Abstract
Background/Objectives: The insertion of engineered scaffolds and tissues requires precise surgical implantation with minimal interfacial scarring. Nanometric scale material polishing technologies developed for manufacturing microelectronic circuits make it possible to polish and sharpen surgical instruments at near-atomic-scale precision. We tested the hypothesis that the use of precision-sharpened scalpel blades would result in less tissue inflammation and incisional scarring. Methods: Parallel contralateral para-spinal longitudinal 4 cm long skin incisions in guinea pigs were performed, one side with a standard scalpel blade (SB) and the other with a polished nanometric scale, engineered experimental scalpel blade (EB). The side used for the polished blade was alternated and blinded from the histochemistry analysis team. The wound was excised at five time points (1, 3, 7, 16, and 60 days) with five animals per group. Histological and histochemical differences were compared. Results: The EB resulted in less bleeding, better wound adherence, relatively less macrophage density, scar volume, and granulation tissue, and significantly reduced levels of M1, M2, and TGF-β expression. Conclusions: Nanometric-scale-polished surgical scalpel blades produce significantly less tissue inflammation, scarring, and fibrosis.
1. Introduction
Each year, hundreds of millions of surgical incisions are made worldwide, with none completely devoid of surgical stress [1]. Still, gentle tissue handling is a fundamental principle of surgical practice to minimize injury and subsequent fibrosis, with the latter relationship being mediated by tissue wound healing [2,3]. In general, wound healing is a complex, genetically programmed process that aims to re-establish the structural integrity of damaged tissue [4,5]. In addition, epigenetic factors, incision, suturing, post-operative care, wound location, and tension, along with age, gender, and overall patient health, contribute to wound healing [6,7,8].
Strategies focusing on nanotherapeutics and mitigating wound healing are on the rise, with the ability to localize their effects on a small scale [9,10]. For surgical procedures, reducing tissue damage is possible due to clinically manageable factors [11]. One way to reduce tissue damage is to improve surgical instruments. Yet, the inadequacies of surgical tool cutting edges are rarely studied on soft biological tissue [12]. In 2021, Liu et al. assessed this concept, highlighting that microcracks have been detected in new steel blades and that the most critical component influencing surgical tool cutting performance is blade sharpness which mitigates adhesion failure [12]. Thus, surgical tools can be improved by sharpening cutting edges. In fact, the microelectronics industry has developed tools for controlling the surface roughness of circuit dyes on a nanometer scale or smaller, and standard surgical blades can also be polished by this technology [13,14]. Thus, to determine if an increase in the quality of the cutting edge of a surgical steel blade has a reproducible effect on wound healing, incisions made by a standard blade (SB) have been analyzed alongside those made by a nanometric-scale-polished, engineered experimental blade (EB).
To test this hypothesis, a study of dorsal skin wound healing was conducted in which the inflammatory and fibrotic responses were compared in a single animal to reduce biological variability. Incisions made by a standard commercially available surgical blade (SB) were analyzed alongside those made by a nanometric-scale-polished, engineered experimental blade (EB) in the same animal. The healing process in response to either the SB or EB was analyzed at different time points (1, 3, 7, 16, and 60 days) after wound closure to gain meaningful insight into the final healing outcome.
Because quantifying the inflammatory response to surgical incisions is typically performed by measuring various biomarkers, we analyzed those that are commonly involved in the healing response. For example, macrophages are pivotal for the regulation of immune and inflammatory responses, and it is generally understood that the density of macrophages at the site of injury is indicative of the inflammatory response magnitude [15]. Specifically, we examined the commonly characterized pro-inflammatory “M1” and anti-inflammatory “M2” macrophage phenotypes. Approximately 5–7 days after injury, the majority of M1 phenotypes matured into M2, with M2-expressing factors important for wound healing and scar formation [16]. In fact, high expressions of “M2” are often associated with abnormal scar pathogenesis [17]. In addition, wound healing and tissue remodeling are partly coordinated by cytokines [18]. We analyzed tumor necrosis factor-alpha (TNF-α) for injury and transforming growth factor-β (TGF-β), which regulates healing and the inflammatory response.
Overall, we quantified wound healing quality through morphological, histological, and histochemical comparisons, i.e., bleeding, wound closure, macrophage density, scar volume, granulation tissue, and the expressions of M1, M2, TGF-β, and TNF-α.
2. Material and Methods
2.1. Scalpel Blades
The blades were either standard Swann-Morton #15 blades or the experimental, nanometric-scale-polished, engineered version of the same blade (Entrepix Medical, Phoenix, AZ, USA). Optical microphotographs illustrate the difference [13,19]. The unprocessed standard blades (SBs) were used as received and were from the same batch as the nanometric scale-polished blades. The experimental blade (EB) was produced by a metal polishing process that minimized surface features along the blades’ surfaces and edges, increasing smoothness [19]. This refinement process involved a variant of chemical mechanical planarization (CMP), which is a process widely used in the manufacturing of advanced semiconductors and computer chips. CMP allows for the outer atomic layer of several ceramic and metal surfaces to be softened following a set of chemical reactions. The softened surface is extracted by mechanical forces exercised by a polishing tool, pad, and associated microscopic particles. The process reliably creates surfaces of near-atomic perfection while the blade’s core mechanical attributes remain unchanged [13]. Blades polished using this technique are shown to be 20-fold more uniform in terms of their root-mean-square roughness in comparison to standard, as-received blades, and the maximum peak-to-valley roughness of the nanometric-scale polished blades is reduced from 4.1 microns to 0.20 microns [20].
2.2. Animals
Female Hartley guinea pigs (weight 300 g ± 20 g) were obtained from Charles River Labs (Wilmington, MA, USA) and housed for at least 48 h prior to surgery. Guinea pigs were appropriate for this initial assessment since the amount of scarring is linked to the amount of tissue damage and guinea pigs are accessible and able to undergo multiple incisions [21]. Standard operating precautions to prevent infection were employed. Each guinea pig was administered a preemptive dose of analgesia consisting of an intramuscular dose of buprenorphine (300 ug/kg). Then, animals were placed in a sealed chamber and administered isoflurane gas (3–4% in 1.5 L/minute oxygen). After removing the guinea pig, anesthesia was administered via an anesthetic cone mask (2–4% in 1.5 L/min oxygen) to maintain a deep anesthetic plane. Immediately after anesthetic sedation, a lubricant was applied to the eyes, and the animal was placed on a heating pad where it would remain for the surgery’s duration. Throughout the procedure, vitals (heart rate, pulse oxygenation, temperature, and respiratory rate) were monitored. After 8 h post-surgery, animals received another dose of analgesia. Post-operative medical care included daily incision healing monitoring and behavioral observations for pain or distress. At each time point (day 1, day 3, day 7, day 16, and 2 months), four animals were sacrificed at the end of their group study via an overdose of pentobarbital (>150 mg/kg) and thoracotomy as a secondary method.
The protocol was approved by the University of Chicago Institutional Animal Care and Use Committee. Animals were cared for using the standard procedure of the central housing facility, following the NIH guidelines described in The Guide for the Care and Use of Laboratory Animals.
2.3. Skin Incision and Repair
Once anesthetic depth was confirmed, dorsal hair was shaved using electric clippers. With the guinea pig in the prone sagittally aligned position, two dorsal paraspinal skin incisions were marked with a standard surgical marker. The marks were located 1 cm lateral to the spinous process. The guinea pig was moved onto the operation table and the back skin was prepped with betadine soap, and then betadine solution. Once the solution was dried, the excess dried betadine was removed with a sterile gauze pad.
The anesthetic depth was rechecked and adjusted as needed by the veterinary staff. To reduce bleeding, the subcutaneous tissue beneath the panniculus carnosus aponeurosis (PCA) was infiltrated with 0.5% lidocaine with epinephrine in water (1:200,000) 15 min before the incisions were made. Two incisions (each 4 cm long) were made through the skin and underlying panniculus carnosus aponeurosis, with one skin incision to the left and one to the right of the midline (Figure 1). To ensure each incision was as uniform as possible and of the same depth, an initial, very small incision was made, and a sterile scalpel guide was gently inserted in the loose areolar plane beneath the panniculus carnosis aponeurosis, precisely beneath the incision skin markings, to ensure that the incisions were made in one fluid motion without injuring skeletal muscle or its fascia. No additional dissection occurred. Any bleeding was managed with epinephrine-soaked Telfa® pads. Electrocautery was not needed or used.

Figure 1.
Skin incisions: one incision is sutured closed. The other is open, ready to be closed with suture; both are 4 cm long.
To prevent bias due to anatomical differences, the EB and SB incisions were alternated between animals to eliminate potential systemic errors. Each incision was approximated with three Vicryl® (5–0, reverse cutting needle)-inverted sutures in the dermal layer without tension for alignment. The epidermis was closed with a Steri-Strip® and Dermabound® glue. The incisions and sutures were performed by one surgeon to reduce variability. The surgical team coded the incisions for each animal and did not provide that information to the histology and histochemistry team.
After euthanasia, incisions were harvested along with the surrounding area of normal tissue. The tissue was then cut into transverse 5 mm wide strips (3 per animal) located midway between the sutures. Each biopsy contained both incisions. Then, the strips were fixed in 10% formalin and processed for paraffin embedding.
2.4. Histology
The histological specimens for the two incision types were collected at 1, 3, 7, 16, and 60 days post-surgery. The embedded sample blocks were cut into 5-micron-thick sections and mounted on standard microscope glass slides. Hematoxylin and Eosin (H&E) stains were used to evaluate structural modifications and vasculature morphology in the tissue samples. Masson trichrome stains were used to visualize collagen and smooth muscle containing granulation tissue and scar.
2.5. Immunohistochemistry
Immunohistochemistry was used to detect wound biomarkers such as macrophages, TGF-β, and TNF-α. The Calprotectin Monoclonal Antibody MAC 387 (Life Technologies, Grand Island, NY, USA) was used to label macrophages in tissue sections following the protocol provided by the supplier. In addition, markers for M1 (IL-1, Sigma, Burlington, MA, USA), M2 (ARG-1, Fisher, Waltham, MA, USA), TGF-β (SMAD3, Sigma, Burlington, MA, USA), and TNF-α (MAP4K4, Sigma, Burlington, MA, USA) were stained in the paraffin-embedded samples according to each respective supplier protocol. The incisions made by both SB and EB from one animal were placed on the same slide and stained.
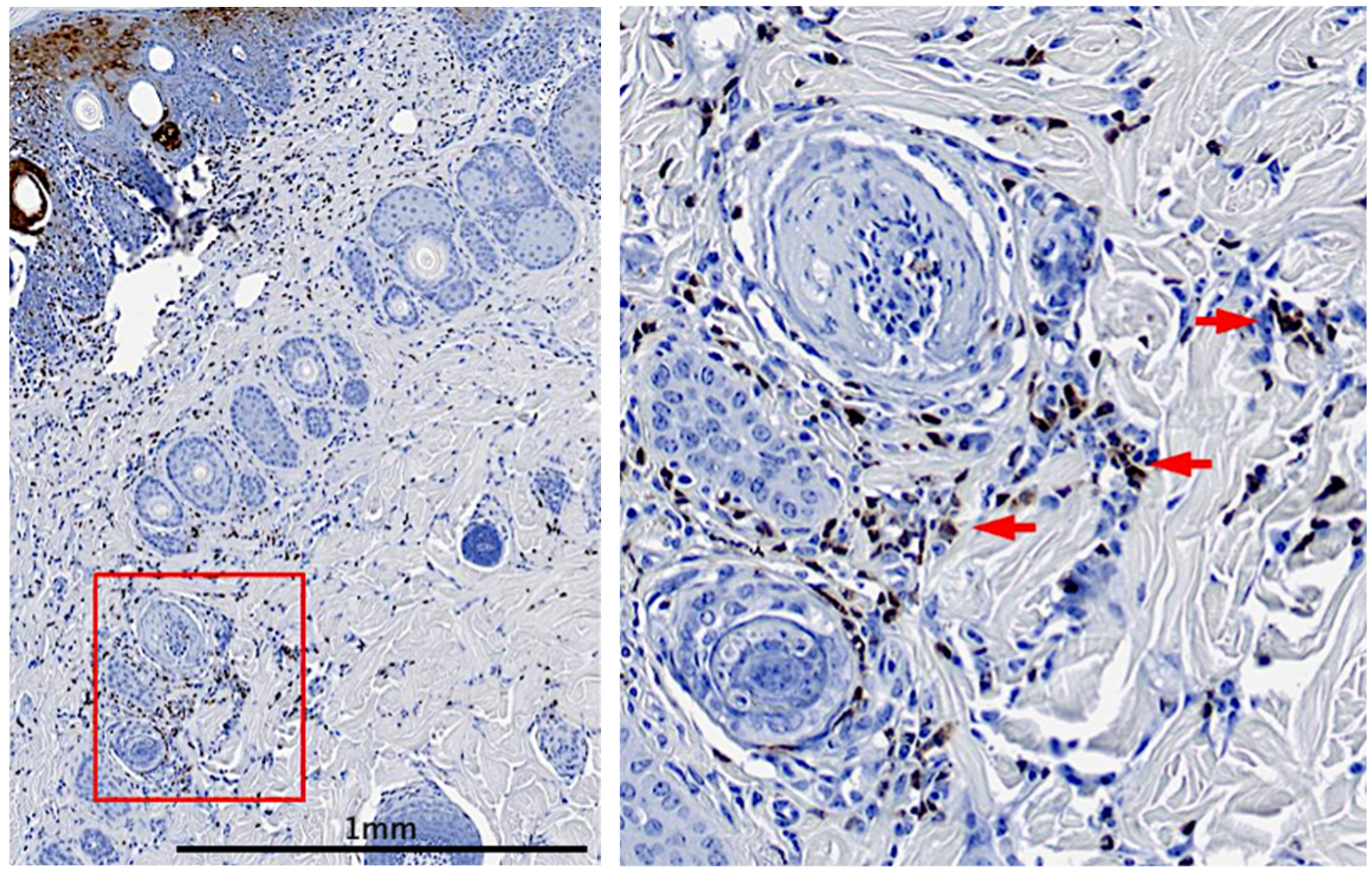
Wound biomarker infiltration was visualized by tissue section analysis (Figure 2). Wound areas were identified by boundaries of the macrophage inflammatory infiltrate. We counted macrophages in 5 random high-power fields, each with a size of 5 mm × 3 mm, within the tissue adjacent to the incision site and calculated the average number of macrophage cells. The quantitation of the macrophage cells was performed from four animals per time point.
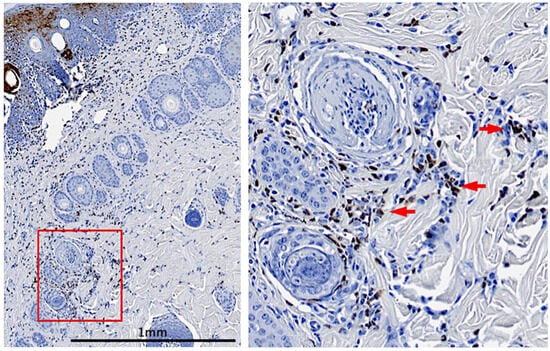
Figure 2.
Immunohistochemistry tissue section: immunohistochemistry macrophage staining with arrows pointing to positively stained macrophages.
2.6. Image Processing
Histology and immunohistochemistry slides were digitized at 40× using a Tri-Panoramic SCAN 40× whole-slide scanner with an Allied Vision Technologies Stingray F146 color emission detector and a 40× 0.95 (na) LWD Zeiss objective with a virtual magnification range from 0.5× to 100× in high resolution (0.12 um/pixel). The slides were then analyzed at 20× with QuPath (v0.5.1) and ImageJ (v1.54k) which are both open-sourced image softwares. For macrophage staining, the data were calculated as the percentage of intensity and the area of staining vs. the total area selected.
2.7. Statistical Analysis
Multiple measurements (i.e., 3) were made for each animal for each condition and multiple animals were used at each time point. These observations were made for 6 time points after the incision was made (i.e., day 0). Data from each condition and time point was normally distributed. The power calculation had ≥ 0.90 reliability for 5 data points, indicating that we had more samples than needed to reach reliability. The reliability was further supported as data points were continuous over time. In addition, we assumed a standard error of the mean of 0.25, calculating α < 0.03 and β < 0.04. All data were considered to be normally distributed, and comparisons were made using a mixed, parametric model. Data are presented as the mean and standard deviation, and a paired two-tailed Student’s t-test was performed to compare biomarker levels. Correlations between the SB and EB groups were tested, and the statistical significance level was set at p < 0.05.
3. Results
3.1. Animal Response
Two animals were lost and removed from the study due to signs of immediate post-anesthesia distress. Both animals were replaced with animals that experienced the surgery successfully without presenting any signs of pain or distress.
3.2. Wound Healing Observations
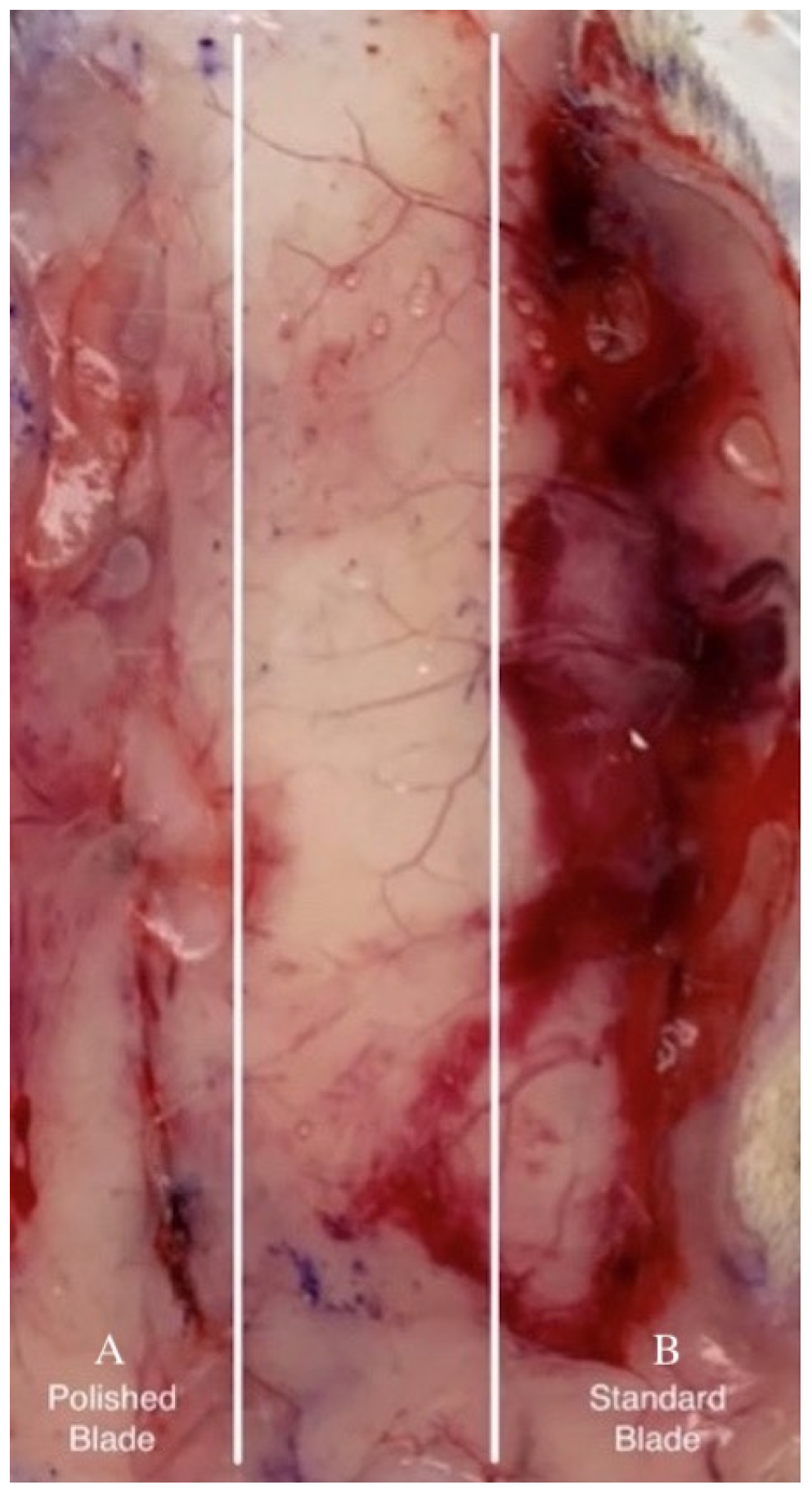
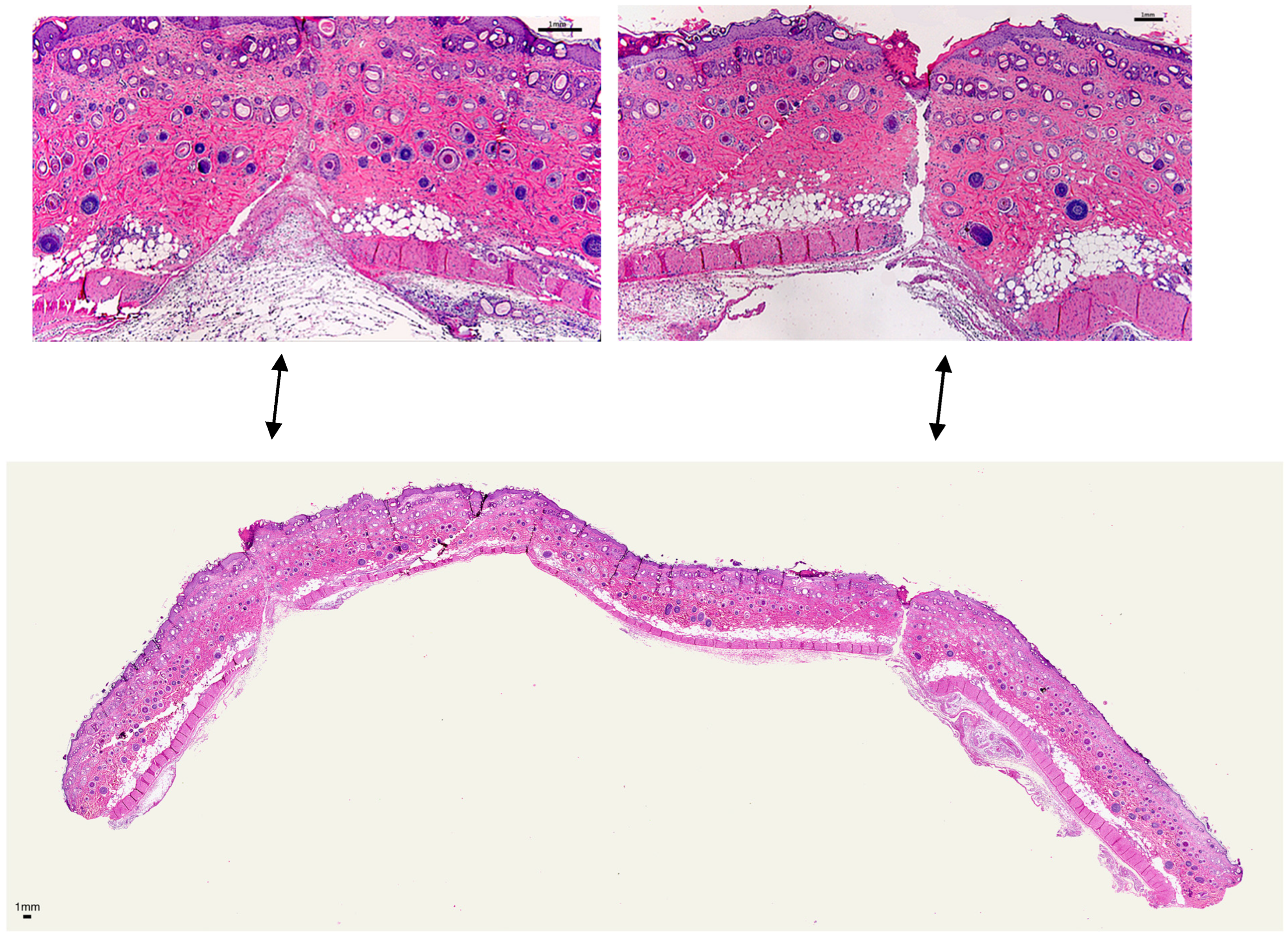
Morphometric wound analysis reveals site-specific differences in healing for the two types of incisions. While not quantified, in tissue samples collected 1 day after surgical incision, subcutaneous blood staining was frequently observed in incisions made with the SB and less frequently with the EB (Figure 3). Monitoring blood staining was not part of the experimental plan. Within 3 days after skin incisions, the majority of wounds produced by SB did not achieve closure (Figure 4). In contrast, approximately 90% of incisions made by EB exhibited adherence in this same period. The results show that the wound treated with SB did not close completely on the third day; however, the one treated with EB did. By day 7, all wounds achieved closure. After 2 months, all incisions were completely healed, and the dorsal skin softness and elasticity were qualitatively judged to be normal.
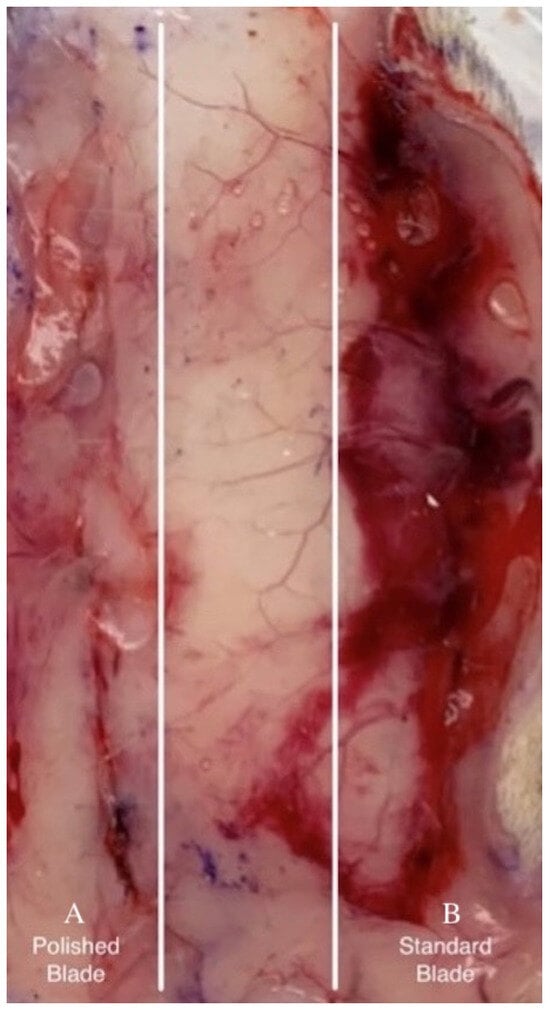
Figure 3.
Bleeding under tissue excised 1 day post-surgery: incisions made by EB (A) and SB (B).
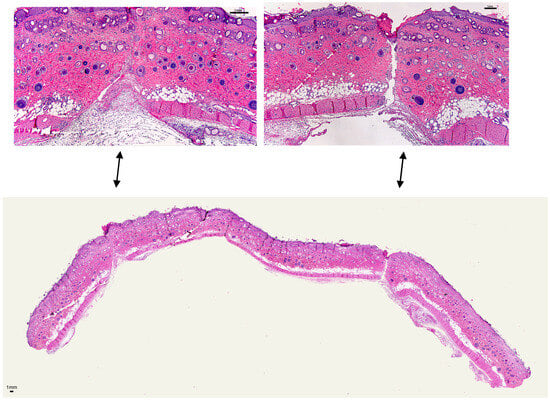
Figure 4.
Wound H&E histology: morphological changes, closure, and re-epithelialization 3 days post-injury: Left: incision by EB; right: incision by SB; bottom: full representative sample with incision by EB (left) and SB (right).
3.3. Macrophage Counts
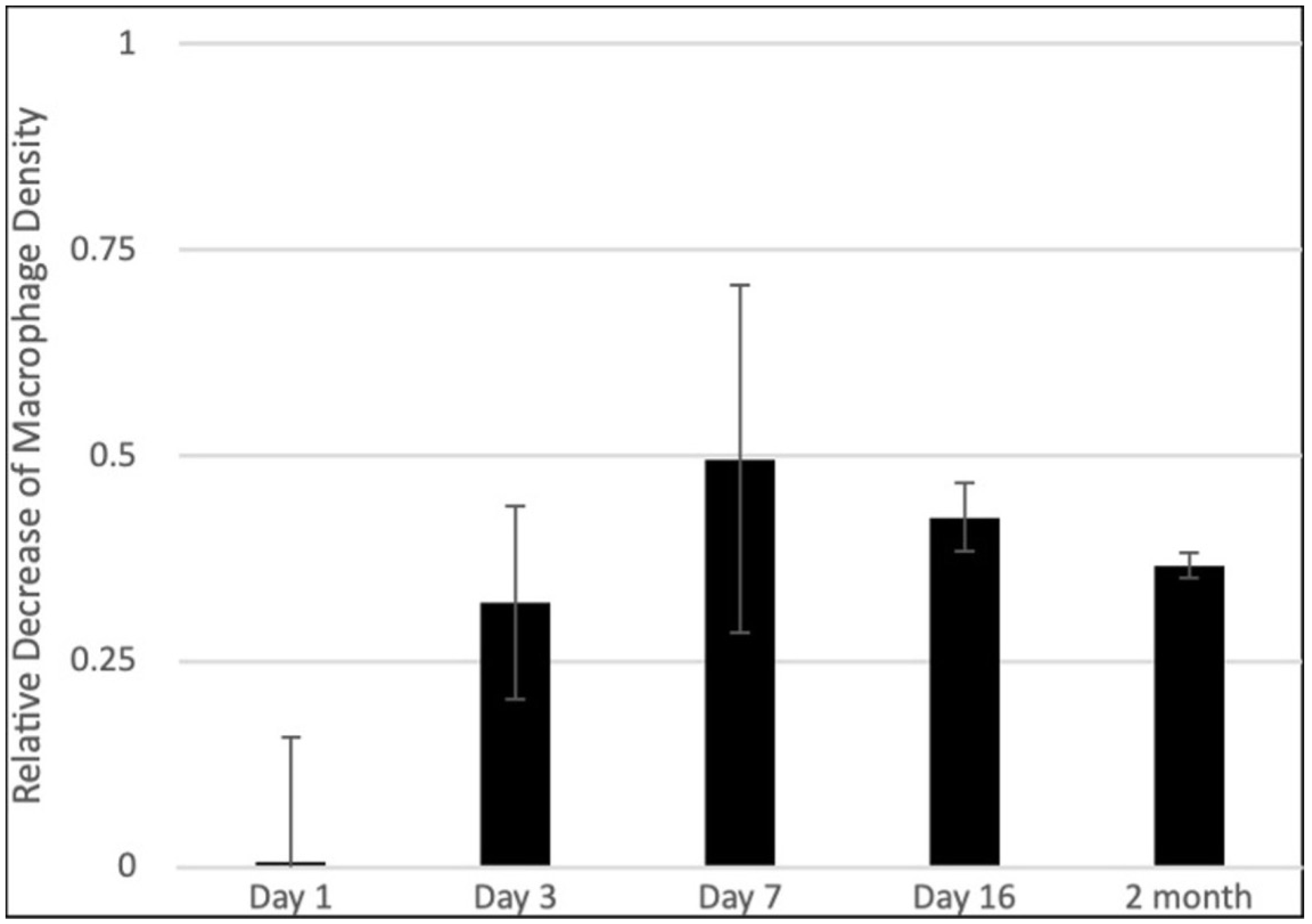
The relative difference between the macrophage density in skin incisions made with the experimental blade MEB vs. the macrophage density corresponding to incisions made with the standard blade MSB is displayed in Figure 5. Data analysis shows that the macrophage infiltration exhibited a noteworthy decrease (M in skin incisions made with the EB compared to that corresponding to skin incisions made with the SB for all time points. These results suggest that the inflammatory response in nanometric-scale-polished blade skin incisions is reduced at all time points post-operation.
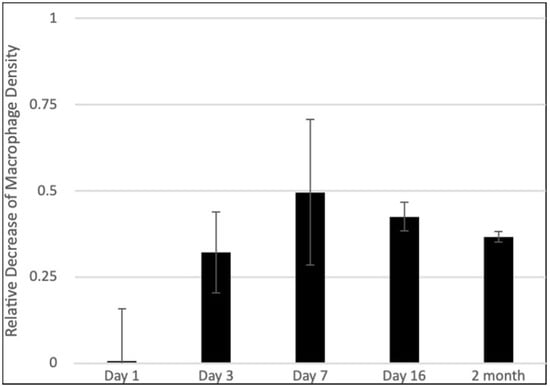
Figure 5.
Macrophage immunohistochemistry and decrease in relative density: average values and standard deviations of M describing the relative decrease in the macrophage density in skin incisions made with EB and relative incisions made with SB.
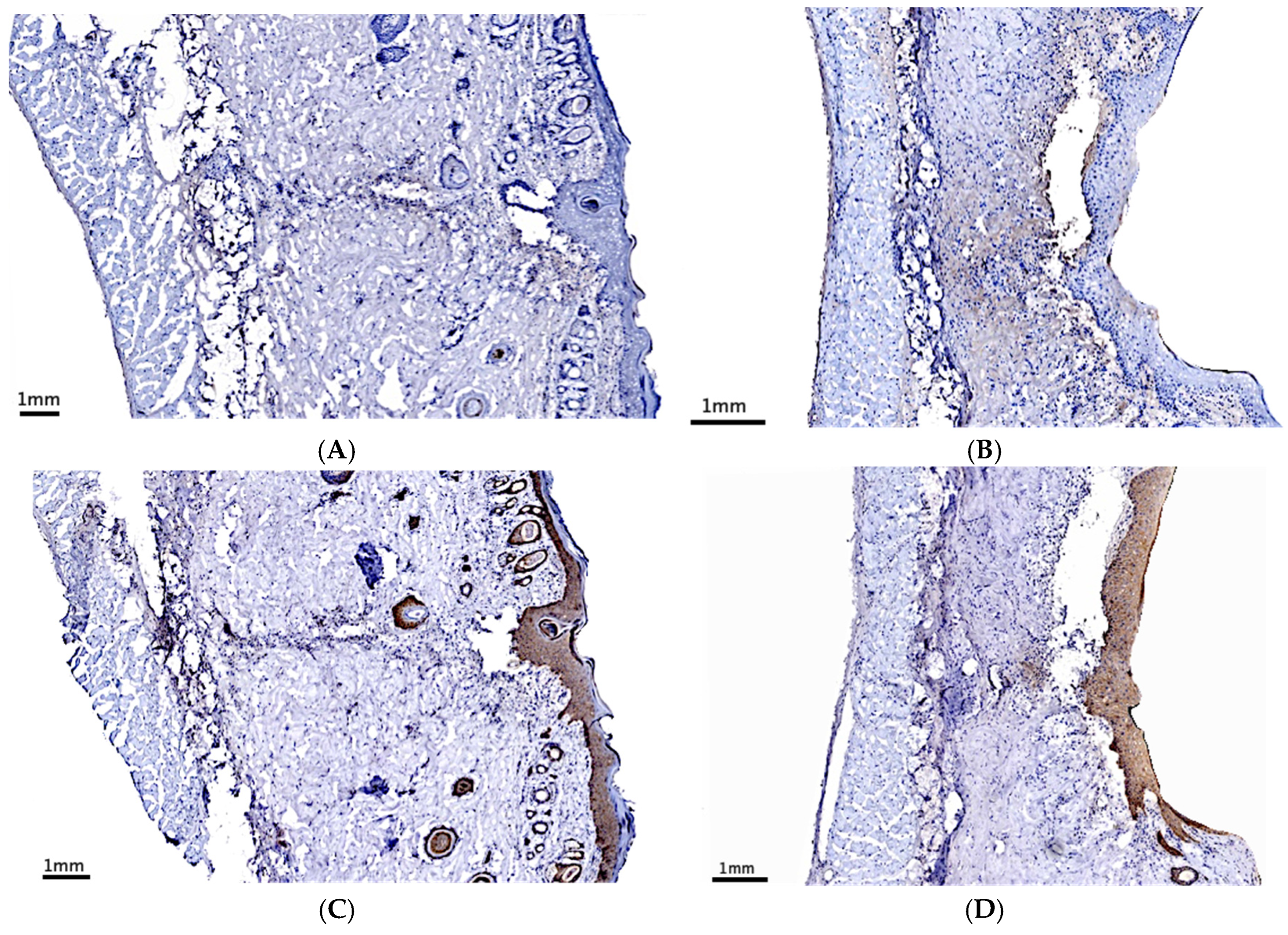
On day 7 post-incision, the expressions of M1, M2, TGF-β, and TNF-α in the scar area were measured by immunohistochemistry (Figure 6). TGF-β, M1, and M2 levels were lower in scar areas made by nanometric-scale-polished blades than those with the control blade (Table 1). While TNF-α was expressed in the scar area made by both blades, no significant differences were observed (Table 1).
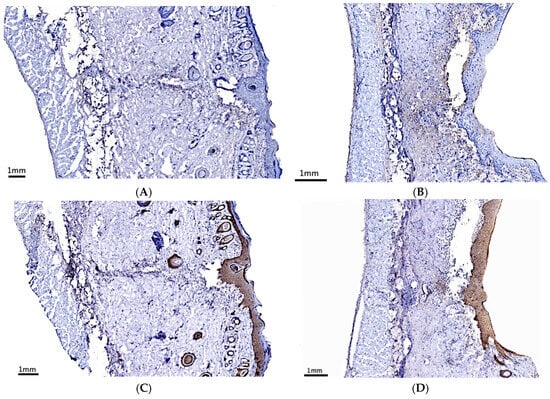
Figure 6.
Cytokine immunohistochemistry: representative images showing the expression of TGF-β (A,B) and IL-1 (C,D) in scars made by SB (A,C) and EB (B,D) 7 days post-surgery.

Table 1.
Quantitative histochemical analysis 7 days post-surgery: expressions of TNF-α, TGF-β, M1 expression, and M2 expression in the scar area; TGF-β, M1, and M2 expressions in the scar area made by EB are significantly lower than SB; data are expressed as the percentage of specific staining vs. the total scar area; data are the mean and standard error from 5 pairs of samples from different animals. (* p < 0.05, t-test).
3.4. Scar Area
The amount of granulation tissue surrounding each incision was calculated from trichrome-stained sample cross-sections. Granulation deposition was not detectable 24 h after incision but was noticeable at the beginning of day 3.
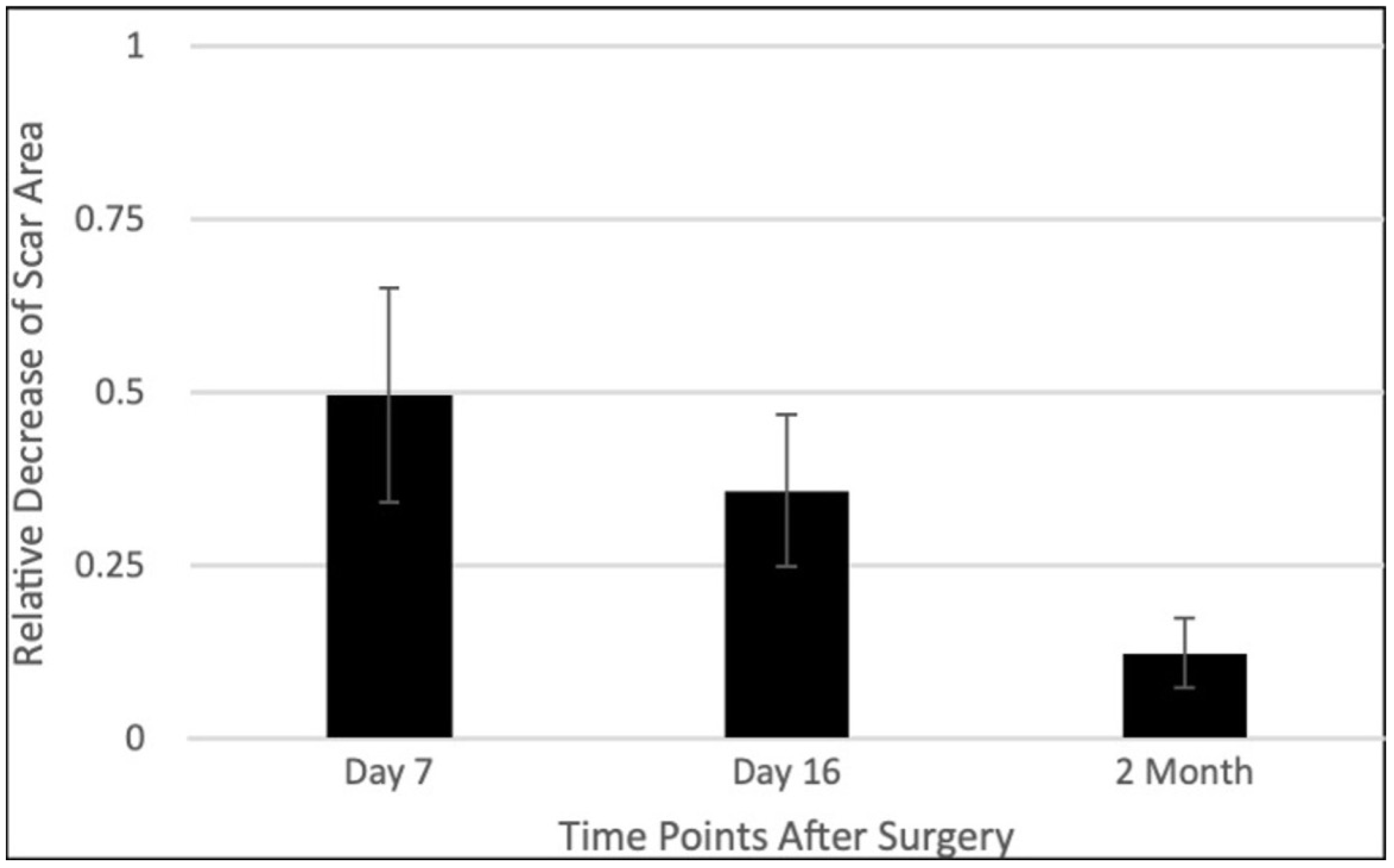
Figure 7 presents the average values of the C = ratio measuring the decrease in the granulation tissue deposition area in the skin incisions made with the experimental blade CEB relative to the area of skin incisions made with standard blades CSB. The amount of granulation tissue was reduced more in the wounds made with nanometric-scale-polished surgical blades. We observed that C at all time points, which means that notably less granulation tissue occurred in skin incisions made by EBs in comparison with SBs. Generally, the reduction in the granulation tissue deposition area in skin incisions made with the EB ranged between 30% and 50% during the proliferation phase and reached approximately 90% 6 months post-incision, with the magnitude of the standard error of the mean being approximately 25% of the mean on day 7 and about 45% of the mean on day 16 and 6 months post-operation.
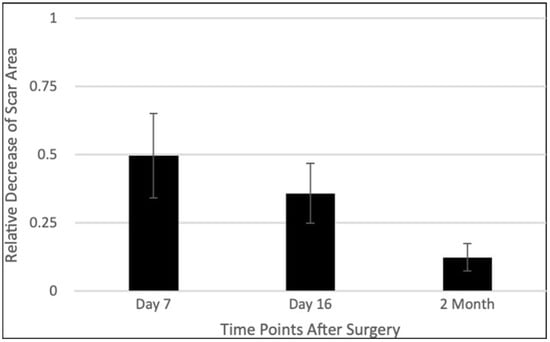
Figure 7.
Scar area decrease: Average values and standard errors of C describing the relative decrease in granulation tissue surrounding skin incisions made with EB relative to SB; results derived from cross-sections of trichrome-stained samples on days 7, 16, and 2 months post-surgery.
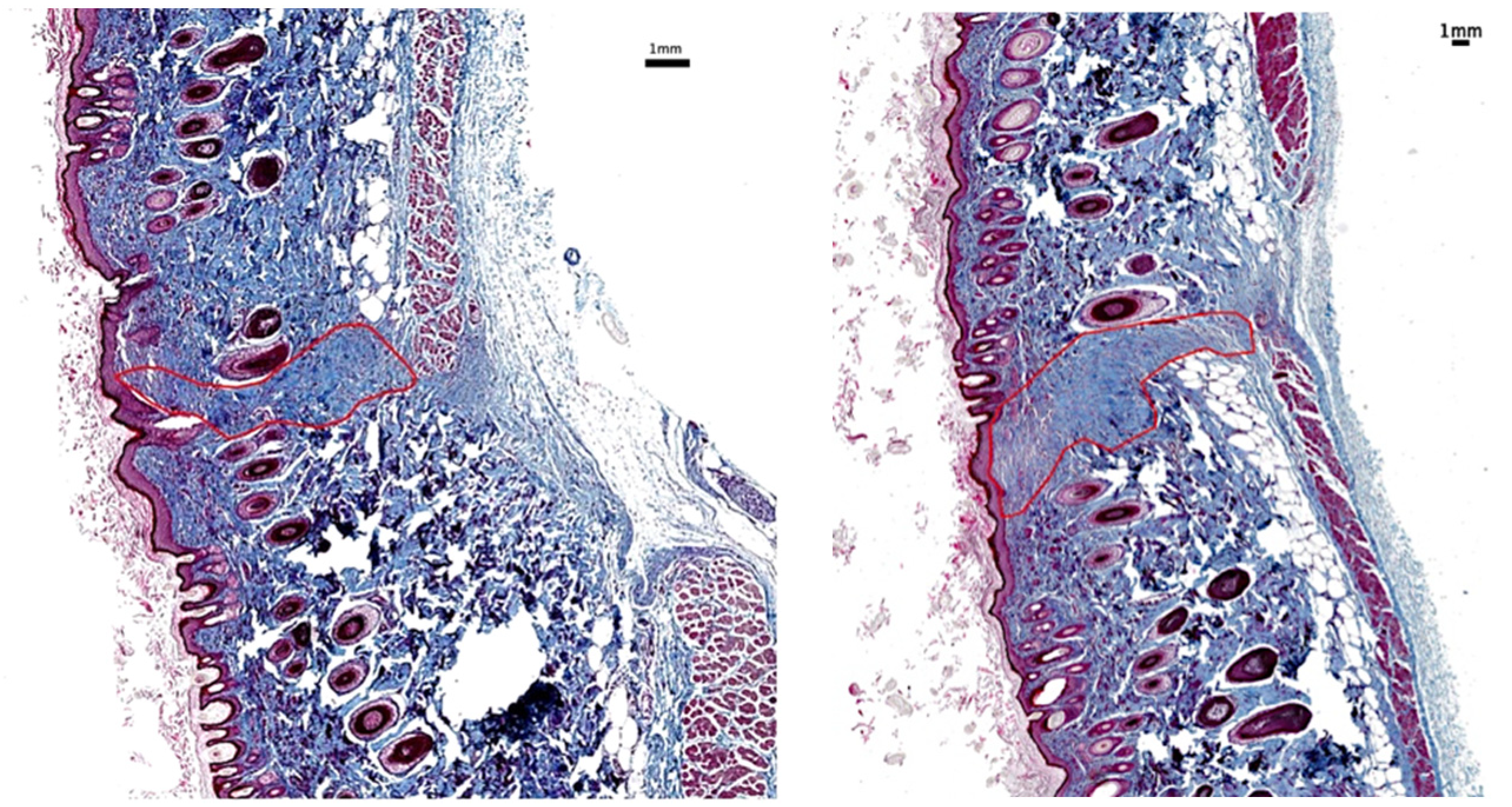
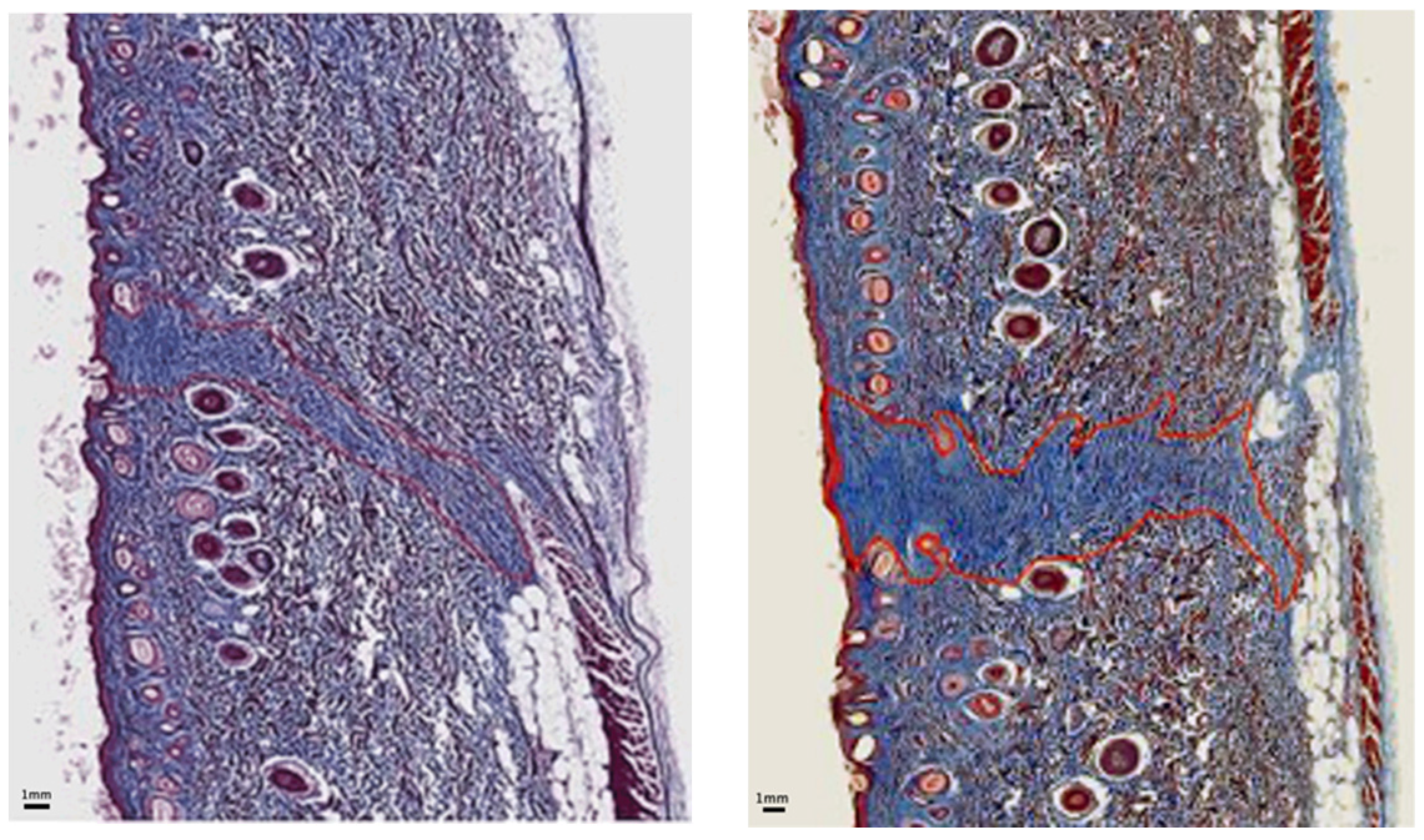
Figure 8 and Figure 9 are representative images of wound histology at 16 days and 2 months post-surgery, respectively. The difference in the amount of scar produced by the EB versus the SB is apparent. In addition, the scar area width is narrower along the incision made with the EB in comparison with that corresponding to the SB.
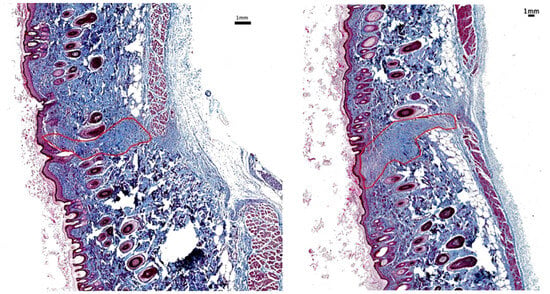
Figure 8.
Scar histology 16 days post-surgery: Histological sample stained with trichrome at 16 days post-surgery showing less scarring in region of EB skin incision (left) than SB skin incision (right).
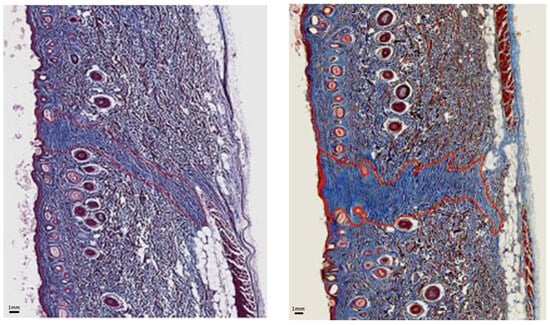
Figure 9.
Scar histology 2 months post-surgery: Histological sample stained with trichrome at 2 months post-surgery showing less scarring in region of EB skin incision (left) than SB skin incision (right).
4. Discussion
The data from this study indicate that using sharper and smoother scalpel blades to make dorsal skin incisions in a guinea pig model produces less inflammation and scarring than a standard scalpel blade. Incisions made with the nanometric-scale-polished, engineered scalpel seem to have less subcutaneous blood staining, better wound adhesion, less macrophage infiltration and granulation tissue, smaller scar volume and reduced TGF-β, M1, and M2 expression (p < 0.05). These results indicate that scar deformity can likely be reduced using nanometric-scale-polished, engineered scalpel blades.
However, there were no significant differences in TNF-α expression levels between the scars produced by the nanometric scale-polished vs. the standard blade at 7 days post-incision. This may suggest that the inflammatory stage of healing progresses toward the proliferative or transitional repair stage. Another possibility is that reduced tissue disruption by nanometric-scale-polished blades did not cause significant TNF-α alterations or that this marker may not be a dominant factor in wound healing under this condition.
Nevertheless, the results are particularly interesting given that guinea pig skin wounds, similar to other loose skin mammals, do not form hypertrophic scars following uncomplicated wound healing as observed, in general, in humans or larger pigs. This suggests that the benefit of polishing scalpel blades witnessed in this study may be amplified in the clinical setting.
Moreover, the clinical implications are vast, and we will explore just a few of them below. Firstly, engineered tissues and extracellular matrix scaffolds are increasingly being used clinically for reconstructive surgery [22,23,24]. The success of this technology is heavily dependent on the precise connection between the implanted tissue equivalent and the surrounding tissue it is replacing. To optimize the incorporation of engineered tissue, surgical trauma, and interfacial scarring must be minimized. Thus, the nanometric scale-controlled scalpel blade sharpness technology holds promise to increase the efficacy of regenerative tissue engineering that requires both accurate tissue materials and integration into the tissue under construction. This is especially true for specialized tissues like nerves and striated muscles.
Alternately, it is noteworthy that the American public, especially hypertrophic scar-prone groups, are concerned about post-surgical scar disfigurement [25,26]. Polishing the scalpel blades may be an important step toward providing the answer to their needs. Furthermore, we expect incisional inflammation to correlate with pain [27]. Human clinical studies will be needed to determine if nanometric-scale-polished scalpel blade incisions are less symptomatic. Finally, there is potential for both reduced post-operative complications and medications if incisions heal with less inflammation and scarring.
Nevertheless, there are limitations to this study, in addition to the need for future studies that could enhance our findings. While one surgeon performed all surgeries to reduce variability, there is inherent animal-to-animal variability in the skin transection and repair process, potentially due to variations in skin thickness and composition. In addition, the small sample size limits statistical power and the ability to generalize findings. Also, while the wound was excised at five time points, studying additional intermediate and later time points may provide a more comprehensive understanding of wound healing progression; while the authors observed that incisions completely healed in a qualitative manner, quantifying this finding after two months may provide additional insights. Last, additional inflammatory markers could be studied to provide a more comprehensive understanding of the healing process.
Author Contributions
Conceptualization, L.M., M.X.L., V.B. and R.C.L.; methodology, L.M., M.X.L., V.B. and R.C.L.; software, L.M., M.X.L., V.B. and R.C.L.; validation, L.M., M.X.L., V.B. and R.C.L.; formal analysis, L.M., M.X.L., V.B. and R.C.L.; investigation, L.M., M.X.L., V.B. and R.C.L.; resources, L.M., M.X.L., V.B. and R.C.L.; data curation, L.M., M.X.L., V.B. and R.C.L.; writing—original draft preparation, M.X.L., V.B. and R.C.L.; writing—review and editing, L.M. and R.C.L.; visualization, L.M., M.X.L., V.B. and R.C.L.; supervision, R.C.L.; project administration, R.C.L.; funding acquisition, R.C.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Entrepix Medical of Phoenix, AZ, FP105357. Entrepix Medical provided scalpel blades for this study. The APC was funded by The University of Chicago.
Institutional Review Board Statement
The study was approved by the Institutional Animal Care and Use Committee of The University of Chicago (#72601, titled “Effect of Entrepix Ultra-Polished Scalpel on Incisional Inflammation and Fibrosis”, and approved on 8 December 2020).
Informed Consent Statement
Not applicable.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
The authors all wish to thank Cliff Spiro (Planatome, Phoenix, AZ, USA) for providing the scalpel blades and technical advice on preparing the scalpel blades for use. Also, the authors appreciate the outstanding veterinary professionals of the A.J Carlson Research Facility, the pathologists of the University of Chicago Human Tissue Resource Center, and the excellent staff of the University of Chicago Integrated Light Microscopy Core for their assistance with this project. Finally, Entrepix Medical has recently been acquired and is now named Planatome, LLC.
Conflicts of Interest
The authors declare no conflicts of interest. None of the authors have any existing or expected financial or non-financial interests related to the business of producing, selling or distributing sharpened scalpel blades. None of the authors have any financial or non-financial interests in Entreprix or any other surgical instrument or scalpel blade manufacturing company. The funder had no role in the design of the study; in the collection, analyses, or interpretation of the data; in the writing of the manuscript; or in the decision to publish the results.
References
- Dobson, G.P. Trauma of major surgery: A global problem that is not going away. Int. J. Surg. 2020, 81, 47–54. [Google Scholar] [CrossRef] [PubMed]
- El Ayadi, A.; Jay, J.W.; Prasai, A. Current Approaches Targeting the Wound Healing Phases to Attenuate Fibrosis and Scarring. Int. J. Mol. Sci. 2020, 21, 1105. [Google Scholar] [CrossRef]
- Martin, P.; Pardo-Pastor, C.; Jenkins, R.G.; Rosenblatt, J. Imperfect wound healing sets the state for chronic diseases. Science 2024, 386, eadp2974. [Google Scholar] [CrossRef]
- Broughton, G., 2nd; Janis, J.E.; Attinger, C.E. The basic science of wound healing. Plast. Reconstr. Surg. 2006, 117 (Suppl. S7), 12S–34S. [Google Scholar] [CrossRef]
- Li, J.; Chen, J.; Kirsner, R. Pathophysiology of acute wound healing. Clin. Dermatol. 2007, 25, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Sangha, M.S.; Deroide, F.; Meys, R. Wound healing, scarring and management. Clin. Exp. Dermatol. 2024, 49, 325–336. [Google Scholar] [CrossRef]
- Yu, H.; Wang, Y.; Wang, D.; Yi, Y.; Liu, Z.; Wu, M.; Wu, Y.; Zhang, Q. Landscape of the epigenetic regulation in wound healing. Front. Physiol. 2022, 13, 949498. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Dipietro, L.A. Factors affecting wound healing. J. Dent. Res. 2010, 89, 219–229. [Google Scholar] [CrossRef]
- Mamun, A.A.; Shao, C.; Geng, P.; Wang, S.; Xiao, J. Recent advances in molecular mechanisms of skin wound healing and its treatments. Front. Immunol. 2024, 15, 1395479. [Google Scholar] [CrossRef]
- Wang, M.; Huang, X.; Zheng, H.; Tang, Y.; Zeng, K.; Shao, L.; Li, L. Nanomaterials applied in wound healing: Mechanisms, limitations and perspectives. J. Control Release 2021, 337, 236–247. [Google Scholar] [CrossRef]
- Roseborough, I.E.; Grevious, M.A.; Lee, R.C. Prevention and treatment of excessive dermal scarring. J. Natl. Med. Assoc. 2004, 96, 108–116. [Google Scholar]
- Liu, Z.; Chen, H.; Sui, J.; Yuan, Z.; Chen, Z.; Fu, J.; Wang, C. Failure behavior and influence of surgical tool edges in soft tissue cutting. J. Manuf. Process. 2021, 68, 69–78. [Google Scholar] [CrossRef]
- Planatome. Available online: https://planatome.com/technology/ (accessed on 12 December 2024).
- Cliff Spiro. Entrepix Medical LLC. USPTO Patent US 7,037,175, 2 May 2006.
- Lee, C.H.; Choi, E.Y. Macrophages and Inflammation. J. Rheum. Dis. 2018, 25, 11. [Google Scholar] [CrossRef]
- Hesketh, M.; Sahin, K.B.; West, Z.E.; Murray, R.Z. Macrophage Phenotypes Regulate Scar Formation and Chronic Wound Healing. Int. J. Mol. Sci. 2017, 18, 1545. [Google Scholar] [CrossRef] [PubMed]
- Kuninaka, Y.; Ishida, Y.; Ishigami, A.; Nosaka, M.; Matsuki, J.; Yasuda, H.; Kofuna, A.; Kimura, A.; Furukawa, F.; Kondo, T. Macrophage polarity and wound age determination. Sci. Rep. 2022, 12, 20327. [Google Scholar] [CrossRef]
- Xiao, T.; Yan, Z.; Xiao, S.; Xia, Y. Proinflammatory cytokines regulate epidermal stem cells in wound epithelialization. Stem Cell Res. Ther. 2020, 11, 232. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Oh, S.; Kim, Y.S.; Spiro, C.L.; Hong, J.P.; Choi, J.W. Effects of an Ultra-Polished Scalpel on Incisional Wounds in a Diabetic Model. J. Craniofac. Surg. 2024, 35, e195–e200. [Google Scholar] [CrossRef]
- Prescher, H.; Ling, M.X.; Bigdelle, V.; Spiro, C.L.; Lee, R.C. Scalpel edge roughness affects post-transection peripheral nerve regeneration. Surg. Open Sci. 2020, 4, 1–6. [Google Scholar] [CrossRef]
- Grada, A.; Mervis, J.; Falanga, V. Research Techniques Made Simple: Animal Models of Wound Healing. J. Investig. Dermatol. 2018, 138, 2095–2105.e1. [Google Scholar] [CrossRef]
- Xu, Y.; Yao, Y.; Gao, J. Cell-Derived Matrix: Production, Decellularization, and Application of Wound Repair. Stem Cells Int. 2024, 2024, 1–11. [Google Scholar] [CrossRef]
- Mahajan, N.; Soker, S.; Murphy, S.V. Regenerative Medicine Approaches for Skin Wound Healing: From Allografts to Engineered Skin Substitutes. Curr. Transpl. Rep. 2024, 11, 207–221. [Google Scholar] [CrossRef]
- Dzobo, K.; Thomford, N.E.; Senthebane, D.A.; Shipanga, H.; Rowe, A.; Dandara, C.; Pillay, M.; Motaung, K.S.C.M. Advances in Regenerative Medicine and Tissue Engineering: Innovation and Transformation of Medicine. Stem Cells Int. 2018, 2018, 2495848. [Google Scholar] [CrossRef] [PubMed]
- Kinani, M.E.; Duteille, F. Scar Epidemiology and Consequences. In Textbook on Scar Management: State of the Art Management and Emerging Technologies [Internet]; Téot, L., Mustoe, T.A., Middelkoop, E., Gauglitz, G.G., Eds.; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar] [CrossRef]
- Monstrey, S.; Middelkoop, E.; Vranckx, J.J.; Bassetto, F.; Ziegler, U.E.; Meaume, S.; Téot, L. Updated scar management practical guidelines: Non-invasive and invasive measures. J. Plast. Reconstr. Aesth. Surg. 2014, 67, 1017–1025. [Google Scholar] [CrossRef]
- Brennan, T.J. Incisional/Postoperative Pain. In Encyclopedia of Neuroscience, 1st ed.; Binder, M.D., Hirokawa, N., Windhorst, U., Eds.; Springer: Berlin/Heidelberg, Germany, 2009; pp. 1941–1945. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).