Abstract
Self-monitoring of blood glucose (SMBG) is common in patients with diabetes. The aim of this study was to explore how frequency/behavior of SMBG affect glucose control in patients with type 2 diabetes. This cross-sectional study was conducted at a regional teaching hospital in Taiwan. All participants completed a structured questionnaire about the frequency and behavior of SMBG, and hemoglobulin A1C (A1C) data were recorded from medical records. A total of 382 diabetes outpatients participated in the study. In the patients using insulin injections, A1C was better in patients with SMBG ≥ 28 times than in those with SMBG < 28 times per month (7.82 ± 1.86% vs. 8.33 ± 1.31%, p = 0.025). In the patients not using insulin, A1C was better in patients with SMBG > 14 times than those with SMBG ≤ 14 times per month (7.08 ± 0.23% vs. 7.55 ± 0.08%, p = 0.038). The patients who more frequently reviewed the causes of hypoglycemia and hyperglycemia had a better A1C level (p for linear trend <0.001). Our study suggested that SMBG ≥ 28 and >14 times could improve glycemic control for insulin-requiring and non-insulin-requiring type 2 diabetes patients, respectively. Further exploration of the cause of hyperglycemia or hypoglycemia shown by SMBG could also improve blood glucose control.
1. Introduction
Self-monitoring of blood glucose (SMBG) is an important component of self-management for persons with diabetes [1]. More frequent SMBG has been shown to reduce hemoglobulin A1C (A1C) [2,3] and acute complications [3] in patients with type 1 diabetes. Checking fasting glucose with SMBG to adjust basal insulin (intermediate-acting insulin, long or ultra-long-acting insulin analogs, once or twice per day) has been shown to result in lower A1C in patients with type 2 diabetes who use basal insulin with or without oral hypoglycemic agents (OHA) [4,5]. Checking SMBG once per week did not improve A1C in type 2 diabetic patients with insulin treatment [6], but more intensified checking SMBG—including before all meals and before sleep—will improve A1C in this group of patients [7]. However, routine SMBG has been reported to have limited benefits in patients with type 2 diabetes not using insulin [8,9,10,11]. Nevertheless, some studies have suggested that structured SMBG including data interpretation, feedback, and drug adjustment can reduce A1C in patients with type 2 diabetes without insulin treatment [12,13]; meta-analysis showed SMBG can reduce A1C in non-insulin treatment type 2 diabetes [13,14,15].
The aim of this study is to explore the behavior of SMBG in everyday clinical-practice patients with type 2 diabetes and to identify the optimal regimens, including timing, frequency, and behavior of SMBG for improving glycemic control.
2. Materials and Methods
This cross-sectional study was conducted at a regional teaching hospital in the Hsin-Chu area of Taiwan. We enrolled patients with type 2 diabetes who had been regularly followed at our Internal Medicine Department for longer than 1 year and visited our Endocrinology Outpatient Clinic with an odd-numbered appointment number on any outpatient day from 22 October 2010 to 15 November 2010. Exclusion criteria were as follows: (1) type 1 diabetes patients who had health insurance administration major injury card, (2) pancreatic disease or disease of exocrine pancreas, and (3) other type of diabetes other than type 1 and type 2 diabetes diagnosed by clinical doctors [16]. At enrollment, the participants filled out the questionnaires by themselves, and some cases were filled by study nurses after asking the participants. Questionnaires please to check at Supplement S1.
The study followed the tenets of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards, and the study was approved by the Institutional Review Board of National Taiwan University Hospital, Hsin-Chu Branch.
The self-designed structured questionnaire [17] (Supplement S1) was used to collect data on age; gender; duration of diabetes; education; annual income; self-care ability; type of treatment; the experience of hypoglycemia; behavior of SMBG (including frequency, timing, whether the results were recorded on a piece of paper or book); and whether the patient reviewed the reason for hypoglycemia (blood glucose < 70 mg/day) or hyperglycemia (pre-prandial blood glucose > 130 or postprandial blood glucose > 180) [18] according to the results of SMBG, adjusted their medication according to the results of SMBG, gave the results of SMBG to medical personnel, and compared both SMBG and laboratory-measured fasting blood glucose levels measured simultaneously [19] at an annual check-up [20]. The questions about behavior related to SMBG and blood glucose control were restricted to patients who had performed SMBG in the past 1 month [21]. The questions were designed with reference to the suggestions of guideline [22]. The tool was validated by a pilot study. The intensity of the behaviors was assessed using a 5-point Likert scale as follows: almost never (<20%), less than half of the time (20–40%), about half of the time (40–60%), most of the time (60–80%), usually (>80%) (Supplement S1).
Potential answer to the frequency of SMBG were as follows: (1) Never, (2) 1/month, (3) 2–4/month, (4) 5–14/month, (5) >14/month, and Please fill in the number of times. (Supplement S1) Subgroups analyses were also conducted for whether persons received insulin injections or not. We collected A1C values from medical chart on the same day of answering the questionnaire to assess blood sugar control. A1C data was within 3 months prior to answering the questionnaire and was measured using high-performance liquid chromatography (Primus Ultra 2, Trinity Biotech, Bray, County Wicklow, Ireland). Patients who refused to be interviewed or did not have A1C data in the recent 3 months were excluded.Wicklow, Ireland). Patients who refused to be interviewed or did not have A1C data in the recent 3 months were excluded.
Statistical Analysis
The content validity index was calculated to evaluate the validity of the questionnaire with regards to the behavior of SMBG, and Cronbach’s alpha was calculated to evaluate the internal consistency [23]. Continuous variables were expressed as mean ± standard deviation (SD), and categorical variables were expressed as number or percentage. Continuous distribution was evaluated using the Shapiro–Wilk test and Kolmogorov–Smirnov test [24]. Demographic, clinical, and A1C data of the patients were compared using the independent t-test or Mann–Whitney U test for continuous variables, whilst using the chi-squared test or Fisher’s exact test for categorical variables. Correlations among variables were calculated using one-way ANOVA and linear trend analysis. A p value < 5% was regarded as being statistically significant. All statistical analyses were performed using IBM SPSS statistical software for Windows (Version 20.0; IBM Corp., Armonk, NY, USA).
3. Results
A total of 386 patients with type 2 diabetes were enrolled in this study. We excluded four cases without A1C data (all data are shown at Supplement S2). All content validity index values were 1 for the questions on behavior, and Cronbach’s alpha was 0.672. After deleting the question about drug adjustments according to the results of SMBG, Cronbach’s alpha was 0.712. The clinical characteristics of the included patients are shown in Table 1.

Table 1.
Clinical characteristics and laboratory data stratified by insulin treatment and no insulin treatment.
About one third of the patients did not check SMBG, and 45.0% of the patients had checked SMBG ≥ 5 times in the past 1 month (Table 2). Most of the patients checked SMBG before and after breakfast (Table 2). Only 0.4% of the patients checked SMBG 7 times a day (Table 2). The frequencies of behavior of SMBG in the past 1 month are shown in Table 3.
Table 2.
Frequency and time of SMBG in the past 1 month.
Table 3.
Behavior of SMBG restricted to patients who checked SMBG in the past 1 month (n = 249).
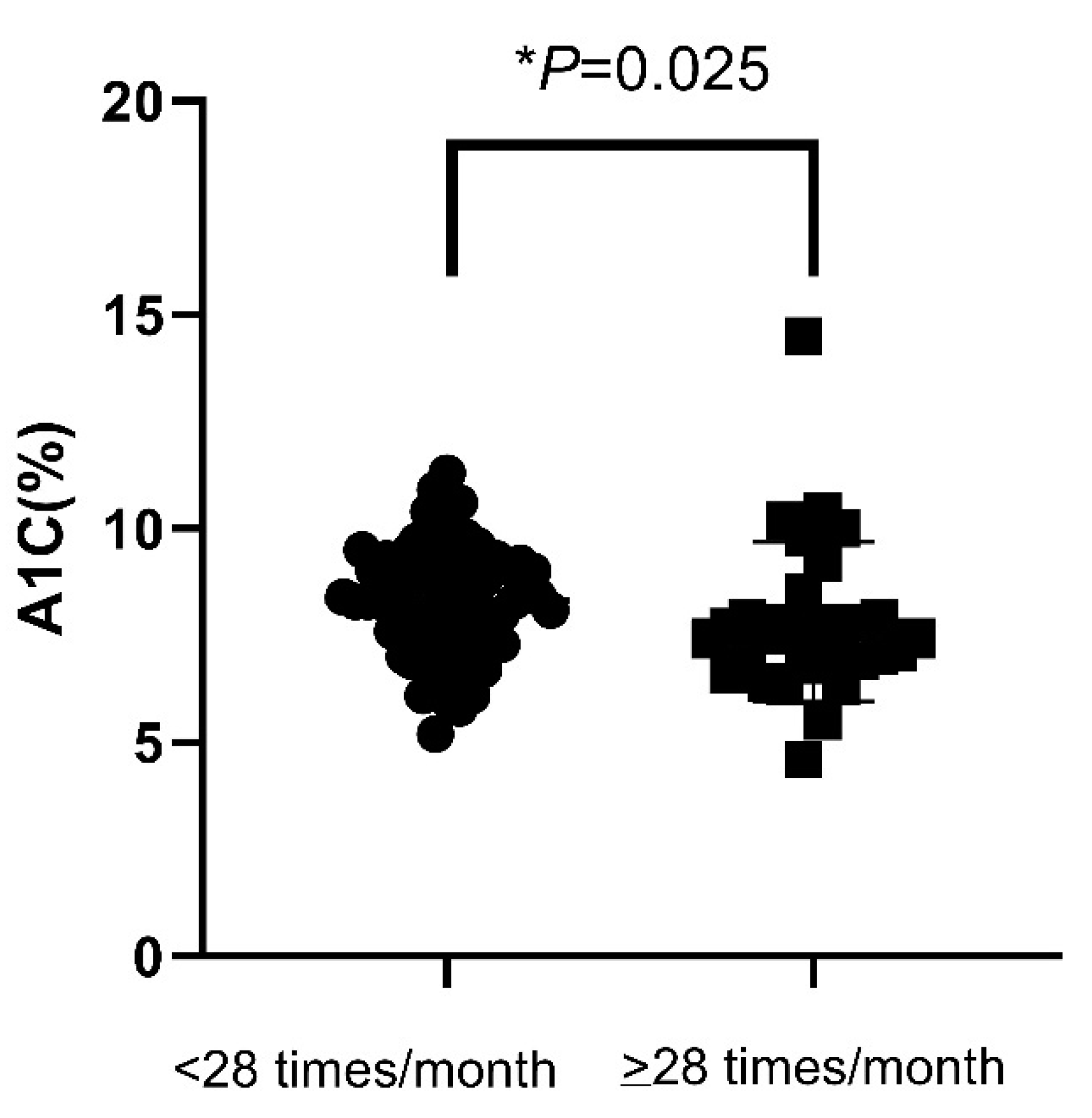
In all patients included, there were no significant difference in mean A1C values between patients with SMBG ≤ 14 and SMBG > 14 per month (7.68 ± 0.08% vs. 7.56 ± 0.20%, p = 0.256). The mean A1C levels were also not different between patients with SMBG < 28 and SMBG ≥ 28 per month (7.68 ± 1.33% vs. 7.47 ± 1.69%, p = 0.163). The percentage of hypoglycemia were also not statistically different between patients with SMBG ≤ 14 and SMBG > 14 per month (9.84% vs. 14.93%, p = 0.222), nor between patients with SMBG < 28 and SMBG ≥ 28 per month (9.74% vs. 16.28%, p = 0.199). Nevertheless, in patients requiring insulin injections, the mean A1C values in patients with SMBG ≥ 28 per month were significantly lower than patients with SMBG < 28 per month (7.82 ± 1.86% vs. 8.33 ± 1.31%, p = 0.025) (Figure 1). However, the percentage of patients who achieved A1C < 7% were not statistically different for patients with SMBG < 28 compared to those with SMBG ≥ 28 per month (p = 0.107). The percentage of hypoglycemia was also not statistically different for patients with SMBG < 28 compared to those with SMBG ≥ 28 per month (p = 0.973). The clinical characteristics and laboratory data including age, gender, duration of diabetes, retinopathy, nephropathy, neuropathy, cardiovascular disease, and stroke were not significantly different between these two groups of patients.
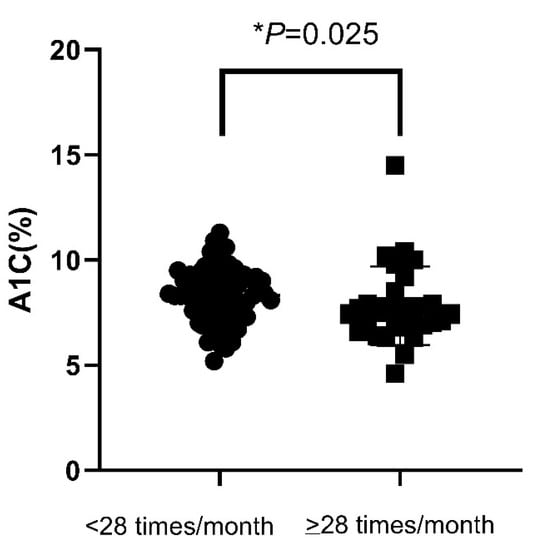
Figure 1.
A1C value in insulin-treated patients according to the frequency of SMBG (<28 or ≥28 measurements a month). A1C—hemoglobin A1C; SMBG—self-monitoring of blood glucose. * p < 0.05.
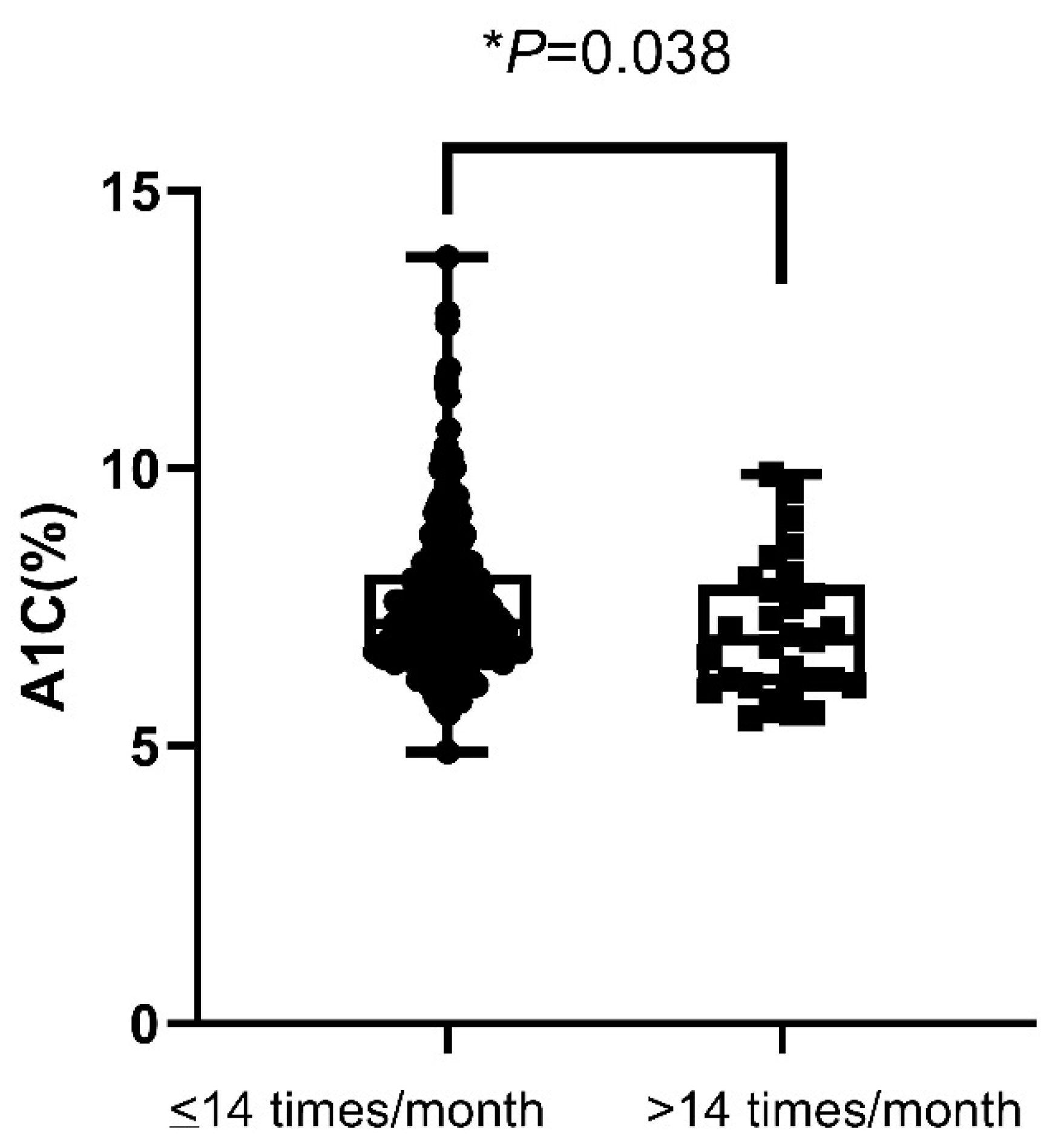
In non-insulin-requiring patients, the mean A1C values in patients with SMBG > 14 per month were significantly lower than patients with SMBG ≤ 14 per month (7.08 ± 0.23 vs. 7.55 ± 0.08%, p = 0.038) (Figure 2). However, the percentages of hypoglycemia and patients who achieved A1C < 7% were not significant in patients with SMBG > 14 compared to those with SMBG ≤ 14 per month (p = 0.705, p = 0.207, respectively). The duration of diabetes was longer in patients with SMBG > 14 (15.01 ± 9.70 years) as compared to patients with SMBG ≤ 14 (11.61 ± 8.65 years) (p = 0.017). The percentage of retinopathy was higher in patients with SMBG > 14 (24.1%) as compared to patients with SMBG ≤ 14 (9.2%) (p = 0.023). Age, gender, nephropathy, neuropathy, cardiovascular disease, and stroke were not significantly different between these two groups of patients.
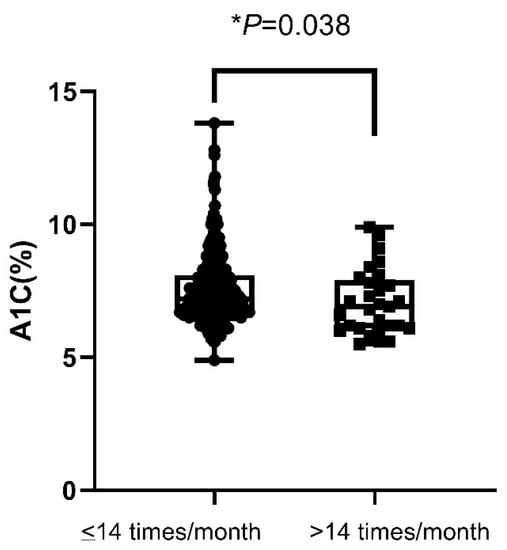
Figure 2.
A1C value in non-insulin-treated patients according to the frequency of SMBG (≤14 or >14 measurements a month). A1C—hemoglobin A1C; SMBG—self-monitoring of blood glucose. * p < 0.05.
Regarding the SMBG-related behaviors, the patients who reviewed the reasons for hypoglycemia and hyperglycemia more frequently had better A1C (one-way ANOVA and linear trend analysis, p < 0.001) (Table 4). However, the behavior of recording the results on a piece of paper or book, adjusting the drugs according to the results of SMBG, giving the results of SMBG to medical personnel, and comparing the results to laboratory-measured fasting plasma glucose did not significantly affect A1C (one-way ANOVA and linear trend analysis, p values 0.284, 0.099, 0.375, and 0.908, respectively) (Table 4).
Table 4.
Behavior of SMBG restricted to patients who checked SMBG in the past 1 month (n = 249).
4. Discussion
In this cross-sectional study about SMBG in type 2 diabetes persons with treatment longer than 1 year, we found that in the group who used insulin injections, A1C was better when they checked SMBG ≥ 28 times a month, but it was better for >14 times a month in persons without insulin injection. In addition, the patients who more frequently reviewed the causes of hypoglycemia and hyperglycemia also had better A1C levels.
The Cronbach’s alpha of the questions on behavior in this study was 0.672. This may be because we included some patients who controlled their diet or received OHA for diabetes. These patients usually do not change the number or type of drugs. After deleting the question about adjusting the drugs according to the results of SMBG, Cronbach’s alpha increased to 0.712.
There is currently no consensus on the frequency of SMBG for all diabetic persons in American Diabetic Association and International Diabetes Federation; it should be individualized depending on the patient’s condition, but checking fasting glucose in patients using basal insulin was suggested [1,25]. According to the recommendation of Diabetes Canada, type 2 diabetic patients with lifestyle control, oral hypoglycemic agent treatment, and meeting the glycemic targets should check SMBG 1–2 times per week, otherwise checking SMBG 1–2 times per day; type 2 diabetic patients with insulin injection at least should check SMBG before insulin injection [26]. So, we choose the cut-off point of 14 times/month in the non-insulin treatment group and 28 times/month in the insulin treatment group. Previous reports showed that SMBG improved A1C in those who used insulin injections, but not in those who did not use insulin [1,2,3,7,8,9,10,11,27]. However, meta-analyses have reported that A1C can be reduced by 0.25–0.3% by SMBG in persons with type 2 diabetes without insulin treatment [13,14,15]; nonetheless, this effect was decreased after 1 year [14]. Our data showed that SMBG ≥ 28 times a month as recommendation improved A1C in type 2 diabetes persons who used insulin injections. We also found that SMBG > 14 times a month improved A1C in non-insulin-requiring type 2 diabetes persons even after treatment longer than 1 year and worse condition.
The presence of hypoglycemia was not significantly different between the groups divided by any points in this study, which is consistent with a previous report [11].
According to the recommendations of the American Diabetes Association, patients with insulin treatment should check SMBG when fasting, before meals and snacks, at bedtime, before exercise, or when hypoglycemia is suspected [1]. Our patients preferred to check SMBG before and after breakfast, although some did not use insulin injections.
Structured SMBG involves specifically defined timing and frequency of SMBG [12,13], food intake, physical activity, and possibly taking notes on SMBG [12]. Structured SMBG may give insights into the profile of blood sugar during a day, relationships between food and physical activity, and other effects on blood sugar. Structured SMBG has been shown to be more efficient in reducing A1C than ordinary SMBG [12,13], which may be because SMBG alone may not reduce blood glucose levels [1]. Measuring fasting glucose level using SMBG with dose adjustments to a target level has been shown to result in better A1C control in patients using basal insulin treatment [4,5]. Most of our patients reviewed the reason for hypoglycemia or hyperglycemia according to the results of SMBG, while few adjusted the drugs according to the results of SMBG (Table 3). Our results showed that the patients who analyzed the data of hyperglycemia and hypoglycemia more often had better A1C control. This result is consistent with reports of structured SMBG [12,13]. Adjusting the drugs did not reduce A1C in our study. This may be because only a few patients did this, and some of our patients did not receive insulin treatment. Reviewing the reasons for hypoglycemia and hyperglycemia is easier than using structured SMBG, so we emphasized the importance of how to interpret abnormal SMBG data by persons with Diabetes.
More frequently checking SMBG did not improve A1C control in all persons with diabetes in previous 2 studies [28,29], but it correlated with reduced A1C in one randomized control study in type 2 diabetes [30] and improved A1C if SMBG 8–14 times/week in one meta-analysis in type 2 diabetes persons without insulin treatment [31]. We did not find SMBG more frequently and better A1C control in all our type 2 diabetic persons, but in subgroup analysis, SMBG ≥ 28 times a month improved A1C in the insulin treatment group, and SMBG > 14 times a month improved A1C in the non-insulin-requiring group.
There are several limitations to this study. First, the treatment of the patients was heterogeneous. Second, it was hard to collect the exact frequency of SMBG; the division of frequency is done with rough estimation. These factors may limit the interpretation of the results. Larger scale of single treatment and well-designed, studies are warranted to verify the results of this study and define the optimal time and frequency of SMBG in type 2 diabetes persons.
5. Conclusions
This study showed that among type 2 diabetes patients treated with insulin injection, those who performed SMBG ≥ 28 times per month had better glucose control, with SMBG > 14 times per month in non-insulin-requiring patients. In addition, the patients who more frequently reviewed the reasons for hypoglycemia and hyperglycemia also had a lower A1C.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/endocrines3020019/s1. Supplementary File S1: The Study Questionnaire; Supplementary File S2: The data presented in this study.
Author Contributions
Conceptualization, C.L. and P.-Y.C.; methodology, C.L. and P.-Y.C.; validation, C.L.; formal analysis, C.L.; investigation, C.L.; resources, C.L. and H.-J.Y.; data curation, C.L.; writing—original draft preparation, C.L. and P.-Y.C.; writing—review and editing, C.-H.T., K.C.-W.L. and M.-D.P.; visualization, C.L. and M.-D.P.; supervision, M.-D.P.; project administration, C.L.; funding acquisition, C.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by National Taiwan University Hospital Hsin-Chu Branch, grant number 2-990007.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and was approved by the Institutional Review Board of National Taiwan University Hospital, Hsin-Chu Branch. (Protocol code HCGH99F005, 21 August 2010).
Informed Consent Statement
Patient consent was waived due to no identity data being collected.
Data Availability Statement
The data presented in this study are available in Supplementary File S2.
Acknowledgments
We thank the staff of Department of Medical Research, National Taiwan University Hospital, Hsin-Chu Branch for their assistance in statistical analysis and providing careful review and insightful comments regarding the manuscript. Yi-Cheng Chang for technology instructions. Kuei-Miao Kuo for assistance to complete the questionnaire.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- American Diabetes Association. 7. Diabetes Technology: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S85–S99. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.M.; Beck, R.W.; Bergenstal, R.M.; Goland, R.S.; Haller, M.J.; McGill, J.B.; Rodriguez, H.; Simmons, J.H.; Hirsch, I.B. Evidence of a strong association between frequency of self-monitoring of blood glucose and hemoglobin A1c levels in T1D exchange clinic registry participants. Diabetes Care 2013, 36, 2009–2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziegler, R.; Heidtmann, B.; Hilgard, D.; Hofer, S.; Rosenbauer, J.; Holl, R. Frequency of SMBG correlates with HbA1c and acute complications in children and adolescents with type 1 diabetes. Pediatric Diabetes 2011, 12, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, J.; Davies, M.; Home, P.D.; Larsen, J.; Koenen, C.; Schernthaner, G. A randomised, 52-week, treat-to-target trial comparing insulin detemir with insulin glargine when administered as add-on to glucose-lowering drugs in insulin-naive people with type 2 diabetes. Diabetologia 2008, 51, 408–416. [Google Scholar] [CrossRef] [Green Version]
- Garber, A.J. Treat-to-target trials: Uses, interpretation and review of concepts. Diabetes Obes. Metab. 2014, 16, 193–205. [Google Scholar] [CrossRef] [Green Version]
- Nauck, M.A.; Haastert, B.; Trautner, C.; Müller, U.A.; Nauck, M.A.; Heinemann, L. A randomised, controlled trial of self-monitoring of blood glucose in patients with type 2 diabetes receiving conventional insulin treatment. Diabetologia 2014, 57, 868–877. [Google Scholar] [CrossRef]
- Murata, G.H.; Shah, J.H.; Hoffman, R.M.; Wendel, C.S.; Adam, K.D.; Solvas, P.A.; Bokhari, S.U.; Duckworth, W.C. Intensified blood glucose monitoring improves glycemic control in stable, insulin-treated veterans with type 2 diabetes: The Diabetes Outcomes in Veterans Study (DOVES). Diabetes Care 2003, 26, 1759–1763. [Google Scholar] [CrossRef] [Green Version]
- Farmer, A.; Wade, A.; Goyder, E.; Yudkin, P.; French, D.; Craven, A.; Holman, R.; Kinmonth, A.L.; Neil, A. Impact of self monitoring of blood glucose in the management of patients with non-insulin treated diabetes: Open parallel group randomised trial. BMJ (Clin. Res. Ed.) 2007, 335, 132. [Google Scholar] [CrossRef] [Green Version]
- O’Kane, M.J.; Bunting, B.; Copeland, M.; Coates, V.E. Efficacy of self monitoring of blood glucose in patients with newly diagnosed type 2 diabetes (ESMON study): Randomised controlled trial. BMJ 2008, 336, 1174–1177. [Google Scholar] [CrossRef] [Green Version]
- Simon, J.; Gray, A.; Clarke, P.; Wade, A.; Neil, A.; Farmer, A. Cost effectiveness of self monitoring of blood glucose in patients with non-insulin treated type 2 diabetes: Economic evaluation of data from the DiGEM trial. BMJ 2008, 336, 1177–1180. [Google Scholar] [CrossRef] [Green Version]
- Young, L.A.; Buse, J.B.; Weaver, M.A.; Vu, M.B.; Mitchell, C.M.; Blakeney, T.; Grimm, K.; Rees, J.; Niblock, F.; Donahue, K.E. Glucose Self-monitoring in Non-Insulin-Treated Patients With Type 2 Diabetes in Primary Care Settings: A Randomized Trial. JAMA Intern. Med. 2017, 177, 920–929. [Google Scholar] [CrossRef] [PubMed]
- Polonsky, W.H.; Fisher, L.; Schikman, C.H.; Hinnen, D.A.; Parkin, C.G.; Jelsovsky, Z.; Petersen, B.; Schweitzer, M.; Wagner, R.S. Structured self-monitoring of blood glucose significantly reduces A1C levels in poorly controlled, noninsulin-treated type 2 diabetes: Results from the Structured Testing Program study. Diabetes Care 2011, 34, 262–267. [Google Scholar] [CrossRef] [Green Version]
- Mannucci, E.; Antenore, A.; Giorgino, F.; Scavini, M. Effects of Structured Versus Unstructured Self-Monitoring of Blood Glucose on Glucose Control in Patients With Non-insulin-treated Type 2 Diabetes: A Meta-Analysis of Randomized Controlled Trials. J. Diabetes Sci. Technol. 2018, 12, 183–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malanda, U.L.; Welschen, L.M.C.; Riphagen, I.I.; Dekker, J.M.; Nijpels, G.; Bot, S.D.M. Self-monitoring of blood glucose in patients with type 2 diabetes mellitus who are not using insulin. Cochrane Database Syst. Rev. 2012, 1, CD005060. [Google Scholar] [CrossRef] [Green Version]
- Willett, L.R.; ACP Journal Club. Meta-analysis: Self-monitoring in non-insulin-treated type 2 diabetes improved HbA1c by 0.25%. Ann. Intern. Med. 2012, 156, Jc6-12. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2022. Diabetes Care 2021, 45, S17–S38. [Google Scholar] [CrossRef]
- Cheung, A.K.L. Structured Questionnaires. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 6399–6402. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee 6. Glycemic Targets: Standards of Medical Care in Diabetes—2022. Diabetes Care 2021, 45, S83–S96. [Google Scholar] [CrossRef]
- Blood Glucose Monitoring Devices. Available online: https://www.fda.gov/medical-devices/in-vitro-diagnostics/blood-glucose-monitoring-devices (accessed on 24 March 2022).
- Cheng, A.Y. Canadian Diabetes Association 2013 clinical practice guidelines for the prevention and management of diabetes in Canada. Introduction. Can. J. Diabetes 2013, 37 (Suppl. 1), S1–S3. [Google Scholar] [CrossRef] [Green Version]
- Gryczynski, J.; Nordeck, C.; Mitchell, S.G.; O’Grady, K.E.; McNeely, J.; Wu, L.T.; Schwartz, R.P. Reference periods in retrospective behavioral self-report: A qualitative investigation. Am. J. Addict. 2015, 24, 744–747. [Google Scholar] [CrossRef] [Green Version]
- Association, A.D. Standards of Medical Care in Diabetes—2010. Diabetes Care 2010, 33, S11–S61. [Google Scholar] [CrossRef] [Green Version]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Ghasemi, A.; Zahediasl, S. Normality tests for statistical analysis: A guide for non-statisticians. Int. J. Endocrinol. Metab. 2012, 10, 486–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guidelines: Self-Monitoring of Blood Glucose in Non-Insulin Treated Type 2 Diabetes. Available online: https://www.idf.org/e-library/guidelines/85-self-monitoring-of-blood-glucose-in-non-insulin-treated-type-2-diabetes.html (accessed on 23 January 2022).
- Self-Monitoring Blood Glucose (SMBG) Frequency & Pattern Tool. Available online: https://guidelines.diabetes.ca/self-management/smbg-tool (accessed on 23 January 2022).
- Nathan, D.M.; Genuth, S.; Lachin, J.; Cleary, P.; Crofford, O.; Davis, M.; Rand, L.; Siebert, C. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N. Engl. J. Med. 1993, 329, 977–986. [Google Scholar] [CrossRef] [PubMed]
- Wambui Charity, K.; Kumar, A.M.V.; Hinderaker, S.G.; Chinnakali, P.; Pastakia, S.D.; Kamano, J. Do diabetes mellitus patients adhere to self-monitoring of blood glucose (SMBG) and is this associated with glycemic control? Experiences from a SMBG program in western Kenya. Diabetes Res. Clin. Pract. 2016, 112, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Iwuala, S.O.; Olamoyegun, M.A.; Sabir, A.A.; Fasanmade, O.A. The relationship between self-monitoring of blood glucose and glycaemic control among patients attending an urban diabetes clinic in Nigeria. Ann. Afr. Med. 2015, 14, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Levine, J.C.; Burns, E.; Whittle, J.; Fleming, R.; Knudson, P.; Flax, S.; Leventhal, H. Randomized trial of technology-assisted self-monitoring of blood glucose by low-income seniors: Improved glycemic control in type 2 diabetes mellitus. J. Behav. Med. 2016, 39, 1001–1008. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Tan, D.H.Y.; Lee, J.Y. Evaluating the impact of self-monitoring of blood glucose frequencies on glucose control in patients with type 2 diabetes who do not use insulin: A systematic review and meta-analysis. Int. J. Clin. Pract. 2019, 73, e13357. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).