can be leveraged to strengthen this dynamic, creating a community of support.
Professional Guidance
Participants valued the expertise of trainers, who provided structured guidance and encouragement.
“The trainers are very knowledgeable and always encourage us to push our limits”.(Participant 15)
“Having someone guide me step by step made all the difference”.(Participant 50)
Professional support instils confidence and ensures participants feel supported throughout their fitness journey. Programmes should prioritise hiring skilled trainers and facilitating consistent interactions.
3.2.4. Perceived Benefits
The reported benefits of engaging in PA programmes spanned physical, mental, and social dimensions.
Physical Health Improvements
Tangible health outcomes, such as weight loss and improved vitality, reinforced participants’ commitment.
“I’ve lost weight, my blood pressure is down, and I feel more energetic”.(Participant 9)
“I used to be on the borderline for diabetes, and my doctor always told me I needed to move more. Since joining the sessions, I feel healthier, and my blood sugar levels have improved”.(Participant 33)
Tangible improvements in physical health serve as both immediate rewards and long-term reinforcements for participants’ commitment to PA. These outcomes highlight the importance of goal-setting and regular health assessments within programmes, which can provide participants with visible markers of progress, fostering motivation and adherence.
Mental Well-Being
Participants frequently associated PA with stress relief and improved mental health.
“…exercising regularly has truly helped with my anxiety and stress levels…”.(Participant 7)
“…it gives me clarity and boosts my mood, especially after a tough day”.(Participant 46)
The findings suggest that PA programmes should emphasise their mental health benefits in promotional materials and design. Incorporating mindfulness elements or relaxation techniques alongside physical activities could further address participants’ emotional well-being and attract those seeking holistic health benefits.
Sense of Community
The sense of belonging fostered through group activities created a positive and supportive environment.
“…I’ve made so many new friends through this programme; it feels like a second family…”.(Participant 24)
“…the community aspect keeps me coming back. It’s not just exercise; it’s connection”.(Participant 39)
The social connections formed within PA programmes enhance not only enjoyment but also accountability and consistency in participation. Programmes should actively foster this sense of community by encouraging group-based activities, team challenges, or regular social events to strengthen these bonds and enhance retention.
3.2.5. Recommendations for Improvement
Participants offered suggestions for addressing barriers and enhancing the inclusivity and effectiveness of PA programmes.
Flexible Scheduling
Participants recommended diverse scheduling options to accommodate varying lifestyles.
“…it would be great if there were more evening classes for those of us who work late”.(Participant 10)
“…weekend sessions would really help people who can’t make it during the week…”.(Participant 23)
Flexibility is crucial for reaching a broader audience. Offering sessions at different times, including evenings and weekends, can significantly enhance accessibility and inclusivity.
Increased Access to Facilities
Improving access to safe, affordable exercise spaces was a recurring theme.
“…I believe more indoor facilities would help, especially during bad weather…”.(Participant 19)
“…affordable gyms in the neighbourhood would be a game-changer”.(Participant 37)
Investing in community infrastructure and offering subsidised memberships can alleviate these barriers, particularly for low-income participants.
Mental Health Support
Participants suggested integrating mental health resources to address psychological barriers.
“…may be incorporating mental health workshops would be beneficial”.(Participant 5)
“It would help if someone addressed the fear of judgment we feel while exercising…”.(Participant 22)
Programmes that combine PA with mental health initiatives can create safer and more supportive spaces, fostering participation among those who may feel intimidated or excluded.
Cultural Sensitivity
Tailoring activities to diverse cultural backgrounds was seen as crucial for inclusivity.
“It would be nice if the programmes included activities that are culturally relevant to our community”.(Participant 8)
“Understanding our cultural background can help tailor the interventions better”.(Participant 32)
Customising programmes to reflect cultural preferences can improve engagement and foster inclusivity. Consulting with diverse communities during programme development is essential.
Exercise Enjoyment
The need for fun, engaging activities was emphasised to sustain long-term participation.
“…I think that when exercise feels like play, it’s easier to stay committed”.(Participant 13)
“I love the dance classes because they don’t feel like exercise…”.(Participant 45)
Making exercise fun through dance classes or recreational sports shifts the focus from obligation to enjoyment, increasing the likelihood of continued involvement. This approach could particularly appeal to participants new to structured PA programmes.
4. Discussion
This study explored the barriers to and enablers of PA participation among women in underserved port towns and coastal communities, integrating quantitative and qualitative findings to provide a comprehensive understanding of these issues. Examining the geographical distinctiveness of these communities, the study highlights how environmental, cultural, and psychological factors intersect to shape PA behaviours. Applying Bronfenbrenner’s Ecological Theory offers an enhanced perspective, emphasising the importance of a multilevel approach to understanding and addressing the complex factors influencing PA participation in these settings [42].
Bronfenbrenner’s Ecological Theory [42] provides a robust framework for examining the barriers to PA through the interaction of multiple systems. At the microsystem level, individual factors such as caregiving responsibilities, low self-confidence, and health concerns emerged as significant barriers. Family commitments, in particular, were a dominant challenge reported by participants. These responsibilities vary significantly across life stages, as younger women in the 18–29 age group may be managing childcare or early family responsibilities, while older women in the 50–70 age group often contend with caregiving for ageing relatives. The absence of age-specific analyses in this study represents a missed opportunity to explore how familial barriers evolve over time. Prior studies report that caregiving demands disproportionately affect women’s ability to engage in health-promoting activities, particularly in underserved populations [11,41].
At the mesosystem level, the interplay between individuals and their immediate environments, such as family, peers, and healthcare providers, was evident. Participants highlighted the importance of emotional and practical support from family and friends in enabling PA participation. However, qualitative findings also revealed that the geographic and social isolation characteristic of port towns and coastal communities often limited the availability of such support systems [43]. The absence of robust social networks was exacerbated by traditional gender roles and societal expectations, further isolating women from potential sources of motivation and accountability.
The exosystem, representing broader environmental and infrastructural factors, was especially relevant in this study. Environmental barriers, including poor weather conditions, inadequate recreational facilities, and unreliable public transportation, were consistently identified as significant obstacles. These findings align with previous research highlighting the underinvestment in coastal infrastructure that exacerbates health inequities [15,43]. The limited availability of weather-resilient indoor spaces and safe outdoor facilities in port towns further restricts PA engagement. Furthermore, the financial burden associated with transportation and gym memberships compounds these barriers, particularly for women in lower socioeconomic brackets [41].
At the macrosystem level, cultural norms and societal attitudes were key determinants of PA behaviour. Women in these communities often reported feeling judged or self-conscious when exercising in public, a sentiment consistent with prior studies emphasising the role of societal expectations in perpetuating psychological barriers to PA [44]. Traditional caregiving roles further entrenched these norms, limiting women’s opportunities to prioritise their health. The chronosystem, which captures temporal and life-course influences, was reflected in participants’ narratives of how barriers evolved with age, health status, and family dynamics. This is consistent with research noting that PA behaviours and motivations often shift across the lifespan, influenced by changing personal and social circumstances [45].
Despite these challenges, the study identified significant enablers that reflect the motivations and support systems necessary for fostering PA engagement. Health improvement emerged as the most significant motivator, with participants frequently citing medical recommendations as a catalyst for initiating PA behaviours. These findings align with evidence highlighting health-related goals and advice from trusted healthcare professionals as critical drivers of PA participation [33,34]. The influence of health providers is particularly relevant in coastal settings, where access to community-driven resources may be limited, and medical professionals often represent a primary source of guidance [12].
The role of social support systems was highlighted as a crucial enabler at both the microsystem and mesosystem levels. Participants valued the encouragement of family and peers, which provided accountability and motivation. However, as previously noted, these support systems were less accessible in geographically isolated coastal regions, where tight-knit communities could simultaneously foster and inhibit PA engagement. Previous research similarly emphasised the dual nature of community dynamics in promoting or constraining health behaviours [37].
A key opportunity for addressing barriers and enhancing enablers lies in the integration of lifestyle coaches in partnership with healthcare providers. Lifestyle coaches, through personalised assessments and support, can address behavioural and psychological barriers while fostering sustainable habits. This approach aligns with findings demonstrating the efficacy of tailored interventions in promoting long-term behaviour change [41]. Addressing barriers such as low self-confidence and lack of motivation would enable lifestyle coaches to facilitate the transition from extrinsic to intrinsic motivation, a critical determinant of sustained engagement, as highlighted by Deci and Ryan [46].
Lifestyle coaches can also complement Bronfenbrenner’s ecological model by operating across multiple levels. At the microsystem level, they provide individualised support, helping clients set realistic goals and adopt healthier habits. At the mesosystem and exosystem levels, they collaborate with healthcare providers, community organisations, and local governments to advocate for structural changes, such as improved access to facilities and culturally relevant PA programmes. These efforts align with strategies emphasising the importance of community-driven, multilevel approaches in promoting PA [41].
The sample’s diversity in age, education level, and religious affiliation presents an opportunity to examine how these factors influence PA behaviours. Women with lower educational attainment may face distinct challenges related to health literacy and access to resources, while cultural or religious norms could shape attitudes toward PA. Including these variables as potential confounders in the analysis could provide a more nuanced understanding of the heterogeneity within the sample. For instance, younger women with limited resources may face unique barriers related to caregiving and financial constraints, while older, more educated women may encounter challenges tied to chronic health conditions or societal expectations [37,41].
Geographical distinctiveness plays a critical role in shaping the barriers to and enablers of PA in port towns and coastal communities. Structural inequities, such as underinvestment in infrastructure and limited employment opportunities, exacerbate financial and logistical barriers [15,33]. However, the strong sense of community and cultural identity in these regions presents unique opportunities for fostering sustainable behaviour change. Through the integration of personalised support of lifestyle coaches with the structural and cultural strengths of these communities, interventions may promote intrinsic motivation and lasting lifestyle transformations [47,48].
Lifestyle coaches may further enhance these efforts by framing PA not merely as a goal-oriented activity but as a central component of identity and daily life. This approach shifts the focus from achieving short-term outcomes to embracing a long-term commitment to health and well-being, creating a foundation for consistent PA engagement [49]. The combination of personalised coaching and community-based strategies may offer a promising pathway for addressing the complex interplay of barriers and enablers in geographically distinct regions [50].
The integration of quantitative and qualitative findings highlights the importance of a multilevel approach to understanding PA behaviours in port towns and coastal communities. Quantitative data provided broad insights into the prevalence of barriers and enablers, while qualitative narratives contextualised these findings within the lived experiences of participants. For example, the quantitative results highlighted caregiving responsibilities as a barrier, while qualitative data revealed the emotional burden and cultural expectations underlying these challenges. Similarly, financial barriers were illuminated by participants’ accounts of transportation costs and the affordability of facilities, which are particularly relevant in geographically isolated areas.
Strengths and Limitations
A key strength of this study is its mixed-methods design, which enabled the integration of quantitative and qualitative data to provide a comprehensive understanding of the barriers to and enablers of PA participation among women in underserved port towns and coastal communities. This approach enriched the analysis by capturing both generalisable trends and the nuanced, context-specific experiences of participants, addressing calls for multi-method approaches in public health research [21,28].
The study’s focus on port towns and coastal communities is another notable strength, as these regions are often underrepresented in health research despite their unique geographic, social, and economic challenges. Examining the interplay of environmental, cultural, and psychological factors in these settings, this research addresses a critical gap in the literature and provides valuable insights into the specific needs of underserved populations [15,33].
The application of Bronfenbrenner’s Ecological Theory adds depth to the analysis by framing the findings within a multilevel model that considers individual, social, and structural influences on behaviour. This theoretical grounding allows for a more holistic understanding of the barriers and enablers of PA and highlights the need for multilevel interventions that address these interconnected factors [42].
Another strength is the study’s use of validated measurement tools, including the International Physical Activity Questionnaire (IPAQ) and the Exercise Benefits and Barriers Scale (EBBS). These instruments are widely recognised for their reliability and validity, ensuring the robustness of the quantitative data collected [33,34]. The inclusion of open-ended reflective prompts alongside these tools further enhances the data quality by capturing participants’ subjective experiences and insights.
The study’s emphasis on diversity within the sample, including a wide age range (18–65 years), varying educational levels, and different cultural and religious affiliations, is also commendable. This diversity allows for a broader exploration of the factors influencing PA behaviours, making the findings more applicable to a range of subpopulations within port towns and coastal communities.
Despite its strengths, the study has several limitations that warrant consideration. One key limitation is the lack of subgroup analyses to examine differences in PA barriers and enablers across age groups, educational levels, and religious affiliations. For instance, while the study identifies caregiving responsibilities as a significant barrier, it does not explore how these responsibilities differ by age or life stage. Younger women (18–29 years) may face pressures related to childcare, whereas older women (50–70 years) may contend with caregiving for ageing relatives. Including age as a moderating variable in the regression model could have provided more granular insights into these variations [37,45].
Similarly, the study does not account for potential confounding variables, such as education level or marital status, which could influence perceptions of PA barriers. For example, women with lower educational attainment may face distinct challenges related to health literacy and access to resources, while single or widowed women may encounter additional constraints compared to their married counterparts [41]. Failing to include these variables limits the ability to fully understand the heterogeneity within the sample.
Another limitation is the reliance on self-reported data, which is subject to recall and social desirability biases. Participants may have overestimated their PA levels or underreported barriers to align with perceived social norms. Although validated tools were used, these biases could affect the accuracy of the findings [33,34].
The study’s geographic scope, while focused on an underserved region, may limit the generalisability of the findings to other rural or coastal areas with different demographic or infrastructural characteristics. For instance, port towns in other regions may face varying degrees of isolation, economic opportunity, and access to healthcare, which could influence PA behaviours in distinct ways.
Furthermore, the study’s cross-sectional design restricts its ability to infer causal relationships between identified barriers or enablers and PA participation. Longitudinal research would be needed to determine how these factors evolve over time and whether specific interventions can lead to sustained behaviour change.
While the study identifies the importance of healthcare professionals and community programmes, it does not explicitly evaluate the effectiveness of existing interventions in the region. Assessing these initiatives could have provided actionable insights into best practices and areas for improvement.
5. Conclusions
The study’s findings highlight the complex interplay of caregiving responsibilities, environmental constraints, financial limitations, and psychological barriers while also identifying critical enablers such as health improvement goals, support from family and peers, and the role of healthcare providers.
One of the key takeaways is the importance of addressing these challenges through multilevel, context-sensitive interventions. The application of Bronfenbrenner’s model highlights the need for strategies that operate across various levels of influence, from individual behaviour change to systemic improvements in infrastructure and societal norms. For example, improving access to safe and affordable recreational facilities, fostering robust support networks, and leveraging the expertise of lifestyle coaches in partnership with healthcare providers can help overcome the entrenched barriers faced by women in these communities.
The study also emphasises the value of recognising diversity within the population. While geographic and social isolation are shared challenges, the experiences of women in port towns and coastal communities vary significantly based on age, education, and cultural background. Tailored interventions that address these differences are essential for achieving equitable outcomes. Future research should prioritise subgroup analyses and longitudinal designs to capture the dynamic nature of PA behaviours and assess the long-term impact of targeted interventions.
Despite its limitations, including the absence of subgroup analysis and reliance on self-reported data, this study addresses a critical gap in the literature by focusing on an underserved population often overlooked in health research. Its findings not only deepen our understanding of PA participation in coastal settings but also provide a foundation for designing holistic, community-driven solutions. These insights have practical implications for policymakers, healthcare providers, and community organisations seeking to enhance the health and well-being of women in similar contexts.
Ultimately, the study demonstrates that promoting PA in geographically distinct and underserved regions requires a nuanced approach that bridges the gaps between individual motivation, social support, and systemic change. Leveraging the unique strengths of port towns and coastal communities, such as their cultural identity and community cohesion, and addressing their specific challenges, interventions can foster sustainable behaviour change, improving health outcomes and reducing health disparities in these regions.
Author Contributions
J.O. led the conceptualisation and methodology development of this study. J.O. conducted the investigation, validated the results, and performed data curation and formal analysis. J.O. also drafted the manuscript and supervised the study, providing the necessary resources to support its completion. A.C. contributed to the study by assisting with analysis, proofreading, and editing. Both authors reviewed and approved the final version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the guidelines of the Declaration of Helsinki and was approved by the University of Suffolk’s Research Ethical Approval System (reference ID: RETH24/018). Ethical approval from the Health Research Authority (HRA) was waived, as the study did not involve patients, minors, or clinical trials or pose any risks to participants, in alignment with UK national regulations.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ethical restrictions.
Acknowledgments
We wish to thank all the women who participated in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PA | Physical Activity |
| IPAQ | International Physical Activity Questionnaire |
| EBBS | Exercise Benefits and Barriers Scale |
| SPSS | Statistical Package for the Social Sciences |
| NVivo | Qualitative Data Analysis Software |
| HRA | Health Research Authority |
| NECAP | Northeast Coast Active Partnership |
| TAAF | Together an Active Future |
References
- World Health Organization. Physical Inactivity Remains a Critical Global Health Concern. 2024. Available online: https://www.who.int/news/item/26-06-2024-nearly-1.8-billion-adults-at-risk-of-disease-from-not-doing-enough-physical-activity (accessed on 31 December 2024).
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Mokdad, A.H.; Marks, J.S.; Stroup, D.F.; Gerberding, J.L. Actual causes of death in the United States, 2000. JAMA 2004, 291, 1238–1245. [Google Scholar] [CrossRef]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.E.; Lee, I.M. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef]
- Patterson, R.; McNamara, E.; Tainio, M.; de Sá, T.H.; Smith, A.D.; Sharp, S.J.; Brage, S.; Wijndaele, K. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: A systematic review and dose response meta-analysis. Eur. J. Epidemiol. 2018, 33, 811–829. [Google Scholar] [CrossRef]
- UK Chief Medical Officers. UK Chief Medical Officers’ Physical Activity Guidelines; UK Chief Medical Officers: London, UK, 2019. Available online: https://assets.publishing.service.gov.uk/media/5d839543ed915d52428dc134/uk-chief-medical-officers-physical-activity-guidelines.pdf (accessed on 5 December 2024).
- Sport England. Active Lives Adult Survey: May 2020/21 Report. Available online: https://sportengland-production-files.s3.eu-west-2.amazonaws.com/s3fs-public/2021-10/Active%20Lives%20Adult%20Survey%20May%202020-21%20Report.pdf (accessed on 5 December 2024).
- Almeida, M.; Martinez, L.; Green, J. Physical activity in diverse urban and rural communities. Public Health Rep. 2022, 137, 515–526. [Google Scholar]
- Office for National Statistics. More Adults Are Active in Areas with a Higher Number of Sports Facilities. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/wellbeing/articles/moreadultsareactiveinareaswithahighernumberofsportsfacilities/2024-03-07 (accessed on 5 December 2024).
- Brown, W.J.; Trost, S.G.; Bauman, A.; Mummery, K.; Owen, N. Test-retest reliability of four physical activity measures used in population surveys. J. Sci. Med. Sport. 2018, 5, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Women’s Sport and Fitness Foundation. Changing the Game for Girls. Available online: https://www.wsff.org.uk/system/1/assets/files/000/000/285/285/f4894dccf/original/Changing_The_Game_For_Girls_Final.pdf (accessed on 5 December 2024).
- Together an Active Future. Together an Active Future: Inspiring Active Lives; Together an Active Future: Burnley, UK, 2023. [Google Scholar]
- Together an Active Future. Strategies for Building Active Communities; Together an Active Future: Burnley, UK, 2020. [Google Scholar]
- Foster, C.; Hillsdon, M.; Thorogood, M. Environmental determinants of physical activity and exercise. Public Health Nutr. 2011, 14, 222–229. [Google Scholar] [CrossRef]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An ecological perspective on health promotion programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.; Martin, B.W. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Smith, M.; Hosking, J.; Woodward, A. Can active travel be part of the solution to obesity? Int. J. Behav. Nutr. Phys. Act. 2021, 18, 1–14. [Google Scholar] [CrossRef]
- Lee, R.E.; Cubbin, C. Striding toward social justice: The eco-social and health equity approaches to physical activity research. Sports Med. 2021, 51, 179–190. [Google Scholar] [CrossRef]
- Local Government Association. Physical Activity: Making Our Communities Fitter, Healthier, and More Active; Local Government Association: London, UK, 2024. [Google Scholar]
- Creswell, J.W. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 4th ed.; SAGE Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Ivankova, N.V.; Creswell, J.W.; Stick, S.L. Using mixed-methods sequential explanatory design: From theory to practice. Field Methods 2006, 18, 3–20. [Google Scholar] [CrossRef]
- Jones, P.; Hillsdon, M.; Coombes, E. Environmental correlates of physical activity in England. Health Place. 2020, 16, 929–936. [Google Scholar] [CrossRef]
- Penedo, F.J.; Dahn, J.R. Exercise and well-being: A review of mental and physical health benefits associated with physical activity. Curr. Opin. Psychiatry 2005, 18, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Tashakkori, A.; Teddlie, C. Handbook of Mixed Methods in Social & Behavioural Research; SAGE Publications: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Morse, J.M. Approaches to qualitative-quantitative methodological triangulation. Nurs. Res. 1991, 40, 120–123. [Google Scholar] [CrossRef]
- Palinkas, L.A.; Horwitz, S.M.; Green, C.A.; Wisdom, J.P.; Duan, N.; Hoagwood, K. Purposeful sampling for qualitative data collection and analysis in mixed-method implementation research. Adm. Policy Ment. Health 2015, 42, 533–544. [Google Scholar] [CrossRef]
- Guest, G.; Bunce, A.; Johnson, L. How many interviews are enough? Field Methods 2006, 18, 59–82. [Google Scholar] [CrossRef]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Green, S.B. How many subjects does it take to do a regression analysis? Multivar. Behav. Res. 1991, 26, 499–510. [Google Scholar] [CrossRef] [PubMed]
- Hulley, S.B.; Cummings, S.R.; Browner, W.S.; Grady, D.G.; Newman, T.B. Designing Clinical Research, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 5th ed.; SAGE Publications: London, UK, 2018. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Sechrist, K.R.; Walker, S.N.; Pender, N.J. Development and psychometric evaluation of the Exercise Benefits/Barriers Scale. Res. Nurs. Health 1987, 10, 357–365. [Google Scholar] [CrossRef] [PubMed]
- European Parliament and Council of the European Union. General Data Protection Regulation (GDPR); Regulation (EU) 2016/679; European Union: Brussels, Belgium, 2016; Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:32016R0679 (accessed on 5 December 2024).
- Flick, U. Triangulation in qualitative research. In A Companion to Qualitative Research; Flick, U., von Kardoff, E., Steinke, I., Eds.; SAGE Publications: London, UK, 2004; pp. 178–183. [Google Scholar]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic analysis: Striving to meet the trustworthiness criteria. Int. J. Qual. Methods 2017, 16, 1–13. [Google Scholar] [CrossRef]
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; Sage: Beverly Hills, CA, USA, 1985. [Google Scholar]
- Braun, V.; Clarke, V. Thematic Analysis: A Practical Guide; Sage: London, UK, 2006. [Google Scholar]
- QSR International. NVivo Qualitative Data Analysis Software, Version 12; QSR International: Burlington, MA, USA, 2024. [Google Scholar]
- Stamatakis, E.; Ekelund, U.; Ding, D.; Hamer, M.; Bauman, A.E.; Lee, I.M. Is the time right for quantitative public health guidelines on sitting? A review of sedentary behaviour epidemiology, evidence, and policy implications. Eur. J. Prev. Cardiol. 2019, 26, 818–829. [Google Scholar]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Richmond, C.; Foster, B. Social support and physical activity among adults living in rural and coastal communities. J. Rural. Health 2020, 36, 347–356. [Google Scholar]
- Doherty, A.R.; Kelly, C.; Warwick, L. Women’s barriers to physical activity: A socio-cultural perspective. Sports Med. 2021, 51, 1349–1362. [Google Scholar] [CrossRef]
- Rebar, A.L.; Taylor, A.; Hagger, M.S. Physical activity and mental health: Evidence and challenges. Health Psychol. 2015, 34, 931–941. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. Intrinsic Motivation and Self-Determination in Human Behaviour; Springer: New York, NY, USA, 2000. [Google Scholar]
- Sullivan, K.; Murphy, N.; Bell, S. Barriers and enablers to physical activity in underserved communities: A review of evidence. Public Health 2019, 175, 93–100. [Google Scholar] [CrossRef]
- Warburton, D.E.; Bredin, S.S. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef] [PubMed]
- Ominyi, J.; Clifton, A.; Cushen-Brewster, N. Long-term effectiveness of physical activity interventions for adults across income contexts: A systematic review of strategies and outcomes. Bull. Fac. Phys. Ther. 2024, 29, 90. [Google Scholar] [CrossRef]
- Ekkekakis, P.; Backhouse, S.H.; Gray, C.; Lind, E. Walking is popular among adults but is it enough? A review of evidence. Sports Med. 2008, 38, 863–880. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).