
Complex Vascular Reconstruction following Resection of a Large Retroperitoneal Teratoma

 and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
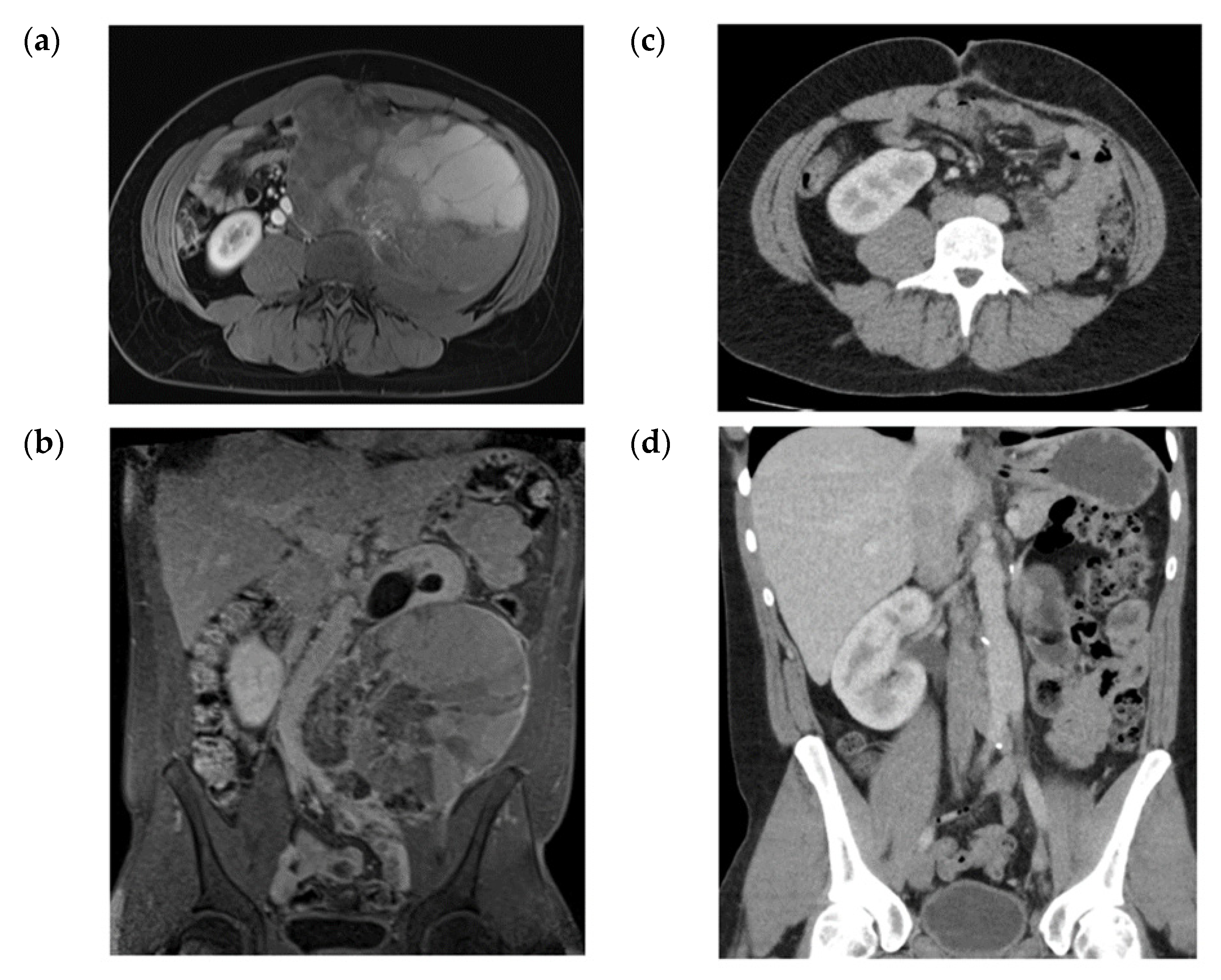
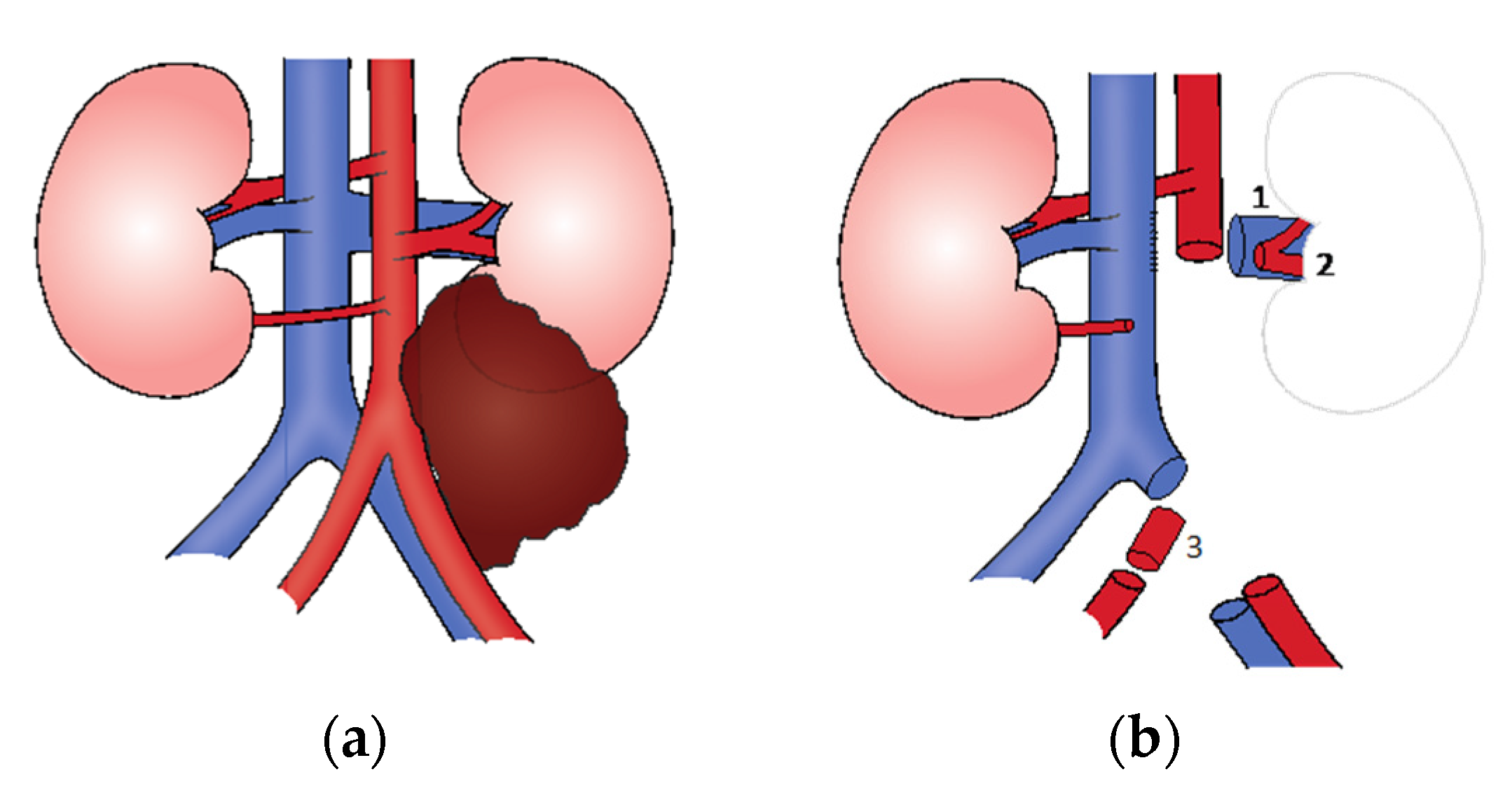
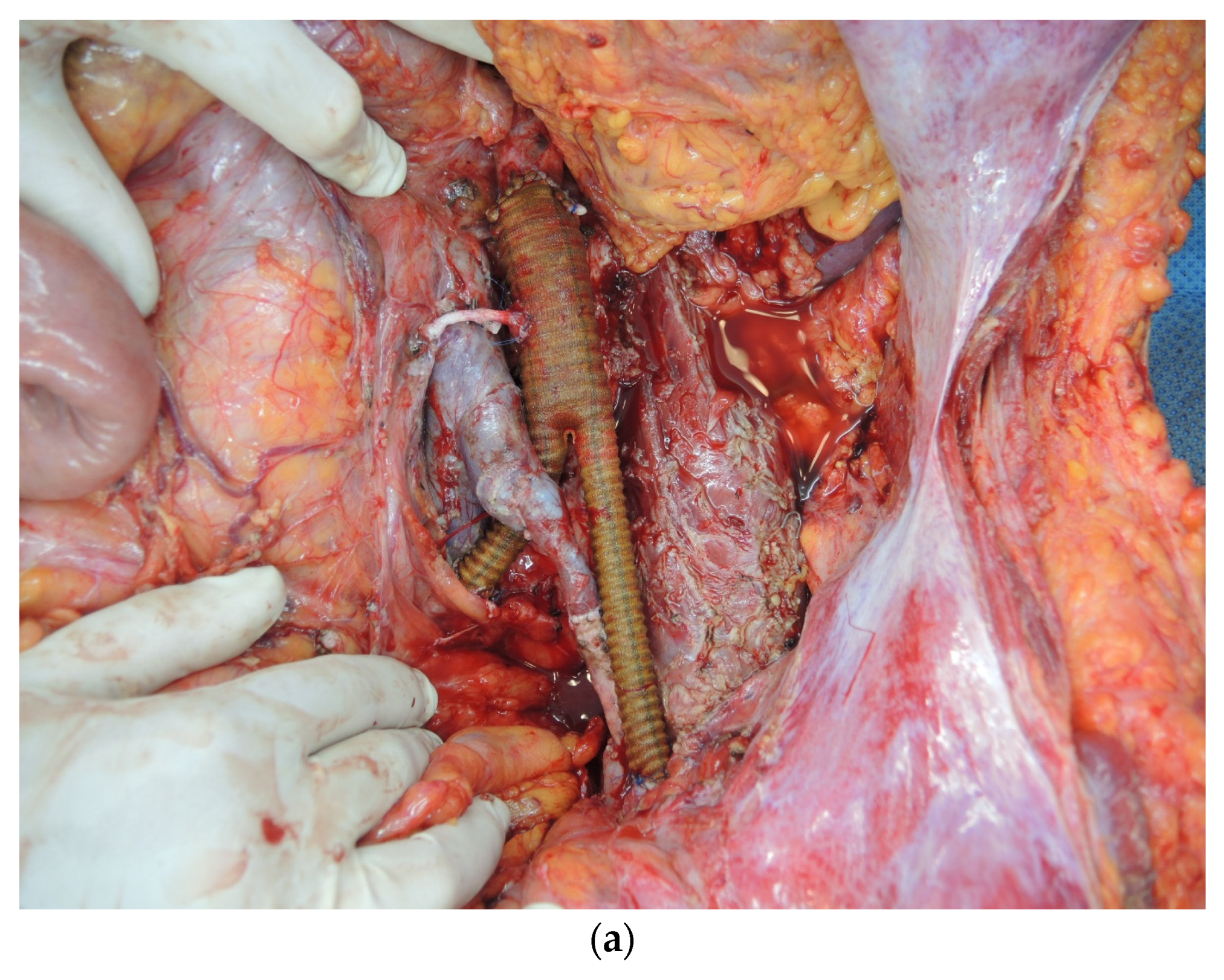
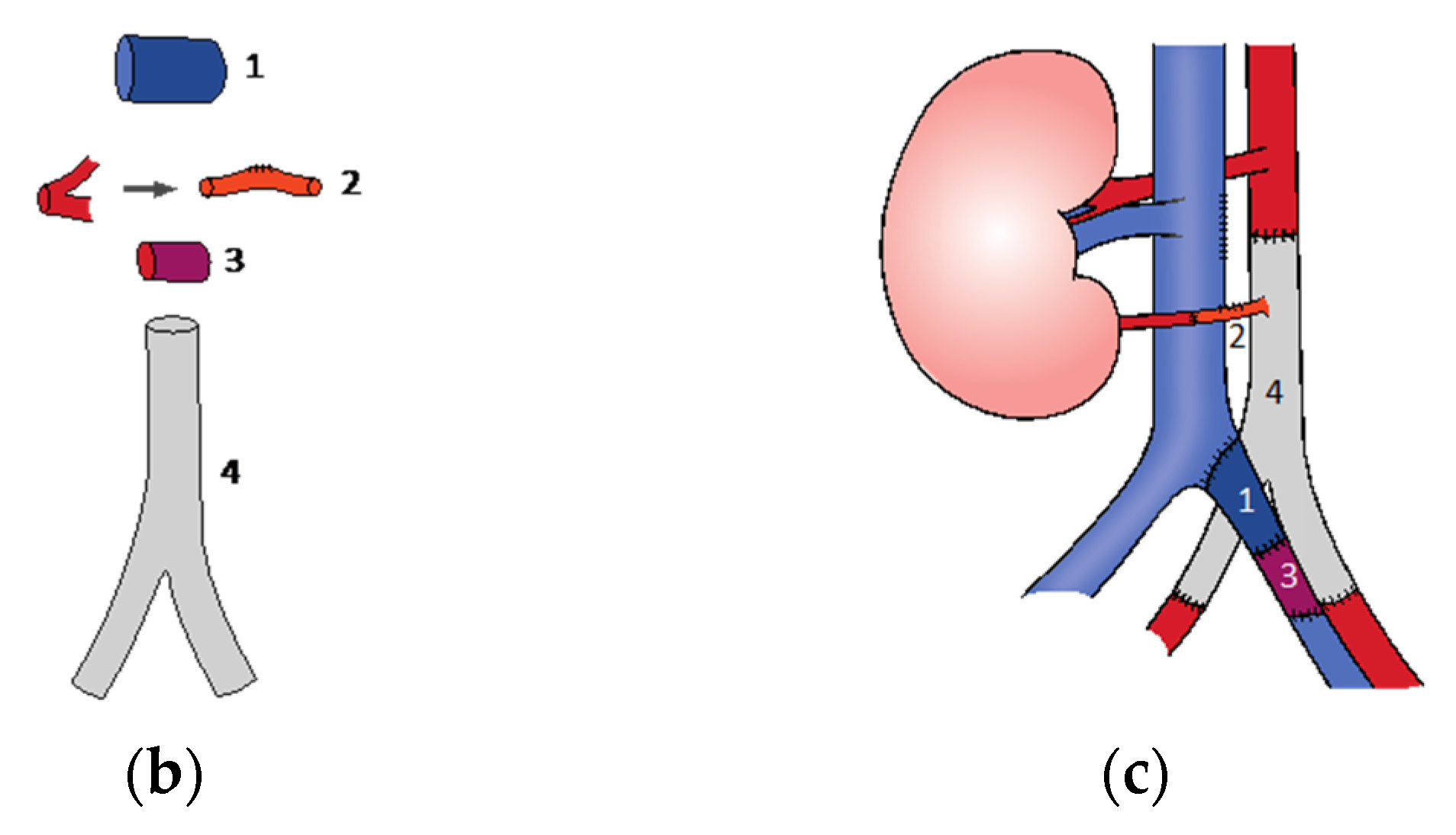
2. Case Description
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hayes-Lattin, B.; Nichols, C.R. Testicular cancer: A prototypic tumor of young adults. Semin. Oncol. 2009, 36, 432–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carver, B.S.; Sheinfeld, J. Germ cell tumors of the testis. Ann. Surg. Oncol. 2005, 12, 871–880. [Google Scholar] [CrossRef] [PubMed]
- McKiernan, J.M.; Goluboff, E.T.; Liberson, G.L.; Golden, R.; Fisch, H. Rising risk of testicular cancer by birth cohort in the United States from 1973 to 1995. J. Urol. 1999, 162, 361–363. [Google Scholar] [CrossRef]
- Purdue, M.P.; Devesa, S.S.; Sigurdson, A.J.; McGlynn, K.A. International patterns and trends in testis cancer incidence. Int. J. Cancer 2005, 115, 822–827. [Google Scholar] [CrossRef] [PubMed]
- Arora, R.S.; Alston, R.D.; Eden, T.O.; Geraci, M.; Birch, J.M. Comparative incidence patterns and trends of gonadal and extragonadal germ cell tumors in England, 1979 to 2003. Cancer 2012, 118, 4290–4297. [Google Scholar] [CrossRef] [PubMed]
- Carver, B.S.; Serio, A.M.; Bajorin, D.; Motzer, R.J.; Stasi, J.; Bosl, G.J.; Vickers, A.J.; Sheinfeld, J. Improved clinical outcome in recent years for men with metastatic nonseminomatous germ cell tumors. J. Clin. Oncol. 2007, 25, 5603–5608. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, T.; Bosl, G.J.; Hajdu, S.I. Teratoma with malignant transformation in germ cell tumors in men. Cancer 1985, 56, 860–863. [Google Scholar] [CrossRef]
- Comiter, C.V.; Kibel, A.S.; Richie, J.P.; Nucci, M.R.; Renshaw, A.A. Prognostic features of teratomas with malignant transformation: A clinicopathological study of 21 cases. J. Urol. 1998, 159, 859–863. [Google Scholar] [CrossRef]
- Motzer, R.J.; Amsterdam, A.; Prieto, V.; Sheinfeld, J.; Murty, V.V.; Mazumdar, M.; Bosl, G.J.; Chaganti, R.S.K.; Reuter, V.E. Teratoma with malignant transformation: Diverse malignant histologies arising in men with germ cell tumors. J. Urol. 1998, 159, 133–138. [Google Scholar] [CrossRef]
- Little, J.S., Jr.; Foster, R.S.; Ulbright, T.M.; Donohue, J.P. Unusual neoplasms detected in testis cancer patients undergoing post-chemotherapy retroperitoneal lymphadenectomy. J. Urol. 1994, 152, 1144–1149. [Google Scholar] [CrossRef]
- Rice, K.R.; Magers, M.J.; Beck, S.D.; Cary, K.C.; Einhorn, L.H.; Ulbright, T.M.; Foster, R.S. Management of germ cell tumors with somatic type malignancy: Pathological features, prognostic factors and survival outcomes. J. Urol. 2014, 192, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Wortmann, M.; Alldinger, I.; Bockler, D.; Ulrich, A.; Hyhlik-Durr, A. Vascular reconstruction after retroperitoneal and lower extremity sarcoma resection. Eur. J. Surg. Oncol. 2017, 43, 407–415. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stüben, B.-O.; Heumann, A.; Giannou, A.D.; Wipper, S.; Bannas, P.; Li, J. Complex Vascular Reconstruction following Resection of a Large Retroperitoneal Teratoma. Surgeries 2021, 2, 139-143. https://doi.org/10.3390/surgeries2020013
Stüben B-O, Heumann A, Giannou AD, Wipper S, Bannas P, Li J. Complex Vascular Reconstruction following Resection of a Large Retroperitoneal Teratoma. Surgeries. 2021; 2(2):139-143. https://doi.org/10.3390/surgeries2020013
Chicago/Turabian StyleStüben, Björn-Ole, Asmus Heumann, Anastasios D. Giannou, Sabine Wipper, Peter Bannas, and Jun Li. 2021. "Complex Vascular Reconstruction following Resection of a Large Retroperitoneal Teratoma" Surgeries 2, no. 2: 139-143. https://doi.org/10.3390/surgeries2020013
APA StyleStüben, B.-O., Heumann, A., Giannou, A. D., Wipper, S., Bannas, P., & Li, J. (2021). Complex Vascular Reconstruction following Resection of a Large Retroperitoneal Teratoma. Surgeries, 2(2), 139-143. https://doi.org/10.3390/surgeries2020013