
Using the Social-Ecological Model to Understand the Current Perspective of Contraceptive Use in the United States: A Narrative Literature Review



Abstract
:1. Introduction
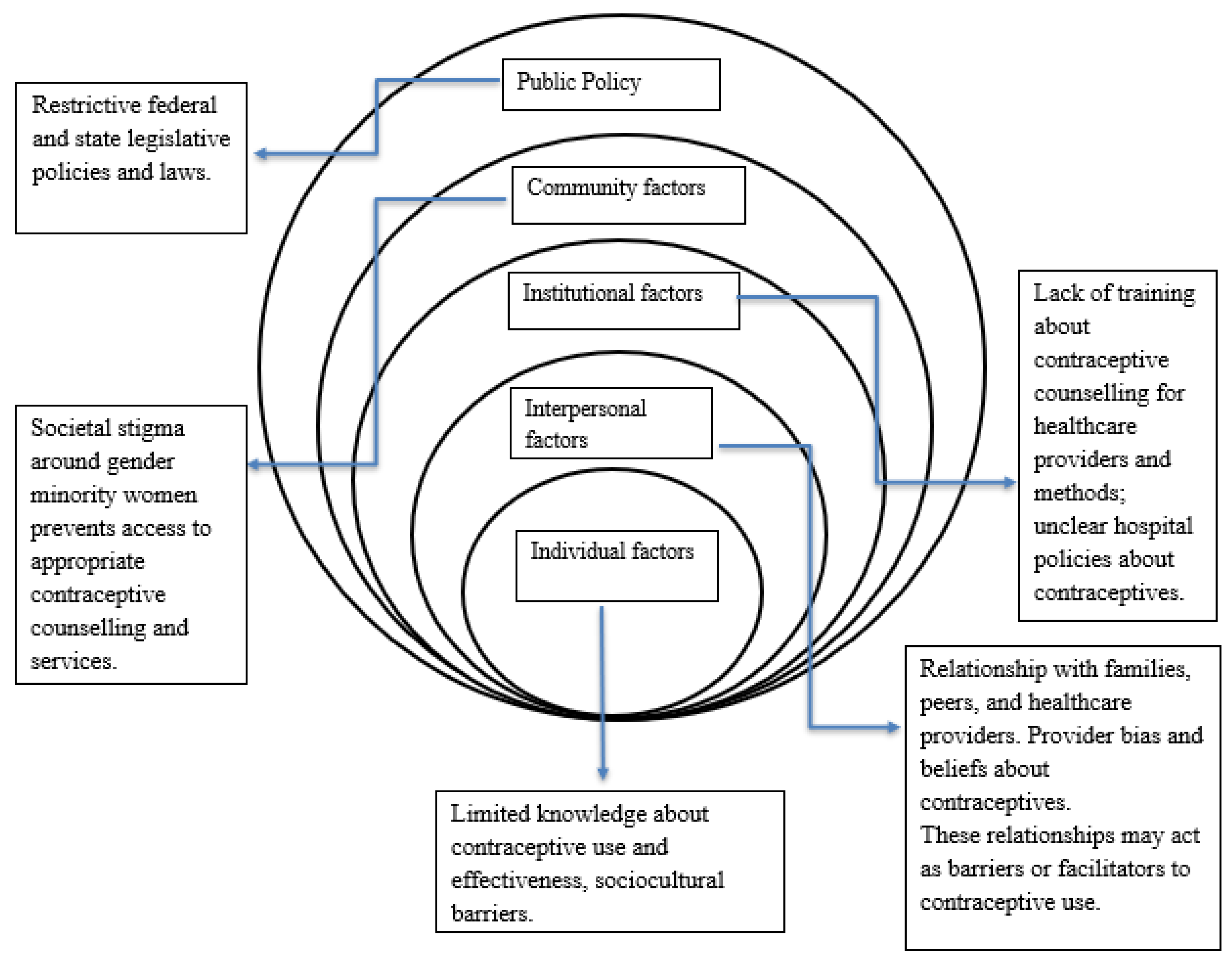
Rationale for Using the Social-Ecological Model
2. Literature Review
Contraception Mechanisms
3. Barriers to Contraceptive Use
3.1. Individual-Level Factors
3.2. Interpersonal-Level Factors
3.3. Institutional-Level Factors
3.4. Community-Level Factors
3.5. Policy-Level Factors
4. Facilitators of Contraceptive Use
5. Recommendations to Increase Contraceptive Use
6. Policy Implications
7. Limitations
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ten Great Public Health Achievements–United States, 1900–1999. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/00056796.htm (accessed on 28 September 2021).
- The Social and Economic Benefits of Women’s Ability to Determine Whether and When to Have Children|Guttmacher Institute. Available online: https://www.guttmacher.org/report/social-and-economic-benefits-womens-ability-determine-whether-and-when-have-children (accessed on 28 September 2021).
- Family Planning/Contraception Methods. Available online: https://www.who.int/news-room/fact-sheets/detail/family-planning-contraception (accessed on 28 September 2021).
- Moving Forward: Family Planning in the Era of Health Reform|Guttmacher Institute. Available online: https://www.guttmacher.org/report/moving-forward-family-planning-era-health-reform (accessed on 28 September 2021).
- Kavanaugh, M.L.; Pliskin, E. Use of Contraception among Reproductive-Aged Women in the United States, 2014 and 2016. F&S Rep. 2020, 1, 83. [Google Scholar] [CrossRef]
- Kavanaugh, M.L.; Jerman, J. Contraceptive Method Use in the United States: Trends and Characteristics between 2008, 2012 and 2014. Contraception 2018, 97, 14–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Products-Data Briefs-Number 388-October 2020. Available online: https://www.cdc.gov/nchs/products/databriefs/db388.htm (accessed on 28 September 2021).
- Daniels, K.; Daugherty, J.; Jones, J. Current contraceptive status among women aged 15-44: United States, 2011–2013. NCHS Data Brief 2014, 173, 1–8. [Google Scholar]
- Abma, J.C.; Martinez, G.M. Sexual Activity and Contraceptive Use among Teenagers in the United States, 2011–2015. Natl. Health Stat. 2017, 104, 1–23. [Google Scholar]
- Birth control methods | Office on Women’s Health. Available online: https://www.womenshealth.gov/a-z-topics/birth-control-methods (accessed on 28 September 2021).
- Contraceptive Needs and Services, 2014 Update | Guttmacher Institute. Available online: https://www.guttmacher.org/report/contraceptive-needs-and-services-2014-update (accessed on 28 September 2021).
- Finer, L.B.; Zolna, M.R. Unintended Pregnancy in the United States: Incidence and Disparities, 2006. Contraception 2011, 84, 478–485. [Google Scholar] [CrossRef] [Green Version]
- Unintended Pregnancy In the United States | Guttmacher Institute. Available online: https://www.guttmacher.org/fact-sheet/unintended-pregnancy-united-states (accessed on 28 September 2021).
- Mcleroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An Ecological Perspective on Health Promotion Programs. Health Educ. Behav. 1988, 15, 351–377. [Google Scholar] [CrossRef]
- Garney, W.; Wilson, K.; Ajayi, K.V.; Panjwani, S.; Love, S.M.; Flores, S.; Garcia, K.; Esquivel, C. Social-Ecological Barriers to Access to Healthcare for Adolescents: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 4138. [Google Scholar] [CrossRef]
- Aura, A.; Sormunen, M.; Tossavainen, K. The Relation of Socio-Ecological Factors to Adolescents’ Health-Related Behaviour: A Literature Review. Health Educ. 2016, 2016, 177–201. [Google Scholar] [CrossRef]
- Guiahi, M. Religious Refusals to Long-Acting Reversible Contraceptives in Catholic Settings: A Call for Evidence. Am. J. Obstet. Gynecol. 2020, 222, S869.e1–S869.e5. [Google Scholar] [CrossRef]
- Hall, K.S.; Ela, E.; Zochowski, M.K.; Caldwell, A.; Moniz, M.; McAndrew, L.; Steel, M.; Challa, S.; Dalton, V.K.; Ernst, S. “I Don’t Know Enough to Feel Comfortable Using Them:” Women’s Knowledge of and Perceived Barriers to Long-Acting Reversible Contraceptives on a College Campus. Contraception 2016, 93, 556–564. [Google Scholar] [CrossRef] [Green Version]
- Raidoo, S.; Kaneshiro, B. Contraception Counseling for Adolescents. Curr. Opin. Obstet. Gynecol. 2017, 29, 310–315. [Google Scholar] [CrossRef]
- Gomez, A.M.; Fuentes, L.; Allina, A. Women or LARC First? Reproductive Autonomy and the Promotion of Long-Acting Contraceptive Methods. Perspect. Sex. Reprod. Health 2014, 46, 171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, S.F.; Strohsnitter, W.; Baecher-Lind, L. Practices and Perceptions among Pediatricians Regarding Adolescent Contraception with Emphasis on Intrauterine Contraception. J. Pediatr. Adolesc. Gynecol. 2013, 26, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Akers, A.Y.; Gold, M.A.; Borrero, S.; Santucci, A.; Schwarz, E.B. Providers’ Perspectives on Challenges to Contraceptive Counseling in Primary Care Settings. J. Women’s Health 2010, 19, 1163–1170. [Google Scholar] [CrossRef]
- Mahony, H.; Spinner, C.; Vamos, C.A.; Daley, E.M. Social Network Influences on Young Women’s Choice to Use Long-Acting Reversible Contraception: A Systematic Review. J. Midwifery Women’s Health 2021, 7. [Google Scholar] [CrossRef]
- Potter, J.E.; Hubert, C.; White, K. The Availability and Use of Postpartum LARC in Mexico and Among Hispanics in the United States. Matern. Child Health J. 2016, 21, 1744–1752. [Google Scholar] [CrossRef] [PubMed]
- Wallace Huff, C.; Potter, J.E.; Hopkins, K. Patients’ Experiences with an Immediate Postpartum Long-Acting Reversible Contraception Program. Women’s Health Issues 2021, 31, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Moniz, M.H.; Roosevelt, L.; Crissman, H.P.; Kobernik, E.K.; Dalton, V.K.; Heisler, M.H.; Low, L.K. Immediate Postpartum Contraception: A Survey Needs Assessment of a National Sample of Midwives. J. Midwifery Women’s Health 2017, 62, 538–544. [Google Scholar] [CrossRef]
- Moniz, M.H.; McEvoy, A.K.; Hofmeister, M.; Plegue, M.; Chang, T. Family Physicians and Provision of Immediate Postpartum Contraception: A Cera Study. Fam. Med. 2017, 49, 600–606. [Google Scholar]
- Rafie, S.; Haycock, M.; Rafie, S.; Yen, S.; Harper, C.C. Direct Pharmacy Access to Hormonal Contraception: California Physician and Advanced Practice Clinician Views. Contraception 2012, 86, 687–693. [Google Scholar] [CrossRef]
- HHiggins, J.A.; Carpenter, E.; Everett, B.G.; Greene, M.Z.; Haider, S.; Hendrick, C.E. Sexual Minority Women and Contraceptive Use: Complex Pathways Between Sexual Orientation and Health Outcomes. Am. J. Public Health 2019, 109, 1680–1686. [Google Scholar] [CrossRef]
- Everett, B.G.; Higgins, J.A.; Haider, S.; Carpenter, E. Do Sexual Minorities Receive Appropriate Sexual and Reproductive Health Care and Counseling? J. Women’s Health 2019, 28, 53–62. [Google Scholar] [CrossRef]
- State Family Planning Funding Restrictions | Guttmacher Institute. Available online: https://www.guttmacher.org/state-policy/explore/state-family-planning-funding-restrictions (accessed on 28 September 2021).
- FFree, C.; Ogden, J.; Lee, R. Young women’s contraception use as a contextual and dynamic behaviour: A qualitative study. Psychol. Health 2005, 20, 673–690. [Google Scholar] [CrossRef]
- Campo, S.; Askelson, N.M.; Spies, E.L.; Losch, M. Preventing Unintended Pregnancies and Improving Contraceptive Use among Young Adult Women in a Rural, Midwestern State: Health Promotion Implications. Women Health 2010, 50, 279–296. [Google Scholar] [CrossRef] [PubMed]
- Politi, M.C.; Estlund, A.; Milne, A.; Buckel, C.M.; Peipert, J.F.; Madden, T. Barriers and Facilitators to Implementing a Patient-Centered Model of Contraceptive Provision in Community Health Centers. Contracept. Reprod. Med. 2016, 1, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez, A.M.; McCullough, C.; Fadda, R.; Ganguly, B.; Gustafson, E.; Severson, N.; Tomlitz, J. Facilitators and barriers to implementing pharmacist-prescribed hormonal contraception in California independent pharmacies. Women Health 2019, 60, 249–259. [Google Scholar] [CrossRef]
- Bhatt, C.B.; Beck-Sague, C.M. Medicaid Expansion and Infant Mortality in the United States. Am. J. Public Health 2018, 108, 565–567. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, M.I.; Caughey, A.B.; Edelman, A.; Darney, P.D.; Foster, D.G. Cost–benefit analysis of state- and hospital-funded postpartum intrauterine contraception at a university hospital for recent immigrants to the United States. Contraception 2010, 81, 304–308. [Google Scholar] [CrossRef]


{kind=link}
| Method | How It Works | Effectiveness: Pregnancies per 100 Women per Year with Consistent and Correct Use | Effectiveness: Pregnancies per 100 Women per Year as Commonly Used |
|---|---|---|---|
| Combined oral contraceptives (COCs) or “the pill” | Prevents the release of eggs from the ovaries (ovulation) | 0.3 | 7 |
| Progestogen-only pills (POPs) or “the minipill” | Thickens cervical mucous to block sperm and egg from meeting and prevents ovulation | 0.3 | 7 |
| Implants | Thickens cervical mucous to blocks sperm and egg from meeting and prevents ovulation | 0.1 | 0.1 |
| Progestogen only injectables | Thickens cervical mucous to block sperm and egg from meeting and prevents ovulation | 0.2 | 4 |
| Monthly injectables or combined injectable contraceptives (CIC) | Prevents the release of eggs from the ovaries (ovulation) | 0.05 | 3 |
| Combined contraceptive patch and combined contraceptive vaginal ring (CVR) | Prevents the release of eggs from the ovaries (ovulation) | 0.3 (for patch) 0.3 (for vaginal ring) | 7 (for patch) 7 (for contraceptive vaginal ring) |
| Intrauterine device (IUD): copper containing | Copper component damages sperm and prevents it from meeting the egg | 0.6 | 0.8 |
| Intrauterine device (IUD) levonorgestrel | Thickens cervical mucous to block sperm and egg from meeting | 0.5 | 0.7 |
| Male condoms | Forms a barrier to prevent sperm and egg from meeting | 2 | 13 |
| Female condoms | Forms a barrier to prevent sperm and egg from meeting | 5 | 21 |
| Male sterilization (Vasectomy) | Keeps sperm out of ejaculated semen | 0.1 | 0.15 |
| Female sterilization (tubal ligation) | Eggs are blocked from meeting sperm | 0.5 | 0.5 |
| Lactational amenorrhea method (LAM) | Prevents the release of eggs from the ovaries (ovulation) | 0.9 (in six months) | 2 (in six months) |
| Standard Days Method or SDM | Prevents pregnancy by avoiding unprotected vaginal sex during most fertile days | 5 | 12 |
| Basal Body Temperature (BBT) Method | Prevents pregnancy by avoiding unprotected vaginal sex during fertile days | Reliable effectiveness rates are not available | |
| TwoDay Method | Prevents pregnancy by avoiding unprotected vaginal sex during most fertile days | 4 | 14 |
| Sympto-thermal Method | Prevents pregnancy by avoiding unprotected vaginal sex during most fertile | <1 | 2 |
| Emergency contraception pills (ulipristal acetate 30 mg or levonorgestrel 1.5 mg) | Prevents or delays the release of eggs from the ovaries. Pills taken to prevent pregnancy up to 5 days after unprotected sex | <1 for ulipristal acetate ECPs 1 for progestin-only ECPs 2 for combined estrogen and progestin ECPs | |
| Calendar method or rhythm method | The couple prevents pregnancy by avoiding unprotected vaginal sex during the first and last estimated fertile days, by abstaining or using a condom. | Reliable effectiveness rates are not available | 15 |
| Withdrawal (coitus interruptus) | Tries to keep sperm out of the woman’s body, preventing fertilization | 4 | 20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ajayi, K.V.; Panjwani, S.; Wilson, K.; Garney, W.R. Using the Social-Ecological Model to Understand the Current Perspective of Contraceptive Use in the United States: A Narrative Literature Review. Women 2021, 1, 212-222. https://doi.org/10.3390/women1040019
Ajayi KV, Panjwani S, Wilson K, Garney WR. Using the Social-Ecological Model to Understand the Current Perspective of Contraceptive Use in the United States: A Narrative Literature Review. Women. 2021; 1(4):212-222. https://doi.org/10.3390/women1040019
Chicago/Turabian StyleAjayi, Kobi V., Sonya Panjwani, Kelly Wilson, and Whitney R. Garney. 2021. "Using the Social-Ecological Model to Understand the Current Perspective of Contraceptive Use in the United States: A Narrative Literature Review" Women 1, no. 4: 212-222. https://doi.org/10.3390/women1040019
APA StyleAjayi, K. V., Panjwani, S., Wilson, K., & Garney, W. R. (2021). Using the Social-Ecological Model to Understand the Current Perspective of Contraceptive Use in the United States: A Narrative Literature Review. Women, 1(4), 212-222. https://doi.org/10.3390/women1040019