
Indolent Adenocarcinoma In Situ Mistaken as Aggressive during Lung Cancer Screening Program: To Heal or to Harm?



Abstract

1. Introduction
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- Field, J.K.; Vulkan, D.; Davies, M.P.A.; Baldwin, D.R.; Brain, K.E.; Devaraj, A.; Eisen, T.; Gosney, J.; Green, B.A.; Holemans, J.A.; et al. Lung cancer mortality reduction by LDCT screening: UKLS randomised trial results and international meta-analysis. Lancet Reg. Health Eur. 2021, 10, 100179. [Google Scholar] [CrossRef] [PubMed]
- Voss, T.; Krag, M.; Martiny, F.; Heleno, B.; Jørgensen, K.J.; Brandt Brodersen, J. Quantification of overdiagnosis in randomised trials of cancer screening: An overview and re-analysis of systematic reviews. Cancer Epidemiol. 2023, 84, 102352. [Google Scholar] [CrossRef] [PubMed]
- Jett, J.R.; Midthun, D.E. Commentary: CT screening for lung cancer—Caveat emptor. Oncologist 2008, 13, 439–444. [Google Scholar] [CrossRef]
- Austin, J.H.; Garg, K.; Aberle, D.; Yankelevitz, D.; Kuriyama, K.; Lee, H.J.; Brambilla, E.; Travis, W.D. Radiologic implications of the 2011 classification of adenocarcinoma of the lung. Radiology 2013, 266, 62–71. [Google Scholar] [CrossRef]
- Moro-Sibilot, D.; Fievet, F.; Jeanmart, M.; Lantuejoul, S.; Arbib, F.; Laverribre, M.H.; Brambilla, E.; Brambilla, C. Clinical prognostic indicators of high-grade pre-invasive bronchial lesions. Eur. Respir. J. 2004, 24, 24–29. [Google Scholar] [CrossRef]
- Russell, P.A.; Wainer, Z.; Wright, G.M.; Daniels, M.; Conron, M.; Williams, R.A. Does lung adenocarcinoma subtype predict patient survival?: A clinicopathologic study based on the new International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society international multidisciplinary lung adenocarcinoma classification. J. Thorac. Oncol. 2011, 6, 1496–1504. [Google Scholar] [CrossRef]
- Silva, M.; Prokop, M.; Jacobs, C.; Capretti, G.; Sverzellati, N.; Ciompi, F.; van Ginneken, B.; Schaefer-Prokop, C.M.; Galeone, C.; Marchianò, A.; et al. Long-Term Active Surveillance of Screening Detected Subsolid Nodules is a Safe Strategy to Reduce Overtreatment. J. Thorac. Oncol. 2018, 13, 1454–1463. [Google Scholar] [CrossRef]
- Pastorino, U.; Boeri, M.; Sestini, S.; Sabia, F.; Milanese, G.; Silva, M.; Suatoni, P.; Verri, C.; Cantarutti, A.; Sverzellati, N.; et al. Baseline computed tomography screening and blood microRNA predict lung cancer risk and define adequate intervals in the BioMILD trial. Ann. Oncol. 2022, 33, 395–405. [Google Scholar] [CrossRef]
- Rami-Porta, R.; Bolejack, V.; Crowley, J.; Ball, D.; Kim, J.; Lyons, G.; Rice, T.; Suzuki, K.; Thomas, C.F., Jr.; Travis, W.D.; et al. IASLC Staging and Prognostic Factors Committee, Advisory Boards and Participating Institutions. The IASLC Lung Cancer Staging Project: Proposals for the Revisions of the T Descriptors in the Forthcoming Eighth Edition of the TNM Classification for Lung Cancer. J Thorac. Oncol. 2015, 10, 990–1003. [Google Scholar]
- Infante, M.; Berghmans, T.; Heuvelmans, M.A.; Hillerdal, G.; Oudkerk, M. Slow-growing lung cancer as an emerging entity: From screening to clinical management. Eur. Respir. J. 2013, 42, 1706–1722. [Google Scholar] [CrossRef] [PubMed]
- Godoy, M.C.; Sabloff, B.; Naidich, D.P. Subsolid pulmonary nodules: Imaging evaluation and strategic management. Curr. Opin Pulm. Med. 2012, 18, 304–312. [Google Scholar] [CrossRef]
- Zhang, T.; Li, X.; Liu, J. Prediction of the Invasiveness of Ground-Glass Nodules in Lung Adenocarcinoma by Radiomics Analysis Using High-Resolution Computed Tomography Imaging. Cancer Control 2022, 29, 10732748221089408. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D.; Brambilla, E.; Noguchi, M.; Nicholson, A.G.; Geisinger, K.R.; Yatabe, Y.; Beer, D.G.; Powell, C.A.; Riely, G.J.; Van Schil, P.E.; et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J. Thorac. Oncol. 2011, 6, 244–285. [Google Scholar] [CrossRef]
- Noguchi, M.; Morikawa, A.; Kawasaki, M.; Matsuno, Y.; Yamada, T.; Hirohashi, S.; Kondo, H.; Shimosato, Y. Small adenocarcinoma of the lung. Histol. Charact. Prognosis. Cancer 1995, 75, 2844–2852. [Google Scholar]
- Liu, J.; Yang, X.; Li, Y.; Xu, H.; He, C.; Zhou, P.; Qing, H. Predicting the Invasiveness of Pulmonary Adenocarcinomas in Pure Ground-Glass Nodules Using the Nodule Diameter: A Systematic Review, Meta-Analysis, and Validation in an Independent Cohort. Diagnostics 2024, 14, 147. [Google Scholar] [CrossRef]
- Ishida, H.; Shimizu, Y.; Sakaguchi, H.; Nitanda, H.; Kaneko, K.; Yamazaki, N.; Yanagihara, A.; Taguchi, R.; Sakai, F.; Yasuda, M.; et al. Distinctive clinicopathological features of adenocarcinoma in situ and minimally invasive adenocarcinoma of the lung: A retrospective study. Lung Cancer 2019, 129, 16–21. [Google Scholar] [CrossRef]
- Hasegawa, M.; Sone, S.; Takashima, S.; Li, F.; Yang, Z.G.; Maruyama, Y.; Watanabe, T. Growth rate of small lung cancers detected on mass CT screening. Br. J. Radiol. 2000, 73, 1252–1259. [Google Scholar] [CrossRef]
- Yousaf-Khan, U.; van der Aalst, C.; de Jong, P.A.; Heuvelmans, M.; Scholten, E.; Lammers, J.W.; van Ooijen, P.; Nackaerts, K.; Weenink, C.; Groen, H.; et al. Final screening round of the NELSON lung cancer screening trial: The effect of a 2.5-year screening interval. Thorax 2017, 72, 48–56. [Google Scholar] [CrossRef]
- Kadota, K.; Villena-Vargas, J.; Yoshizawa, A.; Motoi, N.; Sima, C.S.; Riely, G.J.; Rusch, V.W.; Adusumilli, P.S.; Travis, W.D. Prognostic significance of adenocarcinoma in situ, minimally invasive adenocarcinoma, and nonmucinous lepidic predominant invasive adenocarcinoma of the lung in patients with stage I disease. Am. J. Surg. Pathol. 2014, 38, 448–460. [Google Scholar] [CrossRef]
- Yotsukura, M.; Asamura, H.; Motoi, N.; Kashima, J.; Yoshida, Y.; Nakagawa, K.; Shiraishi, K.; Kohno, T.; Yatabe, Y.; Watanabe, S.I. Long-Term Prognosis of Patients with Resected Adenocarcinoma In Situ and Minimally Invasive Adenocarcinoma of the Lung. J. Thorac. Oncol. 2021, 16, 1312–1320. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Deng, C.; Wang, S.; Li, Y.; Zhang, Y.; Chen, H. Ten-year follow-up of lung cancer patients with resected adenocarcinoma in situ or minimally invasive adenocarcinoma: Wedge resection is curative. J. Thorac. Cardiovasc. Surg. 2022, 164, 1614–1622.e1. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Zhang, C.; Ye, X. Overdiagnosis and overtreatment of ground-glass nodule-like lung cancer. Asia Pac. J. Clin. Oncol. 2024, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ledda, R.E.; Funk, G.C.; Sverzellati, N. The pros and cons of lung cancer screening. Eur. Radiol. 2024, 1–9. [Google Scholar] [CrossRef]
- Nakamura, H.; Hirata, T.; Taguchi, M.; Kitamura, H. Ground-glass opacities showing an adenoma-to-carcinoma sequence in the lung. Gen. Thorac. Cardiovasc. Surg. 2008, 56, 421–423. [Google Scholar] [CrossRef]
- Kaneda, H.; Sakaida, N.; Saito, T.; Maniwa, T.; Uemura, Y.; Saito, Y. Appearance of bronchioloalveolar carcinoma and the rapid progression into invasive papillary adenocarcinoma. Gen. Thorac. Cardiovasc. Surg. 2009, 57, 224–227. [Google Scholar] [CrossRef]
- Sadohara, J.; Fujimoto, K.; Terasaki, H.; Nonoshita, M.; Hayabuchi, N. Bronchioloalveolar carcinoma with fluctuating extent of consolidation on chest radiography. J. Thorac. Imaging 2004, 19, 63–66. [Google Scholar] [CrossRef]
- Shaw, J.P.; Bejarano, P.A.; Thurer, R.J. Pseudocavitating bronchioloalveolar carcinoma followed over a decade. Ann. Thorac. Surg. 2008, 85, 1432–1434. [Google Scholar] [CrossRef]
- Ichinose, J.; Kohno, T.; Fujimori, S.; Harano, T.; Suzuki, S.; Fujii, T. Invasiveness and malignant potential of pulmonary lesions presenting as pure ground-glass opacities. Ann. Thorac. Cardiovasc. Surg. 2014, 20, 347–352. [Google Scholar] [CrossRef]
- Sekihara, K.; Yoshida, J.; Oda, M.; Oki, T.; Ueda, T.; Ito, T.; Miyoshi, T.; Aokage, K.; Tane, K.; Tsuboi, M. Delayed cut-end recurrence after wedge resection for pulmonary ground-glass opacity adenocarcinoma despite negative surgical margin. Gen. Thorac. Cardiovasc. Surg. 2020, 68, 644–648. [Google Scholar] [CrossRef]
- Yano, Y.; Mori, M.; Kagami, S.; Fushitani, K.; Sugano, T.; Namba, Y.; Yoneda, T.; Yokota, S.; Maeda, H.; Ueda, K. Inflammatory pseudotumor of the lung with rapid growth. Intern Med. 2009, 48, 1279–1282. [Google Scholar] [CrossRef] [PubMed]
- Heidinger, B.H.; Anderson, K.R.; Nemec, U.; Costa, D.B.; Gangadharan, S.P.; VanderLaan, P.A.; Bankier, A.A. Lung Adenocarcinoma Manifesting as Pure Ground-Glass Nodules: Correlating CT Size, Volume, Density, and Roundness with Histopathologic Invasion and Size. J. Thorac. Oncol. 2017, 12, 1288–1298. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Harada, T.; Fuke, S.; Konishi, J.; Yamazaki, K.; Kaji, M.; Morikawa, T.; Ota, S.; Itoh, T.; Dosaka-Akita, H.; et al. Lung adenocarcinoma presenting with enlarged and multiloculated cystic lesions over 2 years. Respir. Care 2004, 49, 1522–1524. [Google Scholar] [PubMed]
- Nagata, M.; Otani, S.; Kanai, Y.; Yamamoto, S.; Tsubochi, H.; Endo, S. Laser-Trélat sign improved after the resection of a tiny ground-grass nodule: A case report. J. Surg. Case Rep. 2021, 2021, rjab275. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
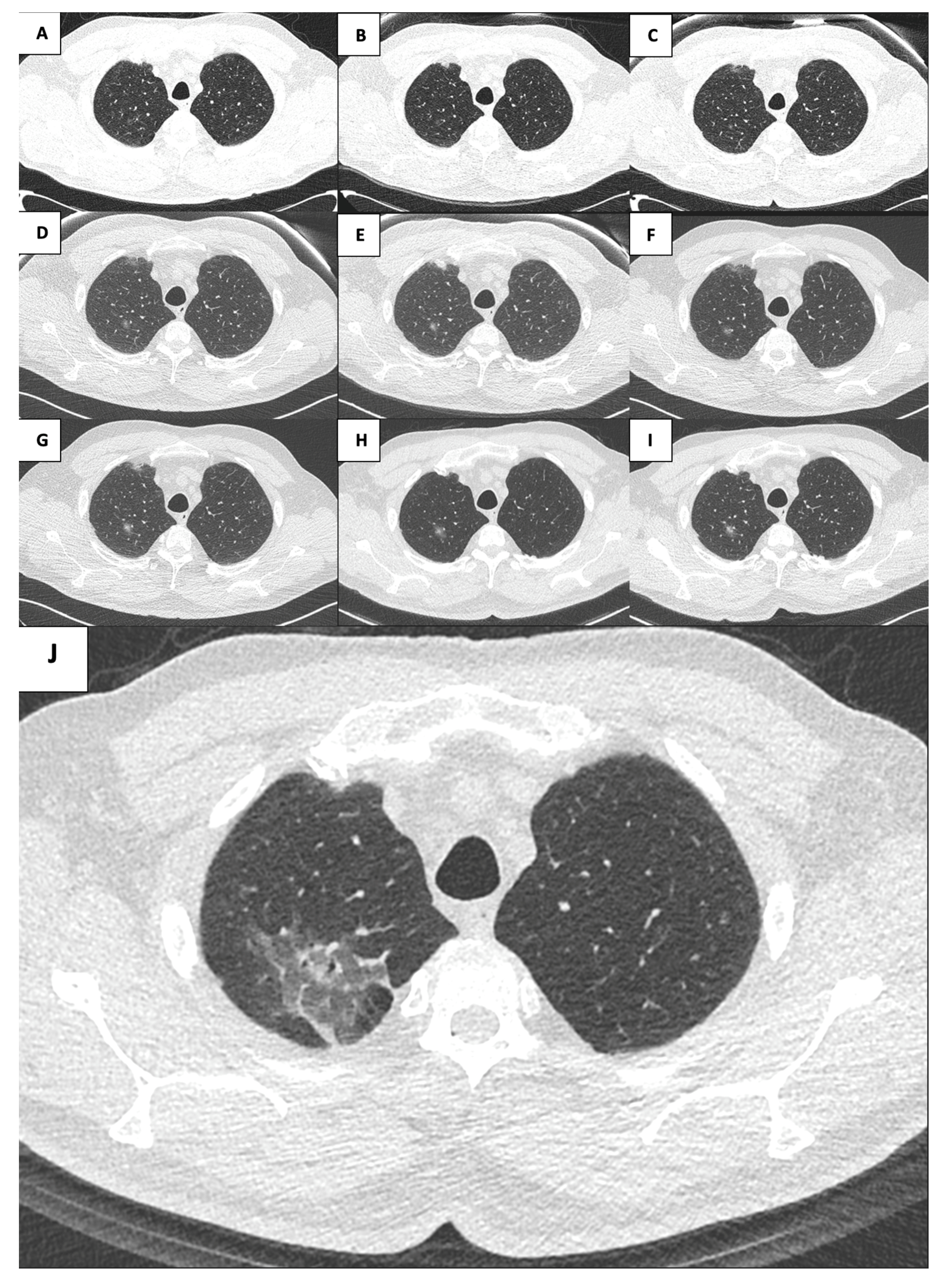
| Year | Dimension mm | Density HU | Solid Component mm3 |
|---|---|---|---|
| 2015 | 13.60 × 8.70 | −158 | 0 |
| 2016 | 11.50 × 9.00 | −292 | 0 |
| 2017 | 11.10 × 7.90 | −244 | 0 |
| 2018 | 15.00 × 8.50 | −190 | 47 |
| 2019 | 19.10 × 10.80 | −314 | 41 |
| 2020 | 16.90 × 10.30 | −208 | 145 |
| 2021 | 49.80 × 37.80 | −581 | 390 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orlandi, R.; Mattioni, G.; Rolli, L.; Pastorino, U. Indolent Adenocarcinoma In Situ Mistaken as Aggressive during Lung Cancer Screening Program: To Heal or to Harm? Surgeries 2024, 5, 867-874. https://doi.org/10.3390/surgeries5030070
Orlandi R, Mattioni G, Rolli L, Pastorino U. Indolent Adenocarcinoma In Situ Mistaken as Aggressive during Lung Cancer Screening Program: To Heal or to Harm? Surgeries. 2024; 5(3):867-874. https://doi.org/10.3390/surgeries5030070
Chicago/Turabian StyleOrlandi, Riccardo, Giovanni Mattioni, Luigi Rolli, and Ugo Pastorino. 2024. "Indolent Adenocarcinoma In Situ Mistaken as Aggressive during Lung Cancer Screening Program: To Heal or to Harm?" Surgeries 5, no. 3: 867-874. https://doi.org/10.3390/surgeries5030070
APA StyleOrlandi, R., Mattioni, G., Rolli, L., & Pastorino, U. (2024). Indolent Adenocarcinoma In Situ Mistaken as Aggressive during Lung Cancer Screening Program: To Heal or to Harm? Surgeries, 5(3), 867-874. https://doi.org/10.3390/surgeries5030070