


Prenatal, Delivery and Postpartum Care Experiences among Black Women in Mississippi during COVID-19 Pandemic 2020–2021

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Protection of Human Participants
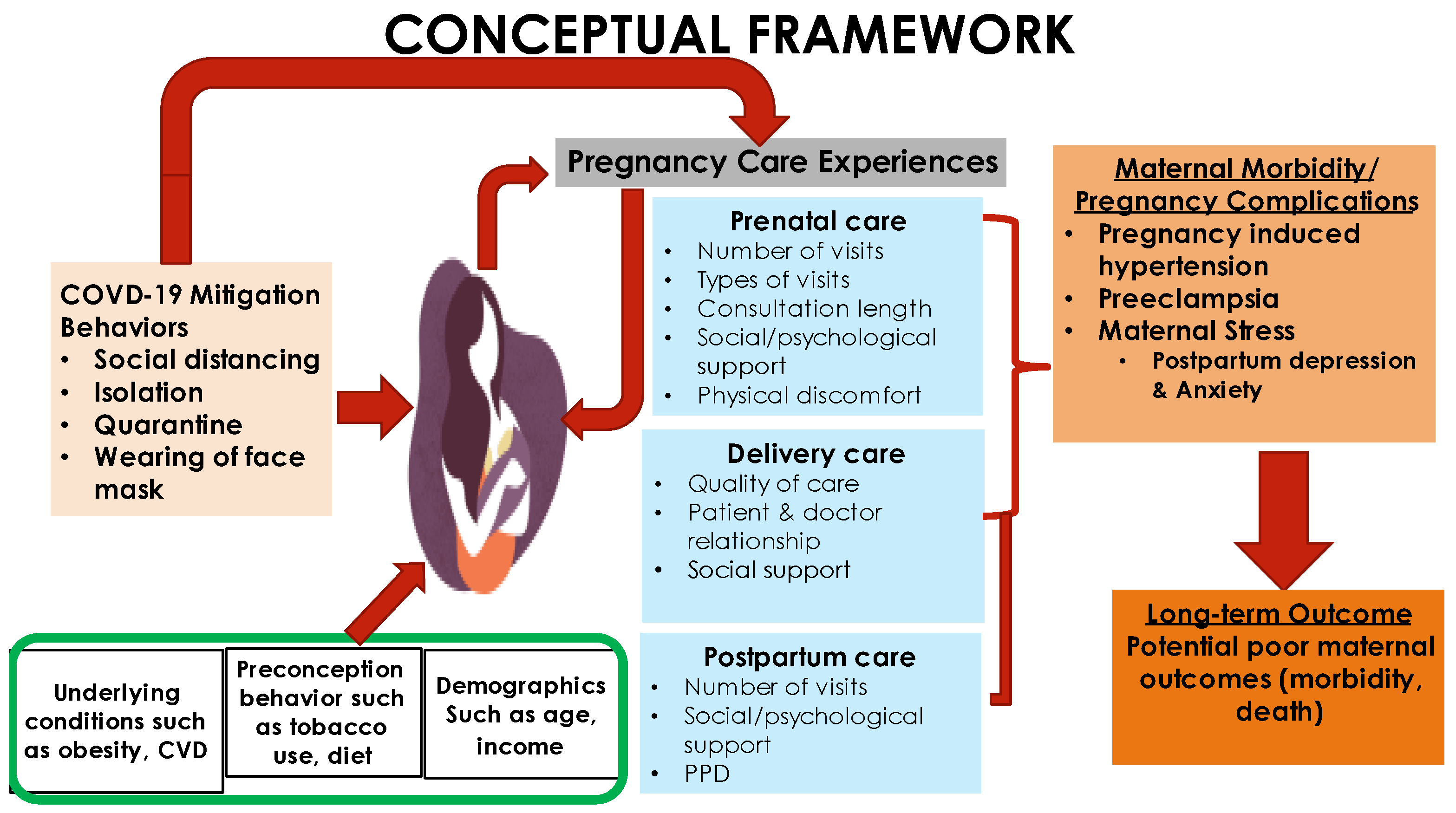
2.2. Maternal Healthcare Framework
- Prenatal care experiences: The pandemic led to limited access to healthcare facilities, which caused limitations and restrictions in prenatal visits [17]. Black postpartum women express their lived experiences with prenatal care during the coronavirus pandemic.
- Delivery care: COVID-19 impacted hospitals by restricting visitation to hospitalized patients to support mandated social distancing. According to [18], most maternity wards allowed solely the woman’s partner in the delivery room. Therefore, a critical element of the MHCF is to have mothers reflect on and describe their childbirth (delivery) experience during the COVID-19 pandemic.
- Postpartum care support: There is a realization that the COVID-19 mitigation strategies were important to curb the spread of coronavirus, but the lack of social support was a non-intended outcome. Most hospitals took precautions by prohibiting visits during postpartum hospital stay [18]. Moreover, the implemented stay-in-place measures prevented visits by family members and friends and limited face-to-face care management by caregivers. These restrictions placed mothers with newborns in an emotionally harmful, psychologically vulnerable space that increased risk of postpartum depression. Therefore, postpartum mothers expressed their lived experiences with the coronavirus pandemic and postpartum care support.
2.3. Study Design
2.4. Population and Sample
2.5. Instrumentation
2.6. Recruitment Strategy
2.7. Data Collection Procedures
2.8. Data Analysis
2.8.1. Quantitative
2.8.2. Qualitative
3. Results
3.1. Demographic Characteristics of Participants
3.2. Participants’ Interview Responses
3.2.1. Theme 1: Stress Related to COVID-19
“Somehow stressed, emotional stress of thinking of the uncertainty of what the virus would do to the child.”
“It was tough, even though I enjoyed lockdown but just being confined to the house with a newborn Umm and still having to like work from home, it was tough. There was moment of frustrations.”
“The COVID-19 restrictions when going to the hospital, it was a little bit stressful.”
“I was kind of nervous about everything,” “it was a little bit stressful.”
“It was a bit stressful you know with the sleepless nights and then trying to get better take care of the baby and do everything by yourself without people around, It was a little you know exhausting.”
“I think it was a little more stressful because I had three kids to take care of, and the mask I was wearing also made it stressful. Very uncomfortable and stressful because at every point in time, we also have to mask up, you’re sleeping and somebody comes into your room, you have to wake up and mask up.”
“Umm stressful, anxious and frustrated and I was moody, very moody but not a bad temper but kind of snappy.”
“Frustrated and stressed and COVID was around and I had to deliver during COVID and I had to dislike wearing face mask.”
“Wearing masks are stressful and uncomfortable and when you’re pregnant, especially when you start getting to the second and third trimester it’s very, when walking you know, sometimes you feel breathless.”
3.2.2. Theme 2: Disruption of Social Life/Support
“They had to limit people coming into the room to just one person to know like I know before the pandemic, you will have your maybe your parents your spouse, but you just have to have only one person present. It was out, personally I wasn’t happy with it because you Know, I like that experience I wanted family and my spouse to be present but it just had to it was one or the other.”
“It was bad to not have, like in during pre-COVID you could have as many people in the room as you want to, but during the COVID I am with one person and you know not having your mom or sister around when you deliver was kind of tough.”
“I feel very much separated, being away from family and friends.”
“I didn’t like the experience that much people where not allow to be with me during delivery, I actually wanted my step mom to be with me because this is my first child.”
“I felt a little I guess alone because people didn’t visit that much and I couldn’t visit as well.”
“I could only choose one person to be with me, but when I delivered him, it was his dad and my mom. It was just weird because I just remember everything, even my friends who have kids you know before COVID, everybody was just in the hospital, you know celebrating the baby and stuff, mine was just so different because you know you can’t invite people because of COVID.”
“Umm not being able to go anywhere and not being able to have anyone come around, and whenever somebody kind of bring something they would leave it on the doorstep, so I feel like I have to play by yourself and like people had to avoid me at all costs, so I felt very isolated.”
“It was a little sad, because due to social distancing I couldn’t go visit people and that made me sad.”
“At home, I felt a little I guess alone because people didn’t visit that much.”
“I feel very much separated, being away from family and friends.”
3.2.3. Theme 3: Disruption of Expected Healthcare Services
“I like the way they handle their social distancing procedures but the waiting period was a long one.”
“What I can say is that they won’t allow you to have your baby until like 39 weeks. They stopped inducing; before COVID-19 they can induce people Okay, but now because of COVID-19, they do not induce people; they want you to get ready, maybe baby almost you know. they will want you to come to the hospital for delivery when you are sure is your due day. This was because they don’t want too much people to be in the hospital at the same time.”
“It was a long wait, the doctor I was seeing had a lot of patients, a patient was about to have a baby so he had to go there, so I either wait or reschedule.”
“They made it in way that once you put to birth within 24 h you are to leave for another person to come in. It was a really tough one.”
“They limit their appointment time or the number of people who are present during each appointment. Just to reduce like exposure to other people may have COVID.”
“I guess unavailability of scheduling by not been able to get a visit within the week I needed to come because of the COVID it may have been delayed, so I will be coming two weeks after.”
“So, I was really concern I don’t want to get COVID while pregnant. My prenatal appointment was cancelled by the Doctor and rescheduled for another date.”
“It was just really the delivery part and about like being sent home too early, because of COVID guidelines. I came to the hospital on 25th night, gave birth to my child on the 26th and I was back home on the 27th. I just feel like there wasn’t enough time to monitor and make sure I am OK before sending me home.”
“I feel badly, because is a new protocols and people don’t stay in the hospital as long as they used to before COVID. Is like you had a baby, are you feeling good? Okay time for you to go home, I feel like I should have stayed longer, but I didn’t. I feel like I was failed honestly because first of all, they didn’t tell me that my blood pressure was high, or what signs to look out for if I need to come back or call, and you know something like that they didn’t educate me on it.”
“I will give it a 7 over 10 because I think they could do better with follow-up. It was just two postpartum follow-ups.”
3.2.4. Theme 4: Uncertainty and Fear about Coronavirus
“I was nervous. I think spend the first three to four months within, unless it was a doctor appointment, because I was afraid of the COVID.”
“Umm it was scary, there was lot of uncertainties if I want to deliver in the hospital, so there was like my anxiety level high at sometimes.”
“I am always scared of getting sick, so it won’t affect my baby, I try to stay six feet away from people.”
“Not wanting to get COVID-19, there was like a barrier to not want to go out or not want to go see the doctor because other people may be sick.”
“Hmm… It was it was scary because you know. It was something new and unfounded and I especially had concerns because, you know being pregnant, even though there was a vaccine, I chose not to take the vaccine, because I did, there was no research on you know the impact of it on pregnant women or the baby.”
“There were some scary parts like getting COVID and all that, which made me to miss some of my doctor’s appointment you know.”
“Somehow stressed, emotional stress of thinking of the uncertainty of what the virus would do to the child.”
3.2.5. Theme 5: COVID-19 Mitigation Strategies-Associated Poor Maternal Health Outcome
“Um I think that’s where my postpartum depression came from, because you know, for a while you can’t leave the house and I actually have a baby, and it was just weird because it felt like this is how is going to be every single day and I barely go to anywhere anyway, because I was still terrified of COVID.”
“I was breastfeeding also in pain after given birth I have forgotten what is called, it had to enter my body for 24 h, so I couldn’t get up for 24 h, it was miserable. I did experience postpartum depression.”
“I had bad postpartum depression, so I was put on some different meds to help with that. I was on Zoloft for a little short period. I was just frustrated at that time because I had to take care of my newborn and my other two children myself.”
“My care was a bit quick they somehow rushed me out of the hospital because of COVID. I was admitted again to the hospital, and I was told that I developed preeclampsia, so I had to stay in hospital for three days, because my blood pressure was extremely high.”
“We should be more proactive with public health; a lot of misinformation that is available so. clinicians should be in the habit of you know. Advising their patients on the truth about COVID. Because there’s a lot of people who still believe that it’s a myth or it’s real.”
“They need to increase the number of hospitals and also the number of healthcare providers. They should improve on the welfare package for insurance.”
“They dig deeper to connect women to the support services that they may be in the future so that whenever you do feel lonely and isolated or frustrated you do not only have people in place to talk to, but you also have access to tools and resources that you may need to help get you through those tough times.”
“Doctors should try and get closer to their patients, try to know them one on one and also try to impact positively in their life.”
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Davis-Floyd, R.; Gutschow, K.; Schwartz, D.A. Pregnancy, Birth and the COVID-19 Pandemic in the United States. Med. Anthropol. 2020, 39, 413–427. [Google Scholar] [CrossRef] [PubMed]
- Eligon, J.; Burch, A.D.; Searcey, D.; Oppel, R.A., Jr. Black Americans face alarming rates of coronavirus infection in some states. N. Y. Times 2020, 7. Available online: https://www.nytimes.com/2020/04/07/us/coronavirus-race.html (accessed on 7 April 2020).
- Center for Disease Control and Prevention. Depression among Women. 2020. Available online: https://www.cdc.gov/reproductivehealth/depression/index.htm (accessed on 23 May 2020).
- Murray, R.; Frank, G. Black Pregnant and COVID-19 Positive. 2020. Available online: https://www.today.com/health/how-coronavirus-affects-black-pregnant-women-t185645 (accessed on 30 June 2020).
- Centers for Disease Control and Prevention (2021). Trends in Out-Of-Hospital Births in the United States, 1990–2012 (No. 2014). US Department of Health and Human Services, National Center for Health Statistics. Available online: https://www.cdc.gov/nchs/products/databriefs/db144.htm (accessed on 6 March 2014).
- Lemke, M.K.; Brown, K.K. Syndemic Perspectives to Guide Black Maternal Health Research and Prevention During the COVID-19 Pandemic. Matern. Child Health J. 2020, 24, 1093–1098. [Google Scholar] [CrossRef]
- Knight, M.; Bunch, K.; Vousden, N.; Morris, E.; Simpson, N.; Gale, C.; O’Brien, P.; Quigley, C.; Brocklehurst, P.; Kurinczuk, J.J.; et al. Characteristics and outcomes of pregnant women admitted to hospital with confirmed SARS-CoV-2 infection in UK: National population-based cohort study. BMJ 2020, 369, m2107. [Google Scholar] [CrossRef]
- Dashraath, P.; Jeslyn, W.J.L.; Karen, L.M.X.; Min, L.L.; Sarah, L.; Biswas, A.; Choolani, M.; Mattar, C.; Lin, S.L. Coronavirus disease 2019 (COVID-19) pandemic and pregnancy. Am. J. Obstet. Gynecol. 2020, 222, 521–531. [Google Scholar] [CrossRef]
- Mein, S.A. COVID-19 and Health Disparities: The reality of “The Great Equalizer”. J. Gen. Intern. Med. 2020, 35, 2439–2440. [Google Scholar] [CrossRef]
- Masjoudi, M.; Aslani, A.; Khazaeian, S.; Fathnezhad-Kazemi, A. Explaining the experience of prenatal care and investigating the association between psychological factors with self-care in pregnant women during COVID-19 pandemic: A mixed method study protocol. Reprod. Health 2020, 17, 1–7. [Google Scholar] [CrossRef]
- Ashokka, B.; Loh, M.H.; Tan, C.H.; Su, L.L.; Young, B.E.; Lye, D.C.; Biswas, A.; Illanes, E.S.; Choolani, M. Care of the pregnant woman with coronavirus disease 2019 in labor and delivery: Anesthesia, emergency cesarean delivery, differential diagnosis in the acutely ill parturient, care of the newborn, and protection of the healthcare personnel. Am. J. Obstet. Gynecol. 2020, 223, 66–74. [Google Scholar] [CrossRef]
- Schwartz, D.A. An analysis of 38 pregnant women with COVID-19, their newborn infants, and maternal-fetal transmission of SARS-CoV-2: Maternal coronavirus infections and pregnancy outcomes. Arch. Pathol. Lab. Med. 2020, 144, 799–805. [Google Scholar] [CrossRef]
- Metz, T.D. LB02 Maternal and neonatal outcomes of pregnant patients with coronavirus disease 2019 (COVID-19): A multistate cohort. Am. J. Obstet. Gynecol. 2021, 224, S722. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, J.; Zhang, C.; Duan, C.; Zhang, H.; Mol, B.W.; Dennis, C.L.; Yin, T.; Yang, J.; Huang, H. Coronavirus disease 2019 among pregnant Chinese women: Case series data on the safety of vaginal birth and breastfeeding. BJOG Int. J. Obstet. Gynaecol. 2020. [Google Scholar] [CrossRef]
- Mississippi State Department of Health. Mississippi Maternal Mortality Report 2013–2016. 2019. Available online: https://msdh.ms.gov/msdhsite/_static/resources/8127.pdf (accessed on 1 April 2019).
- Wagner, E.H. Chronic disease management: What will it take to improve care for chronic illness? Eff. Clin. Pract. 1998, 1, 2–4. [Google Scholar] [PubMed]
- Gomez, H.M.; Mejia Arbelaez, C.; Ocampo Cañas, J.A. A qualitative study of the experiences of pregnant women in accessing healthcare services during the Zika virus epidemic in Villavicencio, Colombia, 2015–2016. Int. J. Gynecol. Obstet. 2020, 148, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Viaux, S.; Maurice, P.; Cohen, D.; Jouannic, J.M. Giving birth under lockdown during the COVID-19 epidemic. J. Gynecol. Obstet. Hum. Reprod. 2020, 49, 101785. [Google Scholar] [CrossRef] [PubMed]
- Bertaux, D. From the life-history approach to the transformation of sociological practice. In Biography and Society: The Life History Approach in the Social Sciences; Sage: London, UK, 1981; pp. 29–45. [Google Scholar]
- Creswell, J.W. Qualitative Inquiry and Research Design: Choosing among Five Approaches; Sage: Thousand Oaks, CA, USA, 1998; p. 135. [Google Scholar]
- Blaylock, R.; Trickey, H.; Sanders, J.; Murphy, C. WRISK voices: A mixed-methods study of women’s experiences of pregnancy-related public health advice and risk messages in the UK. Midwifery 2022, 113, 103433. [Google Scholar] [CrossRef] [PubMed]
- Aydin, R.; Aktaş, S. An investigation of women’s pregnancy experiences during the COVID-19 pandemic: A qualitative study. Int. J. Clin. Pract. 2021, 75, e14418. [Google Scholar] [CrossRef] [PubMed]
- Berthelot, N.; Lemieux, R.; Garon-Bissonnette, J.; Drouin-Maziade, C.; Martel, É.; Maziade, M. Uptrend in distress and psychiatric symptomatology in pregnant women during the coronavirus disease 2019 pandemic. Acta Obstet. Gynecol. Scand. 2020, 99, 848–855. [Google Scholar] [CrossRef]
- Karavadra, B.; Stockl, A.; Prosser-Snelling, E.; Simpson, P.; Morris, E. Women’s perceptions of COVID-19 and their healthcare experiences: A qualitative thematic analysis of a national survey of pregnant women in the United Kingdom. BMC Pregnancy Childbirth 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Sahin, B.M.; Kabakci, E.N. The experiences of pregnant women during the COVID-19 pandemic in Turkey: A qualitative study. Women Birth 2021, 34, 162–169. [Google Scholar] [CrossRef]
- Kotlar, B.; Gerson, E.; Petrillo, S.; Langer, A.; Tiemeier, H. The impact of the COVID-19 pandemic on maternal and perinatal health: A scoping review. Reprod. Health 2021, 18, 1–39. [Google Scholar] [CrossRef]
- Zainiyah, Z.; Susanti, E. Anxiety in Pregnant Women during Coronavirus (COVID-19) Pandemic in East Java, Indonesia. Maj. Kedokt. Bdg. 2020, 52, 149–153. [Google Scholar] [CrossRef]
- Villar, J.; Ariff, S.; Gunier, R.B.; Thiruvengadam, R.; Rauch, S.; Kholin, A.; Ikenoue, S.; Aminu, M.B.; Vecciarelli, C.; Papageorghiou, A.T.; et al. Maternal and neonatal morbidity and mortality among pregnant women with and without COVID-19 infection: The INTERCOVID multinational cohort study. JAMA Paediatr. 2021, 175, 817–826. [Google Scholar] [CrossRef] [PubMed]
- Durankuş, F.; Aksu, E. Effects of the COVID-19 pandemic on anxiety and depressive symptoms in pregnant women: A preliminary study. J. Matern. Fetal Neonatal Med. 2022, 35, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Mortazavi, F.; Ghardashi, F. The lived experiences of pregnant women during COVID-19 pandemic: A descriptive phenomenological study. BMC Pregnancy Childbirth 2021, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Leung, B.M.; Letourneau, N.L.; Giesbrecht, G.F.; Ntanda, H.; Hart, M. Predictors of postpartum depression in partnered mothers and fathers from a longitudinal cohort. Community Ment. Health J. 2017, 53, 420–431. [Google Scholar] [CrossRef]
- Pao, C.; Guintivano, J.; Santos, H.; Meltzer-Brody, S. Postpartum depression and social support in a racially and ethnically diverse population of women. Arch. Women’s Ment. Health 2019, 22, 105–114. [Google Scholar] [CrossRef]
- McLeish, J.; Redshaw, M. Mothers’ accounts of the impact on emotional wellbeing of organised peer support in pregnancy and early parenthood: A qualitative study. BMC Pregnancy Childbirth 2017, 17, 1–14. [Google Scholar] [CrossRef]
- Handley, S.C.; Gallagher, K.; Breden, A.; Lindgren, E.; Lo, J.Y.; Son, M.; Murosko, D.; Dysart, K.; Lorch, S.A.; Burris, H.H.; et al. Birth hospital length of stay and rehospitalization during COVID-19. Pediatrics 2022, 149, e2021053498. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Frequency |
|---|---|
| Age-group | |
| 18–24 years old | 3 |
| 25–34 years old | 5 |
| 35–45 years old | 2 |
| Marital Status | |
| Married | 6 |
| Single | 4 |
| Education Level | |
| Associate degree | 3 |
| College degree | 2 |
| High school degree | 4 |
| Vocational training | 1 |
| Employment Status | |
| Unemployed (not looking for job) | 1 |
| Unemployed (looking for job) | 3 |
| Working full-time | 4 |
| Working part-time | 1 |
| Student | 1 |
| Household Income | |
| $10,000–$19,999 | 1 |
| $20,000–$29,999 | 3 |
| $30,000–$39,999 | 1 |
| $40,000–$59,999 | 5 |
| Insurance Status | |
| Medicaid | 4 |
| Other (marketplace) | 2 |
| Private | 4 |
| Delivery Status | |
| Late preterm | 2 |
| Past-due | 2 |
| Due date | 6 |
| Pre-existing Health Conditions | |
| ADHD | 1 |
| High blood pressure | 1 |
| Incompetence pelvic | 1 |
| None | 7 |
| Themes | Supporting Quotes |
|---|---|
| Stress related to COVID-19 | “Somehow stressed, emotional stress of thinking of the uncertainty of what the virus would do to the child.” “It was tough, even though I enjoyed lockdown but just being confined to the house with a newborn Umm and still having to like work from home, it was tough. There was moment of frustrations.” “The COVID-19 restrictions when going to the hospital, it was a little bit stressful.” “I was kind of nervous about everything”, “it was a little bit stressful.” “It was a bit stressful you know with the sleepless nights and then trying to get better take care of the baby and do everything by yourself without people around, It was a little you know exhausting.” “I think it was a little more stressful because I had three kids to take care of, and the mask I was wearing also made it stressful. very uncomfortable and stressful because at every point in time, we also have to maskup, you’re sleeping and somebody comes into your room, you have to wake up and mask up.” “Umm stressful, anxious and frustrated and “I was moody, very moody but not a bad temper but kind of snappy.” “Frustrated and stressed and COVID was around and I had to deliver during COVID and I had to dislike wearing face mask.” “Wearing masks are stressful and uncomfortable and when you’re pregnant, especially when you start getting to the second and third trimester it’s very, when walking you know, sometimes you feel breathless.” |
| Disruption of social life/support | “They had to limit people coming into the room to just one person to know like I know before the pandemic, you will have your maybe your parents your spouse, but you just have to have only one person present. It was out, personally I wasn’t happy with it because you Know, I like that experience I wanted family and my spouse to be present but it just had to it was one or the other.” “It was bad to not have, like in during pre-COVID you could have as many people in the room as you want to, but during the COVID I am with one person and you know not having your mom or sister around when you deliver was kind of tough.” “I feel very much separated, being away from family and friends.” “I didn’t like the experience that much people where not allow to be with me during delivery, I actually wanted my step mom to be with me because this is my first child.” “I felt a little I guess alone because people didn’t visit that much and I couldn’t visit as well.” “I could only choose one person to be with me, but when I delivered him, it was his dad and my mom. It was just weird because I just remember everything, even my friends who have kids you know before COVID, everybody was just in the hospital, you know celebrating the baby and stuff, mine was just so different because you know you can’t invite people because of COVID.” “Umm not being able to go anywhere and not being able to have anyone come around, and whenever somebody kind of bring something they would leave it on the doorstep, so I feel like I have to play by yourself and like people had to avoid me at all costs, so I felt very isolated.” “It was a little sad, because due to social distancing I couldn’t go visit people and that made me sad.” “At home, I felt a little I guess alone because people didn’t visit that much.” “I feel very much separated, being away from family and friends.” |
| Disruption of expected healthcare services | “I like the way they handle their social distancing procedures but the waiting period was a long one.” “What I can say is that they won’t allow you to have your baby until like 39 weeks. They stopped inducing; before COVID-19 they can induce people Okay, but now because of COVID-19, they do not induce people; they want you to get ready, maybe baby almost you know. they will want you to come to the hospital for delivery when you are sure is your due day. This was because they don’t want too much people to be in the hospital at the same time.” “It was a long wait, the doctor I was seeing had a lot of patients, a patients was about to have a baby so he had to go there, so I either wait or reschedule.” “They made it in way that once you put to birth within 24 h you are to leave for another person to come in. It was a really tough one.” “They limit their appointment time or the number of people who are present during each appointment. Just to reduce like exposure to other people may have COVID.” “I guess unavailability of scheduling by not been able to get a visit within the week I needed to come because of the COVID it may have been delayed, so I will be coming two weeks after.” “So I was really concern I don’t want to get COVID while pregnant. My prenatal appointment was cancelled by the Doctor and rescheduled for another date.” “It was just really the delivery part and about like being sent home too early, because of COVID guidelines. I came to the hospital on 25th night, gave birth to my child on the 26th and I was back home on the 27th. I just feel like there wasn’t enough time to monitor and make sure I am OK before sending me home.” “I feel badly, because is a new protocols and people don’t stay in the hospital as long as they used to before COVID. Is like you had a baby, are you feeling good? Okay time for you to go home, I feel like I should have stayed longer, but I didn’t. I feel like I was failed honestly because first of all, they didn’t tell me that my blood pressure was high, or what signs to look out for if I need to come back or call, and you know something like that they didn’t educate me on it.” “I will give it a 7 over 10 because I think they could do better with follow up. It was just two postpartum follow-ups.” |
| Uncertainty and fear about coronavirus | “I was nervous. I think spend the first three to four months within, unless it was a doctor appointment, because I was afraid of the COVID.” “Umm it was scary, there was lot of uncertainties if I want to deliver in the hospital, so there was like my anxiety level high at sometimes.” “I am always scared of getting sick, so it won’t affect my baby, I try to stay six feet away from people.” “Not wanting to get COVID-19, there was like a barrier to not want to go out or not want to go see the doctor because other people may be sick.” “Hmm…It was it was scary because you know. It was something new and unfounded and I especially had concerns because, you know being pregnant, even though there was a vaccine, I chose not to take the vaccine, because I did, there was no research on you know the impact of it on pregnant women or the baby.” “There were some scary parts like getting COVID and all that, which made me to miss some of my doctor’s appointment you know.” “Somehow stressed, emotional stress of thinking of the uncertainty of what the virus would do to the child.” |
| COVID-19 mitigation strategies-associated poor maternal health outcome | “Um I think that’s where my postpartum depression came from, because you know, for a while you can’t leave the house and I actually have a baby, and it was just weird because it felt like this is how is going to be every single day and I barely go to anywhere anyway, because I was still terrified of COVID.” “I was breastfeeding also in pain after given birth I have forgotten what is called, it had to enter my body for 24 h, so I couldn’t get up for 24 h, it was miserable. I did experience postpartum depression.” “I had bad postpartum depression, so I was put on some different meds to help with that. I was on Zoloft for a little short period. I was just frustrated at that time because I had to take care of my newborn and my other two children myself.” “My care was a bit quick they somehow rushed me out of the hospital because of COVID. I was admitted again to the hospital, and I was told that I developed preeclampsia, so I had to stay in hospital for three days, because my blood pressure was extremely high.” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tangbe, P.E.; Shaw-Ridley, M.; Cannon-Smith, G.; McKinney, S.; Atehortua, N.; Bennett, R. Prenatal, Delivery and Postpartum Care Experiences among Black Women in Mississippi during COVID-19 Pandemic 2020–2021. Women 2023, 3, 295-309. https://doi.org/10.3390/women3020022
Tangbe PE, Shaw-Ridley M, Cannon-Smith G, McKinney S, Atehortua N, Bennett R. Prenatal, Delivery and Postpartum Care Experiences among Black Women in Mississippi during COVID-19 Pandemic 2020–2021. Women. 2023; 3(2):295-309. https://doi.org/10.3390/women3020022
Chicago/Turabian StyleTangbe, Praise Ebimaye, Mary Shaw-Ridley, Gerri Cannon-Smith, Sheila McKinney, Nelson Atehortua, and Russell Bennett. 2023. "Prenatal, Delivery and Postpartum Care Experiences among Black Women in Mississippi during COVID-19 Pandemic 2020–2021" Women 3, no. 2: 295-309. https://doi.org/10.3390/women3020022
APA StyleTangbe, P. E., Shaw-Ridley, M., Cannon-Smith, G., McKinney, S., Atehortua, N., & Bennett, R. (2023). Prenatal, Delivery and Postpartum Care Experiences among Black Women in Mississippi during COVID-19 Pandemic 2020–2021. Women, 3(2), 295-309. https://doi.org/10.3390/women3020022