Abstract
Introduction: Patients receiving bariatric surgery are at risk for sleep apnea (OSA) and need extensive surveillance in the postoperative period. There is evidence of respiratory events (RE) several hours after leaving PACU. We analyzed the late onset of RE in patients recovering from bariatric surgery and their opiate requirements through the first night after surgery. Methods: We studied 52 patients with OSA and 38 non-OSA patients. Preoperative studies comprised meticulous OSA evaluation for all patients and computing the predictive score PRODIGY to stratify for the risk of RE. All patients received intraoperative multimodal non-opioid anesthesia. After PACU recovery, patients were admitted to a ward and continuously monitored for pulse oximetry, heart rate, and acoustic respiratory rate for up to 18 h using MASIMO RAD-97 and TRACE software (Masimo, USA). Results: All patients showed a progressing reduction in the frequency of RE after admission to the floor. Desaturations and bradypnea, however, increased significantly for a second peak between 14 and 16 h in the OSA group. The opiate doses administered to OSA and non-OSA patients were not different and remained low during the increases in RE. Discussion: After bariatric surgery, patients with OSA show significant late-desaturation and bradypnea events. Opiate administration cannot be invoked as the cause.
1. Introduction
Patients undergoing bariatric surgery are at a particularly increased risk for obstructive sleep apnea (OSA), with a prevalence of OSA between 35 and 94% [1]. This high number, combined with a higher risk of postoperative complications following surgery in patients with OSA, has made screening for OSA a significant focus in bariatric surgery [2,3]. However, an analysis of perioperative management of OSA guidelines has found that only half of the guidelines could be recommended as published, with improvement needs, particularly within stakeholder involvement and applicability [4]. In particular, postoperative respiratory depression has become critical in caring for these patients. The recently derived PRODIGY score, which evaluates the risk for respiratory depression in inpatient wards, emphasizes sleep disorders, particularly OSA [5]. This score was derived from opioid-induced respiratory depression associated with an increased chance for readmission, cost, and longer length of stay [6]. These findings are particularly exacerbated in patients with OSA, with increased sensitivity to the respiratory depressive effects of opioids being proposed within this population [7]. The distribution of respiratory events has been unevenly distributed, with the frequency of these events peaking late, up to 16 h after surgery [8]. Ishikawa et al. also found that desaturation events peaked at 14 h following extubation, while the incidence of bradypnea continually decreased following extubation [9].
We sought to evaluate how the timing of opiate administration related to the frequency of respiratory events and compare differences in how patients with and without OSA reacted to opiate administration overnight following bariatric surgery. This group of patients was not previously studied regarding postoperative respiratory compromise.
2. Methods
The University of South Florida IRB approved this study with protocol number Pro00036836 (second extension). All patients signed the informed consent. Patients underwent bariatric surgery between February 2022 and May 2023, most commonly a Roux-en-Y gastric bypass (53 patients) or insertion of a gastric sleeve (23 patients). We included 52 patients with OSA and 38 patients without OSA. Patient’s (19–70 year) preoperative studies comprised meticulous OSA evaluation for all patients. Those screened high-risk for OSA, with STOP-BANG 3+ or ESS 10+, underwent polysomnography (PSG). Patients using CPAP were evaluated for compliance > 70% extended more than 4 days per week before surgery. Preoperative preparation included OSA evaluation for all patients, sleep studies for severe OSA grades, and evaluation of risk for respiratory depression (low, intermediate, or high) using the PRODIGY scoring. Moderate to severe OSA evaluation comprised STOP-bang value >3 or Epworth Sleepiness Scale (ESS) > 10. The majority of patients studied who received gastric bypass or gastric sleeve surgery had been diagnosed with obstructive sleep apnea (OSA). They were actively using a CPAP or nasal PAP during sleep. Patients with known OSA were required to comply with PAP therapy to qualify for surgery. PAP machine compliance was defined as >70% usage in the following categories: usage 5+ nights per week and used for 4+ hours a night; compliance maintenance was updated every 3 months in the preoperative period and again the week before surgery.
In addition, all patients received multimodal intraoperative non-opioid anesthesia; at our institution, low or no-opioid anesthesia is becoming the new standard for surgery and is in managing agreement with published consensus [1,10].
Additionally, we utilized the predictive score PRODIGY to stratify for the risk of respiratory depression events (RE) [5]. All patients received multimodal intraoperative non-opioid or very-low opioid anesthesia. Patients with OSA were treated with positive pressure therapy (PPT) after surgery. After PACU recovery, patients were admitted to a ward and continuously monitored utilizing the MASIMO RAD-97 (Masimo, Irvine, CA, USA), which uses acoustic respiratory monitoring to determine the respiratory rate. We carefully compiled every 2 h the postoperative opiate analgesics, which included small boluses of fentanyl (25 mcg), morphine (2 mg IV), or oxycodone (5 mg). Non-opiate analgesics included magnesium chloride, ketorolac, and cyclobenzaprine. All respiratory variables were continuously collected through TRACE software (Masimo, USA) for pulse oximetry, heart rate, acoustic respiratory rate, and perfusion index every 2 h up to 18 h, but with the termination of monitoring at 7:00 a.m. the morning following surgery. Patients’ data were only counted if the timing of respiratory monitoring exceeded 8 h, which excluded some patients from completing the initial collection. Table 1 shows the characteristics of all patients evaluated.

Table 1.
Patient characteristics.
Masimo TRACE basic software-provided data were used to count RE (desaturation events: oxygen saturation < 89% for >30 s or desaturation of 3% below baseline for >30 s; bradypnea: respiratory rate < 10 breaths/min for >30 s).
Statistical Analysis
Statistical comparisons were obtained by Mann–Whitney U test, Wilcoxon signed-rank test, Kruskal–Wallis test, Dwass–Steel–Critchlow–Fligner test, 2 samples 2-sided T-test, Chi-squared test, and paired 2-sided sample T-tests for various criteria. Mann–Whitney U tests were performed to compare patients with OSA to patients without OSA for frequency of RE. Opioid usage between OSA and non-OSA patients was evaluated via 2-sample 2-sided T-tests. Wilcoxon signed-rank test and paired 2-sided sample T-tests were utilized to compare RE and opioid usage, respectively, between the various periods. The Kruskal–Wallis test was used to compare the three PRODIGY levels (low, intermediate, and high), and the Dwass–Steel–Critchlow–Fligner test was performed for specific post hoc contrast.
3. Results
Intraoperative MME (IV milligram morphine equivalents) were, on average, 1.7 mg during the 3 h and 20 min surgery and 4.4 mg, respectively, during the PACU stay, lasting 2 h and 26 min; the average duration of monitoring after PACU discharge was 15 h and 2 min. Patients’ REs are summarized in Table 2. There were 724 total desaturation events and 210 total bradypnea events. In our study group, 40% of patients experienced a desaturation event, while 49% experienced bradypnea. A total of 54% of patients with OSA experienced at least one desaturation event, and 56% had at least one bradypnea event. These numbers were 21% and 39% for patients without OSA, respectively.
Table 2.
Comparison of respiratory events and MME after PACU discharge (mg IV morphine equivalents).
The table shows that the number of RE in OSA patients was significantly higher than for non-OSA patients. Specifically, OSA status was significantly associated with a higher number of desaturation events (mean 12.7, median 1: IQR (0–11.25) vs. non-OSA (1.7, 0: IQR (0–0)) p < 0.001) and similarly for bradypnea (3.7, 1: IQR (0–3) vs. 1.0, 0: IQR (0–1) p = 0.035).
OSA patients had a progressive reduction in the frequency of RE during the first few hours after admission to the floor (Figure 1A). This peak for OSA patients from 0 to 6 h was significantly different from the trough from 6 to 10 h when the desaturation events of the periods were compared (p = 0.008). In addition, desaturations increased significantly for a second peak between 14 and 16 h compared to the trough between 6 and 10 h (p = 0.045). For bradypnea, a similar trend is seen; however, a comparison of the peak at 8 to 14 h and the trough at 6 to 8 h did not show any significant differences (p = 0.078) (Figure 1B). These previous two peaks are particularly evident in the eight patients with a high PRODIGY score, all of whom had OSA. However, the exact comparisons in this group with high PRODIGY scores were insignificant (p = 0.371, 0.289, respectively, for desaturations and bradypnea). The distribution during the overnight monitoring did not reveal increased doses of opioid administration in concert with increases in RE. In addition, the opiate doses administered at night to OSA and non-OSA patients were not different (Figure 2).
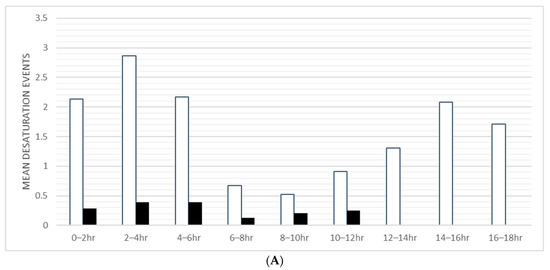
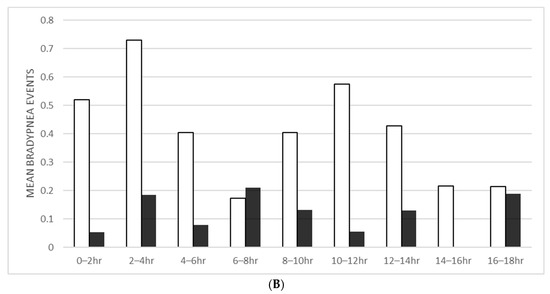
Figure 1.
(A) Mean desaturation events (oxygen saturation < 89% for >30 s or desaturation of 3% below baseline for >30 s) by OSA status vs. time after leaving PACU. (B) Mean bradypnea events (Respiratory rate < 10 breaths/min for >30 s) by OSA status vs. time after leaving PACU. (OSA 52 patients; non-OSA 38 patients.)
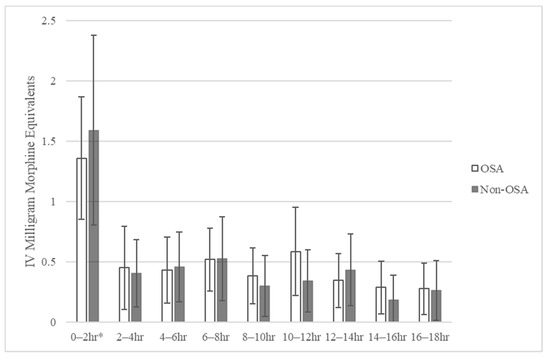
Figure 2.
Average MME (IV morphine) for OSA and non-OSA patients every 2 h after leaving PACU: OSA 52 patients, non-OSA 38 patients (* = significantly different MME from 0 to 2 h when compared to 2–18 h, p < 0.001; error bars represent a 95% confidence interval).
Kruskal–Wallis test comparisons between various PRODIGY levels (low, intermediate, and high) revealed a significant difference between the three groups for RE, desaturation events, and bradypnea events in the whole cohort regardless of OSA status (p < 0.001 for all). The difference in total RE, desaturation events, and bradypnea for patients with OSA by PRODIGY score was also significant in this same analysis (p = 0.013 for all). Comparisons between high and low PRODIGY score patients were significant via the Dwass–Steel–Critchlow–Fligner test for each type of event both for the overall cohort and when performed for patients with OSA only (Table 3). A similar observation was also accurate for high and intermediate PRODIGY score patients, except for the whole cohort compared to bradypnea events (p = 0.051 for this analysis). No significant differences were discovered on the Dwass–Steel–Critchlow–Fligner test between intermediate and low PRODIGY score patients. OSA status was also a substantial factor significantly differentiating low PRODIGY Score patients in terms of desaturation events (median: 0 (IQR 0–4.25) for OSA; median: 0 (IQR 0–0) for non-OSA, p = 0.043).
Table 3.
PRODIGY score and respiratory depression events.
Most patients with OSA received the first surgery of the day at a 7:30 a.m. induction time, leading to arrival on the general care floor by 17:00. This group of 39 patients could be evaluated by the absolute clock time for the onset of their RE, and it was re-analyzed separately (Figure 3). These patients saw a peak in desaturation events from 16:00 to 18:00 and a second surge from 04:00 to 06:00 the morning following surgery. This later peak again appears unrelated to opioid usage, as most opioids were administered while still in PACU, as seen in Figure 3, with most opiates on the general care floor given within the first 2 h only. The correlation coefficient between mean MME and respiratory events from 12:00 to 06:00 in the 2 h intervals was 0.049, demonstrating the lack of relationship. The trend shown in these patients matches those seen in Figure 1A.
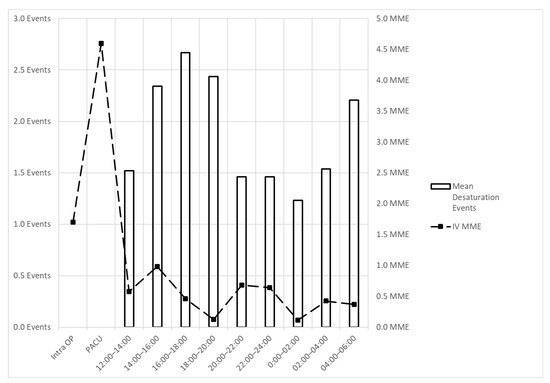
Figure 3.
Mean desaturation events and MME (IV morphine) vs. clock time (time of day) for 1st surgery of the day patients with OSA (39 patients).
4. Discussion
Patients with OSA have been consistently described as more likely to experience postoperative complications. Memtsoudis et al. found sleep apnea a risk factor for aspiration pneumonia, ARDS, and intubation/mechanical ventilation for orthopedic and general surgical procedures [11]. Patients with acute respiratory failure post-major abdominal surgery have a 40–65% mortality rate and decreased 5- and 10-year survival [12]. Thirty days after major noncardiac surgery, OSA had almost a 50% increased risk for cardiovascular complications (hazard ratio = 1.49; 95% CI = 1.19–2.01) [13]. For patients at high risk for atelectasis following major abdominal surgery, CPAP utilization prevents endotracheal intubation in those who develop early hypoxemia [14]. Despite these observations, a specific evaluation of the dangers of bariatric surgery patients has not been proposed. Our results demonstrate that obesity surgery similarly carries postoperative RE risks.
Previous studies have described the frequency and temporal distribution of postoperative respiratory events. A survey of 1024 patients utilizing an acoustic respiratory rate device to determine desaturation (SpO2 < 90% for > 10 s) and bradypnea (rate < 8 breaths/min for >2 min) saw 12.1% and 5.1% of patients experience desaturation and bradypnea, respectively [9]. In addition, they saw a peak for desaturation at 14 h post-extubation; this would be comparable to our 12–14 h interval given our average PACU stay exceeding 2 h. There also was a smaller peak from 6 to 8 h, like our 4–6 h interval. Their values progressively decreased after extubation for bradypnea, with their rise at 0–1 h post-extubation. This finding is similar to our own and suggests there may be an early peak 2–4 h after arrival on a general care floor, but we also see a second rise in bradypnea from the 10 to 12 h mark, which is less visible in their data [9].
The PRODIGY score was developed to subdivide patients into categories of high, intermediate, or low to stratify for the risk of opiate-induced respiratory depression [5]. The opiates utilized in our patients were low, with a median IV MME value of 2.5 (7.5 oral MME) during monitoring. In Khanna et al., patients with no respiratory depression episodes had a median MME value of 20 mg, which would be almost double ours if referring to oral MME (however, their duration of monitoring was longer with a median of 24 h). Our findings suggest that the difference between high and intermediate/low patients is much more significant than between intermediate and low PRODIGY scores. In addition, with careful OSA screening as we performed, it is worthwhile to consider patients with OSA at higher risk, regardless of their PRODIGY category. Our discussion for the intermediate/high PRODIGY score patients is more limited, as there were only four non-OSA patients with an intermediate PRODIGY score and none with a high PRODIGY score.
Driver et al. evaluated postsurgical patients in the PRODIGY trial at two hospital sites. They utilized capnography to record respiratory events and observed a peak in respiratory events between 2:00 and 4:00 a.m. In addition, they saw a single rise in the number of respiratory depression episodes they watched, with a median value of 15.7 h after surgery. However, we noted a bimodal distribution; this can at least be partly explained by the methodology utilized in their process. They did not mandate the application of capnography at a particular point, nor did they record when admission to the general care floor was [8]. Thus, if monitoring was started later for patients than in our analysis, they may have missed the first peak described from 0 to 6 h after arriving on the general care floor. For patients in our study who were within the first group of patients undergoing surgery each day, the trend for desaturation events seen after PACU discharge for patients with OSA was again noted when the time was altered to the time of day.
We previously evaluated the presence of respiratory events during a shorter observation time limited to the PACU stay following bariatric surgery [15]. There was no difference in the number of respiratory events depending on the PRODIGY score, but patients with OSA had significantly more respiratory events than patients without OSA (1.8 vs. 0.5, p = 0.0002). We attributed this to the early CPAP utilization in the PACU and opioid-free or opioid-sparing analgesia [14]. Of note, we previously utilized capnography and pulse oximetry to detect respiratory events (Capnostream 35, Medtronic Inc., Minneapolis, MN, USA and Profox Respiratory Oximetry software), in contrast to our current approach utilizing acoustic respiratory monitoring and pulse oximetry (MASIMO RAD 97 with TRACE software). Compliance was much higher using this new approach, with no patient removing the acoustic monitor during the screening. On the other hand, it was common for patients under capnography monitoring to remove the device, citing discomfort. This advantage for acoustic respiratory tracking was noted, though capnography and acoustic monitoring were comparable in efficacy [16].
Robotic surgery was exclusively utilized in our patients, with either the Roux-en-Y gastric bypass or the sleeve gastrectomy most performed. Using robotics in fields other than bariatric surgery has shown decreased pain compared to other approaches [17]. However, research in bariatric surgery regarding pain or opiate consumption utilizing a robotic approach is lacking.
Opiate usage has the potential to increase following bariatric surgery, particularly in patients who previously were daily opioid users before surgery [18]. There is also a small population with no preoperative opiate usage, which increases use afterward [19]. Thus, recommendations to prescribe fewer and shorter-duration opiate analgesics have been popularized [18]. As a result, our patients received low to no opiate analgesia during and after surgery.
Monitoring of opiate usage in patients concurrently with respiratory events has not been previously described in the literature to our knowledge. Thus, our data suggest that there may be a strong relationship between opiate usage and respiratory events, particularly within the first 6 h post-admission to the floor after PACU discharge. Despite this appearing to be the case, it is of note that we used particularly low doses of opiates in our patients. Patients received only 5 MME (IV morphine equivalents) on average (median = 2.5 IV MME) within the duration of their monitoring; the peak opiate usage was seen within the first two hours of monitoring and was most commonly 12.5 or 25 mg fentanyl boluses. However, opiate use does not increase, with the last peak in respiratory events seen later from 12 to 16 h. Therefore, we suggest that OSA patients tend to desaturate and experience bradypnea regardless of positive pressure therapy and despite low or no opiate usage.
Limitations of our observations stem from the variety of surgical interventions, from gastric bypass to insertion of gastric sleeve, the variable range of patients’ BMI, from 25 up to 67 kg/m2, to the diverse techniques of three surgeons. However, anesthesia methods and drugs were closely standardized, and opioid utilization was limited. All patients received laparoscopic robot-aided surgery, postoperative respiratory pressure support if OSA-positive, and active early mobilization. Variations in the duration of respiratory monitoring and the end of the surgery made it more challenging to establish a pattern of what time of day is most risky for patients. Despite these limitations, there were also no respiratory depression events that required clinical nursing or physician intervention during monitoring, so it is unclear as to the significance of these events postoperatively. Due to software limitations, we could not measure direct apnea events as reported in previous studies; thus, bradypnea events encompass bradypnea and apnea. Finally, the patient population undergoing bariatric surgery at our hospital was predominantly female with lower PRODIGY scores than what was seen in the initial study by Khanna et al. This observation makes it more challenging to pinpoint conclusions based on the PRODIGY score, particularly seeing only four non-OSA patients with an intermediate score and none with a high score.
5. Conclusions
After bariatric surgery, patients with OSA have significantly more desaturation and bradypnea events, displaying a bimodal peak. A second peak was previously described in the literature for different groups of patients [8,9]. In our patients, however, opioid administration did not increase during the monitoring period and cannot be invoked as a cause for the increased number of respiratory depression events. Systematic OSA screening can also correctly identify patients at risk for respiratory depression events. Despite optimization with preoperative screening, opioid-sparing, and ERAS protocols, these patients still experience respiratory depression, though, fortunately, at a mild level. OSA is thus a significant obesity-related co-morbidity requiring careful and extended monitoring, which could not be provided in an ambulatory setting.
Author Contributions
Conceptualization, E.C.; Methodology, E.C.; Software, E.C.; Validation, C.P.; Formal analysis, C.P., G.M., M.B. and E.C.; Investigation, C.P., A.M., C.D., S.D. and E.C.; Resources, E.C.; Data curation, C.P. and E.C.; Writing—original draft, C.P., G.M. and E.C.; Writing—review and editing, C.P., G.M., M.B. and E.C.; Project administration, A.M., C.D., S.D. and E.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The University of South Florida IRB approved this study with protocol number Pro00036836 (second extension).
Informed Consent Statement
Informed consent was obtained in writing from all subjects involved in the study.
Data Availability Statement
All data obtained can be gladly shared upon appropriate request to the corresponding author.
Acknowledgments
Masimo provided equipment support in part for the monitoring use of RAD-97 and the software use of TRACE.
Conflicts of Interest
The authors declare no conflict of interest.
References
- de Raaff, C.A.; Gorter-Stam, M.A.; de Vries, N.; Sinha, A.C.; Bonjer, H.J.; Chung, F.; Coblijn, U.K.; Dahan, A.; Helder, R.S.V.D.; Hilgevoord, A.A.; et al. Perioperative management of obstructive sleep apnea in bariatric surgery: A consensus guideline. Surg. Obes. Relat. Dis. 2017, 13, 1095–1109. [Google Scholar] [CrossRef] [PubMed]
- Devaraj, U.; Rajagopala, S.; Kumar, A.; Ramachandran, P.; Devereaux, P.J.; D’Souza, G.A. Undiagnosed Obstructive Sleep Apnea and Postoperative Outcomes: A Prospective Observational Study. Respiration 2017, 94, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Reed, K.; Pengo, M.F.; Steier, J. Screening for sleep-disordered breathing in a bariatric population. J. Thorac. Dis. 2016, 8, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Tian, C.; Hyman, J.B.; Siddiqui, S.; Auckley, D.; Khanna, A.K.; Wong, J.; Englesakis, M.; Singh, K.P.; Ramachandran, S.K. Level of Evidence of Guidelines for Perioperative Management of Patients with Obstructive Sleep Apnea: An Evaluation Using the Appraisal of Guidelines for Research and Evaluation II Tool. Anesth. Analg. 2023, 136, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Khanna, A.K.; Bergese, S.D.; Jungquist, C.R.; Morimatsu, H.; Uezono, S.; Lee, S.; Ti, L.K.; Urman, R.D.; McIntyre, R.; Tornero, C.; et al. Prediction of Opioid-Induced Respiratory Depression on Inpatient Wards Using Continuous Capnography and Oximetry: An International Prospective, Observational Trial. Anesth. Analg. 2020, 131, 1012–1024. [Google Scholar] [CrossRef] [PubMed]
- Dahan, A.; Aarts, L.; Smith, T.W. Incidence, Reversal, and Prevention of Opioid-induced Respiratory Depression. Anesthesiology 2010, 112, 226–238. [Google Scholar] [CrossRef]
- Cozowicz, C.; Chung, F.; Doufas, A.G.; Nagappa, M.; Memtsoudis, S.G. Opioids for Acute Pain Management in Patients With Obstructive Sleep Apnea: A Systematic Review. Anesth. Analg. 2018, 127, 988–1001. [Google Scholar] [CrossRef] [PubMed]
- Driver, C.N.; Laporta, M.L.; Bergese, S.D.; Urman, R.D.; Di Piazza, F.; Overdyk, F.J.; Sprung, J.; Weingarten, T.N. Frequency and Temporal Distribution of Postoperative Respiratory Depressive Events. Anesth. Analg. 2021, 132, 1206–1214. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, M.; Sakamoto, A. Postoperative desaturation and bradypnea after general anesthesia in non-ICU patients: A retrospective evaluation. J. Clin. Monit. Comput. 2020, 34, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Epie, N.; Budiansky, A.S. Perioperative Pain Management in Bariatric Anesthesia. Saudi J. Anaesth. 2022, 16, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Memtsoudis, S.; Liu, S.S.; Ma, Y.; Chiu, Y.L.; Walz, J.M.; Gaber-Baylis, L.K.; Mazumdar, M. Perioperative pulmonary outcomes in patients with sleep apnea after noncardiac surgery. Anesth. Analg. 2011, 112, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Ferreyra, G.; Long, Y.; Ranieri, V.M. Respiratory complications after major surgery. Curr. Opin. Crit. Care. 2009, 15, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.T.V.; Wang, C.Y.; Seet, E.; Tam, S.; Lai, H.Y.; Chew, E.F.F.; Wu, W.K.K.; Cheng, B.C.P.; Lam, C.K.M.; Short, T.G.; et al. Association of Unrecognized Obstructive Sleep Apnea With Postoperative Cardiovascular Events in Patients Undergoing Major Noncardiac Surgery. JAMA 2019, 321, 1788–1798. [Google Scholar] [CrossRef] [PubMed]
- Squadrone, V.; Coha, M.; Cerutti, E.; Schellino, M.M.; Biolino, P.; Occella, P.; Belloni, G.; Vilianis, G.; Fiore, G.; Cavallo, F.; et al. Continuous positive airway pressure for treatment of postoperative hypoxemia: A randomized controlled trial. JAMA 2005, 293, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Ambert, M.; Reddy, N.; Melloni, G.; Balouch, M.; Sujka, J.; Mooney, A.; DuCoin, C.; Camporesi, E. Respiratory Monitoring after Opioid-Sparing Bariatric Surgery in Patients with Obstructive Sleep Apnea (OSA). Surgeries 2023, 4, 26–35. [Google Scholar] [CrossRef]
- Mimoz, O.; Benard, T.; Gaucher, A.; Frasca, D.; Debaene, B. Accuracy of respiratory rate monitoring using a non-invasive acoustic method after general anesthesia. Br. J. Anaesth. 2012, 108, 872–875. [Google Scholar] [CrossRef] [PubMed]
- Yaxley, J.W.; Coughlin, G.D.; Chambers, S.K.; Occhipinti, S.; Samaratunga, H.; Zajdlewicz, L.; Dunglison, N.; Carter, R.; Williams, S.; Payton, D.J.; et al. Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: Early outcomes from a randomized controlled phase 3 study. Lancet 2016, 388, 1057–1066. [Google Scholar] [CrossRef] [PubMed]
- Heinberg, L.J.; Pudalov, L.; Alameddin, H.; Steffen, K. Opioids and bariatric surgery: A review and suggested recommendations for assessment and risk reduction. Surg. Obes. Relat. Dis. 2019, 15, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Raebel, M.A.; Newcomer, S.R.; Bayliss, E.A.; Boudreau, D.; DeBar, L.; Elliott, T.E.; Ahmed, A.T.; Pawloski, P.A.; Fisher, D.; Toh, S.; et al. Chronic opioid use emerging after bariatric surgery. Pharmacoepidemiol. Drug Saf. 2014, 23, 1247–1257. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).