
Studying Satisfaction with the Restriction Measures Implemented in Greece during the First COVID-19 Pandemic Wave

Abstract
:1. Introduction
2. Material and Methods
3. Results
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lam, M.E. United by the Global COVID-19 Pandemic: Divided by Our Values and Viral Identities. Humanit. Soc. Sci. Commun. 2021, 8, 31. [Google Scholar] [CrossRef]
- Capano, G.; Howlett, M.; Jarvis, D.S.L.; Ramesh, M.; Goyal, N. Mobilizing Policy (In)Capacity to Fight COVID-19: Understanding Variations in State Responses. Policy Soc. 2020, 39, 285–308. [Google Scholar] [CrossRef]
- Sabat, I.; Neuman-Böhme, S.; Varghese, N.E.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. United but Divided: Policy Responses and People’s Perceptions in the EU during the COVID-19 Outbreak. Health Policy 2020, 124, 909–918. [Google Scholar] [CrossRef] [PubMed]
- Cristea, I.A.; Naudet, F.; Ioannidis, J.P.A. Preserving Equipoise and Performing Randomised Trials for COVID-19 Social Distancing Interventions. Epidemiol. Psychiatr. Sci. 2020, 29, e184. [Google Scholar] [CrossRef] [PubMed]
- Glover, A.; Heathcote, J.; Krueger, D.; Ríos-Rull, J.-V. Health versus Wealth: On the Distributional Effects of Controlling a Pandemic. Natl. Bur. Econ. Res. 2020. Available online: http://www.nber.org/papers/w27046 (accessed on 7 April 2021).
- Ashkenazi, I.; Rapaport, C. Saving Lives Versus Saving Dollars: The Acceptable Loss for Coronavirus Disease 2019*. Crit. Care Med. 2020, 48, 1243–1244. [Google Scholar] [CrossRef]
- Chaudhary, M.; Sodani, P.R.; Das, S. Effect of COVID-19 on Economy in India: Some Reflections for Policy and Programme. J. Health Manag. 2020, 22, 169–180. [Google Scholar] [CrossRef]
- Douglas, M.; Katikireddi, S.V.; Taulbut, M.; McKee, M.; McCartney, G. Mitigating the Wider Health Effects of Covid-19 Pandemic Response. BMJ 2020, 369, m1557. [Google Scholar] [CrossRef]
- Lytras, T.; Tsiodras, S. Lockdowns and the COVID-19 Pandemic: What Is the Endgame? Scand. J. Public Health 2021, 49, 37–40. [Google Scholar] [CrossRef]
- Appleby, J. Tackling COVID-19: Are the Costs Worth the Benefits? BMJ 2020, 369, m1496. [Google Scholar] [CrossRef] [Green Version]
- Viscusi, W.K. Pricing the Global Health Risks of the COVID-19 Pandemic. J. Risk Uncertain. 2020, 61, 101–128. [Google Scholar] [CrossRef] [PubMed]
- Joffe, A.R. COVID-19: Rethinking the Lockdown Groupthink. Front. Public Health 2021, 9, 625778. [Google Scholar] [CrossRef] [PubMed]
- Altig, D.; Baker, S.; Barrero, J.M.; Bloom, N.; Bunn, P.; Chen, S.; Davis, S.J.; Leather, J.; Meyer, B.; Mihaylov, E.; et al. Economic uncertainty before and during the COVID-19 pandemic. J. Public Econ. 2020, 191, 104274. [Google Scholar] [CrossRef] [PubMed]
- Santos-Pinto, L.; Mata, J. Strategies for COVID-19: The Option Value of Waiting. VoxEU CERP, 2020. Available online: https://voxeu.org (accessed on 24 January 2021).
- Sun, N. Applying Siracusa: A Call for a General Comment on Public Health Emergencies. Health Hum. Rights J. 2020, 22, 387–390. [Google Scholar]
- Hansel, T.C.; Saltzman, L.Y.; Bordnick, P.S. Behavioral Health and Response for COVID-19. Disaster Med. Public Health Prep. 2020, 14, 670–676. [Google Scholar] [CrossRef]
- Godinic, D.; Obrenovic, B.; Khudaykulov, A. Effects of Economic Uncertainty on Mental Health in the COVID-19 Pandemic Context: Social Identity Disturbance, Job Uncertainty and Psychological Well-Being Model. Int. J. Innov. Econ. Dev. 2020, 6, 61–74. [Google Scholar] [CrossRef]
- Aquino, E.M.L.; Silveira, I.H.; Pescarini, J.M.; Aquino, R.; de Souza-Filho, J.A.; dos Santos Rocha, A.; Ferreira, A.; Victor, A.; Teixeira, C.; Machado, D.B.; et al. Medidas de Distanciamento Social No Controle Da Pandemia de COVID-19: Potenciais Impactos e Desafios No Brasil. Ciênc. Saúde Coletiva 2020, 25, 2423–2446. [Google Scholar] [CrossRef]
- Baker, S.R.; Bloom, N.; Davis, S.J.; Terry, S.J. COVID-Induced Economic Uncertainty. Natl. Bur. Econ. Res. 2020. Available online: http://www.nber.org/papers/w26983 (accessed on 12 September 2020).
- Glowacz, F.; Schmits, E. Psychological Distress during the COVID-19 Lockdown: The Young Adults Most at Risk. Psychiatry Res. 2020, 293, 113486. [Google Scholar] [CrossRef]
- Boone, L. Tackling the Fallout from COVID-19. In Economics in the Time of COVID-19; Baldwin, R.E., di Mauro, B.W., Eds.; Centre for Economic Policy Research: London, UK, 2020; pp. 37–44. ISBN 978-1-912179-28-2. [Google Scholar]
- Chen, C.W.S.; Lee, S.; Dong, M.C.; Taniguchi, M. What Factors Drive the Satisfaction of Citizens with Governments’ Responses to COVID-19? Int. J. Infect. Dis. 2021, 102, 327–331. [Google Scholar] [CrossRef]
- Wu, C.; Shi, Z.; Wilkes, R.; Wu, J.; Gong, Z.; He, N.; Xiao, Z.; Zhang, X.; Lai, W.; Zhou, D.; et al. Chinese Citizen Satisfaction with Government Performance during COVID-19. J. Contemp. China 2021, 1–15. [Google Scholar] [CrossRef]
- Martín, J.C.; Román, C. COVID-19 Is Examining the EU and the Member States: The Role of Attitudes and Sociodemographic Factors on Citizens’ Support towards National Policies. Soc. Sci. 2021, 10, 46. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2020. Available online: https://covid19.who.int/ (accessed on 6 June 2021).
- Moris, D.; Schizas, D. Lockdown during COVID-19: The Greek Success. In Vivo 2020, 34, 1695–1699. [Google Scholar] [CrossRef] [PubMed]
- National Public Health Organization. Current State of Covid-19 Outbreak in Greece and Timeline of Key Containment Events. 2020. Available online: https://eody.gov.gr/en/current-state-of-covid-19-outbreak-in-greece-and-timeline-of-key-containmentevents/ (accessed on 19 April 2021).
- Bamias, G.; Lagou, S.; Gizis, M.; Karampekos, G.; Kyriakoulis, K.G.; Pontas, C.; Mantzaris, G.J. The Greek Response to COVID-19: A True Success Story from an IBD Perspective. Inflamm. Bowel Dis. 2020, 26, 1144–1148. [Google Scholar] [CrossRef]
- Petrakis, P.E.; Kostis, P.C. The Requirements for a Pro-growth Long-Term View. In The Evolution of the Greek Economy.; Springer International Publishing: Cham, Switzerland, 2020; pp. 233–256. ISBN 978-3-030-47209-2. [Google Scholar]
- European Parliament. Public Opinion in the EU in Time of Coronavirus Crisis. 2020. Available online: https://www.europarl.europa.eu/at-your-service/en/be-heard/eurobarometer/public-opinion-in-the-eu-in-time-of-coronavirus-crisis (accessed on 18 September 2020).
- Lipsitz, S.R.; Fitzmaurice, G.M.; Molenberghs, G. Goodness-of-Fit Tests for Ordinal Response Regression Models. Appl. Stat. 1996, 45, 175. [Google Scholar] [CrossRef]
- Tastle, W.J.; Wierman, M.J. Consensus and Dissention: A Measure of Ordinal Dispersion. Int. J. Approx. Reason. 2007, 45, 531–545. [Google Scholar] [CrossRef] [Green Version]
- Hendrickx, J. Using Categorical Variables in Stata. Stata Tech. Bull. 1999, STB-52, 2–8. [Google Scholar]
- Fagerland, M.W. Adjcatlogit, ccrlogit, and ucrlogit: Fitting Ordinal Logistic Regression Models. Stata J. 2014, 14, 947–964. [Google Scholar] [CrossRef] [Green Version]
- Fagerland, M.W.; Hosmer, D.W. How to Test for Goodness of Fit in Ordinal Logistic Regression Models. Stata J. 2017, 17, 668–686. [Google Scholar] [CrossRef]
- Openshaw, M. CNS: Stata Module to Compute Consensus Measure for Ordinal Scales. 2010. Available online: https://ideas.repec.org/c/boc/bocode/s457130.html (accessed on 15 May 2021).
- Organization for Economic Co-operation and Development. Policy Responses to the COVID-19 Crisis. 2020. Available online: http://www.oecd.org/social/Covid-19-Employment-and-Social-Policy-Responses-by-Country.xlsx (accessed on 19 April 2021).
- National Public Health Organization. Daily Reports on COVID-19. 2020. Available online: https://eody.gov.gr/ (accessed on 15 December 2020). (In Greek)
- Fragkaki, I.; Maciejewski, D.F.; Weijman, E.L.; Feltes, J.; Cima, M. Human Responses to Covid-19: The Role of Optimism Bias, Perceived Severity, and Anxiety. Personal. Individ. Differ. 2021, 176, 110781. [Google Scholar] [CrossRef]
- Fouda, A.; Mahmoudi, N.; Moy, N.; Paolucci, F. The COVID-19 Pandemic in Greece, Iceland, New Zealand, and Singapore: Health Policies and Lessons Learned. Health Policy Technol. 2020, 9, 510–524. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, R.; Zhao, J.; Molina, M.J. Understanding Transmission and Intervention for the COVID-19 Pandemic in the United States. Sci. Total Environ. 2020, 748, 141560. [Google Scholar] [CrossRef] [PubMed]
- Njindan Iyke, B. Economic Policy Uncertainty in Times of COVID-19 Pandemic. Asian Econ. Lett. 2020. [Google Scholar] [CrossRef]
- Manski, C.F. Forming COVID-19 Policy Under Uncertainty. J. Benefit Cost Anal. 2020, 11, 341–356. [Google Scholar] [CrossRef]
- Chang, S.L.; Harding, N.; Zachreson, C.; Cliff, O.M.; Prokopenko, M. Modelling Transmission and Control of the COVID-19 Pandemic in Australia. Nat. Commun. 2020, 11, 5710. [Google Scholar] [CrossRef] [PubMed]
- Gapen, M.; Millar, J.; Blerina, U.; Sriram, P. Assessing the Effectiveness of Alternative Measures to Slow the Spread of COVID-19 in the United States; Covid Economics, Centre for Economic Policy Research Press: London, UK, 2020; pp. 46–75. Available online: https://cepr.org/content/covid-economics-vetted-and-real-time-papers-0 (accessed on 16 May 2021).
- Alfano, V.; Ercolano, S. The Efficacy of Lockdown Against COVID-19: A Cross-Country Panel Analysis. Appl. Health Econ. Health Policy 2020, 18, 509–517. [Google Scholar] [CrossRef]
- Zhou, Y.; Xu, R.; Hu, D.; Yue, Y.; Li, Q.; Xia, J. Effects of Human Mobility Restrictions on the Spread of COVID-19 in Shenzhen, China: A Modelling Study Using Mobile Phone Data. Lancet Digit. Health 2020, 2, e417–e424. [Google Scholar] [CrossRef]
- Susskind, D.; Vines, D. The Economics of the COVID-19 Pandemic: An Assessment. Oxf. Rev. Econ. Policy 2020, 36, S1–S13. [Google Scholar] [CrossRef]
- Gössling, S.; Scott, D.; Hall, C.M. Pandemics, Tourism and Global Change: A Rapid Assessment of COVID-19. J. Sustain. Tour. 2021, 29, 1–20. [Google Scholar] [CrossRef]
- Vasileiou, E.; Samitas, A.; Karagiannaki, M.; Dandu, J. Health Risk and the Efficient Market Hypothesis in the Time of COVID-19. Int. Rev. Appl. Econ. 2021, 35, 210–223. [Google Scholar] [CrossRef]
- Abel, T.; McQueen, D. Critical health literacy and the COVID-19 crisis. Health Promot. Int. 2020, 35, 1612–1613. [Google Scholar] [CrossRef] [PubMed]
- Siegrist, M.; Luchsinger, L.; Bearth, A. The Impact of Trust and Risk Perception on the Acceptance of Measures to Reduce COVID-19 Cases. Risk Anal. 2021, 41, 787–800. [Google Scholar] [CrossRef]
- Drosos, D.; Skordoulis, M.; Tsotsolas, N.; Kyriakopoulos, G.L.; Gkika, E.C.; Komisopoulos, F. Retail Customers’ Satisfaction with Banks in Greece: A Multicriteria Analysis of a Dataset. Data Brief. 2021, 35, 106915. [Google Scholar] [CrossRef]
- Petrakis, P.E. The Greek Economy in the World. In The New Political Economy of Greece up to 2030; The Political Economy of Greek Growth up to 2030; Springer International Publishing: Cham, Switzerland, 2020; pp. 95–112. ISBN 978-3-030-47074-6. [Google Scholar]
- Hazakis, K.J. Is There a Way out of the Crisis? Macroeconomic Challenges for Greece after the Covid-19 Pandemic. Eur. Politics Soc. 2021, 1–15. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Rapid Risk Assessment. Increased Transmission of COVID-19 in the EU/EEA and the UK-Twelfth Update 2020. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/covid-19-risk-assessment-increased-transmission-12th-update-september-2020.pdf (accessed on 24 May 2021).
- Ashraf, B.N. Economic Impact of Government Interventions during the COVID-19 Pandemic: International Evidence from Financial Markets. J. Behav. Exp. Financ. 2020, 27, 100371. [Google Scholar] [CrossRef] [PubMed]
- Papanikos, G.T. The Impact of the Covid-19 Pandemic on Greek Tourism. AJT 2020, 7, 87–100. [Google Scholar] [CrossRef]
- Politis, I.; Georgiadis, G.; Nikolaidou, A.; Kopsacheilis, A.; Fyrogenis, I.; Sdoukopoulos, A.; Verani, E.; Papadopoulos, E. Mapping Travel Behavior Changes during the COVID-19 Lock-down: A Socioeconomic Analysis in Greece. Eur. Transp. Res. Rev. 2021, 13, 21. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Gender % (n) | |
|---|---|---|
| Male | Female | |
| 16–24 | 8.57 (90) | 8.48 (89) |
| 25–34 | 11.05 (116) | 11.24 (118) |
| 35–44 | 14.95 (157) | 14.95 (157) |
| 45–54 | 15.43 (162) | 15.33 (161) |
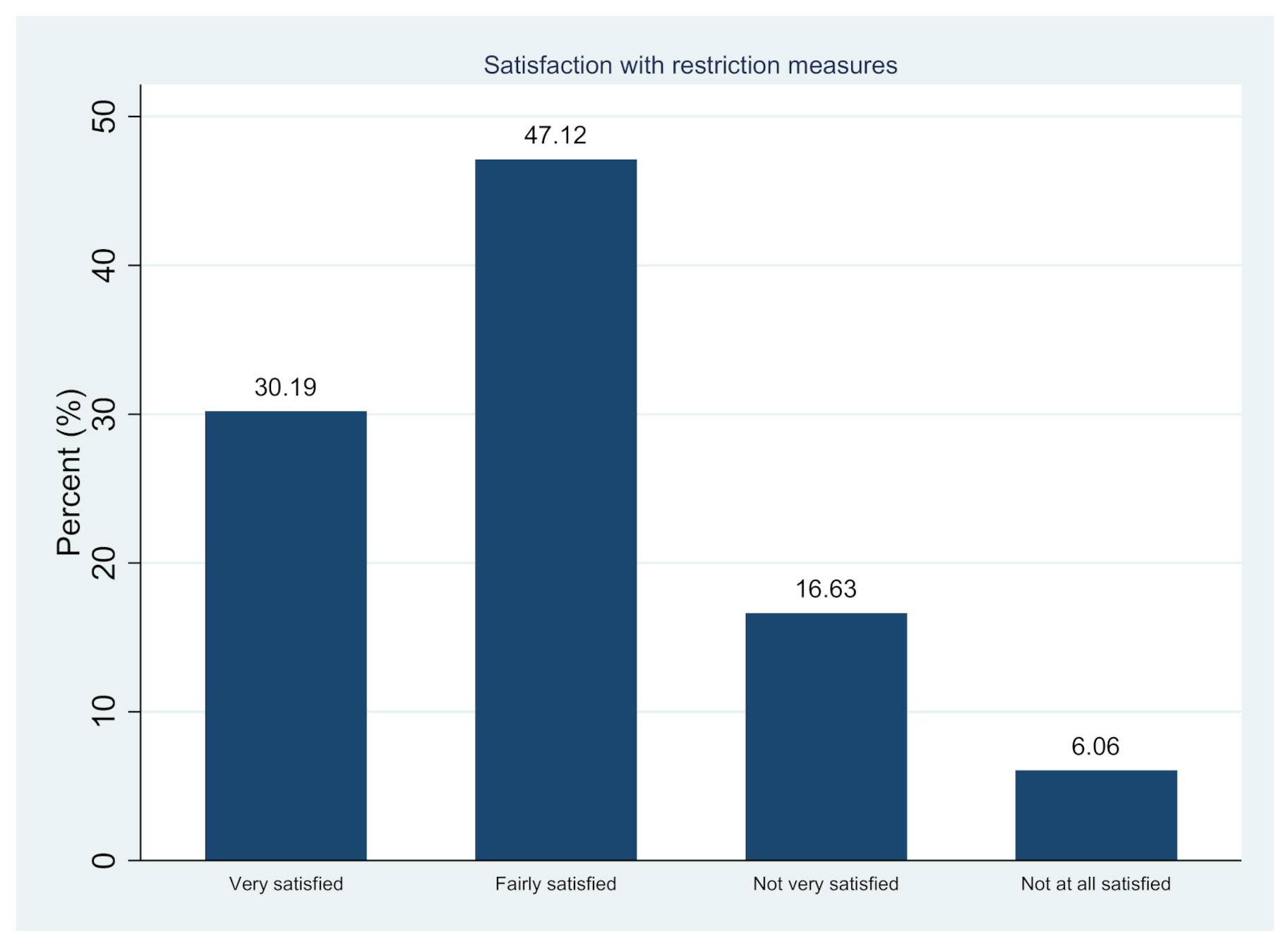
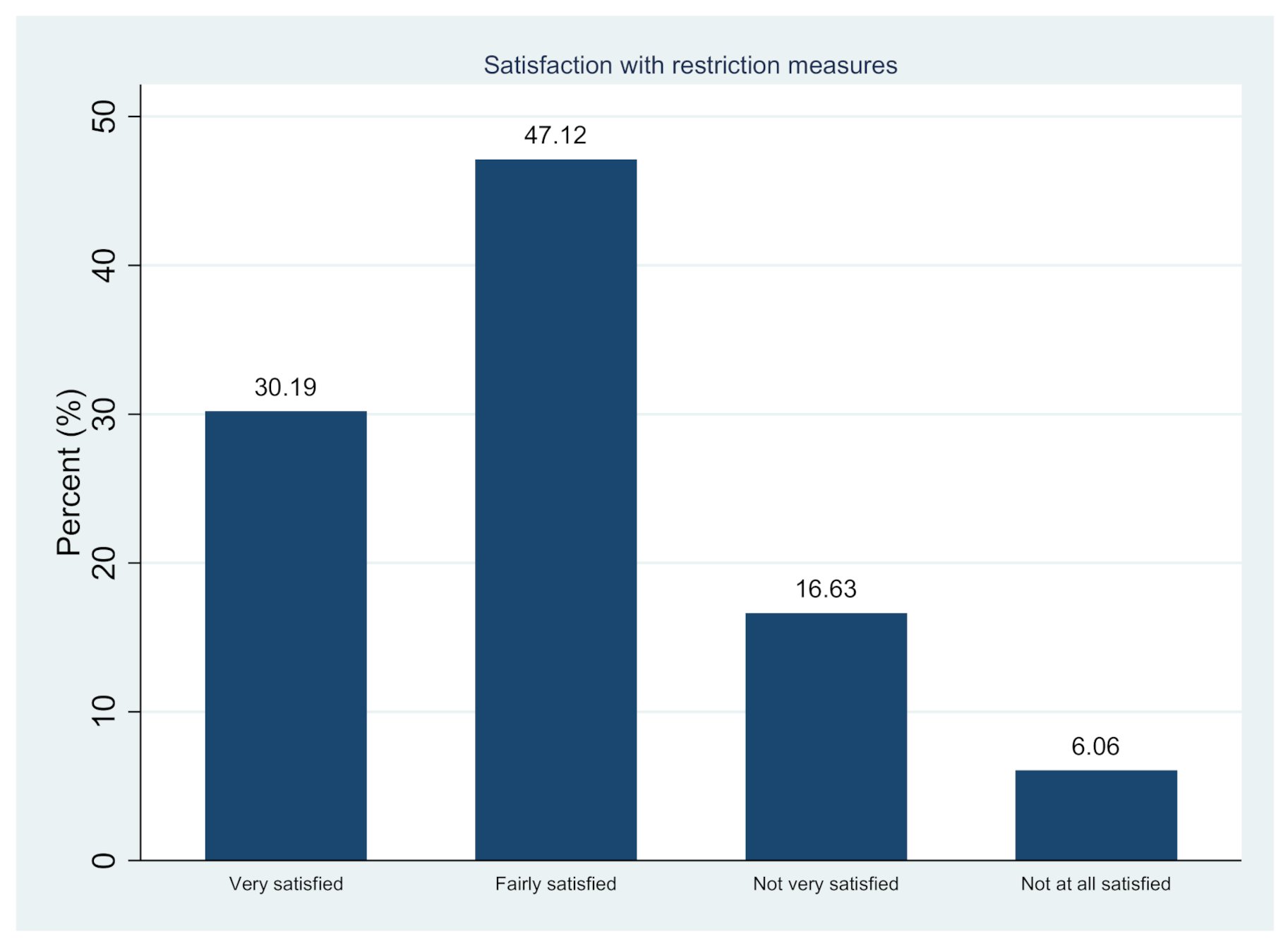
| Category | % (n) |
|---|---|
| Very satisfied | 30.19 (314) |
| Fairly satisfied | 47.12 (490) |
| Not very satisfied | 16.63 (173) |
| Not at all satisfied | 6.06 (63) |
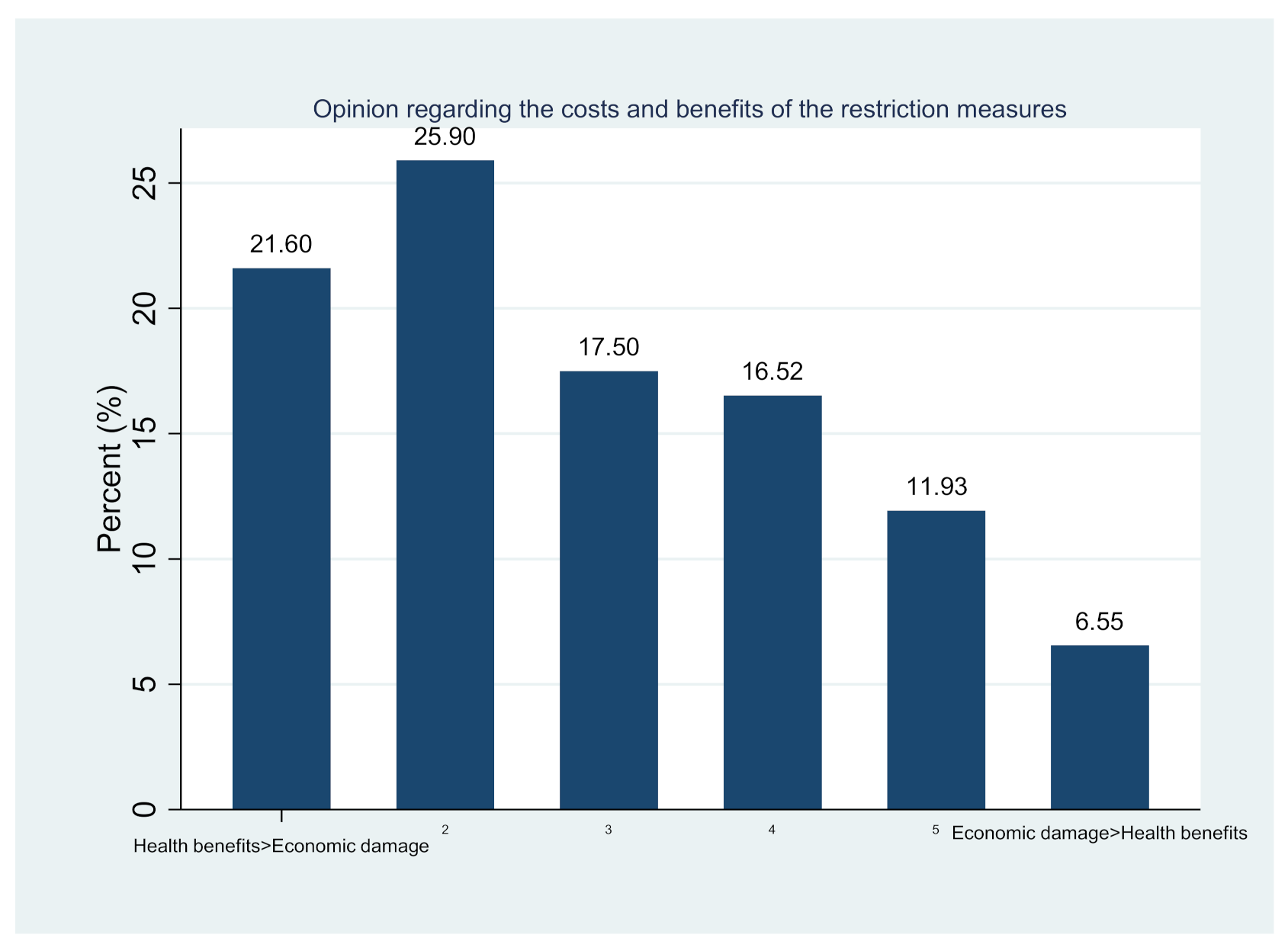
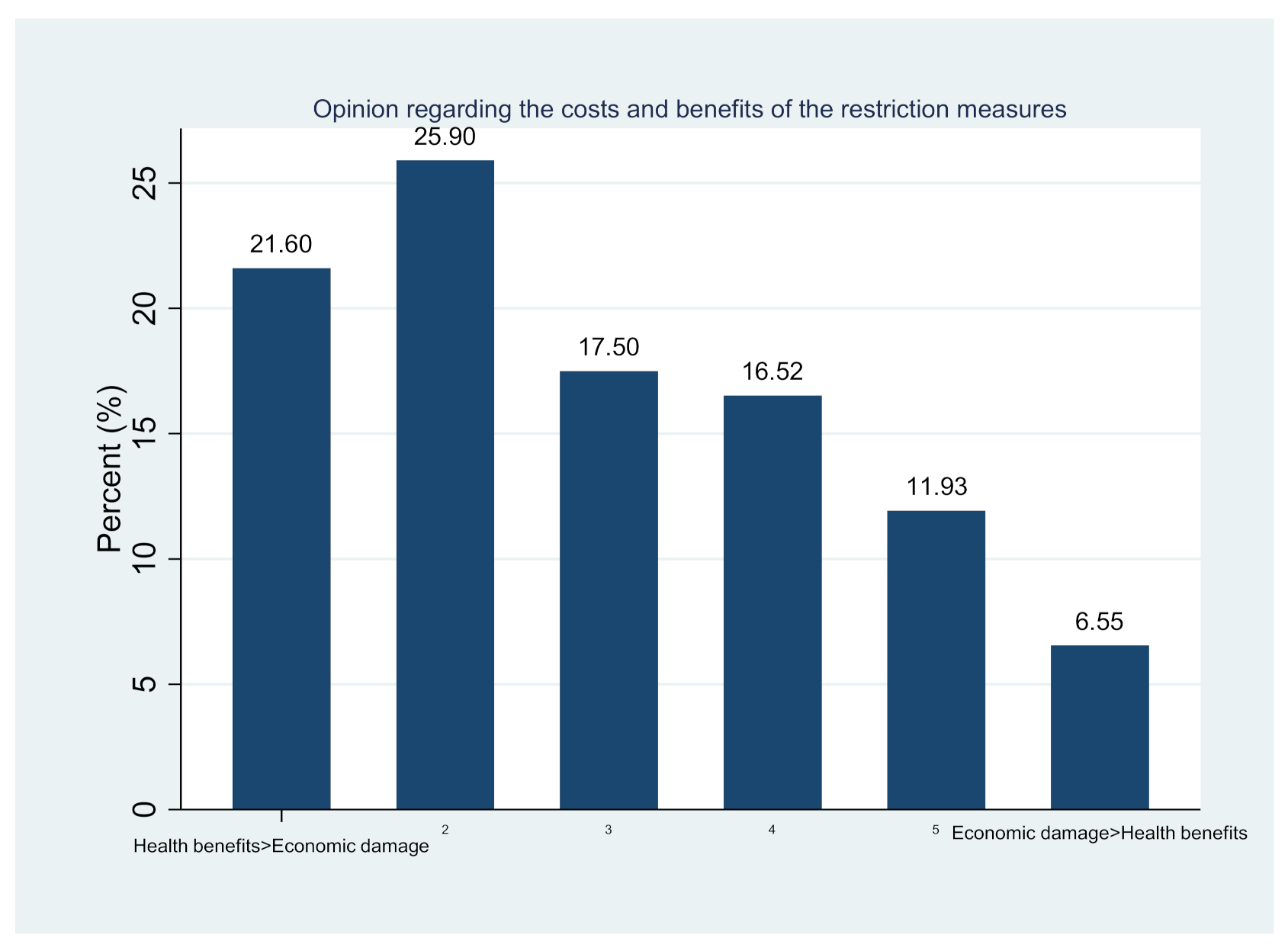
| Category | % (n) |
|---|---|
| The health benefits are greater than the economic damage | 21.60 (221) |
| 2 | 25.90 (265) |
| 3 | 17.50 (179) |
| 4 | 16.52 (169) |
| 5 | 11.93 (122) |
| The economic damage is greater than the health benefits | 6.55 (67) |
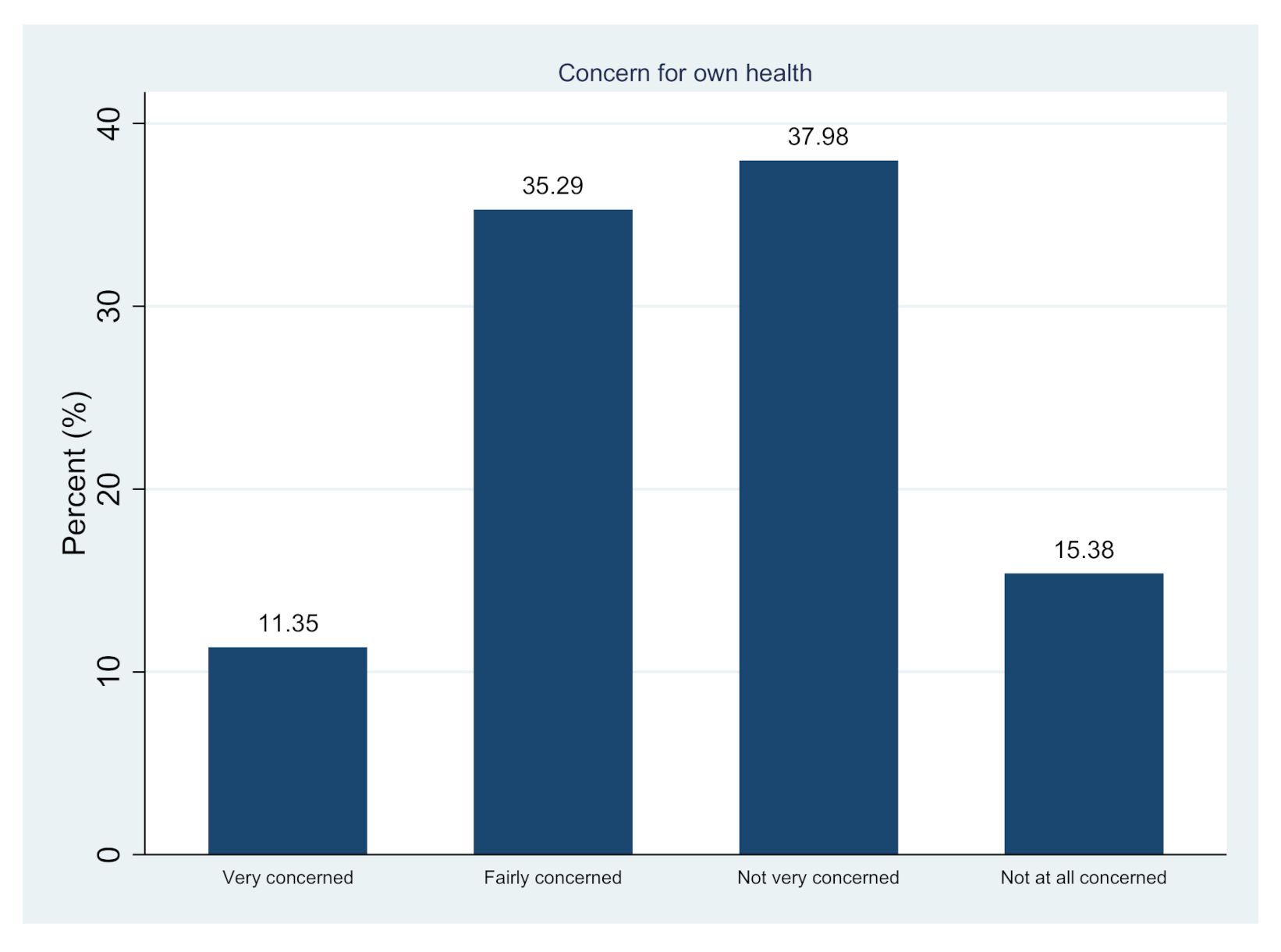
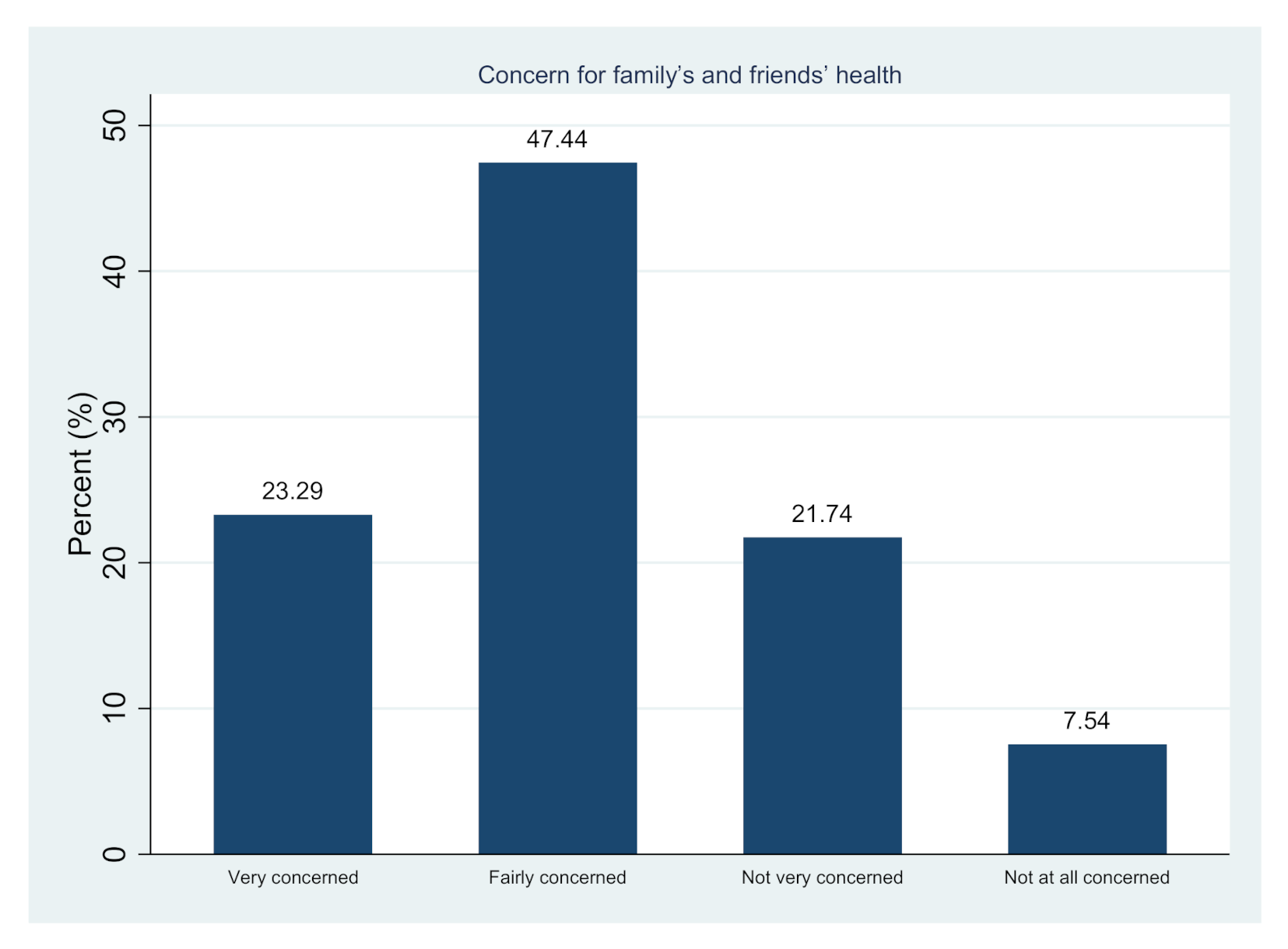
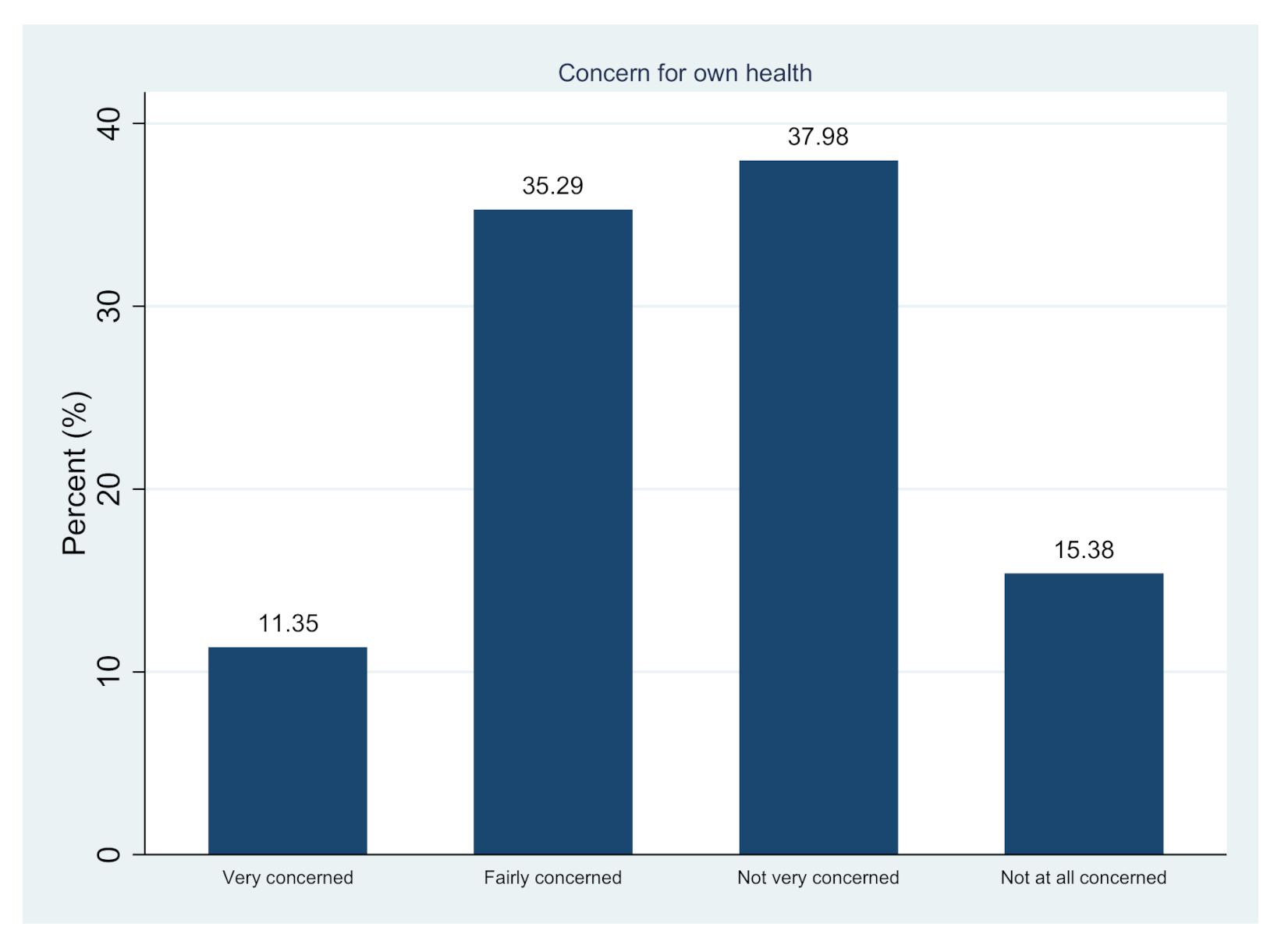
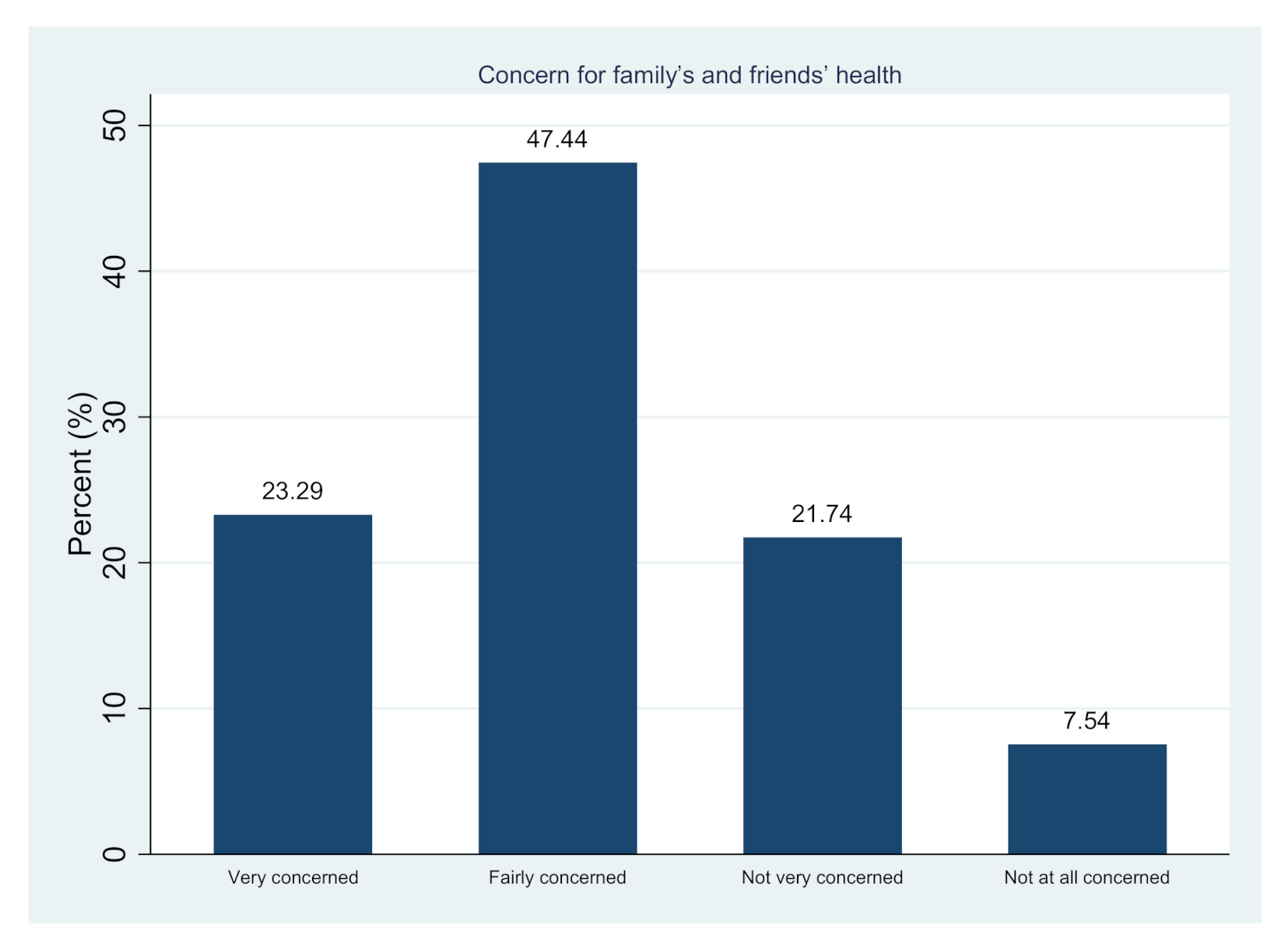
| Category | Concern for Own Health % (n) | Concern for Family’s and Friends’ Health % (n) |
|---|---|---|
| Very concerned | 11.35 (118) | 23.29 (241) |
| Fairly concerned | 35.29 (367) | 47.44 (491) |
| Not very concerned | 37.98 (395) | 21.74 (225) |
| Not at all concerned | 15.38 (160) | 7.54 (78) |
| Variable | OR | p | 95% CI | |
|---|---|---|---|---|
| Experiencing difficulties to have proper and decent quality meals since the beginning of the COVID-19 pandemic | 1.674 | <0.001 | 1.268 | 2.211 |
| Experiencing other financial issues since the beginning of the COVID-19 pandemic | 1.432 | 0.001 | 1.163 | 1.764 |
| Public opinion regarding the costs and benefits of the restriction measures | <0.001 | |||
| The health benefits are greater than the economic damage | 0.560 | <0.001 | 0.446 | 0.702 |
| 2 | 0.487 | <0.001 | 0.391 | 0.607 |
| 3 | 0.655 | 0.001 | 0.513 | 0.837 |
| 4 | 0.548 | <0.001 | 0.416 | 0.720 |
| 5 | 0.525 | 0.001 | 0.360 | 0.765 |
| COVID-19-related concern for own health | 0.025 | |||
| Very concerned vs. subsequent levels | 0.647 | 0.009 | 0.466 | 0.899 |
| Fairly concerned vs. subsequent levels | 0.812 | 0.065 | 0.651 | 1.013 |
| Not very concerned vs. not at all concerned | 0.795 | 0.097 | 0.607 | 1.043 |
| COVID-19-related concern for health of family and friends | 0.011 | |||
| Very concerned vs. subsequent levels | 0.696 | 0.008 | 0.532 | 0.910 |
| Fairly concerned vs. subsequent levels | 0.741 | 0.017 | 0.580 | 0.948 |
| Not very concerned vs. not at all concerned | 0.636 | 0.012 | 0.448 | 0.904 |
| Cons1 | 2.097 | <0.001 | 1.748 | 2.515 |
| Cons2 | 0.353 | <0.001 | 0.286 | 0.436 |
| Cons3 | 0.240 | <0.001 | 0.177 | 0.324 |
| Variable | Coefficient | p | 95% CI | |
|---|---|---|---|---|
| h | 1.020 | <0.001 | 0.843 | 1.197 |
| h2 | −0.045 | 0.586 | −0.206 | 0.116 |
| Cons1 | 0.760 | <0.001 | 0.585 | 0.935 |
| Cons2 | −1.031 | <0.001 | −1.185 | −0.877 |
| Cons2 | −1.403 | <0.001 | −1.692 | −1.115 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zavras, D. Studying Satisfaction with the Restriction Measures Implemented in Greece during the First COVID-19 Pandemic Wave. World 2021, 2, 379-390. https://doi.org/10.3390/world2030024
Zavras D. Studying Satisfaction with the Restriction Measures Implemented in Greece during the First COVID-19 Pandemic Wave. World. 2021; 2(3):379-390. https://doi.org/10.3390/world2030024
Chicago/Turabian StyleZavras, Dimitris. 2021. "Studying Satisfaction with the Restriction Measures Implemented in Greece during the First COVID-19 Pandemic Wave" World 2, no. 3: 379-390. https://doi.org/10.3390/world2030024
APA StyleZavras, D. (2021). Studying Satisfaction with the Restriction Measures Implemented in Greece during the First COVID-19 Pandemic Wave. World, 2(3), 379-390. https://doi.org/10.3390/world2030024