
Marital Disruption and Disparity in Tobacco Use in Reproductive-Aged Women: Evidence from India


Abstract
1. Introduction
Aims
2. Results
3. Discussion
4. Methods
4.1. Participants and Study Design
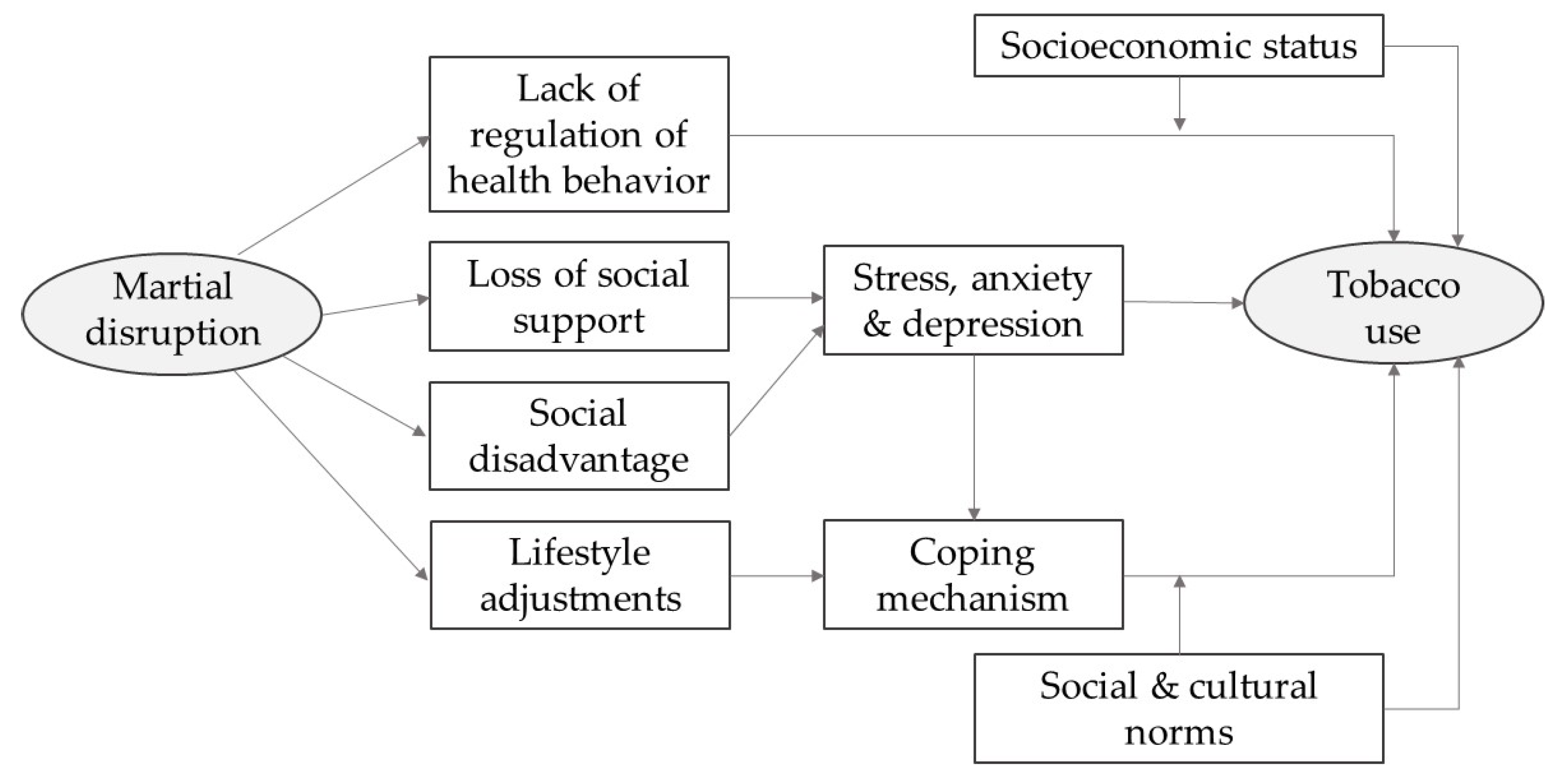
4.2. Conceptual Framework
4.3. Assessment Tools and Outcome Variables
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carr, D.; Bodnar-Deren, S. Gender, Aging and Widowhood. In International Handbook of Population Aging; Uhlenberg, P., Ed.; Springer: Dordrecht, The Netherlands, 2009; pp. 705–728. [Google Scholar] [CrossRef]
- Smith, K.R.; Waitzman, N.J. Double Jeopardy: Interaction Effects of Marital and Poverty Status on the Risk of Mortality. Demography 1994, 31, 487–507. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Gale, J.; Bauman, A.; Phongsavan, P.; Nguyen, B. Effects of Divorce and Widowhood on Subsequent Health Behaviours and Outcomes in a Sample of Middle-Aged and Older Australian Adults. Sci. Rep. 2021, 11, 15237. [Google Scholar] [CrossRef] [PubMed]
- Dhindsa, D.S.; Khambhati, J.; Schultz, W.M.; Tahhan, A.S.; Quyyumi, A.A. Marital Status and Outcomes in Patients with Cardiovascular Disease. Trends Cardiovasc. Med. 2020, 30, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Van de Walle, D. Lasting Welfare Effects of Widowhood in a Poor Country; Policy Research Working Papers; The World Bank: Washington, DC, USA, 2011. [Google Scholar] [CrossRef]
- Dube, M. Isolation and Its Impact on Widows: Insights from Low-Resourced Communities in Binga District, Zimbabwe. Soc. Sci. 2022, 11, 298. [Google Scholar] [CrossRef]
- Thiombiano, B.G.; Schoumaker, B. Effects of Marital Breakdown on Women’s Living Conditions in Burkina Faso. CSP 2012, 39, 1. [Google Scholar] [CrossRef][Green Version]
- Drèze, J.; Srinivasan, P.V. Widowhood and Poverty in Rural India: Some Inferences from Household Survey Data. J. Dev. Econ. 1997, 54, 217–234. [Google Scholar] [CrossRef]
- Lloyd-Sherlock, P.; Corso, B.; Minicuci, N. Widowhood, Socio-Economic Status, Health and Wellbeing in Low and Middle-Income Countries. J. Dev. Stud. 2015, 51, 1374–1388. [Google Scholar] [CrossRef]
- Nnodim, A.U.; Albert, O.C.; Isife, B.I. The Effect of Widowhood on the Income Generation and Well-Being of Rural Women in Rivers State, Nigeria. Dev. Ctry. Stud. 2012, 2, 135–143. [Google Scholar]
- Asiimwe, F.A.; Crankshaw, O. The Impact of Customary Laws on Inheritance: A Case Study of Widows in Urban Uganda. J. Law Confl. Resolut. 2011, 3, 7–13. [Google Scholar]
- Peterman, A. Widowhood and Asset Inheritance in Sub-Saharan Africa: Empirical Evidence from 15 Countries. Dev. Policy Rev. 2012, 30, 543–571. [Google Scholar] [CrossRef]
- Djuikom, M.A.; van de Walle, D. Marital Status and Women’s Nutrition in Africa. World Dev. 2022, 158, 106005. [Google Scholar] [CrossRef]
- Milazzo, A.; van de Walle, D. Nutrition, Religion, and Widowhood in Nigeria. Econ. Dev. Cult. Chang. 2021, 69, 951–1001. [Google Scholar] [CrossRef]
- Lawson, D.W.; Schaffnit, S.B.; Hassan, A.; Ngadaya, E.; Ngowi, B.; Mfinanga, S.G.M.; James, S.; Borgerhoff Mulder, M. Father Absence but Not Fosterage Predicts Food Insecurity, Relative Poverty, and Poor Child Health in Northern Tanzania. Am. J. Hum. Biol. 2017, 29, e22938. [Google Scholar] [CrossRef] [PubMed]
- Alam, N.; Saha, S.K.; Razzaque, A.; van Ginneken, J.K. The Effect of Divorce on Infant Mortality in a Remote Area of Bangladesh. J. Biosoc. Sci. 2001, 33, 271–278. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Tirivayi, N. Widowhood and Access to Health Care: A Population Based Study in Uganda. J. Health Care Poor Underserved 2016, 27, 1555–1566. [Google Scholar] [CrossRef] [PubMed]
- Perkins, J.M.; Lee, H.; James, K.S.; Oh, J.; Krishna, A.; Heo, J.; Lee, J.; Subramanian, S.V. Marital Status, Widowhood Duration, Gender and Health Outcomes: A Cross-Sectional Study among Older Adults in India. BMC Public Health 2016, 16, 1032. [Google Scholar] [CrossRef]
- Myroniuk, T.W. Marital Dissolutions and the Health of Older Individuals in a Rural African Context. GERONB 2016, 72, gbw077. [Google Scholar] [CrossRef]
- Srivastava, S.; Debnath, P.; Shri, N.; Muhammad, T. The Association of Widowhood and Living Alone with Depression among Older Adults in India. Sci. Rep. 2021, 11, 21641. [Google Scholar] [CrossRef]
- Amato, P.R. The Consequences of Divorce for Adults and Children. J. Marriage Fam. 2000, 62, 1269–1287. [Google Scholar] [CrossRef]
- Williams, K. The Transition to Widowhood and the Social Regulation of Health: Consequences for Health and Health Risk Behavior. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2004, 59, S343–S349. [Google Scholar] [CrossRef]
- Leopold, T. Gender Differences in the Consequences of Divorce: A Study of Multiple Outcomes. Demography 2018, 55, 769–797. [Google Scholar] [CrossRef] [PubMed]
- Slopen, N.; Kontos, E.Z.; Ryff, C.D.; Ayanian, J.Z.; Albert, M.A.; Williams, D.R. Psychosocial Stress and Cigarette Smoking Persistence, Cessation, and Relapse over 9–10 Years: A Prospective Study of Middle-Aged Adults in the United States. Cancer Causes Control 2013, 24, 1849–1863. [Google Scholar] [CrossRef] [PubMed]
- Dehle, C.; Larsen, D.; Landers, J.E. Social Support in Marriage. Am. J. Fam. Ther. 2001, 29, 307–324. [Google Scholar] [CrossRef]
- Jackson, E.S.; Tucker, C.M.; Herman, K.C. Health Value, Perceived Social Support, and Health Self-Efficacy as Factors in a Health-Promoting Lifestyle. J. Am. Coll. Health 2007, 56, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.M.; Kowalsky, J.M.; Christian, L.M.; Belury, M.A.; Cole, R.M. Perceived Social Support Predicts Self-Reported and Objective Health and Health Behaviors among Pregnant Women. J. Behav. Med. 2022, 45, 589–602. [Google Scholar] [CrossRef]
- Lakey, B.; Orehek, E. Relational Regulation Theory: A New Approach to Explain the Link between Perceived Social Support and Mental Health. Psychol. Rev. 2011, 118, 482–495. [Google Scholar] [CrossRef]
- Adamczyk, K.; Segrin, C. Perceived Social Support and Mental Health Among Single vs. Partnered Polish Young Adults. Curr. Psychol. 2015, 34, 82–96. [Google Scholar] [CrossRef]
- Croezen, S.; Picavet, H.S.J.; Haveman-Nies, A.; Verschuren, W.M.M.; de Groot, L.C.P.G.M.; van’t Veer, P. Do Positive or Negative Experiences of Social Support Relate to Current and Future Health? Results from the Doetinchem Cohort Study. BMC Public Health 2012, 12, 65. [Google Scholar] [CrossRef]
- Amato, P.R. Research on Divorce: Continuing Trends and New Developments. J. Marriage Fam. 2010, 72, 650–666. [Google Scholar] [CrossRef]
- Cornwell, B. Spousal Network Overlap as a Basis for Spousal Support. J. Marriage Fam. 2012, 74, 229–238. [Google Scholar] [CrossRef]
- Thomas, K.; Nilsson, E.; Festin, K.; Henriksson, P.; Lowén, M.; Löf, M.; Kristenson, M. Associations of Psychosocial Factors with Multiple Health Behaviors: A Population-Based Study of Middle-Aged Men and Women. Int. J. Env. Res. Public Health 2020, 17, 1239. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Veronese, N.; Vancampfort, D.; Prina, A.M.; Lin, P.-Y.; Tseng, P.-T.; Evangelou, E.; Solmi, M.; Kohler, C.; Carvalho, A.F.; et al. Perceived Stress and Smoking across 41 Countries: A Global Perspective across Europe, Africa, Asia and the Americas. Sci. Rep. 2017, 7, 7597. [Google Scholar] [CrossRef] [PubMed]
- Cummings, K.M.; Fong, G.T.; Borland, R. Environmental Influences on Tobacco Use: Evidence from Societal and Community Influences on Tobacco Use and Dependence. Annu. Rev. Clin. Psychol. 2009, 5, 433–458. [Google Scholar] [CrossRef] [PubMed]
- Nystedt, P. Marital Life Course Events and Smoking Behaviour in Sweden 1980–2000. Soc. Sci. Med. 2006, 62, 1427–1442. [Google Scholar] [CrossRef]
- Cho, H.-J.; Khang, Y.-H.; Jun, H.-J.; Kawachi, I. Marital Status and Smoking in Korea: The Influence of Gender and Age. Soc. Sci. Med. 2008, 66, 609–619. [Google Scholar] [CrossRef]
- Bourassa, K.J.; Ruiz, J.M.; Sbarra, D.A. Smoking and Physical Activity Explain the Increased Mortality Risk Following Marital Separation and Divorce: Evidence From the English Longitudinal Study of Ageing. Ann. Behav. Med. 2019, 53, 255–266. [Google Scholar] [CrossRef]
- Perkins, J.M.; Lee, H.-Y.; Lee, J.-K.; Heo, J.; Krishna, A.; Choi, S.; Nam, Y.-S.; Oh, J.; Subramanian, S.V. Widowhood and Alcohol, Tobacco, and Other Drug Use Among Older Adults in India. GERONB 2016, 73, gbw134. [Google Scholar] [CrossRef]
- Loomba Foundation. World Widows Report: A Critical Issue for the Sustainable Development Goals; Loomba Foundation: London, UK, 2016. [Google Scholar]
- Rossouw, L. Socioeconomic Status and Tobacco Consumption: Analyzing Inequalities in China, Ghana, India, Mexico, the Russian Federation and South Africa. Tob. Prev. Cessat. 2021, 7, 47. [Google Scholar] [CrossRef]
- Trivedi, J.; Sareen, H.; Dhyani, M. Psychological Aspects of Widowhood and Divorce. Mens Sana Monogr. 2009, 7, 37. [Google Scholar] [CrossRef]
- Liu, R.X.; Chen, Z. The Effects of Marital Conflict and Marital Disruption on Depressive Affect: A Comparison Between Women In and Out of Poverty. Soc. Sci. Q 2006, 87, 250–271. [Google Scholar] [CrossRef]
- Boateng-Poku, A.; Benca-Bachman, C.E.; Najera, D.D.; Whitfield, K.E.; Taylor, J.L.; Thorpe, R.J.; Palmer, R.H.C. The Role of Social Support on the Effects of Stress and Depression on African American Tobacco and Alcohol Use. Drug Alcohol Depend. 2020, 209, 107926. [Google Scholar] [CrossRef] [PubMed]
- Siedlecki, K.L.; Salthouse, T.A.; Oishi, S.; Jeswani, S. The Relationship Between Social Support and Subjective Well-Being Across Age. Soc. Indic Res. 2014, 117, 561–576. [Google Scholar] [CrossRef] [PubMed]
- Martín-María, N.; Caballero, F.F.; Moreno-Agostino, D.; Olaya, B.; Haro, J.M.; Ayuso-Mateos, J.L.; Miret, M. Relationship between Subjective Well-Being and Healthy Lifestyle Behaviours in Older Adults: A Longitudinal Study. Aging Ment. Health 2020, 24, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Yawson, A.E.; Baddoo, A.; Hagan-Seneadza, N.A.; Calys-Tagoe, B.; Hewlett, S.; Dako-Gyeke, P.; Mensah, G.; Minicuci, N.; Naidoo, N.; Chatterji, S.; et al. Tobacco Use in Older Adults in Ghana: Sociodemographic Characteristics, Health Risks and Subjective Wellbeing. BMC Public Health 2013, 13, 979. [Google Scholar] [CrossRef]
- Aassve, A.; Betti, G.; Mazzuco, S.; Mencarini, L. Marital Disruption and Economic Well-Being: A Comparative Analysis. J. R. Stat. Soc. A 2007, 170, 781–799. [Google Scholar] [CrossRef]
- Siddiqi, N. Gender Inequality as a Social Construction in India: A Phenomenological Enquiry. Women’s Stud. Int. Forum 2021, 86, 102472. [Google Scholar] [CrossRef]
- Allen, L.; Williams, J.; Townsend, N.; Mikkelsen, B.; Roberts, N.; Foster, C.; Wickramasinghe, K. Socioeconomic Status and Non-Communicable Disease Behavioural Risk Factors in Low-Income and Lower-Middle-Income Countries: A Systematic Review. Lancet Glob. Health 2017, 5, e277–e289. [Google Scholar] [CrossRef]
- Subramanian, S.V.; Nandy, S.; Kelly, M.; Gordon, D.; Davey Smith, G. Patterns and Distribution of Tobacco Consumption in India: Cross Sectional Multilevel Evidence from the 1998-9 National Family Health Survey. BMJ 2004, 328, 801–806. [Google Scholar] [CrossRef]
- Singh, A.; Ladusingh, L. Prevalence and Determinants of Tobacco Use in India: Evidence from Recent Global Adult Tobacco Survey Data. PLoS ONE 2014, 9, e114073. [Google Scholar] [CrossRef]
- Palipudi, K.; Rizwan, S.A.; Sinha, D.N.; Andes, L.J.; Amarchand, R.; Krishnan, A.; Asma, S. Prevalence and Sociodemographic Determinants of Tobacco Use in Four Countries of the World Health Organization: South-East Asia Region: Findings from the Global Adult Tobacco Survey. Indian J. Cancer 2014, 51 (Suppl. 1), S24–S32. [Google Scholar] [CrossRef]
- Tiwari, R.V.; Gupta, A.; Agrawal, A.; Gandhi, A.; Gupta, M.; Das, M. Women and Tobacco Use: Discrepancy in the Knowledge, Belief and Behavior towards Tobacco Consumption among Urban and Rural Women in Chhattisgarh, Central India. Asian Pac J. Cancer Prev. 2015, 16, 6365–6373. [Google Scholar] [CrossRef] [PubMed]
- Datta, B.K.; Husain, M.J. Uncontrolled Hypertension among Tobacco-Users: Women of Prime Childbearing Age at Risk in India. BMC Women’s Health 2021, 21, 146. [Google Scholar] [CrossRef]
- Ghosal, S.; Sinha, A.; Kanungo, S.; Pati, S. Declining Trends in Smokeless Tobacco Use among Indian Women: Findings from Global Adult Tobacco Survey I and II. BMC Public Health 2021, 21, 2047. [Google Scholar] [CrossRef] [PubMed]
- Bhan, N.; Karan, A.; Srivastava, S.; Selvaraj, S.; Subramanian, S.V.; Millett, C. Have Socioeconomic Inequalities in Tobacco Use in India Increased Over Time? Trends From the National Sample Surveys (2000–2012). NICTOB 2016, 18, 1711–1718. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, R.; Janssen, F.; Vogt, T. The Progression of the Tobacco Epidemic in India on the National and Regional Level, 1998-2016. BMC Public Health 2022, 22, 317. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Women and Tobacco Use. 2014. Available online: http://apps.who.int/iris/bitstream/handle/10665/204209/Fact_Sheet_TFI_2014_EN_15320.pdf;jsessionid=D1493DAFBB459BE605E7C231CD95E909?sequence=1 (accessed on 2 August 2022).
- Mohan, P.; Lando, H.A.; Panneer, S. Assessment of Tobacco Consumption and Control in India. Indian J. Clin. Med. 2018, 9, 117991611875928. [Google Scholar] [CrossRef]
- Narain, J.P. Public Health Challenges in India: Seizing the Opportunities. Indian J. Community Med. 2016, 41, 85–88. [Google Scholar] [CrossRef]
- Mishra, G.A.; Kulkarni, S.V.; Majmudar, P.V.; Gupta, S.D.; Shastri, S.S. Community-Based Tobacco Cessation Program among Women in Mumbai, India. Indian J. Cancer 2014, 51 (Suppl. 1), S54–S59. [Google Scholar] [CrossRef]
- Patel, S.A.; Dhillon, P.K.; Kondal, D.; Jeemon, P.; Kahol, K.; Manimunda, S.P.; Purty, A.J.; Deshpande, A.; Negi, P.C.; Ladhani, S.; et al. Chronic Disease Concordance within Indian Households: A Cross-Sectional Study. PLoS Med. 2017, 14, e1002395. [Google Scholar] [CrossRef]
- International Institute for Population Sciences; ICF. National Family Health Survey (NFHS-5), 2019–2021; IIPS: Mumbai, India, 2021. [Google Scholar]
- Fluharty, M.; Taylor, A.E.; Grabski, M.; Munafò, M.R. The Association of Cigarette Smoking With Depression and Anxiety: A Systematic Review. Nicotine Tob. Res. 2017, 19, 3–13. [Google Scholar] [CrossRef]
- Lawless, M.H.; Harrison, K.A.; Grandits, G.A.; Eberly, L.E.; Allen, S.S. Perceived Stress and Smoking-Related Behaviors and Symptomatology in Male and Female Smokers. Addict. Behav. 2015, 51, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Nomaguchi, K.M. Are There Race and Gender Differences in the Effect of Marital Dissolution on Depression? Race Gend. Cl. 2005, 12, 11–30. [Google Scholar]
- Kristiansen, C.B.; Kjær, J.N.; Hjorth, P.; Andersen, K.; Prina, A.M. The Association of Time since Spousal Loss and Depression in Widowhood: A Systematic Review and Meta-Analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 781–792. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.; Umberson, D. Marital Status, Marital Transitions, and Health: A Gendered Life Course Perspective. J. Health Soc. Behav. 2004, 45, 81–98. [Google Scholar] [CrossRef]
- Wills, T.A.; Hirky, A.E. Coping and Substance Abuse: A Theoretical Model and Review of the Evidence. In Handbook of Coping: Theory, Research, Applications; John Wiley & Sons: New York, NY, USA, 1996; pp. 279–302. [Google Scholar]
- Skewes, M.C.; Gonzalez, V.M. The Biopsychosocial Model of Addiction. In Principles of Addiction: Comprehensive Addictive Behaviors and Disorders; Academic Press: Amsterdam, The Netherlands, 2013; Volume 1, pp. 61–70. [Google Scholar]
- Garrett, B.E.; Dube, S.R.; Babb, S.; McAfee, T. Addressing the Social Determinants of Health to Reduce Tobacco-Related Disparities. Nicotine Tob. Res. 2015, 17, 892–897. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Share of Women Maritally Disrupted 1 | Share of Women Consuming Tobacco | |||||
|---|---|---|---|---|---|---|
| All | Age 18–34 | Age 35–49 | All | Age 18–34 | Age 35–49 | |
| Currently married | - | - | - | 4.87 | 3.29 | 6.72 |
| (4.76, 4.97) | (3.18, 3.40) | (6.56, 6.89) | ||||
| Widowed/divorced/separated | 5.58 | 2.54 | 8.93 | 9.78 | 7.10 | 10.62 |
| (5.48, 5.68) | (2.45, 2.63) | (8.76, 9.09) | (9.31, 10.25) | (6.36, 7.83) | (10.06, 11.18) | |
| Difference (ΔWDS − ΔMarried) | - | - | - | 4.91 *** | 3.81 *** | 3.90 *** |
| (4.45, 5.38) | (3.08, 4.54) | (3.34, 4.46) | ||||
| Share of All Women Aged 18–49 1 | Share of Women Aged 18–34 | Share of Women Aged 35–49 | ||||
|---|---|---|---|---|---|---|
| Married | WDS | Married | WDS | Married | WDS | |
| N = 510,192 | N = 30,383 | N = 273,443 | N = 7482 | N = 236,749 | N = 22,901 | |
| Education | ||||||
| No education | 27.51 | 42.41 | 17.73 | 25.26 | 39.01 | 47.78 |
| Primary | 13.86 | 17.84 | 12.36 | 17.47 | 15.62 | 17.96 |
| Secondary | 45.7 | 33.58 | 53.45 | 46.68 | 36.57 | 29.48 |
| Higher | 12.93 | 6.17 | 16.45 | 10.58 | 8.79 | 4.78 |
| Wealth index quintiles | ||||||
| Poorest | 18.7 | 21.09 | 20.11 | 24.4 | 17.03 | 20.05 |
| Poorer | 19.91 | 22.32 | 20.87 | 24.92 | 18.79 | 21.51 |
| Middle | 20.43 | 23.6 | 20.69 | 21.61 | 20.12 | 24.22 |
| Richer | 20.81 | 20.14 | 20.49 | 18.17 | 21.2 | 20.75 |
| Richest | 20.14 | 12.85 | 17.84 | 10.89 | 22.86 | 13.47 |
| Religion | ||||||
| Hindu | 81.96 | 82.23 | 81.59 | 79.69 | 82.4 | 83.02 |
| Muslim | 13.12 | 11.09 | 14.05 | 13.32 | 12.02 | 10.39 |
| Christian | 2.19 | 3.43 | 1.88 | 3.5 | 2.55 | 3.41 |
| Other | 2.73 | 3.25 | 2.48 | 3.49 | 3.04 | 3.17 |
| Caste | ||||||
| None | 26.12 | 23.23 | 24.95 | 20.94 | 27.49 | 23.95 |
| Scheduled caste | 21.58 | 24.96 | 22.42 | 26.42 | 20.59 | 24.51 |
| Scheduled tribe | 9.16 | 11.16 | 9.68 | 13.05 | 8.55 | 10.57 |
| Other backward class | 43.14 | 40.64 | 42.95 | 39.59 | 43.37 | 40.97 |
| Residence | ||||||
| Rural | 68.56 | 64.64 | 70.92 | 67.31 | 65.78 | 63.8 |
| Urban | 31.44 | 35.36 | 29.08 | 32.69 | 34.22 | 36.2 |
| All 1 | Currently Married | Maritally Disrupted | |
|---|---|---|---|
| Age | 1.052 *** | 1.050 *** | 1.032 *** |
| (1.050, 1.054) | (1.048, 1.053) | (1.024, 1.039) | |
| Education | |||
| No education | Ref. | Ref. | Ref. |
| Primary | 0.800 *** | 0.799 *** | 0.856 * |
| (0.766, 0.835) | (0.764, 0.836) | (0.742, 0.987) | |
| Secondary | 0.284 *** | 0.286 *** | 0.359 *** |
| (0.273, 0.297) | (0.274, 0.299) | (0.315, 0.409) | |
| Higher | 0.045 *** | 0.045 *** | 0.082 *** |
| (0.039, 0.053) | (0.038, 0.053) | (0.054, 0.123) | |
| Wealth index quintiles | |||
| Poorest | Ref. | Ref. | Ref. |
| Poorer | 0.601 *** | 0.598 *** | 0.626 *** |
| (0.577, 0.627) | (0.573, 0.624) | (0.555, 0.707) | |
| Middle | 0.379 *** | 0.374 *** | 0.411 *** |
| (0.359, 0.399) | (0.354, 0.394) | (0.353, 0.478) | |
| Richer | 0.202 *** | 0.195 *** | 0.281 *** |
| (0.189, 0.215) | (0.182, 0.209) | (0.234, 0.337) | |
| Richest | 0.091 *** | 0.090 *** | 0.130 *** |
| (0.081, 0.102) | (0.080, 0.101) | (0.097, 0.173) | |
| Religion | |||
| Hindu | Ref. | Ref. | Ref. |
| Muslim | 1.029 | 1.042 | 0.988 |
| (0.961, 1.101) | (0.972, 1.118) | (0.825, 1.183) | |
| Christian | 1.693 *** | 1.707 *** | 1.315 ** |
| (1.565, 1.832) | (1.574, 1.851) | (1.116, 1.551) | |
| Other | 0.725 *** | 0.668 *** | 1.084 |
| (0.629, 0.834) | (0.583, 0.766) | (0.697, 1.686) | |
| Caste | |||
| None | Ref. | Ref. | Ref. |
| Scheduled caste | 1.422 *** | 1.425 *** | 1.226 * |
| (1.335, 1.514) | (1.336, 1.520) | (1.033, 1.455) | |
| Scheduled tribe | 3.576 *** | 3.611 *** | 2.906 *** |
| (3.356, 3.811) | (3.382, 3.855) | (2.459, 3.435) | |
| Other backward class | 0.877 *** | 0.887 *** | 0.758 *** |
| (0.828, 0.928) | (0.836, 0.941) | (0.644, 0.892) | |
| Residence | |||
| Rural | Ref. | Ref. | Ref. |
| Urban | 0.499 *** | 0.479 *** | 0.609 *** |
| (0.468, 0.532) | (0.448, 0.512) | (0.529, 0.701) |
| All 1 | Age 18–34 | Age 35–49 | |
|---|---|---|---|
| A. Unadjusted | |||
| Marital disruption | 2.119 *** | 2.245 *** | 1.649 *** |
| (2.008, 2.236) | (2.005, 2.514) | (1.551, 1.752) † | |
| Observations | 540,575 | 280,925 | 259,650 |
| B. Adjusted | |||
| Marital disruption | 1.478 *** | 1.683 *** | 1.455 *** |
| (1.393, 1.569) | (1.484, 1.909) | (1.363, 1.553) † | |
| Observations | 540,575 | 280,925 | 259,650 |
| All 1 | Urban | Rural | Poor | Non-poor | |
|---|---|---|---|---|---|
| A. Not adjusted for age and education | |||||
| Marital disruption | 2.777 *** | 2.695 *** | 2.797 *** | 2.430 *** | 3.399 *** |
| (2.435, 3.201) | (1.996, 3.653) | (2.407, 3.276) | (2.048, 2.917) | (2.743, 4.272) | |
| Observations | 10,551 | 1665 | 8886 | 6067 | 4484 |
| Number of households | 4874 | 757 | 4117 | 2861 | 2013 |
| B. Adjusted for age and education | |||||
| Marital disruption | 1.355 ** | 1.459 | 1.330 ** | 1.270 | 1.477 * |
| (1.123, 1.63) | (0.956, 2.151) | (1.091, 1.684) | (1.001, 1.635) | (1.097, 2.052) | |
| Observations | 10,551 | 1665 | 8886 | 6067 | 4484 |
| Number of households | 4874 | 757 | 4117 | 2861 | 2013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Datta, B.; Ravula, H.; Pollard, E.; Shimul, S. Marital Disruption and Disparity in Tobacco Use in Reproductive-Aged Women: Evidence from India. Women 2022, 2, 371-384. https://doi.org/10.3390/women2040034
Datta B, Ravula H, Pollard E, Shimul S. Marital Disruption and Disparity in Tobacco Use in Reproductive-Aged Women: Evidence from India. Women. 2022; 2(4):371-384. https://doi.org/10.3390/women2040034
Chicago/Turabian StyleDatta, Biplab, Havilah Ravula, Elinita Pollard, and Shafiun Shimul. 2022. "Marital Disruption and Disparity in Tobacco Use in Reproductive-Aged Women: Evidence from India" Women 2, no. 4: 371-384. https://doi.org/10.3390/women2040034
APA StyleDatta, B., Ravula, H., Pollard, E., & Shimul, S. (2022). Marital Disruption and Disparity in Tobacco Use in Reproductive-Aged Women: Evidence from India. Women, 2(4), 371-384. https://doi.org/10.3390/women2040034