

Analytical Characteristics and Clinical Performance of Anti-Müllerian Hormone Immunoassay on the ADVIA Centaur® System: A Comparison with Other Chemiluminescent Methods

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Study Design
2.2. Ethical Approval
2.3. Analytical Performance of AMH Assay
2.4. Clinical Sensitivity and Specificity of the ADVIA Centaur AMH Assay
2.5. Statistical Analysis
3. Results
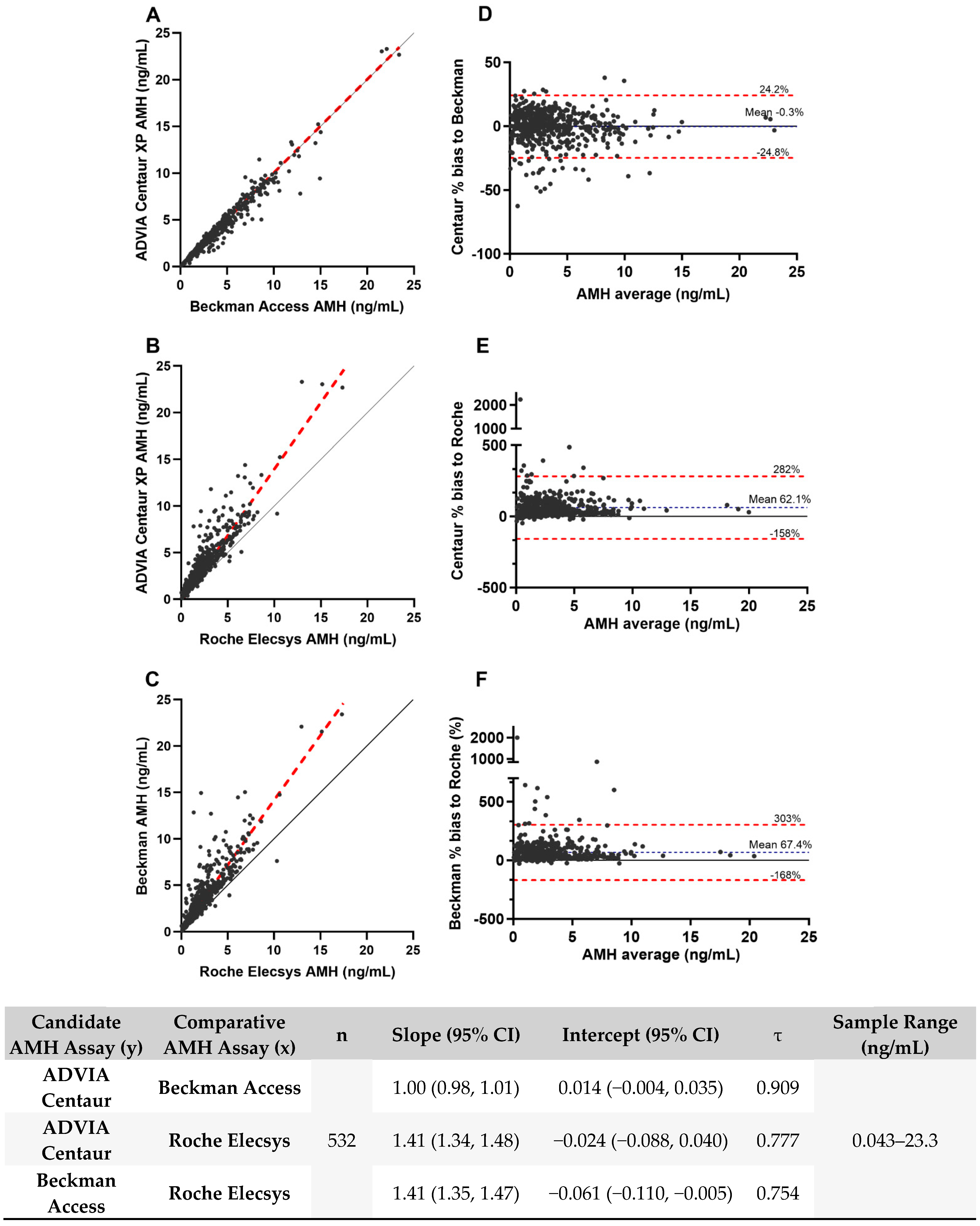
3.1. Analytical Performance
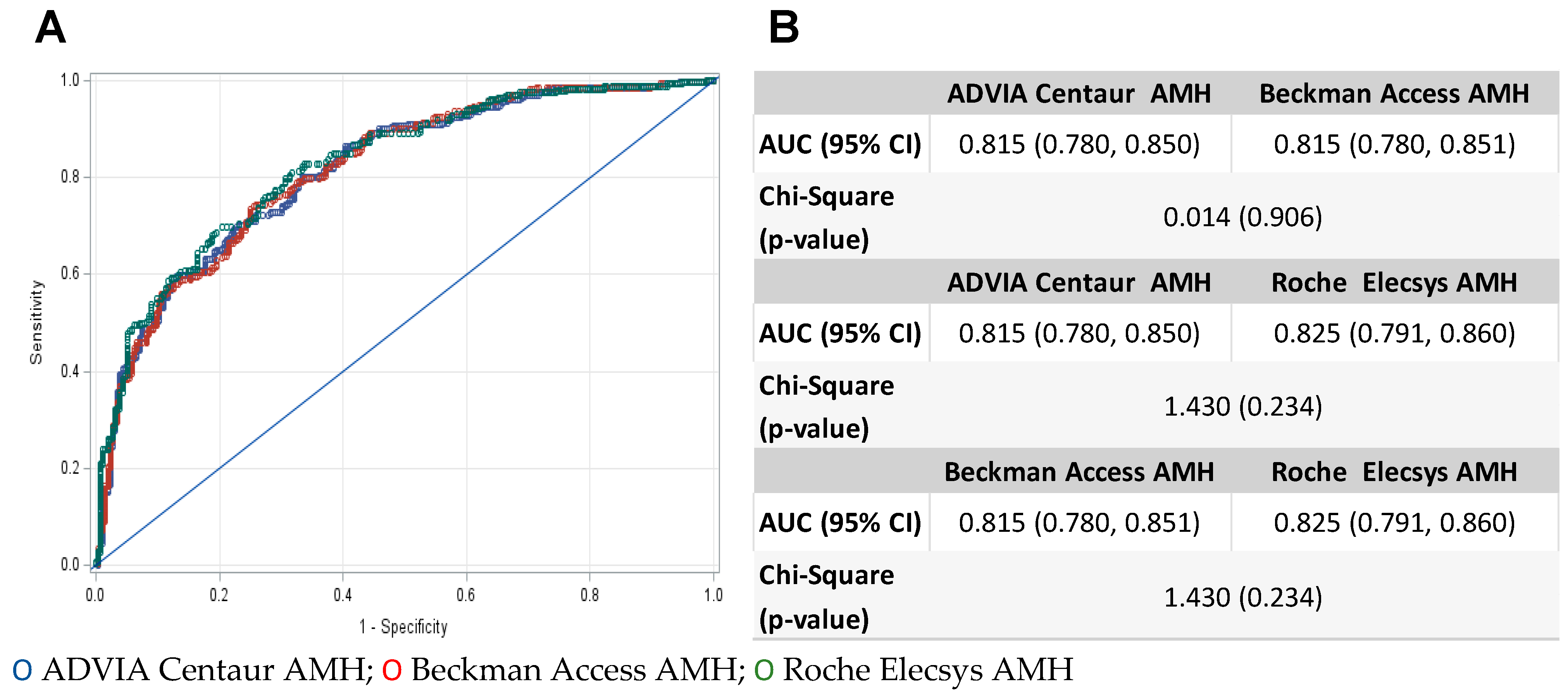
3.2. Clinical Performance
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Institutional Review Board Site Approvals (Date and Code)

{kind=link}
{kind=link}
{kind=link}
| Site | Code | Approval Date |
|---|---|---|
| Fertility and IVF Center of Miami | SSU00128953 | 14 August 2020 |
| Bloom Reproductive Institute | SSU00129719 | 25 August 2020 |
| Fertility Treatment Center | SSU00125180 | 2 July 2020 |
| Reproductive Endocrinology Associates of Charlotte | SSU00129791 | 25 August 2020 |
| Center for Assisted Reproduction | SSU00125251 | 2 July 2020 |
| Reproductive Associated of Delaware | SSU00128589 | 13 August 2020 |
| Utah Fertility Clinic | SSU00129326 | 19 August 2020 |
| Women’s Medical Research Group | SSU00125192 | 2 July 2020 |
| Center for Reproductive Medicine | SSU00132960 | 15 October 2020 |
| Shady Grove Fertility Center | SSU00126730 | 16 July 2020 |
| Houston Fertility Clinic | SSU00125481 | 9 July 2020 |
References
- Infertility Workup for the Women’s Health Specialist: ACOG Committee Opinion, Number 781. Obstet. Gynecol. 2019, 133, e377–e384. [CrossRef] [PubMed]
- Moolhuijsen, L.M.; Visser, J.A. Anti-Müllerian Hormone and Ovarian Reserve: Update on Assessing Ovarian Function. J. Clin. Endocrinol. Metab. 2020, 105, 3361–3373. [Google Scholar] [CrossRef] [PubMed]
- Penzias, A.; Azziz, R.; Bendikson, K.; Falcone, T.; Hansen, K.; Hill, M.; Hurd, W.; Jindal, S.; Kalra, S.; Mersereau, J.; et al. Testing and interpreting measures of ovarian reserve: A committee opinion. Fertil. Steril. 2020, 114, 1151–1157. [Google Scholar] [CrossRef] [PubMed]
- Baker, V.L.; Gracia, C.; Glassner, M.J.; Schnell, V.L.; Doody, K.; Coddington, C.C.; Shin, S.S.; Marshall, L.A.; Alper, M.M.; Morales, A.J.; et al. Multicenter evaluation of the Access AMH antimüllerian hormone assay for the prediction of antral follicle count and poor ovarian response to controlled ovarian stimulation. Fertil. Steril. 2018, 110, 506–513.e3. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, M.H.; Reuter, L.M.; Baker, V.L.; Craig, L.B.; Sakkas, D.; Surrey, E.; Doody, K.J.; Jungheim, E.S.; Bayrak, A.B.; Hund, M.; et al. A multicentre evaluation of the Elecsys® anti-Müllerian hormone immunoassay for prediction of antral follicle count. Reprod. BioMedicine Online 2019, 38, 845–852. [Google Scholar] [CrossRef] [PubMed]
- van Disseldorp, J.; Lambalk, C.B.; Kwee, J.; Looman, C.W.N.; Eijkemans, M.J.C.; Fauser, B.C.; Broekmans, F.J. Comparison of inter-and intra-cycle variability of anti-Müllerian hormone and antral follicle counts. Hum. Reprod. 2010, 25, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Dumanski, S.M.; Ahmed, S.B. Fertility and reproductive care in chronic kidney disease. J. Nephrol. 2019, 32, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Kelley, A.S.; Badon, S.E.; Lanham, M.S.; Fisseha, S.; Moravek, M.B. Body mass index restrictions in fertility treatment: A national survey of OB/GYN subspecialists. J. Assist. Reprod. Genet. 2019, 36, 1117–1125. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Karvonen-Gutierrez, C.; Kong, S.; Arends, V.; Steffes, M.; McConnell, D.S.; Randolph, J.F.; Harlow, S.D. Antimüllerian hormone among women with and without type 1 diabetes: The Epidemiology of Diabetes Interventions and Complications Study and the Michigan Bone Health and Metabolism Study. Fertil. Steril. 2016, 106, 1446–1452. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, A.L.; Kazemi, M.; Lujan, M.E. Impact of obesity on anti-mullerian hormone (Amh) levels in women of reproductive age. J. Clin. Med. 2021, 10, 3192. [Google Scholar] [CrossRef] [PubMed]
- Robertson, D.M.; Lee, C.H.; Baerwald, A. Interrelationships among reproductive hormones and antral follicle count in human menstrual cycles. Endocr. Connect. 2016, 5, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Lin, C.; Zhang, M.; Lv, F.; Zhu, X.; Han, X.; Cai, X.; Ji, L. Assessment of ovarian reserve in patients with type 1 diabetes: A systematic review and meta-analysis. Endocrine 2022, 77, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Akobeng, A.K. Understanding diagnostic tests 3: Receiver operating characteristic curves. Acta Paediatr. Int. J. Paediatr. 2007, 96, 644–647. [Google Scholar] [CrossRef] [PubMed]
- Access®. Anti-Müllerian Hormone (AMH) Assay Instructions for Use; B15676_Rev C; Beckman: Marseille, France, 2019. [Google Scholar]
- Vrzáková, R.; Šimánek, V.; Topolčan, O.; Vurm, V.; Slouka, D.; Kučera, R. The Stability of the Anti-Müllerian Hormone in Serum and Plasma Samples under Various Preanalytical Conditions. Diagnostics 2023, 13, 1501. [Google Scholar] [CrossRef] [PubMed]
- ADVIA Centaur®. Anti-Müllerian Hormone (AMH) Assay Instructions for Use; 10998436_EN Rev.01; Siemens Diagnostics Inc.: Tarrytown, NY, USA, 2023. [Google Scholar]
- Cobas®. Elecsys Anti-Müllerian Hormone (AMH) Assay Instructions for Use; 08819378501_Rev 02; Roche: Mannheim, Germany, 2022. [Google Scholar]
- Committee opinion no. 589. Female age-related fertility decline. Obstet. Gynecol. 2014, 123, 719–721. [Google Scholar]
- Nelson, S.M.; Pastuszek, E.; Kloss, G.; Malinowska, I.; Liss, J.; Lukaszuk, A.; Plociennik, L.; Lukaszuk, K. Two new automated, compared with two enzyme-linked immunosorbent, antimüllerian hormone assays. Fertil. Steril. 2015, 104, 1016–1021e6. [Google Scholar] [CrossRef] [PubMed]
- Punchoo, R.; Bhoora, S. Variation in the Measurement of Anti-Müllerian Hormone–What Are the Laboratory Issues? Front. Endocrinol. 2021, 12, 719029. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, J.; Hockley, J.; Rigsby, P.; Burns, C. Establishment of a WHO Reference Reagent for anti-Mullerian hormone. Reprod. Biol. Endocrinol. 2020, 18, 86. [Google Scholar] [CrossRef] [PubMed]
- Li, H.W.R.; Robertson, D.M.; Burns, C.; Ledger, W.L. Challenges in Measuring AMH in the Clinical Setting. Front. Endocrinol. 2021, 12, 691432. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Feng, G.; Ma, C.; Han, Y.; Zhou, J.; Song, J.; Su, Y.; Zhong, Q.; Chen, F.; Cui, L.; et al. AMH converter: An online tool for converting results between the different anti-Müllerian hormone assays of Roche Elecsys®, Beckman Access, and Kangrun. PeerJ 2023, 11, e15301. [Google Scholar] [CrossRef] [PubMed]

| Inclusion Criteria | Exclusion Criteria |
|---|---|
| 22 to <46 years of age | BMI ≥ 40 |
| Both ovaries present (as visualized on TVUS) | Pregnant within the past 3 months |
| Transvaginal ultrasound of the antral follicle count (measuring 2–10 mm diameter) between days 2–4 of menstrual cycle a | Taking chemical contraceptives within the past 3 months or hormonal medication in the past 21 days prior to the study blood draw |
| Polycystic ovary syndrome diagnosis following Rotterdam criteria, of which 2 out of 3 criteria are met | |
| Ovarian abnormalities such as cysts or solid masses > 2 cm or surgically confirmed endometrioma | |
| Ovarian surgery within 6 months prior to study blood draw | |
| Actively undergoing treatment for malignancy | |
| Positive hCG levels | |
| History of ≥3 previous ovarian IVF stimulation cycles b | |
| Endocrine or metabolic disorders, including diabetes, pituitary, adrenal, pancreas, liver and kidney disease, hypothalamic disorders, high prolactin, congenital hyperplasia, premature ovarian failure, and premature ovarian insufficiency |
| Sample | Mean (ng/mL) | Repeatability | Repeatability | Within-Lab | Within-Lab | Reproducibility (Total Imprecision) | |
|---|---|---|---|---|---|---|---|
| SD (ng/mL) | %CV (95% CI) | SD (ng/mL) | %CV (95% CI) | SD (ng/mL) | %CV (95% CI) | ||
| Serum A | 0.112 | 0.0032 | 2.9 (2.6–3.1) | 0.0036 | 3.2 (2.9–3.6) | 0.0049 | 4.4 (3.1–7.8) |
| Serum B | 0.193 | 0.0046 | 2.4 (2.2–2.6) | 0.0053 | 2.7 (2.5–3.0) | 0.0066 | 3.4 (2.6–5.1) |
| Serum C | 0.969 | 0.0205 | 2.1 (1.9–2.3) | 0.0236 | 2.4 (2.3–2.6) | 0.0240 | 2.5 (2.3–2.7) |
| Serum D | 3.60 | 0.092 | 2.6 (2.3–2.8) | 0.107 | 3.0 (2.8–3.2) | 0.115 | 3.2 (2.8–3.8) |
| Serum E | 6.71 | 0.156 | 2.3 (2.1–2.6) | 0.198 | 3.0 (2.7–3.2) | 0.224 | 3.3 (2.8–4.2) |
| Serum F | 6.93 | 0.158 | 2.3 (2.1–2.5) | 0.177 | 2.6 (2.4–2.8) | 0.206 | 3.0 (2.4–4.1) |
| Serum G | 16.2 | 0.34 | 2.1 (1.9–2.3) | 0.40 | 2.5 (2.2–2.7) | 0.52 | 3.2 (2.3–5.4) |
| Serum H | 16.4 | 0.37 | 2.3 (2.1–2.5) | 0.42 | 2.6 (2.4–2.8) | 0.47 | 2.9 (2.4–3.7) |
| Control 1 | 0.955 | 0.0252 | 2.6 (2.4–2.9) | 0.0284 | 3.0 (2.8–3.2) | 0.0312 | 3.3 (2.8–3.9) |
| Control 2 | 4.75 | 0.120 | 2.5 (2.3–2.8) | 0.135 | 2.8 (2.7–3.1) | 0.140 | 2.9 (2.7–3.2) |
| Control 3 | 14.1 | 0.33 | 2.3 (2.1–2.6) | 0.37 | 2.6 (2.4–2.8) | 0.41 | 2.9 (2.4–3.6) |
| Analysis | ||
|---|---|---|
| N = 255 | N = 277 | |
| Variable | AFC ≤ 15 | AFC > 15 |
| Mean Age in Years (SD) | 36.1 (4.44) | 32.9 (4.02) |
| Mean BMI (kg/m2) (SD) | 27.05 (5.274) | 26.74 (4.946) |
| Centaur Mean AMH (SD) | 2.21 (2.138) | 4.94 (3.164) |
| Beckman Mean AMH (SD) | 2.23 (2.127) | 5.05 (3.256) |
| Roche Mean AMH (SD) | 1.42 (1.259) | 3.35 (2.206) |
| Race n/N (%) | ||
| American Indian or Alaska Native | 1/255 (0.4%) | 3/277 (1.1%) |
| Asian | 23/255 (9.0%) | 16/277 (5.8%) |
| Black or African American | 40/255 (15.7%) | 31/277 (11.2%) |
| Native Hawaiian or Other Pacific Islander | 1/255 (0.4%) | 0/277 (0.0%) |
| White | 186/255 (72.9%) | 218/277 (78.7%) |
| Other | 0/255 (0.0%) | 5/277 (1.8%) |
| Not Reported | 4/255 (1.6%) | 4/277 (1.4%) |
| Ethnicity n/N (%) | ||
| Not Hispanic or Latino | 203/255 (79.6%) | 226/277 (81.6%) |
| Hispanic or Latino | 50/255 (19.6%) | 50/277 (18.1%) |
| Not Reported | 2/255 (0.8%) | 1/277 (0.4%) |
| ADVIA Centaur | Beckman Access | Roche Elecsys | |||||
|---|---|---|---|---|---|---|---|
| AFC, Determined by Ultrasound | |||||||
| >15 | ≤15 | >15 | ≤15 | >15 | ≤15 | ||
| AMH result | >1.77 ng/mL | 250 | 123 | 249 | 125 | 214 | 74 |
| ≤1.77 ng/mL | 27 | 132 | 28 | 130 | 63 | 181 | |
| Total | 277 | 255 | 277 | 255 | 277 | 255 | |
| Sensitivity (95% CI) | 90.2% (86.2, 93.2) | 89.9% (85.8, 92.9) | 77.3% (72.0, 81.8) | ||||
| Specificity (95% CI) | 51.8% (45.6, 57.8) | 51.0% (44.9, 57.1) | 71.0% (65.1, 76.2) | ||||
| Positive Predictive Value (95% CI) | 67.0% (62.1, 71.6) | 66.6% (61.6, 71.2) | 74.3% (69.0, 79.0) | ||||
| Negative Predictive Value (95% CI) | 83.0% (76.4, 88.1) | 82.3% (75.6, 87.4) | 74.2% (68.3, 79.3) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bogdanovic, J.; Freeman, K.; Brown, C.; Singleton, R.; Behera, M.; O’Brien, J.E.; Zbella, E.; Christenson, R.H. Analytical Characteristics and Clinical Performance of Anti-Müllerian Hormone Immunoassay on the ADVIA Centaur® System: A Comparison with Other Chemiluminescent Methods. Endocrines 2024, 5, 516-528. https://doi.org/10.3390/endocrines5040037
Bogdanovic J, Freeman K, Brown C, Singleton R, Behera M, O’Brien JE, Zbella E, Christenson RH. Analytical Characteristics and Clinical Performance of Anti-Müllerian Hormone Immunoassay on the ADVIA Centaur® System: A Comparison with Other Chemiluminescent Methods. Endocrines. 2024; 5(4):516-528. https://doi.org/10.3390/endocrines5040037
Chicago/Turabian StyleBogdanovic, Jelena, Kaitlin Freeman, Chadwick Brown, Rachel Singleton, Millie Behera, Jeanne E. O’Brien, Edward Zbella, and Robert H. Christenson. 2024. "Analytical Characteristics and Clinical Performance of Anti-Müllerian Hormone Immunoassay on the ADVIA Centaur® System: A Comparison with Other Chemiluminescent Methods" Endocrines 5, no. 4: 516-528. https://doi.org/10.3390/endocrines5040037
APA StyleBogdanovic, J., Freeman, K., Brown, C., Singleton, R., Behera, M., O’Brien, J. E., Zbella, E., & Christenson, R. H. (2024). Analytical Characteristics and Clinical Performance of Anti-Müllerian Hormone Immunoassay on the ADVIA Centaur® System: A Comparison with Other Chemiluminescent Methods. Endocrines, 5(4), 516-528. https://doi.org/10.3390/endocrines5040037