
Esophageal Stent in Sleeve Gastrectomy Leak Treatment: Observations Based on a Challenging Surgical Case and Literature

 ,
,  , and
, and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
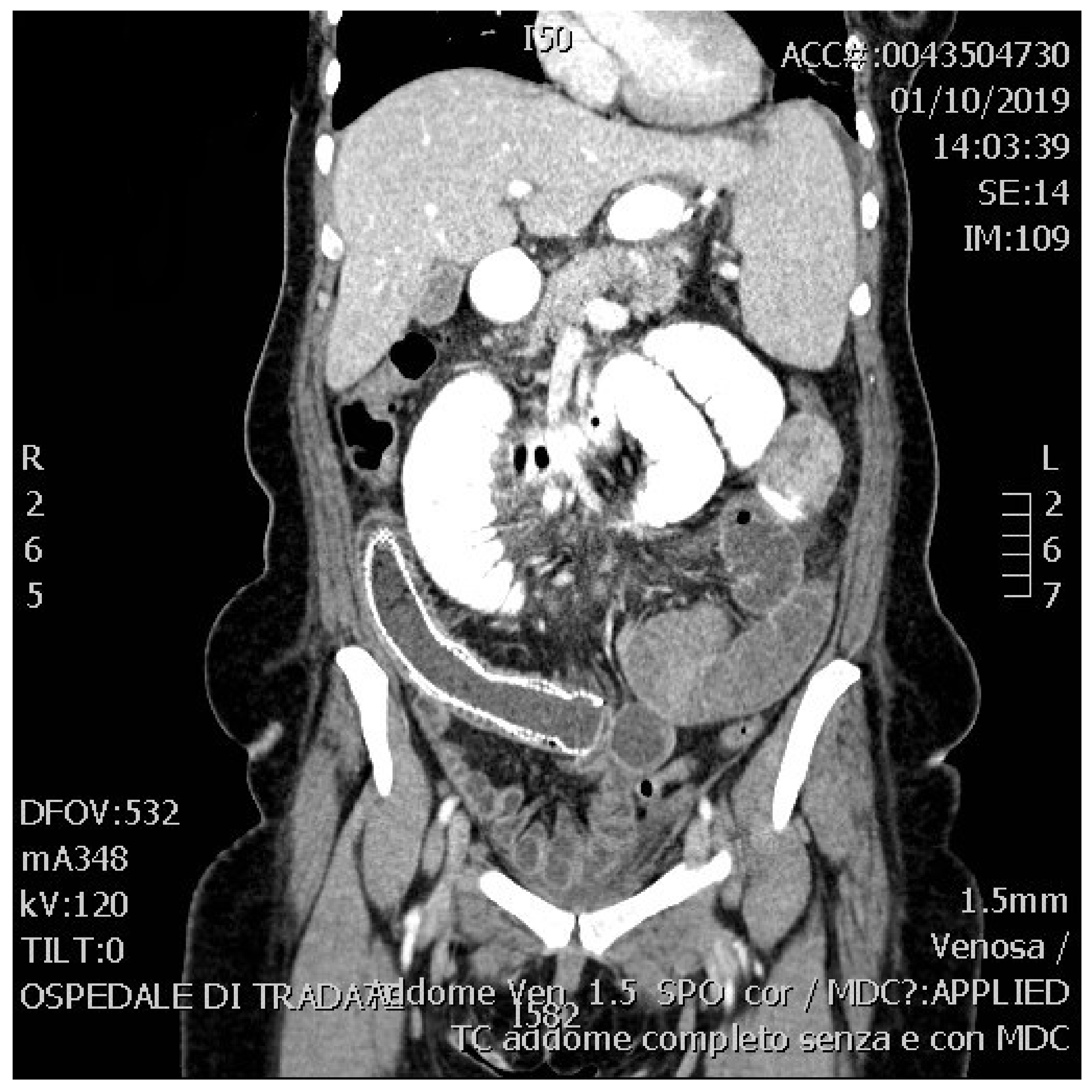
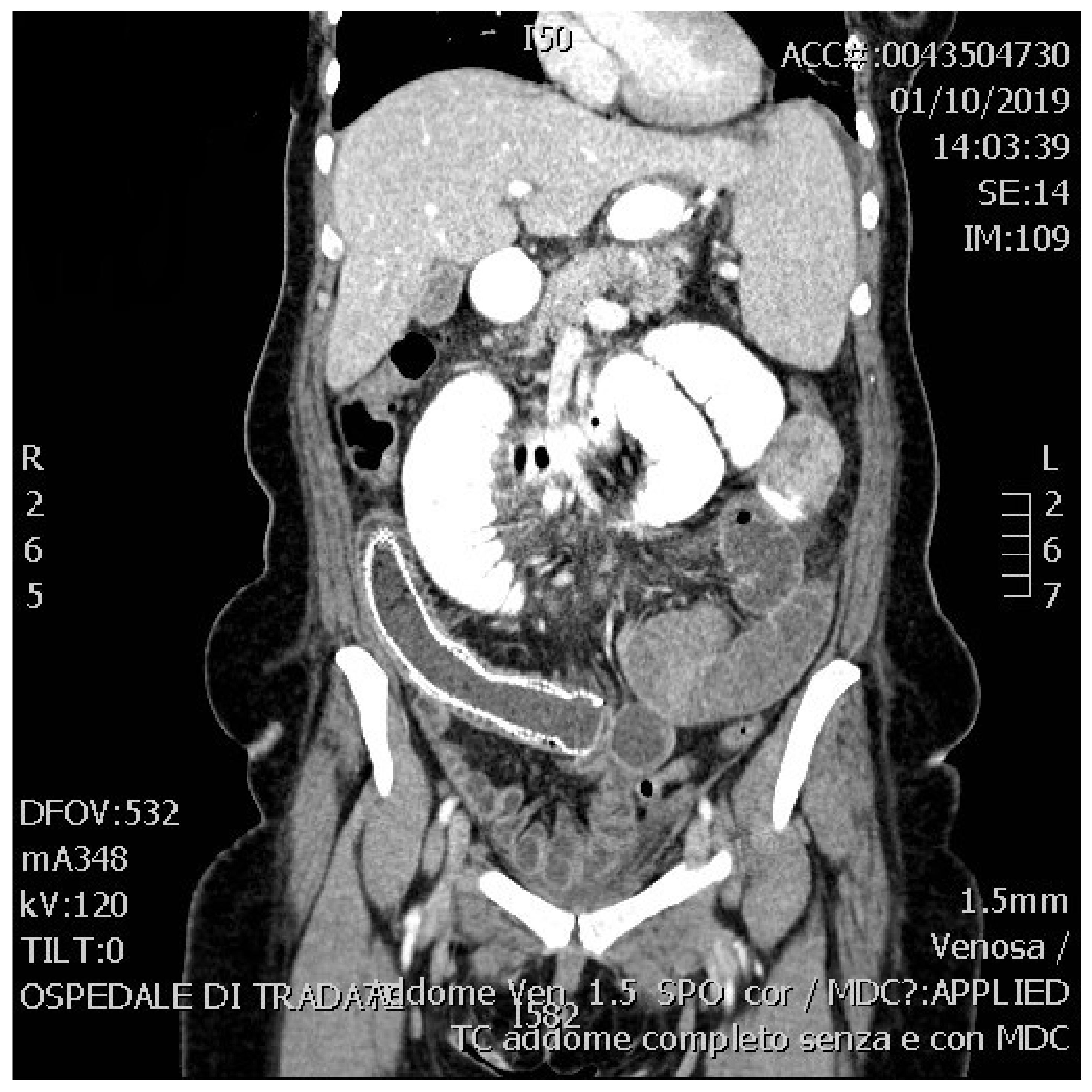
2. Presentation of the Case
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Angrisani, L.; Santonicola, A.; Iovino, P.; Vitiello, A.; Higa, K.; Himpens, J.; Buchwald, H.; Scopinaro, N. IFSO worldwide survey 2016: Primary, endoluminal and revisional procedures. Obes. Surg. 2018, 28, 3783–3794. [Google Scholar] [CrossRef] [PubMed]
- Gagner, M.; Buchwald, J.N. Comparison of laparoscopic sleeve gastrectomy leak rate in four staple-line reinforcement options: A systematic review. Surg. Obes. Relat. Dis. 2014, 10, 713–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nedelcu, M.; Manos, T.; Cotirlet, A.; Noel, P.; Gagner, M. Outcome of leaks after sleeve gastrectomy based on a new algorithm adressing leak size and gastric stenosis. Obes. Surg. 2015, 25, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Gjeorgjievski, M.; Imam, Z.; Cappell, M.S.; Jamil, L.H.; Kahaleh, K. A comprehensive review of endoscopic management of sleeve gastrectomy leaks. J. Clin. Gastroenterol. 2021, 7, 551–576. [Google Scholar]
- Emile, S.H.; Elfeki, H.; Elalfy, K.; Abdallah, E. Laparoscopic sleeve gastrectomy then and now: An updated systematic review of the progress and short-term outcomes over the last 5 years. Surg. Laparosc. Endosc. Percutan. Tech. 2017, 27, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Iossa, A.; Abdelgawad, M.; Watkins, B.M.; Silecchia, G. Leaks after laparoscopic sleeve gastrectomy: Overview of pathogenesis and risk factors. Langenbeck’s Arch. Surg. 2016, 401, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, R.J.; Diaz, A.A.; Baker, R.S.; Basso, N.; Bellanger, D.; Boza, C.; El Mourad, H.; France, M.; Gagner, M. International sleeve gastrectomy Expert Panel consensus statement: Best practice guidelines based on experience of >12,000 cases. Surg. Obes. Relat. Dis. 2012, 8, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Hughes, D.; Hughes, I.; Khanna, A. Management of Staple Line Leaks Following Sleeve Gastrectomy—A Systematic Review. Obes. Surg. 2019, 29, 2759–2772. [Google Scholar] [CrossRef] [PubMed]
- Lazzarin, G.; Di Furia, M.; Romano, L.; Di Sibio, A.; Di Giacomo, C.; Lombardi, L.; Giuliani, A.; Schietroma, M.; Pessia, B.; Carlei, F.; et al. Endoscopic double-pigtail catheter (EDPC) internal drainage as first-line treatment of gastric leak: A case eries during laparoscopic sleeve gastrectomy learning curve for morbid obesity. Minim. Invasive Surg. 2020, 2020, 8250904. [Google Scholar] [CrossRef] [PubMed]
- Galloro, G.; Ruggiero, S.; Russo, T.; Telesca, D.A.; Musella, M.; Milone, M.; Manta, R. Staple-line leak after sleeve gastrectomy in obese patients: A hot topic in bariatric surgery. World J. Gastrointest. Endosc. 2015, 7, 843–846. [Google Scholar] [PubMed]
- Spaander, M.C.; Baron, T.H.; Siersema, P.D.; Fuccio, L.; Schumacher, B.; Escorsell, À.; Garcia-Pagán, J.C.; Dumonceau, J.M.; Conio, M.; De Ceglie, A.; et al. Esophageal stenting for benign and malignant disease: European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline. Endoscopy 2016, 48, 939–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Azagury, D.; Eisenberg, D.; DeMaria, E.; Campos, G.M. ASMBS position statement on prevention, detection and treatment of gastrointestinal leak after gastric bypass and sleeve gastrectomy, including the roles of imaging, surgical exploration, and nonoperative management. Surg. Obes. Relat. Dis. 2015, 11, 739–748. [Google Scholar] [PubMed]
- Hamed, H.; Said, M.; Elghadban, H.; Elgeidie, A. Outcome and Adverse Events of Endoscopic Bariatric Stents for Management of Leakage after Bariatric Surgery. Obes. Surg. 2020, 30, 982–991. [Google Scholar] [PubMed]
- Liu, S.Y.; Wong, S.K.; Ng, E.K. Novel oesophago-gastro-duodenal stenting for gastric leaks after laparoscopic sleeve gastrectomy. Obes. Res. Clin. Pract. 2015, 9, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, V.T.; Huang, A.Y.; Tariq, N.; Dunkin, B.J. Endoscopic suture fixation of self-expanding metallic stents with and without submucosal injection. Surg. Endosc. 2015, 29, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Hamid, H.K.S.; Emile, S.H.; Saber, A.A.; Dincer, M.; de Moura, D.T.; Glissen, L.; Almadi, M.A.; Montuori, M.; Vix, M.; Perisse, L.G.S.; et al. Customized bariatric stents for sleeve gastrectomy leak: Are they superior to conventional esophageal stents? A systematic review and proportion meta-analysis. Surg. Endosc. 2021, 35, 1025–1038. [Google Scholar] [CrossRef] [PubMed]
- Casella, G.; Soricelli, E.; Rizzello, M.; Trentino, P.; Fiocca, F.; Fantini, A.; Salvatori, F.M.; Basso, N. Nonsurgical treatment of staple line leaks after laparoscopic sleeve gastrectomy. Obes. Surg. 2009, 19, 821–826. [Google Scholar] [CrossRef] [PubMed]
- Donatelli, G.; Dumont, J.L.; Cereatti, F.; Ferretti, S.; Vergeau, B.M.; Tuszynky, T.; Pourcher, G.; Tranchart, H.; Mariani, P.; Meduri, A.; et al. Treatment of leaks following sleeve gastrectomy by endoscopic internal drainage. Obes. Surg. 2015, 25, 1293–1301. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frattini, F.; Rizzi, A.; Segato, S.; Cortellezzi, C.C.; Rota Bacchetta, G.L.; Cassinotti, A.; Gianazza, S.; Conti, L.; Carrano, F.M.; Rausei, S. Esophageal Stent in Sleeve Gastrectomy Leak Treatment: Observations Based on a Challenging Surgical Case and Literature. Surgeries 2021, 2, 378-383. https://doi.org/10.3390/surgeries2040037
Frattini F, Rizzi A, Segato S, Cortellezzi CC, Rota Bacchetta GL, Cassinotti A, Gianazza S, Conti L, Carrano FM, Rausei S. Esophageal Stent in Sleeve Gastrectomy Leak Treatment: Observations Based on a Challenging Surgical Case and Literature. Surgeries. 2021; 2(4):378-383. https://doi.org/10.3390/surgeries2040037
Chicago/Turabian StyleFrattini, Francesco, Andrea Rizzi, Sergio Segato, Claudio Camillo Cortellezzi, Gian Luca Rota Bacchetta, Andrea Cassinotti, Simone Gianazza, Lorenzo Conti, Francesco Maria Carrano, and Stefano Rausei. 2021. "Esophageal Stent in Sleeve Gastrectomy Leak Treatment: Observations Based on a Challenging Surgical Case and Literature" Surgeries 2, no. 4: 378-383. https://doi.org/10.3390/surgeries2040037
APA StyleFrattini, F., Rizzi, A., Segato, S., Cortellezzi, C. C., Rota Bacchetta, G. L., Cassinotti, A., Gianazza, S., Conti, L., Carrano, F. M., & Rausei, S. (2021). Esophageal Stent in Sleeve Gastrectomy Leak Treatment: Observations Based on a Challenging Surgical Case and Literature. Surgeries, 2(4), 378-383. https://doi.org/10.3390/surgeries2040037