
Communicable Disease Surveillance in Lebanon during the Syrian Humanitarian Crisis, 2013–2019


Abstract
1. Introduction
2. Materials and Methods
2.1. Indicator-Based Surveillance
2.1.1. Routine Surveillance System
2.1.2. Disease-Specific Surveillance Systems within ESU
2.1.3. Syndromic Surveillance
2.2. Sensitization Activities
2.3. Data Sharing and Collaboration
3. Results
4. Discussion
4.1. Strengths
4.2. Challenges and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNHCR. Situation Syria Regional Refugee Response. Available online: https://data.unhcr.org/en/situations/syria/location/71 (accessed on 3 June 2022).
- UNHCR Lebanon at a Glance. UNHCR Lebanon. Available online: https://www.unhcr.org/lb/at-a-glance (accessed on 20 April 2023).
- World Food Programme. Vulnerability Assessment of Syrian Refugees in Lebanon—VASyR 2018. 2018. Available online: https://www.wfp.org/publications/vulnerability-assessment-syrian-refugees-lebanon-vasyr-2018 (accessed on 3 June 2022).
- United Nations-Lebanon. Lebanon Crisis Response Plan (2017–2020). United Nations in Lebanon. 2020. Available online: https://lebanon.un.org/en/102825-lebanon-crisis-response-plan-2017-2020 (accessed on 3 June 2022).
- Abubakar, I.; Aldridge, R.W.; Devakumar, D.; Orcutt, M.; Burns, R.; Barreto, M.L.; Dhavan, P.; Fouad, F.M.; Groce, N.; Guo, Y.; et al. The UCL-Lancet Commission on Migration and Health: The health of a world on the move. Lancet 2018, 392, 2606–2654. [Google Scholar] [CrossRef] [PubMed]
- Saleh, M.; Farah, Z.; Howard, N. Infectious disease surveillance for refugees at borders and in destination countries: A scoping review. BMC Public Health 2022, 22, 227. [Google Scholar] [CrossRef]
- World Health Organization. Hepatitis A. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-a (accessed on 3 June 2022).
- Syrian Refugee Response: Vulnerability Assessment of Syrian Refugees in Lebanon, 8 August 2014—Lebanon. ReliefWeb, 12 August 2014. Available online: https://reliefweb.int/report/lebanon/syrian-refugee-response-vulnerability-assessment-syrian-refugees-lebanon-8-aug-2014 (accessed on 18 April 2023).
- Mellou, K.; Chrisostomou, A.; Sideroglou, T.; Georgakopoulou, T.; Kyritsi, M.; Hadjichristodoulou, C.; Tsiodras, S. Hepatitis A among refugees, asylum seekers and migrants living in hosting facilities, Greece, April to December 2016. Eurosurveillance 2017, 22, 30448. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Leishmaniasis. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/leishmaniasis (accessed on 3 June 2022).
- World Health Organization. Regional Situation Reports-Syria. World Health Organization—Regional Office for the Eastern Mediterranean. Available online: http://www.emro.who.int/syr/syria-infocus/regional-situation-reports-2015.html (accessed on 3 June 2022).
- Ministry of Public Health-Lebanon. Epidemiological Surveillance. Available online: http://www.moph.gov.lb (accessed on 3 June 2022).
- Ozaras, R.; Leblebicioglu, H.; Sunbul, M.; Tabak, F.; Balkan, I.I.; Yemisen, M.; Sencan, I.; Ozturk, R. The Syrian conflict and infectious diseases. Expert Rev. Anti Infect. Ther. 2016, 14, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Haddad, N.; Naja, H.A.; Kassouf, S.; Jimenez, A.P.; Mrad, G.A.; Ammar, W.; Ghosn, N. Effectiveness of Previous Mumps Vaccination during the 2014–2015 Outbreak in Lebanon. World Health Organization—Regional Office for the Eastern Mediterranean. 2019. Available online: http://www.emro.who.int/in-press/research/effectiveness-of-previous-mumps-vaccination-during-the-20142015-outbreak-in-leba.html (accessed on 3 June 2022).
- World Health Organization. Measles. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/measles (accessed on 3 June 2022).
- MSF. Syria: Measles Epidemic Signals Growing Humanitarian Needs. Médecins Sans Frontières (MSF) International. 2013. Available online: https://www.msf.org/syria-measles-epidemic-signals-growing-humanitarian-needs (accessed on 3 June 2022).
- World Health Organization. Poliomyelitis (Polio). Available online: https://www.who.int/health-topics/poliomyelitis#tab=tab_1 (accessed on 3 June 2022).
- Polio Global Eradication Initiave. GPEI-Syria Achieves Polio Milestone. 2016. Available online: https://polioeradication.org/news-post/syria-achieves-polio-milestone/ (accessed on 3 June 2022).
- German, R.R.; Lee, L.M.; Horan, J.M.; Milstein, R.L.; A Pertowski, C.; Waller, M.N. Updated Guidelines for Evaluating Public Health Surveillance Systems. 2001. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5013a1.htm (accessed on 3 June 2022).
- Ammar, W.; Kdouh, O.; Hammoud, R.; Hamadeh, R.; Harb, H.; Ammar, Z.; Atun, R.; Christiani, D.; A Zalloua, P. Health system resilience: Lebanon and the Syrian refugee crisis. J. Glob. Health 2016, 6, 020704. [Google Scholar] [CrossRef]
- Napoli, C.; Riccardo, F.; Declich, S.; Dente, M.G.; Pompa, M.G.; Rizzo, C.; Rota, M.C.; Bella, A.; The National Working Group. An Early Warning System Based on Syndromic Surveillance to Detect Potential Health Emergencies among Migrants: Results of a Two-Year Experience in Italy. Int J. Environ. Res. Public Health 2014, 11, 8529–8541. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | Year | Total | ||||||
|---|---|---|---|---|---|---|---|---|
| 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | ||
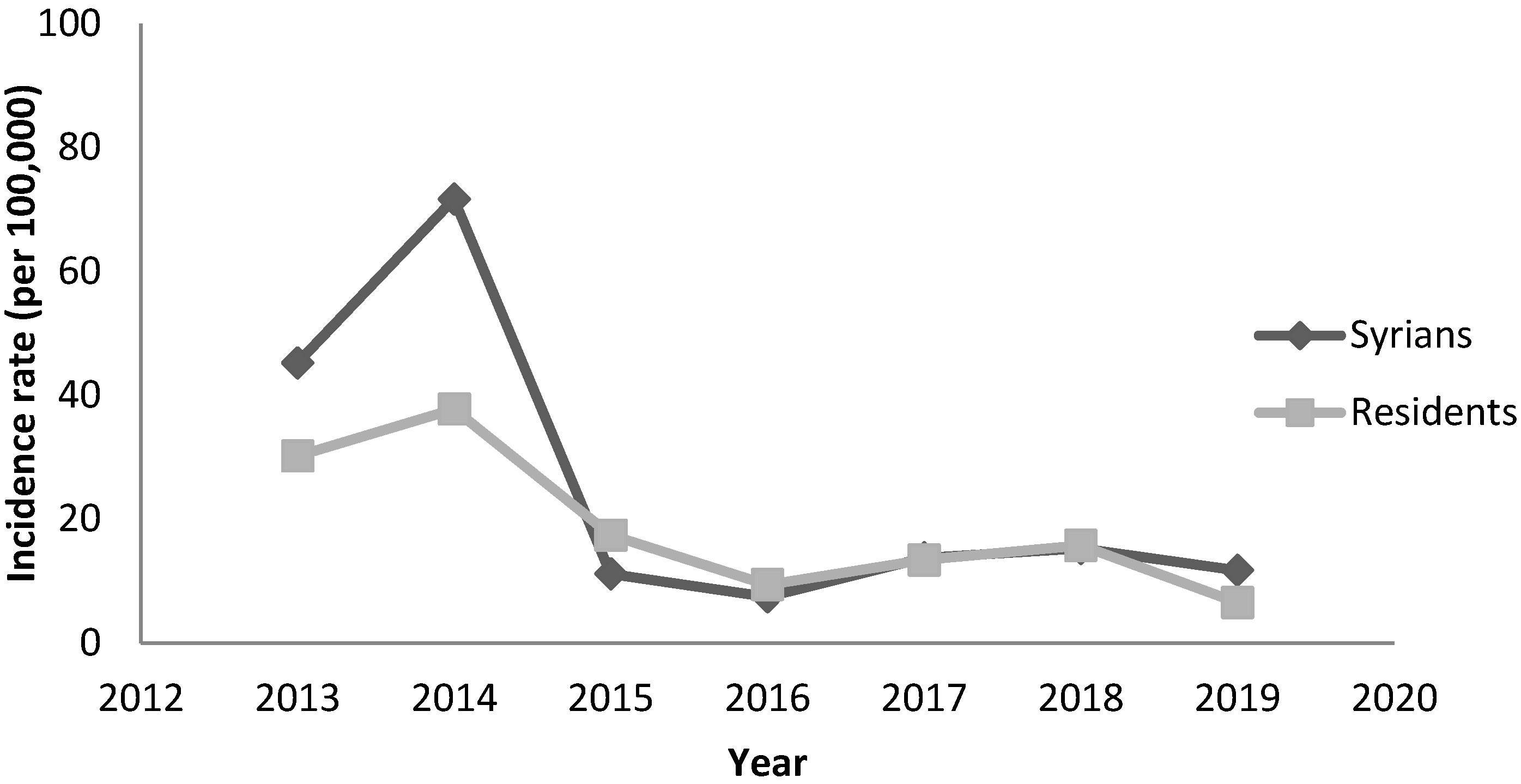
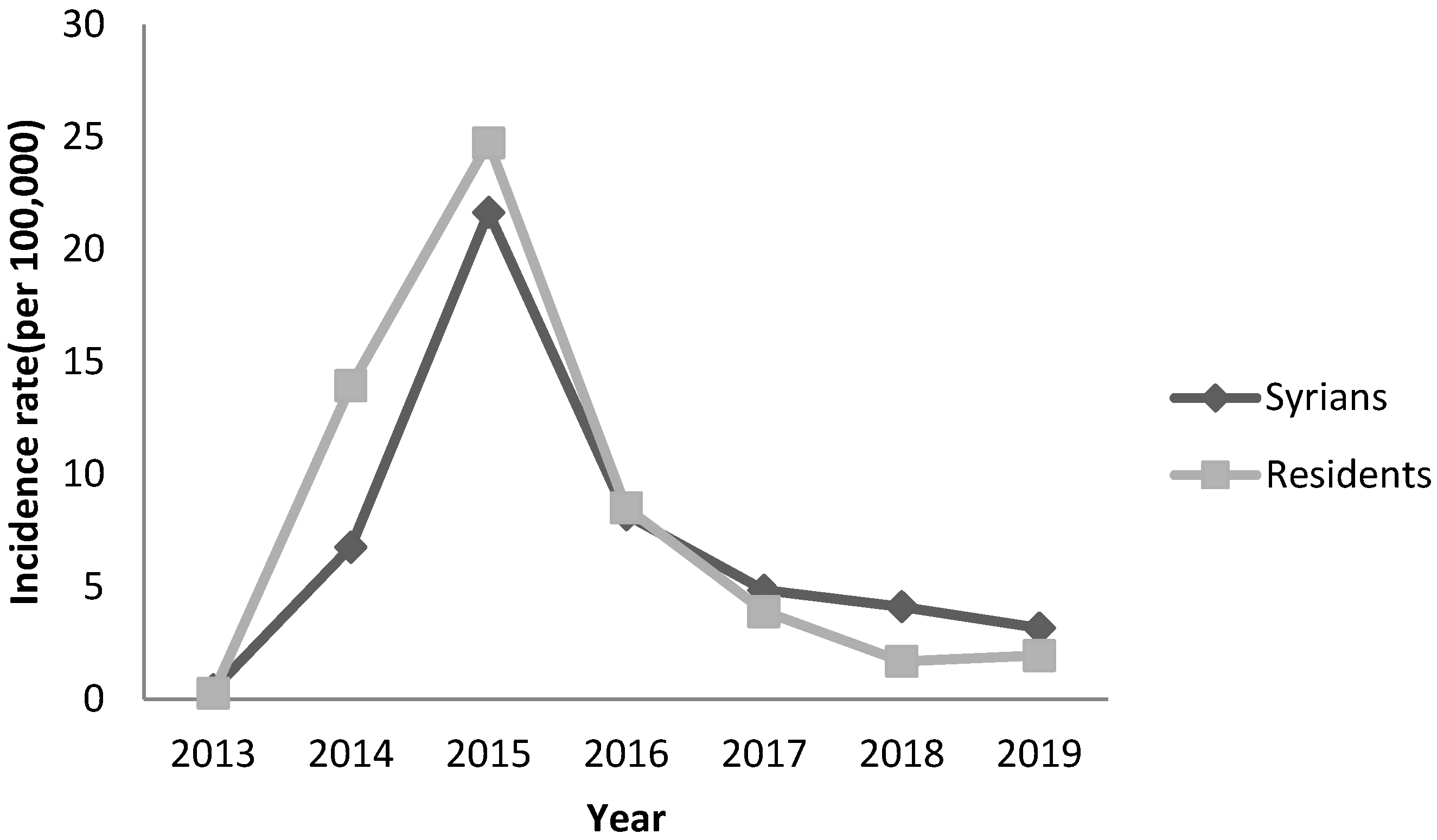
| Viral hepatitis A | 220 | 859 | 182 | 78 | 139 | 152 | 111 | 1741 |
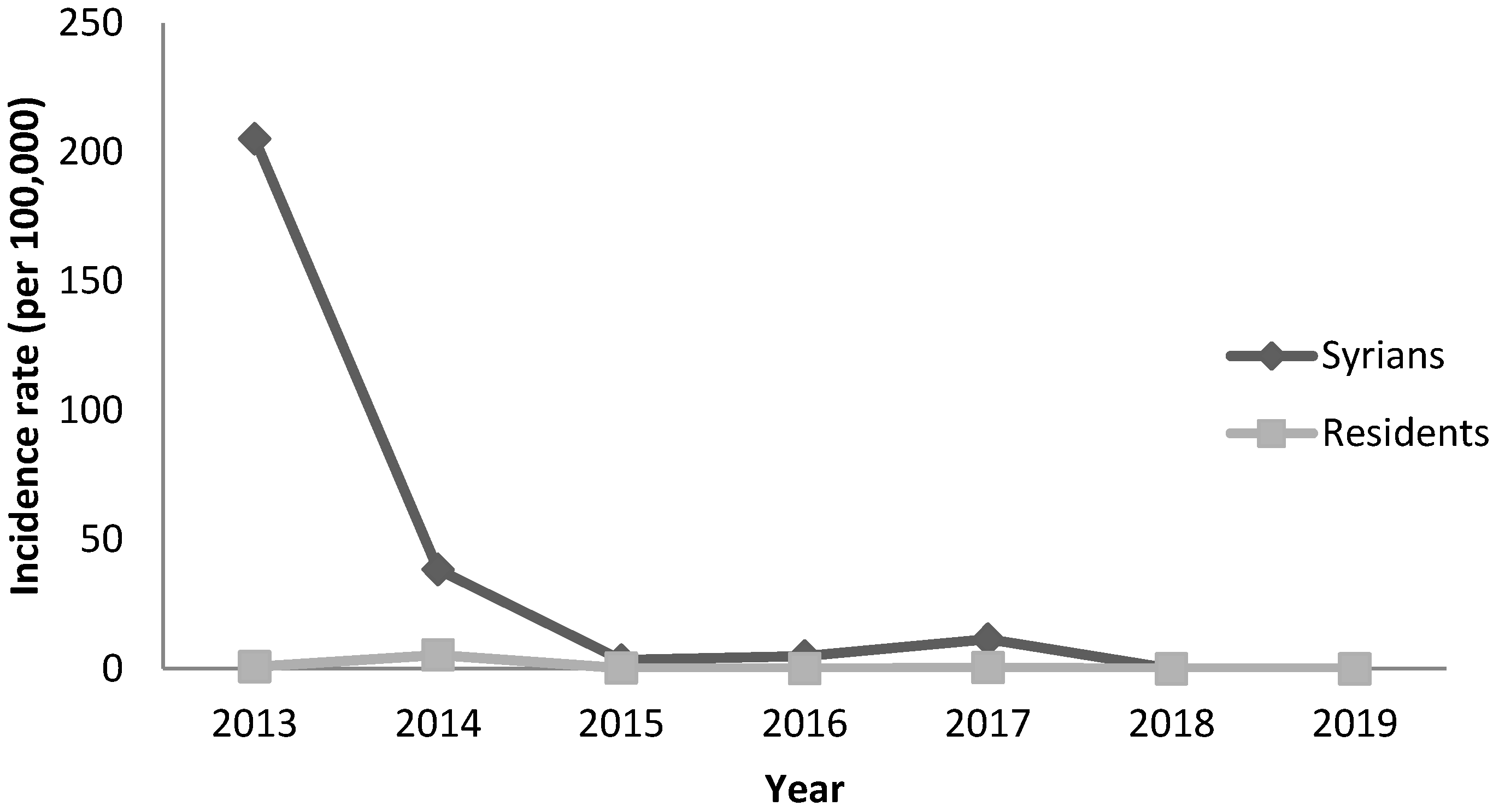
| Leishmaniasis | 998 | 461 | 56 | 52 | 116 | 0 | 0 | 1683 |
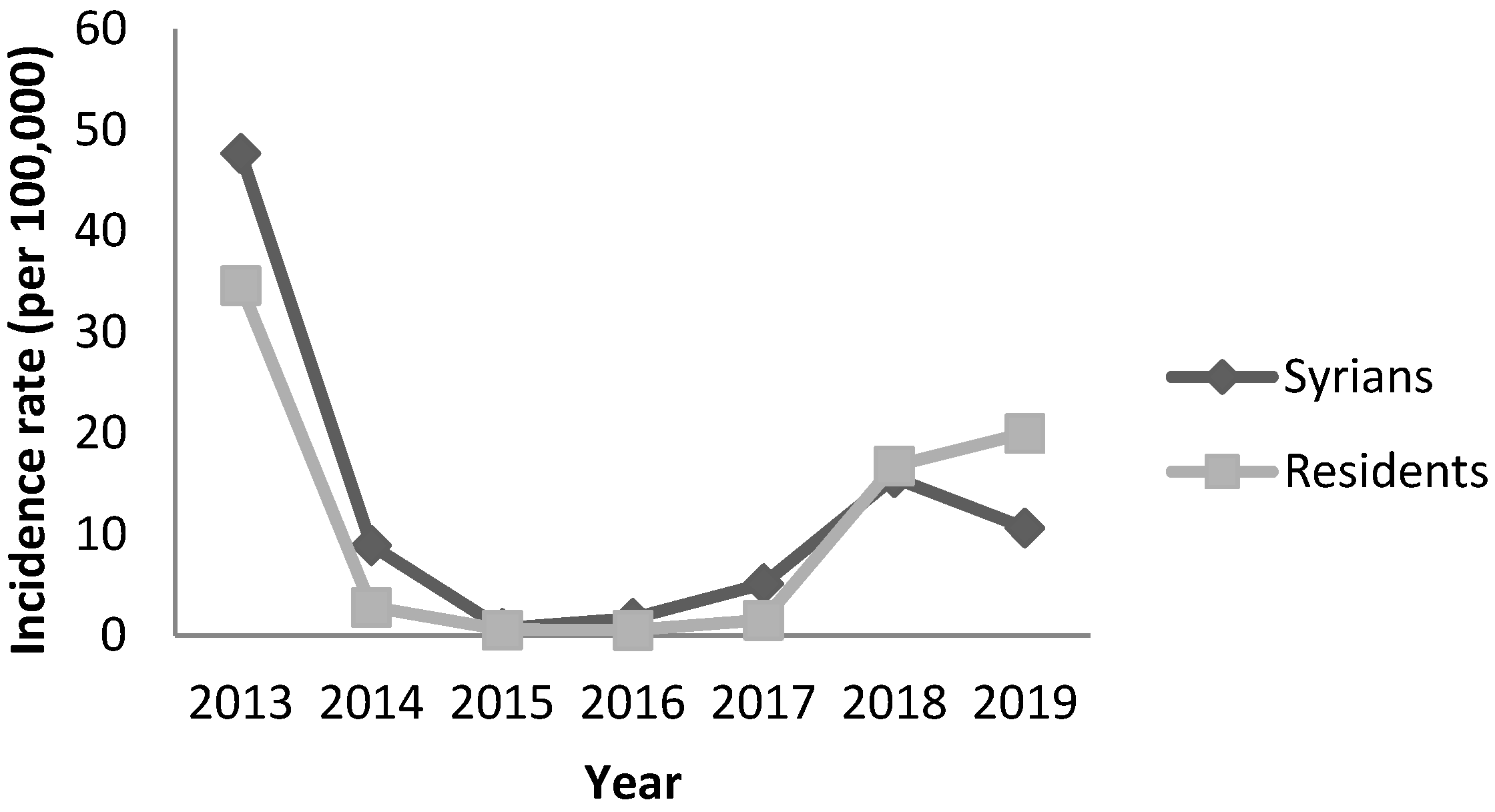
| Measles | 232 | 107 | 12 | 18 | 52 | 156 | 101 | 678 |
| Mumps | 2 | 81 | 354 | 86 | 49 | 41 | 30 | 643 |
| Brucellosis | 12 | 35 | 85 | 165 | 149 | 26 | 32 | 504 |
| Viral hepatitis B | 8 | 31 | 53 | 48 | 52 | 28 | 36 | 256 |
| Malaria | 1 | 5 | 3 | 0 | 75 | 82 | 80 | 246 |
| Meningitis | 24 | 34 | 61 | 63 | 0 | 0 | 0 | 182 |
| Food poisoning | 11 | 30 | 16 | 28 | 74 | 14 | 0 | 173 |
| Typhoid fever | 21 | 26 | 70 | 11 | 19 | 4 | 6 | 157 |
| Pertussis | 9 | 25 | 8 | 18 | 22 | 26 | 23 | 131 |
| Acute flaccid paralysis | 7 | 12 | 10 | 17 | 19 | 33 | 18 | 116 |
| Rubella | 1 | 12 | 2 | 6 | 6 | 4 | 9 | 40 |
| Viral hepatitis C | 4 | 5 | 6 | 8 | 0 | 0 | 0 | 23 |
| Rabies | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 3 |
| Leprosy | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 2 |
| Tetanus | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 |
| Gonorrhea | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 |
| Syphilis | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 |
| Poliomyelitis | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farah, Z.; Saleh, M.; Abou El Naja, H.; Chaito, L.; Ghosn, N. Communicable Disease Surveillance in Lebanon during the Syrian Humanitarian Crisis, 2013–2019. Epidemiologia 2023, 4, 255-266. https://doi.org/10.3390/epidemiologia4030026
Farah Z, Saleh M, Abou El Naja H, Chaito L, Ghosn N. Communicable Disease Surveillance in Lebanon during the Syrian Humanitarian Crisis, 2013–2019. Epidemiologia. 2023; 4(3):255-266. https://doi.org/10.3390/epidemiologia4030026
Chicago/Turabian StyleFarah, Zeina, Majd Saleh, Hala Abou El Naja, Lina Chaito, and Nada Ghosn. 2023. "Communicable Disease Surveillance in Lebanon during the Syrian Humanitarian Crisis, 2013–2019" Epidemiologia 4, no. 3: 255-266. https://doi.org/10.3390/epidemiologia4030026
APA StyleFarah, Z., Saleh, M., Abou El Naja, H., Chaito, L., & Ghosn, N. (2023). Communicable Disease Surveillance in Lebanon during the Syrian Humanitarian Crisis, 2013–2019. Epidemiologia, 4(3), 255-266. https://doi.org/10.3390/epidemiologia4030026