Patient-Reported Expectations, Outcome and Satisfaction in Thoracic and Lumbar Spine Stabilization Surgery: A Prospective Study


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Study Population
3.2. Preoperative Symptom Burden
3.3. Postoperative Outcome for Pain and Disability
3.4. Patient Expectations
3.5. Patient Satisfaction
3.6. The Relation of Patient Factors and Outcome
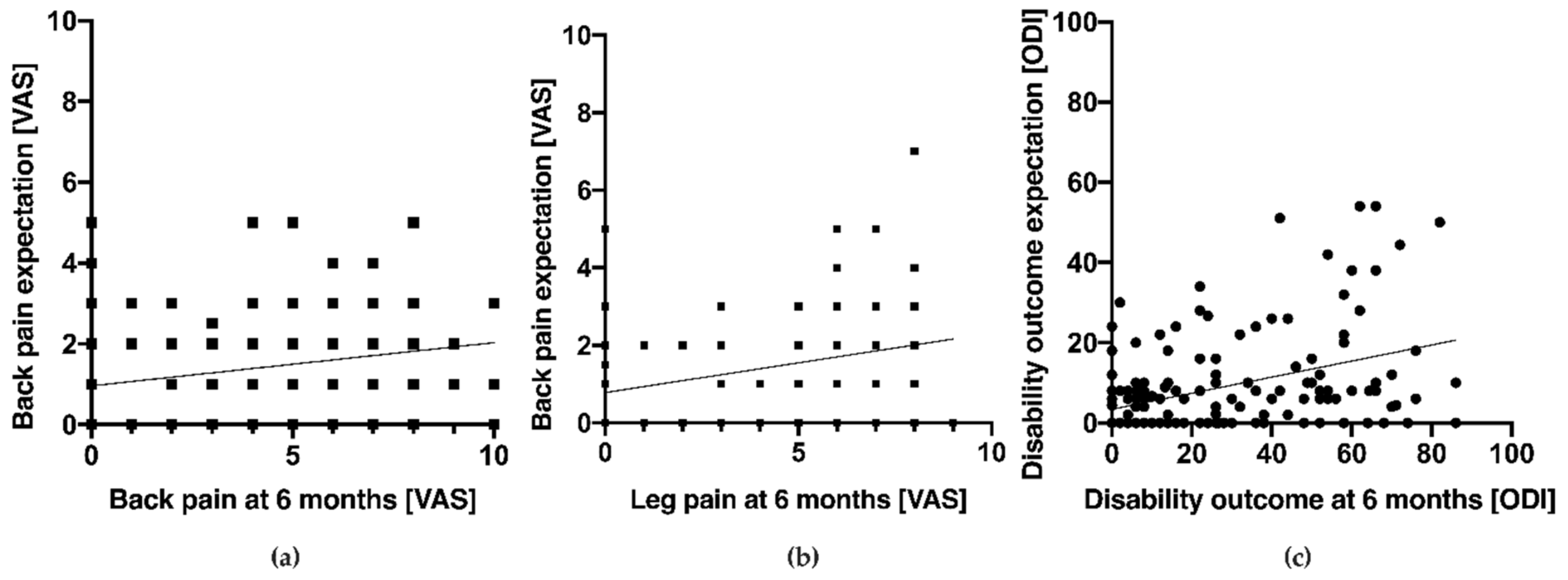
3.7. The Relation of Preoperative Status, Expectations, Pain and Disability Outcome and Satisfaction
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gentry, S.; Badrinath, P. Defining Health in the Era of Value-based Care: Lessons from England of Relevance to Other Health Systems. Cureus 2017, 9, e1079. [Google Scholar] [CrossRef]
- Menendez, J.Y.; Omar, N.B.; Chagoya, G.; Tabibian, B.E.; Elsayed, G.A.; Walters, B.C.; Guthrie, B.L.; Hadley, M.N. Patient Satisfaction in Spine Surgery: A Systematic Review of the Literature. Asian Spine J. 2019, 13, 1047–1057. [Google Scholar] [CrossRef] [PubMed]
- Oliver, R.L. Effect of Expectation and Disconfirmation on Postexposure Product Evaluations-an Alternative Interpretation. J. Appl. Psychol. 1977, 62, 480–486. [Google Scholar] [CrossRef]
- Oliver, R.L. A Cognitive Model of the Antecedents and Consequences of Satisfaction Decisions. J. Mark. Res. 1980, 17, 460–469. [Google Scholar] [CrossRef]
- Abbott, A.D.; Tyni-Lenne, R.; Hedlund, R. Leg pain and psychological variables predict outcome 2–3 years after lumbar fusion surgery. Eur. Spine J. 2011, 20, 1626–1634. [Google Scholar] [CrossRef]
- Carr, F.A.; Healy, K.M.; Villavicencio, A.T.; Nelson, E.L.; Mason, A.; Burneikiene, S.; Hernandez, T.D. Effect on clinical outcomes of patient pain expectancies and preoperative Mental Component Summary scores from the 36-Item Short Form Health Survey following anterior cervical discectomy and fusion. J. Neurosurg. Spine 2011, 15, 486–490. [Google Scholar] [CrossRef]
- Cobo Soriano, J.; Sendino Revuelta, M.; Fabregate Fuente, M.; Cimarra Diaz, I.; Martinez Urena, P.; Deglane Meneses, R. Predictors of outcome after decompressive lumbar surgery and instrumented posterolateral fusion. Eur. Spine J. 2010, 19, 1841–1848. [Google Scholar] [CrossRef]
- Culliton, S.E.; Bryant, D.M.; Overend, T.J.; MacDonald, S.J.; Chesworth, B.M. The relationship between expectations and satisfaction in patients undergoing primary total knee arthroplasty. J. Arthroplast. 2012, 27, 490–492. [Google Scholar] [CrossRef]
- De Groot, K.I.; Boeke, S.; Passchier, J. Preoperative expectations of pain and recovery in relation to postoperative disappointment in patients undergoing lumbar surgery. Med. Care 1999, 37, 149–156. [Google Scholar] [CrossRef]
- Den Boer, J.J.; Oostendorp, R.A.; Beems, T.; Munneke, M.; Evers, A.W. Continued disability and pain after lumbar disc surgery: The role of cognitive-behavioral factors. Pain 2006, 123, 45–52. [Google Scholar] [CrossRef]
- Gepstein, R.; Arinzon, Z.; Adunsky, A.; Folman, Y. Decompression surgery for lumbar spinal stenosis in the elderly: Preoperative expectations and postoperative satisfaction. Spinal Cord 2006, 44, 427–431. [Google Scholar] [CrossRef] [PubMed]
- Iversen, M.D.; Daltroy, L.H.; Fossel, A.H.; Katz, J.N. The prognostic importance of patient pre-operative expectations of surgery for lumbar spinal stenosis. Patient Educ. Couns. 1998, 34, 169–178. [Google Scholar] [CrossRef]
- Lutz, G.K.; Butzlaff, M.E.; Atlas, S.J.; Keller, R.B.; Singer, D.E.; Deyo, R.A. The relation between expectations and outcomes in surgery for sciatica. J. Gen. Intern. Med. 1999, 14, 740–744. [Google Scholar] [CrossRef] [PubMed]
- McGregor, A.H.; Dore, C.J.; Morris, T.P. An exploration of patients’ expectation of and satisfaction with surgical outcome. Eur. Spine J. 2013, 22, 2836–2844. [Google Scholar] [CrossRef] [PubMed]
- Ronnberg, K.; Lind, B.; Zoega, B.; Halldin, K.; Gellerstedt, M.; Brisby, H. Patients’ satisfaction with provided care/information and expectations on clinical outcome after lumbar disc herniation surgery. Spine (Phila Pa 1976) 2007, 32, 256–261. [Google Scholar] [CrossRef]
- Saban, K.L.; Penckofer, S.M. Patient expectations of quality of life following lumbar spinal surgery. J. Neurosci. Nurs. 2007, 39, 180–189. [Google Scholar] [CrossRef]
- Soroceanu, A.; Ching, A.; Abdu, W.; McGuire, K. Relationship between preoperative expectations, satisfaction, and functional outcomes in patients undergoing lumbar and cervical spine surgery: A multicenter study. Spine (Phila Pa 1976) 2012, 37, E103–E108. [Google Scholar] [CrossRef]
- Toyone, T.; Tanaka, T.; Kato, D.; Kaneyama, R.; Otsuka, M. Patients’ expectations and satisfaction in lumbar spine surgery. Spine (Phila Pa 1976) 2005, 30, 2689–2694. [Google Scholar] [CrossRef]
- Xiong, D.D.; Ye, W.; Xiao, R.; Miller, J.A.; Mroz, T.E.; Steinmetz, M.P.; Nagel, S.J.; Machado, A.G. Patient-reported allergies predict postoperative outcomes and psychosomatic markers after spine surgery. Spine J. 2019, 19, 121–130. [Google Scholar] [CrossRef]
- Yee, A.; Adjei, N.; Do, J.; Ford, M.; Finkelstein, J. Do patient expectations of spinal surgery relate to functional outcome? Clin. Orthop. Relat. Res. 2008, 466, 1154–1161. [Google Scholar] [CrossRef]
- Yoo, J.S.; Patel, D.V.; Mayo, B.C.; Massel, D.H.; Karmarkar, S.S.; Lamoutte, E.H.; Singh, K. Postoperative satisfaction following lumbar spinal fusion surgery: Patient expectation versus actuality. J. Neurosurg. Spine 2019, 31, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Porter, M.E.; Lee, T.H. The strategy that will fix health care. Harv. Bus. Rev. 2013, 91, 24. [Google Scholar]
- Porter, M.E. A Strategy for Health Care Reform—Toward a Value-Based System. N. Engl. J. Med. 2009, 361, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Porter, M.E.; Guth, C. Redefining German Health Care; Springer Press: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Porter, M.E. Measuring Health Outcomes: The Outcome Hierarchy. N. Engl. J. Med. 2010, 363, 2477–2481. [Google Scholar] [CrossRef]
- Stokes, O.M.; Cole, A.A.; Breakwell, L.M.; Lloyd, A.J.; Leonard, C.M.; Grevitt, M. Do we have the right PROMs for measuring outcomes in lumbar spinal surgery? Eur. Spine J. 2017, 26, 816–824. [Google Scholar] [CrossRef]
- Falavigna, A.; Dozza, D.C.; Teles, A.R.; Wong, C.C.; Barbagallo, G.; Brodke, D.; Al-Mutair, A.; Ghogawala, Z.; Riew, K.D. Current Status of Worldwide Use of Patient-Reported Outcome Measures (PROMs) in Spine Care. World Neurosurg. 2017, 108, 328–335. [Google Scholar] [CrossRef]
- Staartjes, V.E.; Siccoli, A.; De Wispelaere, M.P.; Schroder, M.L. Patient-reported outcomes unbiased by length of follow-up after lumbar degenerative spine surgery: Do we need 2 years of follow-up? Spine J. 2019, 19, 637–644. [Google Scholar] [CrossRef]
- Siccoli, A.; Staartjes, V.E.; De Wispelaere, M.P.; Schroder, M.L. Gender differences in degenerative spine surgery: Do female patients really fare worse? Eur. Spine J. 2018, 27, 2427–2435. [Google Scholar] [CrossRef]
- Triebel, J.; Snellman, G.; Sanden, B.; Stromqvist, F.; Robinson, Y. Women do not fare worse than men after lumbar fusion surgery: Two-year follow-up results from 4780 prospectively collected patients in the Swedish National Spine Register with lumbar degenerative disc disease and chronic low back pain. Spine J. 2017, 17, 656–662. [Google Scholar] [CrossRef]
- Sielatycki, J.A.; Chotai, S.; Stonko, D.; Wick, J.; Kay, H.; McGirt, M.J.; Devin, C.J. Is obesity associated with worse patient-reported outcomes following lumbar surgery for degenerative conditions? Eur. Spine J. 2016, 25, 1627–1633. [Google Scholar] [CrossRef]
- Gaetani, P.; Aimar, E.; Panella, L.; Debernardi, A.; Tancioni, F.; Rodriguez y Baena, R. Surgery for herniated lumbar disc disease: Factors influencing outcome measures. An analysis of 403 cases. Funct. Neurol. 2004, 19, 43–49. [Google Scholar] [PubMed]
- Asadi-Lari, M.; Tamburini, M.; Gray, D. Patients’ needs, satisfaction, and health related quality of life: Towards a comprehensive model. Health Qual. Life Outcomes 2004, 2, 32. [Google Scholar] [CrossRef] [PubMed]
- Urban-Baeza, A.; Zarate-Kalfopulos, B.; Romero-Vargas, S.; Obil-Chavarria, C.; Brenes-Rojas, L.; Reyes-Sanchez, A. Influence of depression symptoms on patient expectations and clinical outcomes in the surgical management of spinal stenosis. J. Neurosurg. Spine 2015, 22, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Sinikallio, S.; Aalto, T.; Airaksinen, O.; Herno, A.; Kroger, H.; Savolainen, S.; Turunen, V.; Viinamaki, H. Lumbar spinal stenosis patients are satisfied with short-term results of surgery-younger age, symptom severity, disability and depression decrease satisfaction. Disabil. Rehabil. 2007, 29, 537–544. [Google Scholar] [CrossRef]
- Schroeder, G.D.; Coric, D.; Kim, H.J.; Albert, T.J.; Radcliff, K.E. Are patient-reported outcomes predictive of patient satisfaction 5 years after anterior cervical spine surgery? Spine J. 2017, 17, 943–952. [Google Scholar] [CrossRef]
- Copay, A.G.; Martin, M.M.; Subach, B.R.; Carreon, L.Y.; Glassman, S.D.; Schuler, T.C.; Berven, S. Assessment of spine surgery outcomes: Inconsistency of change amongst outcome measurements. Spine J. 2010, 10, 291–296. [Google Scholar] [CrossRef]
- Chotai, S.; Sivaganesan, A.; Parker, S.L.; McGirt, M.J.; Devin, C.J. Patient-Specific Factors Associated With Dissatisfaction After Elective Surgery for Degenerative Spine Diseases. Neurosurgery 2015, 77, 157–163. [Google Scholar] [CrossRef]
- Rief, W.; Shedden-Mora, M.C.; Laferton, J.A.; Auer, C.; Petrie, K.J.; Salzmann, S.; Schedlowski, M.; Moosdorf, R. Preoperative optimization of patient expectations improves long-term outcome in heart surgery patients: Results of the randomized controlled PSY-HEART trial. BMC Med. 2017, 15, 4. [Google Scholar] [CrossRef]
- Schwarz, K.A.; Pfister, R.; Buchel, C. Rethinking Explicit Expectations: Connecting Placebos, Social Cognition, and Contextual Perception. Trends Cogn. Sci. 2016, 20, 469–480. [Google Scholar] [CrossRef]
- Den Ouden, H.; Vos, R.C.; Rutten, G. Effectiveness of shared goal setting and decision making to achieve treatment targets in type 2 diabetes patients: A cluster-randomized trial (OPTIMAL). Health Expect. 2017, 20, 1172–1180. [Google Scholar] [CrossRef]
- Wei, H.; Zhou, L.; Zhang, H.; Chen, J.; Lu, X.; Hu, L. The Influence of Expectation on Nondeceptive Placebo and Nocebo Effects. Pain Res. Manag. 2018, 2018, 8459429. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Dorsal Instrumentation Only | 360 Degree Fusion | |||
|---|---|---|---|---|
| Decompression | yes | no | yes | no |
| Pts. excluded | 26 | 7 | 43 | 5 |
| Pts. included (females) | 79 (36) | 16 (10) | 82 (43) | 22 (12) |
| Pts. w. f/u at disch./6/12/mo. | 79/64/54 | 13/13/9 | 79/64/59 | 21/21/17 |
| Females at disch./6/12/mo. | 36/30/27 | 9/9/6 | 41/35/31 | 11/11/9 |
| Age at day of inclusion | 67 ± 13 | 57 ± 19 | 66 ± 13 | 65 ± 11 |
| BMI at day of inclusion | 27 ± 5 | 26 ± 4 | 27 ± 5 | 28 ± 5 |
| Preop. | Expect. | Disch. | 6 Mo. | Exp. Fulf. | 12 Mo. | Exp. Fulf. | |
|---|---|---|---|---|---|---|---|
| Back pain (VAS) | |||||||
| All Patients | 6.7 ± 3.0 | 1.3 ± 1.5 | 4.8 ± 3.0 | 2.9 ± 2.9 | 48% | 2.6 ± 3.1 | 54% |
| Degenerative | 6.8 ± 2.7 | 1.6 ± 1.6 | 4.8 ± 3.2 | 3.3 ± 3.0 | 43% | 3.0 ± 3.2 | 50% |
| no revision | 6.9 ± 2.5 | 1.4 ± 1.4 | 4.9 ± 3.1 | 2.8 ± 2.8 | 46% | 2.6 ± 3.1 | 57% |
| revision stabilization | 6.8 ± 3.1 | 1.9 ± 1.9 | 4.5 ± 3.4 | 4.6 ± 3.3 | 35% | 3.9 ± 3.4 | 33% |
| Non-Degenerative | 6.4 ± 3.5 | 0.9 ± 1.2 | 4.8 ± 2.8 | 2.1 ± 2.7 | 56% | 1.8 ± 2.6 | 63% |
| Infection | 6.9 ± 3.3 | 1.2 ± 1.4 | 4.2 ± 2.8 | 1.4 ± 2.6 | 68% | 1.6 ± 2.7 | 71% |
| Tumor | 7.0 ± 3.5 | 0.9 ± 1.3 | 5.5 ± 2.9 | 2.8 ± 2.5 | 38% | 1.0 ± 1.8 | 73% |
| Trauma | 5.4 ± 3.7 | 0.4 ± 0.7 | 5.4 ± 1.6 | 4.0 ± 3.9 | 29% | 2.0 ± 2.3 | 43% |
| Osteoporosis | 4.8 ± 3.5 | 0.8 ± 0.9 | 4.2 ± 2.9 | 1.4 ± 1.9 | 69% | 2.8 ± 3.1 | 55% |
| Leg pain (VAS) | |||||||
| All Patients | 4.7 ± 3.7 | 1.6 ± 2.6 | 1.6 ± 2.6 | 1.5 ± 2.6 | 73% | 1.3 ± 2.5 | 77% |
| Degenerative | 5.9 ± 3.2 | 1.2 ± 1.4 | 2.2 ± 2.9 | 1.9 ± 2.9 | 66% | 1.7 ± 2.8 | 71% |
| no revision | 6.2 ± 3.1 | 1.1 ± 1.1 | 2.2 ± 2.9 | 1.8 ± 2.7 | 68% | 1.5 ± 2.7 | 75% |
| revision stabilization | 5.4 ± 3.6 | 1.4 ± 1.8 | 2.1 ± 2.9 | 4.6 ± 3.3 | 63% | 2.2 ± 3.1 | 62% |
| Non-Degenerative | 2.8 ± 3.4 | 0.7 ± 1.2 | 0.8 ± 1.9 | 0.7 ± 1.8 | 85% | 0.5 ± 1.5 | 89% |
| Infection | 2.9 ± 3.4 | 0.8 ± 1.0 | 0.6 ± 1.3 | 0.1 ± 0.4 | 95% | 0.8 ± 2.1 | 82% |
| Tumor | 2.9 ± 3.8 | 0.6 ± 1.4 | 0.5 ± 1.8 | 0.8 ± 1.9 | 85% | 0.2 ± 0.6 | 91% |
| Trauma | 1.0 ± 1.9 | 0.3 ± 0.5 | 1.1 ± 2.5 | 1.7 ± 2.9 | 71% | 0.7 ± 1.9 | 86% |
| Osteoporosis | 3.3 ± 3.4 | 0.9 ± 1.4 | 1.8 ± 2.7 | 1.2 ± 2.2 | 77% | 0.0 ± 0.0 | 100% |
| ODI | |||||||
| All Patients | 48 ± 22 | 9 ± 13 | - | 28 ± 25 | 28% | 24 ± 23 | 36% |
| Degenerative | 45 ± 20 | 10 ± 13 | - | 30 ± 25 | 22% | 27 ± 24 | 33% |
| no revision | 42 ± 20 | 6 ± 7 | - | 23 ± 23 | 27% | 21 ± 22 | 38% |
| revision stabilization | 53 ± 18 | 20 ± 19 | - | 46 ± 25 | 10% | 41 ± 26 | 19% |
| Non-Degenerative | 53 ± 25 | 9 ± 12 | - | 23 ± 23 | 40% | 19 ± 20 | 41% |
| Infection | 58 ± 25 | 12 ± 15 | - | 15 ± 18 | 50% | 12 ± 18 | 53% |
| Tumor | 49 ± 19 | 7 ± 8 | - | 36 ± 28 | 31% | 23 ± 22 | 27% |
| Trauma | 54 ± 39 | 1 ± 3 | - | 21 ± 26 | 29% | 19 ± 22 | 29% |
| Osteoporosis | 49 ± 25 | 11 ± 12 | - | 23 ± 23 | 38% | 25 ± 20 | 45% |
| Satisfaction Rate | |||||||
| All Patients | - | - | 82% | 70% | 78% | ||
| Degenerative | - | - | 79% | 65% | 75% | ||
| no revision | - | - | 82% | 74% | 84% | ||
| revision stabilization | - | - | 72% | 47% | 54% | ||
| Non-Degenerative | - | - | 86% | 78% | 85% | ||
| Infection | - | - | 93% | 92% | 89% | ||
| Tumor | - | - | 82% | 71% | 100% | ||
| Trauma | - | - | 88% | 57% | 71% | ||
| Osteoporosis | 77% | 69% | 75% |
| Sex | Smoker | BMI (kg/m2) | Prior Spinal Surgery | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Yes | No | <25 | 25 < 30 | 30 < 35 | ≥35 | Yes | No | |
| All patients | 22.1% | 37.6% | 39.3% | 28.4% | 23.6% | 35.7% | 30.3% | 33.3% | 42.2% | 22.4% |
| p = 0.04 | p = 0.26 | p = 0.58 | p < 0.01 | |||||||
| Degenerative | 25.0% | 42.9% | 40.9 | 32.9 | 24.1% | 40.1% | 36.0% | 27.3% | 44.4% | 24.0% |
| p = 0.06 | p = 0.49 | p = 0.53 | p = 0.03 | |||||||
| Deg. no rev. | 18.8% | 32.5% | 18.2% | 27.9% | 14.3% | 26.2% | 35.3% | 28.6% | 31.8% | 24.0% |
| p = 0.19 | p = 0.50 | p = 0.51 | p = 0.49 | |||||||
| Deg. revision | 37.5% | 68.8% | 63.6% | 47.6% | 50.0% | 72.7% | 37.5% | 25.0% | - | - |
| p = 0.08 | p = 0.39 | p = 0.29 | - | |||||||
| Non-deg. | 17.2% | 27.6% | 21.2% | 33.3% | 24.0% | 26.3% | 0.0% | 50.0% | 30.0% | 20.8% |
| p = 0.35 | p = 0.49 | p = 0.29 | p = 0.53 | |||||||
| Preoperative | Expectations | 6 Months | |||||||
|---|---|---|---|---|---|---|---|---|---|
| All Patients | Sat. | Non-Sat. | p | Sat. | Non-Sat. | p | Sat. | Non-Sat. | p |
| Back pain [VAS] | 6.5 ± 3.1 | 6.5 ± 2.9 | 0.94 | 1.1 ± 1.3 | 1.7 ± 1.6 | 0.02 | 2.0 ± 2.5 (58%) | 5.0 ± 2.9 (22%) | <0.001 (<0.001) |
| Leg pain [VAS] | 4.5 ± 3.8 | 5.0 ± 3.5 | 0.40 | 0.9 ± 1.4 | 1.2 ± 1.5 | 0.17 | 0.9 ± 2.0 (80%) | 2.7 ± 3.3 (57%) | <0.001 (<0.01) |
| Disability [ODI] | 45 ± 23 | 50 ± 22 | 0.23 | 9 ± 13 | 10 ± 12 | 0.17 | 18 ± 20 (39%) | 50 ± 22 (2%) | <0.001 (<0.001) |
| Degenerative | |||||||||
| Back pain [VAS] | 6.7 ± 2.9 | 6.9 ± 2.7 | 0.77 | 1.3 ± 1.5 | 1.9 ± 1.7 | 0.04 | 2.3 ± 2.6 (54%) | 5.5 ± 2.7 (21%) | <0.001 (<0.01) |
| Leg pain [VAS] | 6.0 ± 3.4 | 5.7 ± 3.3 | 0.63 | 1.1 ± 1.4 | 1.3 ± 1.5 | 0.59 | 1.4 ± 2.4 (72%) | 2.9 ± 3.4 (57%) | 0.03 (0.14) |
| Disability [ODI] | 42 ± 21 | 50 ± 18 | 0.04 | 9 ± 14 | 10 ± 12 | 0.26 | 18.2 ± 19.8 (33%) | 52.7 ± 18.6 (0%) | <0.001 (<0.001) |
| Deg. No Revision | |||||||||
| Back pain [VAS] | 6.7 ± 2.7 | 6.8 ± 2.6 | 0.94 | 1.2 ± 1.4 | 1.7 ± 1.4 | 0.18 | 2.1 ± 2.4 (54%) | 4.8 ± 2.8 (22%) | <0.001 (0.02) |
| Leg pain [VAS] | 5.9 ± 3.4 | 6.6 ± 2.7 | 0.43 | 0.9 ± 1.1 | 1.5 ± 1.5 | 0.12 | 1.2 ± 2.0 (73%) | 3.2 ± 3.6 (56%) | 0.03 (0.17) |
| Disability [ODI] | 39 ± 21 | 48 ± 19 | 0.09 | 6 ± 7 | 4 ± 4 | 0.95 | 13.3 ± 14.1 (37%) | 49.4 ± 19.8 (0%) | <0.001 (<0.01) |
| Deg. Revision | |||||||||
| Back pain [VAS] | 6.5 ± 3.6 | 6.9 ± 2.8 | 0.72 | 1.7 ± 1.9 | 2.3 ± 2.0 | .043 | 2.7 ± 3.2 (53%) | 6.3 ± 2.4 (19%) | <0.01 (0.04) |
| Leg pain [VAS] | 6.2 ± 3.7 | 4.6 ± 3.6 | 0.22 | 1.9 ± 2.0 | 1.0 ± 1.5 | 0.18 | 2.2 ± 3.3 (67%) | 2.5 ± 3.4 (59%) | 0.78 (0.65) |
| Disability [ODI] | 53 ± 19 | 52 ± 17 | 0.88 | 23 ± 23 | 16 ± 14 | 0.66 | 34.8 ± 26.9 (20%) | 56.5 ± 17.1 (0%) | 0.02 (0.06) |
| Non-Deg. | |||||||||
| Back pain [VAS] | 6.3 ± 3.5 | 5.5 ± 3.5 | 0.47 | 0.8 ± 1.0 | 0.9 ± 0.9 | 0.61 | 1.6 ± 2.5 (65%) | 3.6 ± 3.1 (25%) | 0.03 (0.01) |
| Leg pain [VAS] | 2.2 ± 3.1 | 3.3 ± 3.4 | 0.31 | 0.6 ± 1.2 | 1.2 ± 1.4 | 0.16 | 0.3 ± 1.0 (93%) | 2.3 ± 2.9 (58%) | 0.04 (<0.01) |
| Disability [ODI] | 50 ± 25 | 49 ± 31 | 0.89 | 7 ± 11 | 10 ± 12 | 0.49 | 17.9 ± 19.9 (49%) | 40.5 ± 27.1 (8%) | <0.01 (0.01) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krauss, P.; Sonnleitner, C.; Reinartz, F.; Meyer, B.; Meyer, H.S. Patient-Reported Expectations, Outcome and Satisfaction in Thoracic and Lumbar Spine Stabilization Surgery: A Prospective Study. Surgeries 2020, 1, 63-76. https://doi.org/10.3390/surgeries1020008
Krauss P, Sonnleitner C, Reinartz F, Meyer B, Meyer HS. Patient-Reported Expectations, Outcome and Satisfaction in Thoracic and Lumbar Spine Stabilization Surgery: A Prospective Study. Surgeries. 2020; 1(2):63-76. https://doi.org/10.3390/surgeries1020008
Chicago/Turabian StyleKrauss, Philipp, Clara Sonnleitner, Feline Reinartz, Bernhard Meyer, and Hanno S. Meyer. 2020. "Patient-Reported Expectations, Outcome and Satisfaction in Thoracic and Lumbar Spine Stabilization Surgery: A Prospective Study" Surgeries 1, no. 2: 63-76. https://doi.org/10.3390/surgeries1020008
APA StyleKrauss, P., Sonnleitner, C., Reinartz, F., Meyer, B., & Meyer, H. S. (2020). Patient-Reported Expectations, Outcome and Satisfaction in Thoracic and Lumbar Spine Stabilization Surgery: A Prospective Study. Surgeries, 1(2), 63-76. https://doi.org/10.3390/surgeries1020008