
Does Testosterone Salvage PDE5i Non-Responders? A Scoping Review


Abstract
1. Introduction
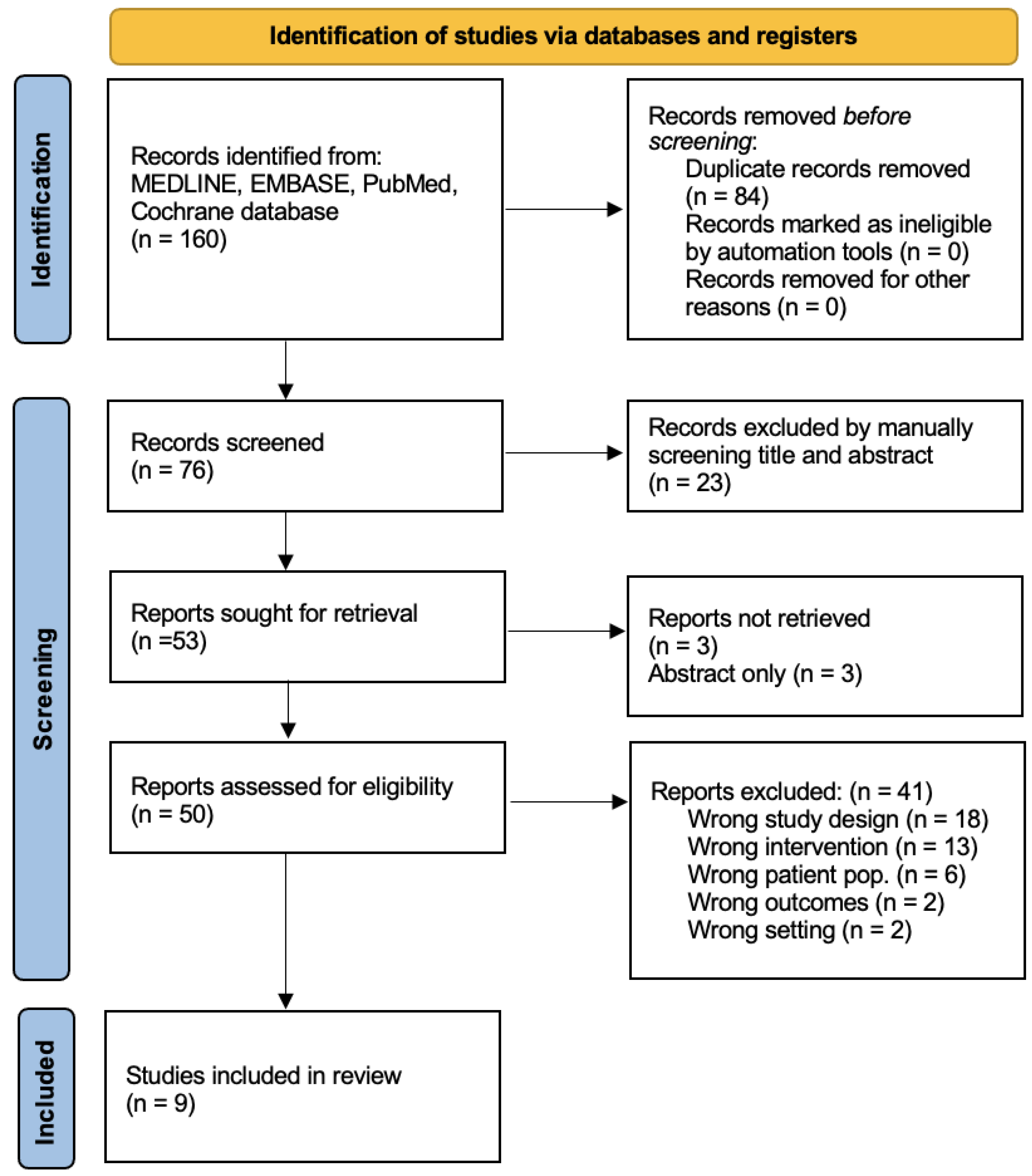
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Burnett, A.L.; Nehra, A.; Breau, R.H.; Culkin, D.J.; Faraday, M.M.; Hakim, L.S.; Heidelbaugh, J.; Khera, M.; McVary, K.T.; Miner, M.M.; et al. AUA Guideline ED. AUA Clin. Guidel. 2018, 1–36. [Google Scholar] [CrossRef]
- Feldman, H.A.; Goldstein, I.; Hatzichristou, D.G.; Krane, R.J.; McKinlay, J.B. Impotence and its medical and psychosocial correlates: Results of the Massachusetts Male Aging Study. J. Urol. 1994, 151, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Selvin, E.; Burnett, A.L.; Platz, E.A. Prevalence and Risk Factors for Erectile Dysfunction in the US. Am. J. Med. 2007, 120, 151–157. [Google Scholar] [CrossRef]
- Ayta, I.A.; McKinlay, J.B.; Krane, R.J. The likely worldwide increase in erectile dysfunction between 1995 and 2025: EBSCOhost. BJU Int. 1999, 84, 50–56. [Google Scholar] [CrossRef]
- Domes, T.; Najafabadi, B.T.; Roberts, M.; Campbell, J.; Flannigan, R.; Bach, P.; Patel, P.; Langille, G.; Krakowsky, Y.; Violette, P.D. CUA GUIDELINE Canadian Urological Association guideline: Erectile dysfunction. Can. Urol. Assoc. J. 2021, 15, 310. [Google Scholar] [CrossRef]
- Prieto, D. Physiological regulation of penile arteries and veins. Int. J. Impot. Res. 2008, 20, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, A.M.B.; Meehan, J.P.; Zakhary, R.; Buckley, P.A.; Rogers, F.A. New observations on microarchitecture of corpora cavernosa in man and possible relationship to mechanism of erection. Urology 1982, 20, 259–266. [Google Scholar] [CrossRef]
- Andersson, K.E. Mechanisms of penile erection and basis for pharmacological treatment of erectile dysfunction. Pharmacol. Rev. 2011, 63, 811–859. [Google Scholar] [CrossRef]
- Williams-Ashman, H.G. Enigmatic Features of Penile Development and Functions. Perspect. Biol. Med. 1990, 33, 335–374. [Google Scholar] [CrossRef]
- Burnett, A.L. Nitric Oxide in the Penis: Physiology and Pathology. J. Urol. 1997, 157, 320–324. [Google Scholar] [CrossRef]
- Burnett, A.; Musicki, B. The Nitric Oxide Signaling Pathway in the Penis. Curr. Pharm. Des. 2005, 11, 3987–3994. [Google Scholar] [CrossRef] [PubMed]
- Christ, G.; Richards, S.; Winkler, A. Integrative erectile biology: The role of signal transduction and cell-to-cell communication in coordinating corporal smooth muscle tone and penile erection. Int. J. Impot. Res. 1997, 9, 69–84. [Google Scholar] [CrossRef]
- Wingard, C.J.; Lewis, R.; Mills, T.M. Erection and NO override the vasoconstrictive effect of α-adrenergic stimulation in the rat penile vasculature. Int. J. Impot. Res. 2001, 13, 212–220. [Google Scholar] [CrossRef]
- Card, G.L.; England, B.P.; Suzuki, Y.; Fong, D.; Powell, B.; Lee, B.; Luu, C.; Tabrizizad, M.; Gillette, S.; Ibrahim, P.N.; et al. Structural Basis for the Activity of Drugs that Inhibit Phosphodiesterases. Structure 2004, 12, 2233–2247. [Google Scholar] [CrossRef]
- Corbin, J.D. Mechanisms of action of PDE5 inhibition in erectile dysfunction. Int. J. Impot. Res. 2004, 16 (Suppl. 1), S4–S7. [Google Scholar] [CrossRef]
- Giuliano, F.; Jackson, G.; Montorsi, F.; Martin-Morales, A.; Raillard, P. Safety of sildenafil citrate: Review of 67 double-blind placebo-controlled trials and the postmarketing safety database. Int. J. Clin. Pr. 2010, 64, 240–255. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, I.; Lue, T.F.; Padma-Nathan, H.; Rosen, R.C.; Steers, W.D.; Wicker, P.A. Oral sildenafil in the treatment of erectile dysfunction. Sildenafil Study Group. N. Engl. J. Med. 1998, 338, 1397–1404. [Google Scholar] [CrossRef] [PubMed]
- Hellstrom, W.J.G.; Gittelman, M.; Karlin, G.; Segerson, T.; Thibonnier, M.; Taylor, T.; Padma-Nathan, H. Vardenafil for treatment of men with erectile dysfunction: Efficacy and safety in a randomized, double-blind, placebo-controlled trial. J. Androl. 2002, 23, 763–771. [Google Scholar]
- Jung, J.; Choi, S.; Cho, S.H.; Ghim, J.L.; Hwang, A.; Kim, U.; Kim, B.S.; Koguchi, A.; Miyoshi, S.; Okabe, H.; et al. Tolerability and pharmacokinetics of avanafil, a phosphodiesterase type 5 inhibitor: A single- and multiple-dose, double-blind, randomized, placebo-controlled, dose-escalation study in healthy Korean male volunteers. Clin. Ther. 2010, 32, 1178–1187. [Google Scholar] [CrossRef]
- Madeira, C.R.; Tonin, F.S.; Fachi, M.M.; Borba, H.H.; Ferreira, V.L.; Leonart, L.P.; Bonetti, A.F.; Moritz, R.P.; Trindade, A.C.L.B.; Gonçalves, A.G.; et al. Efficacy and safety of oral phosphodiesterase 5 inhibitors for erectile dysfunction: A network meta-analysis and multicriteria decision analysis. World J. Urol. 2021, 39, 953–962. [Google Scholar] [CrossRef]
- Corona, G.; Rastrelli, G.; Burri, A.; Serra, E.; Gianfrilli, D.; Mannucci, E.; Jannini, E.A.; Maggi, M. First-generation phosphodiesterase type 5 inhibitors dropout: A comprehensive review and meta-analysis. Andrology 2016, 4, 1002–1009. [Google Scholar] [CrossRef]
- Alemany, M. The Roles of Androgens in Humans: Biology, Metabolic Regulation and Health. Int. J. Mol. Sci. 2022, 23, 11952. [Google Scholar] [CrossRef] [PubMed]
- Lugg, J.A.; Rajfer, J.; González-Cadavid, N.F. Dihydrotestosterone is the active androgen in the maintenance of nitric oxide-mediated penile erection in the rat. Endocrinology 1995, 136, 1495–1501. [Google Scholar] [CrossRef] [PubMed]
- Bhasin, S.; Brito, J.P.; Cunningham, G.R.; Hayes, F.J.; Hodis, H.N.; Matsumoto, A.M.; Snyder, P.J.; Swerdloff, R.S.; Wu, F.C.; Yialamas, M.A. Testosterone Therapy in Men with Hypogonadism: An Endocrine Society* Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2018, 103, 1715–1744. [Google Scholar] [CrossRef]
- Kandeel, F.R.; Koussa, V.K.T.; Swerdloff, R.S. Male Sexual Function and Its Disorders: Physiology, Pathophysiology, Clinical Investigation, and Treatment. Endocr. Rev. 2001, 22, 342–388. [Google Scholar] [CrossRef] [PubMed]
- Snyder, P.J.; Ellenberg, S.S.; Cunningham, G.R.; Alvin, M.; Farrar, J.T.; Cella, D.; Rosen, R.C.; Susan, M. The Testosterone Trials: The Design of Seven. Clin. Trials 2015, 11, 362–375. [Google Scholar] [CrossRef]
- Barone, B.; Napolitano, L.; Abate, M.; Cirillo, L.; Reccia, P.; Passaro, F.; Turco, C.; Morra, S.; Mastrangelo, F.; Scarpato, A.; et al. The Role of Testosterone in the Elderly: What Do We Know? Int. J. Mol. Sci. 2022, 23, 3535. [Google Scholar] [CrossRef]
- Mulhall, J.P.; Trost, L.W.; Brannigan, R.E.; Kurtz, E.G.; Redmon, J.B.; Chiles, K.A.; Lightner, D.J.; Miner, M.M.; Murad, M.H.; Nelson, C.J.; et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. J. Urol. 2018, 200, 423–432. [Google Scholar] [CrossRef]
- Jayasena, C.N.; Anderson, R.A.; Llahana, S.; Barth, J.H.; MacKenzie, F.; Wilkes, S.; Smith, N.; Sooriakumaran, P.; Minhas, S.; Wu, F.C.W.; et al. Society for Endocrinology guidelines for testosterone replacement therapy in male hypogonadism. Clin. Endocrinol. 2022, 96, 200–219. [Google Scholar] [CrossRef]
- Corona, G.; Goulis, D.G.; Huhtaniemi, I.; Zitzmann, M.; Toppari, J.; Forti, G.; Vanderschueren, D.; Wu, F.C.; Behre, H.; Punab, M.; et al. European Academy of Andrology (EAA) guidelines on investigation, treatment and monitoring of functional hypogonadism in males: Endorsing organization: European Society of Endocrinology. Andrology 2020, 8, 970–987. [Google Scholar] [CrossRef]
- Grober, E.D.; Krakowsky, Y.; Khera, M.; Holmes, D.T.; Lee, J.C.; Grantmyre, J.E.; Patel, P.; Bebb, R.A.; Fitzpatrick, R.; Campbell, J.D.; et al. Original Guideline Canadian Urological Association Guideline on Testosterone Deficiency in Men: Evidence-Based Q & A. Can. Urol. Assoc. J. 2021, 15, E234–E243. [Google Scholar] [CrossRef] [PubMed]
- Armagan, A.; Kim, N.N.; Goldstein, I.; Traish, A.M. Dose-Response Relationship Between Testosterone and Erectile Function: Evidence for the Existence of a Critical Threshold. J. Androl. 2006, 27, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Zitzmann, M.; Faber, S.; Nieschlag, E. Association of specific symptoms and metabolic risks with serum testosterone in older men. J. Clin. Endocrinol. Metab. 2006, 91, 4335–4343. [Google Scholar] [CrossRef] [PubMed]
- Park, K.; Ku, J.H.; Kim, S.W.; Paick, J.-S. Risk factors in predicting a poor response to sildenafil citrate in elderly men with erectile dysfunction. BJU Int. 2005, 95, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Mulhall, J.P.; Brock, G.B.; Glina, S.; Baygani, S.; Donatucci, C.; Maggi, M. Impact of Baseline Total Testosterone Level on Successful Treatment of Sexual Dysfunction in Men Taking Once-Daily Tadalafil 5 mg for LUTS/BPH: An Integrated Analysis of Three Randomized Trials. J. Sex. Med. 2016, 13, 843–851. [Google Scholar] [CrossRef]
- Kalinchenko, S.Y.; Kozlov, G.I.; Gontcharov, N.P.; Katsiya, G.V. Oral testosterone undecanoate reverses erectile dysfunction associated with diabetes mellitus in patients failing on sildenafil citrate therapy alone. Aging Male 2003, 6, 94–99. [Google Scholar] [CrossRef]
- Aversa, A.; Isidori, A.M.; Spera, G.; Lenzi, A.; Fabbri, A. Androgens improve cavernous vasodilation and response to sildenafil in patients with erectile dysfunction. Clin. Endocrinol. 2003, 58, 632–638. [Google Scholar] [CrossRef]
- Shabsigh, R.; Kaufman, J.M.; Steidle, C.; Padma-Nathan, H. Randomized study of testosterone gel as adjunctive therapy to sildenafil in hypogonadal men with erectile dysfunction who do not respond to sildenafil alone. J. Urol. 2004, 172, 658–663. [Google Scholar] [CrossRef]
- Shamloul, R.; Ghanem, H.; Fahmy, I.; El-Meleigy, A.; Ashoor, S.; Elnashaar, A.; Kamel, I. Testosterone Therapy Can Enhance Erectile Function Response to Sildenafil in Patients with PADAM: A Pilot Study. J. Sex. Med. 2005, 2, 559–564. [Google Scholar] [CrossRef]
- Hwang, T.-S.; Chen, H.-E.; Tsai, T.-F.; Lin, Y.C. Combined use of androgen and sildenafil for hypogonadal patients unresponsive to sildenafil alone. Int. J. Impot. Res. 2006, 18, 400–404. [Google Scholar] [CrossRef]
- Buvat, J.; Montorsi, F.; Maggi, M.; Porst, H.; Kaipia, A.; Colson, M.H.; Cuzin, B.; Moncada, I.; Martin-Morales, A.; Yassin, A.; et al. Hypogonadal Men Nonresponders to the PDE5 Inhibitor Tadalafil Benefit from Normalization of Testosterone Levels with a 1% Hydroalcoholic Testosterone Gel in the Treatment of Erectile Dysfunction (TADTEST Study). J. Sex. Med. 2011, 8, 284–293. [Google Scholar] [CrossRef]
- Garcia, J.A.; Sanchez, P.E.; Fraile, C.; Escovar, P. Testosterone undecanoate improves erectile dysfunction in hypogonadal men with the metabolic syndrome refractory to treatment with phosphodiesterase type 5 inhibitors alone. Andrologia 2011, 43, 293–296. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, M.; Basaria, S.; Travison, T.G.; Davda, M.N.; Paley, A.; Cohen, B.; Mazer, N.A.; Knapp, P.E.; Hanka, S.; Lakshman, K.M.; et al. Effect of Testosterone Replacement on Response to Sildenafil Citrate in Men with Erectile Dysfunction. Ann. Intern. Med. 2012, 157, 681–691. [Google Scholar] [CrossRef]
- Kim, J.W.; Oh, M.M.; Park, M.G.; Park, J.Y.; Bae, J.H.; Kim, J.J.; Moon, D.G. Combination therapy of testosterone enanthate and tadalafil on PDE5 inhibitor non-reponders with severe and intermediate testosterone deficiency. Int. J. Impot. Res. 2013, 25, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Baba, K.; Yajima, M.; Carrier, S.; Morgan, D.M.; Nunes, L.; Lue, T.F.; Iwamoto, T. Delayed testosterone replacement restores nitric oxide synthase-containing nerve fibres and the erectile response in rat penis. BJU Int. 2000, 85, 953–958. [Google Scholar] [CrossRef]
- Baba, K.; Yajima, M.; Carrier, S.; Akkus, E.; Reman, J.; Nunes, L.; Lue, T.F.; Iwamoto, T. Effect of testosterone on the number of NADPH diaphorase-stained nerve fibers in the rat corpus cavernosum and dorsal nerve. Urology 2000, 56, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Shabsigh, R. The effects of testosterone on the cavernous tissue and erectile function. World J. Urol. 1997, 15, 21–26. [Google Scholar] [CrossRef]
- Traish, A.M.; Goldstein, I.; Kim, N.N. Testosterone and Erectile Function: From Basic Research to a New Clinical Paradigm for Managing Men. Eur. Urol. 2008, 52, 54–70. [Google Scholar] [CrossRef]
- Morelli, A.; Filippi, S.; Mancina, R.; Luconi, M.; Vignozzi, L.; Marini, M.; Orlando, C.; Vannelli, G.B.; Aversa, A.; Natali, A.; et al. Androgens Regulate Phosphodiesterase Type 5 Expression and Functional Activity in Corpora Cavernosa. Endocrinology 2004, 145, 2253–2263. [Google Scholar] [CrossRef]
- Traish, A.M.; Park, K.; Dhir, V.; Kim, N.N.; Moreland, R.B.; Goldstein, I. Effects of Castration and Androgen Replacement on Erectile Function in a Rabbit Model. Endocrinology 1999, 140, 1861–1868. [Google Scholar] [CrossRef]
- Zhang, X.-H.; Morelli, A.; Luconi, M.; Vignozzi, L.; Filippi, S.; Marini, M.; Vannelli, G.B.; Mancina, R.; Forti, G.; Maggi, M. Testosterone Regulates PDE5 Expression and in vivo Responsiveness to Tadalafil in Rat Corpus Cavernosum. Eur. Urol. 2005, 47, 409–416. [Google Scholar] [CrossRef]
- Lee, D.S.; Sohn, D.W. The Role of Testosterone in Amplifying the Effect of a Phosphodiesterase Type 5 Inhibitor After Pelvic Irradiation. J. Sex. Med. 2020, 17, 1268–1279. [Google Scholar] [CrossRef]
- Manning, B.D.; Cantley, L.C. AKT/PKB Signaling: Navigating Downstream. Cell 2007, 129, 1261–1274. [Google Scholar] [CrossRef]
- Efesoy, O.; Çayan, S.; Akbay, E. The Effect of Testosterone Replacement Therapy on Penile Hemodynamics in Hypogonadal Men With Erectile Dysfunction, Having Veno-Occlusive Dysfunction. Am. J. Men’s Health 2018, 12, 634–638. [Google Scholar] [CrossRef]
- Yassin, A.A.; Saad, F.; Traish, A. Testosterone Undecanoate Restores Erectile Function in a Subset of Patients with Venous Leakage: A Series of Case Reports. J. Sex. Med. 2006, 3, 727–735. [Google Scholar] [CrossRef]
- Bella, A.J.; Lee, J.C.; Carrier, S.; Bénard, F.; Brock, G.B. 2015 CUA Practice guidelines for erectile dysfunction. Can. Urol. Assoc. J. 2015, 9, 23–29. [Google Scholar] [CrossRef]


{kind=link}
| Study, Year | n | Study Type, Country | Testosterone Formulation | PDE5i | Control | Duration of Treatment (Weeks) | Outcome Measure |
|---|---|---|---|---|---|---|---|
| * Kalinchenko 2003 [36] | 120 | Cohort, Russia | Oral testosterone undecanoate (120 mg/day) | Sildenafil (100 mg PRN) | 8 | IIEF | |
| * Aversa 2003 [37] | 20 | RCT, Italy | Transdermal patch (5 mg/day) | Sildenafil (100 mg PRN) | Placebo | 10 | IIEF |
| Shabsigh 2004 [38] | 75 | RCT, USA | 1% testosterone gel | Sildenafil (100 mg PRN) | Placebo | 14 | IIEF |
| Shamloul 2005 [39] | 40 | Prospective cohort, Egypt | Oral undecanoate (120 mg/day) | Sildenafil (50–100 mg PRN) | 12 | PADAM, IIEF | |
| Hwang 2006 [40] | 32 | Cohort, Taiwan | Oral undecanoate (160–240 mg/day) | Sildenafil (100 mg PRN) | 4 | IIEF | |
| Buvat 2011 [41] | 173 | Multi-centered RCT, European | 1% hydroalcoholic T gel (up to 10 mg) | Tadalafil (10 mg/day) | Placebo | 8 | IIEF |
| Garcia 2011 [42] | 29 | Cohort, Venezuela | Parenteral testosterone undecanoate (2 injections q6 weeks, followed by 12-weekly injections) | Unspecified | 102 | IIEF | |
| † Spitzer 2012 [43] | 140 | RCT, USA | 1% transdermal testosterone gel (10 g/day) | Sildenafil (25–100 mg PRN) | Placebo | 12 | IIEF |
| Kim 2013 [44] | 46 | Cohort, Korea | Parental testosterone enanthate q4 weeks | Tadalafil (5 mg/day) | 36 | IIEF |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pignanelli, M.; Stern, N.; Brock, G. Does Testosterone Salvage PDE5i Non-Responders? A Scoping Review. Endocrines 2023, 4, 117-127. https://doi.org/10.3390/endocrines4010011
Pignanelli M, Stern N, Brock G. Does Testosterone Salvage PDE5i Non-Responders? A Scoping Review. Endocrines. 2023; 4(1):117-127. https://doi.org/10.3390/endocrines4010011
Chicago/Turabian StylePignanelli, Mike, Noah Stern, and Gerald Brock. 2023. "Does Testosterone Salvage PDE5i Non-Responders? A Scoping Review" Endocrines 4, no. 1: 117-127. https://doi.org/10.3390/endocrines4010011
APA StylePignanelli, M., Stern, N., & Brock, G. (2023). Does Testosterone Salvage PDE5i Non-Responders? A Scoping Review. Endocrines, 4(1), 117-127. https://doi.org/10.3390/endocrines4010011