
HSCT with Mismatched Unrelated Donors (MMUD): A Comparison of Different Platforms for GvHD Prophylaxis

 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Patients and Methods
2.1. HLA Typing
2.2. Engraftment and GvHD Prophylaxis
2.3. Statistical Analysis
3. Results
3.1. Disease Risk Index and EBMT Risk Score
3.2. HLA Typing
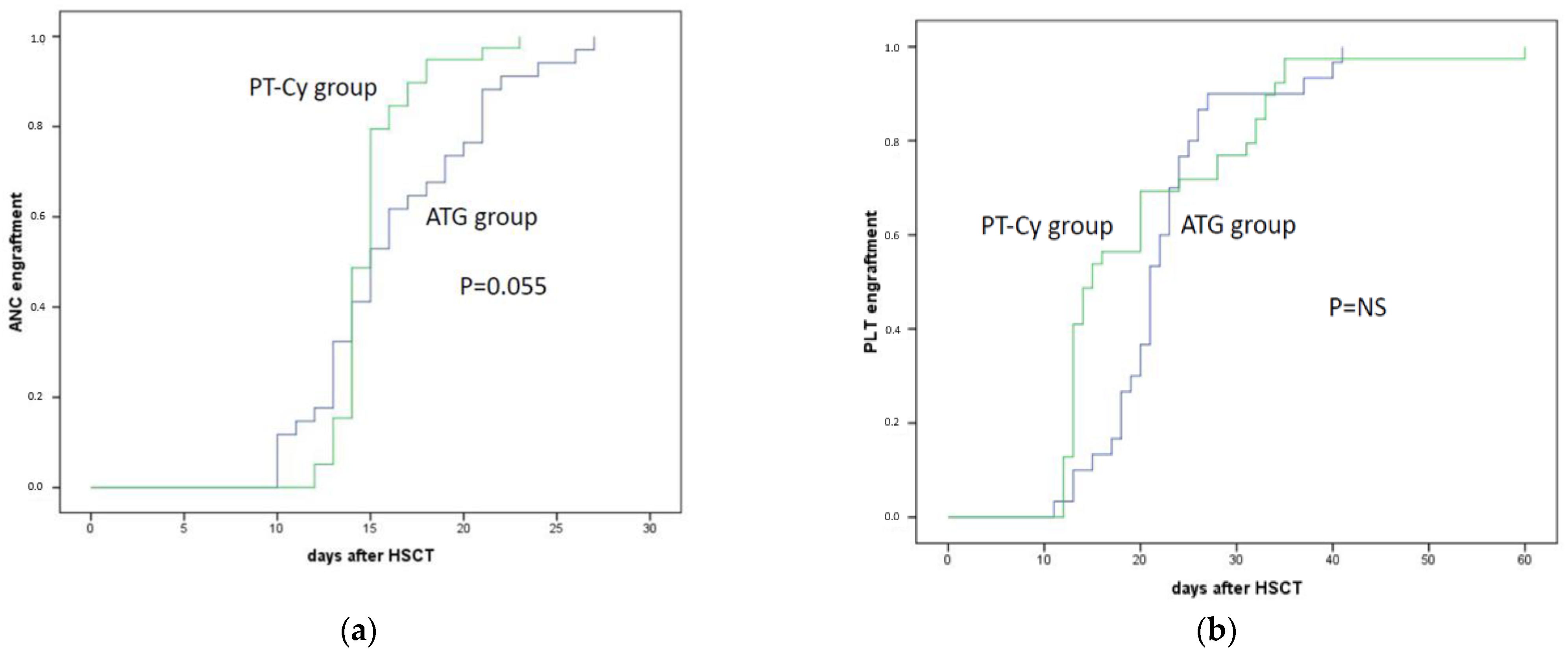
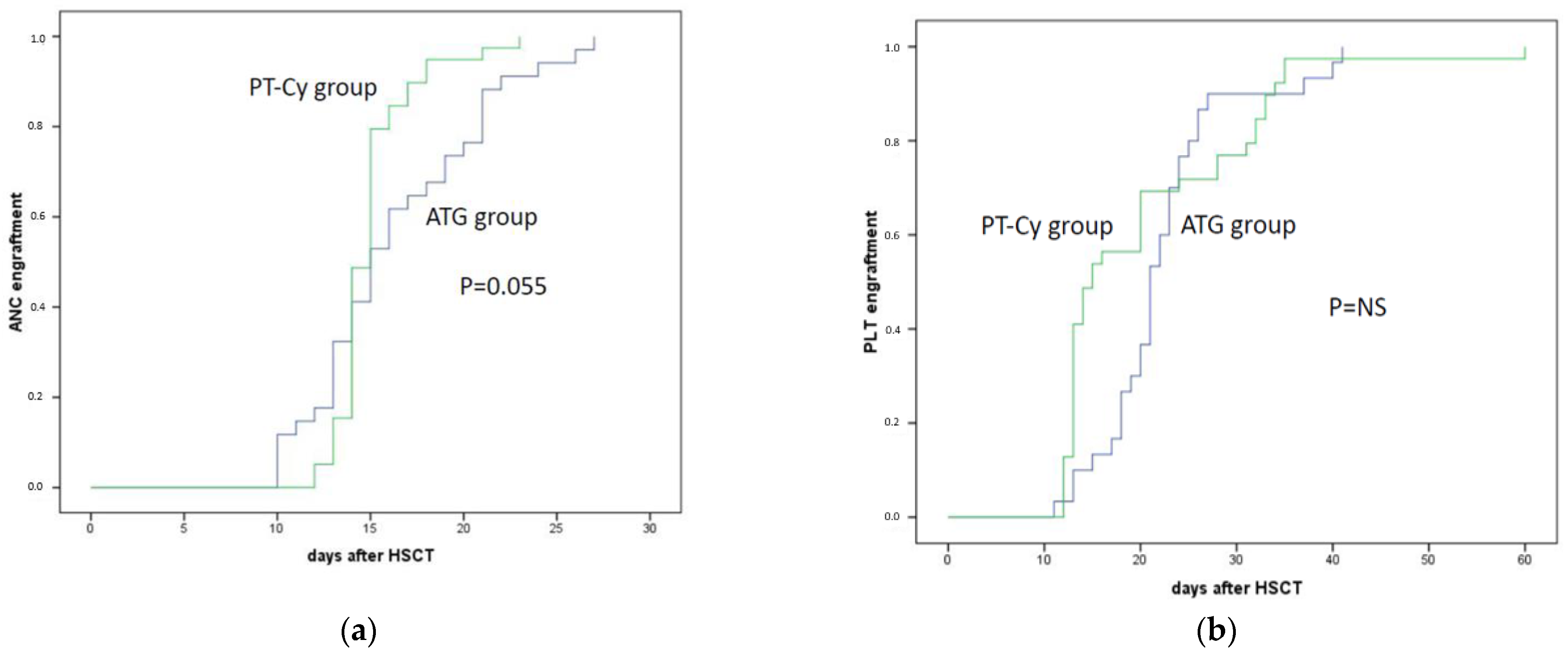
3.3. Neutrophils and Platelet Engraftment
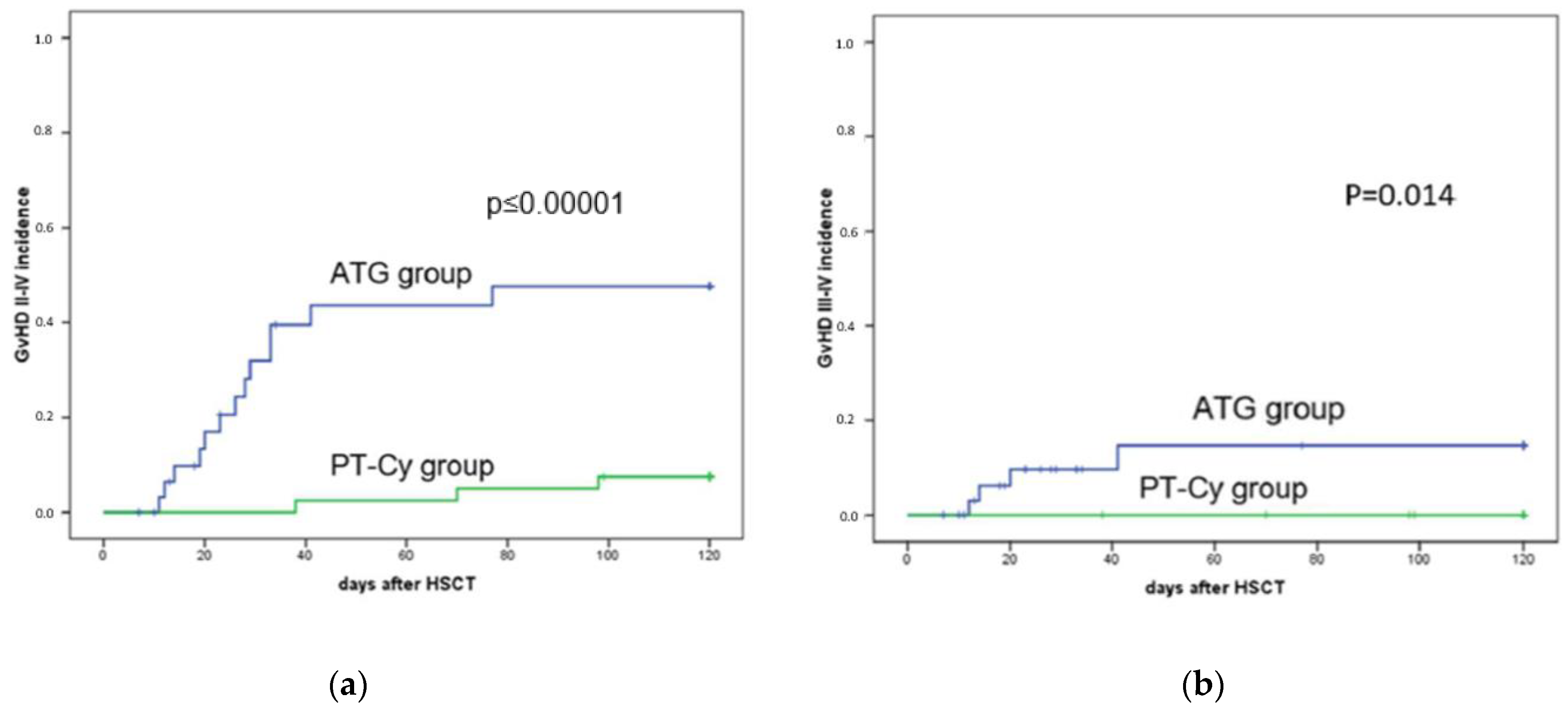
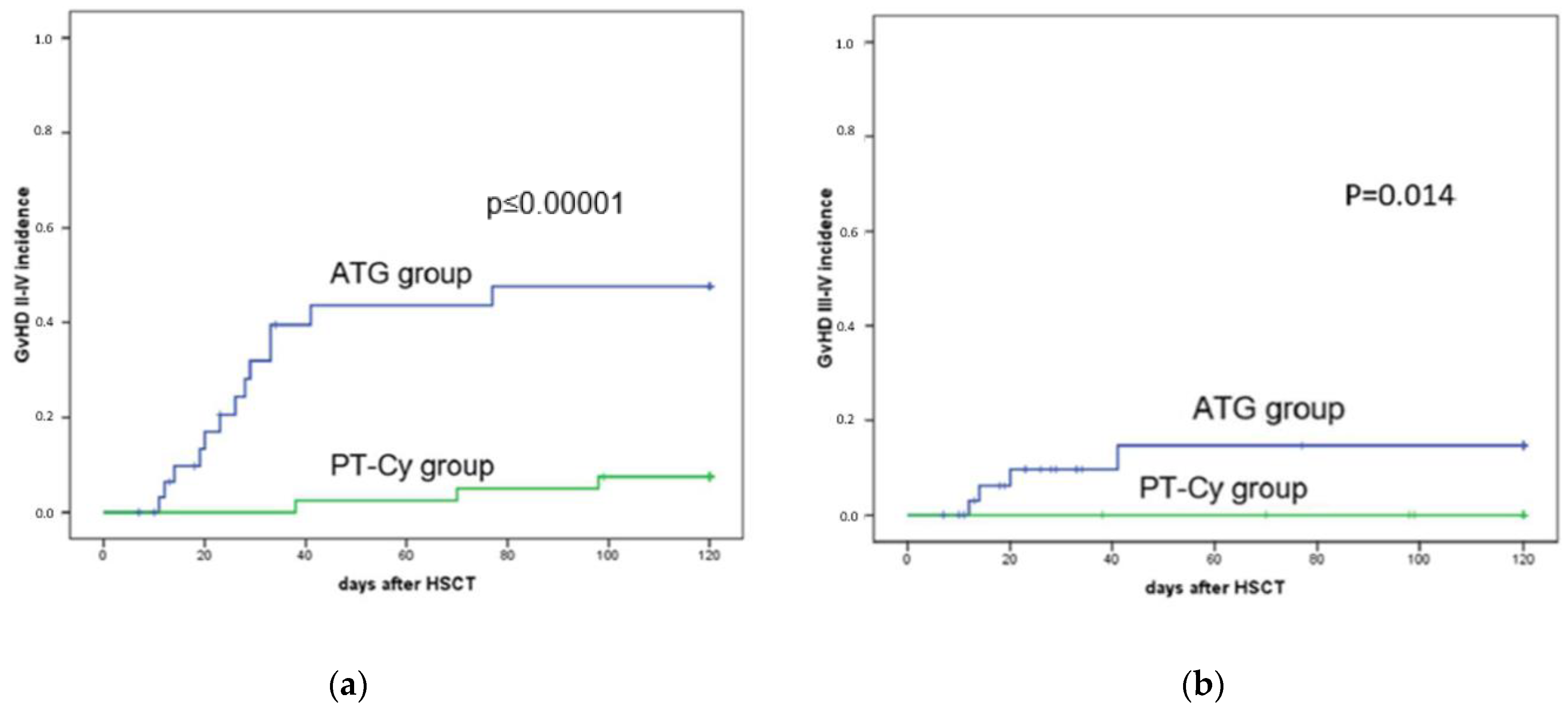
3.4. Acute GvHD
3.5. Chronic GvHD Incidence
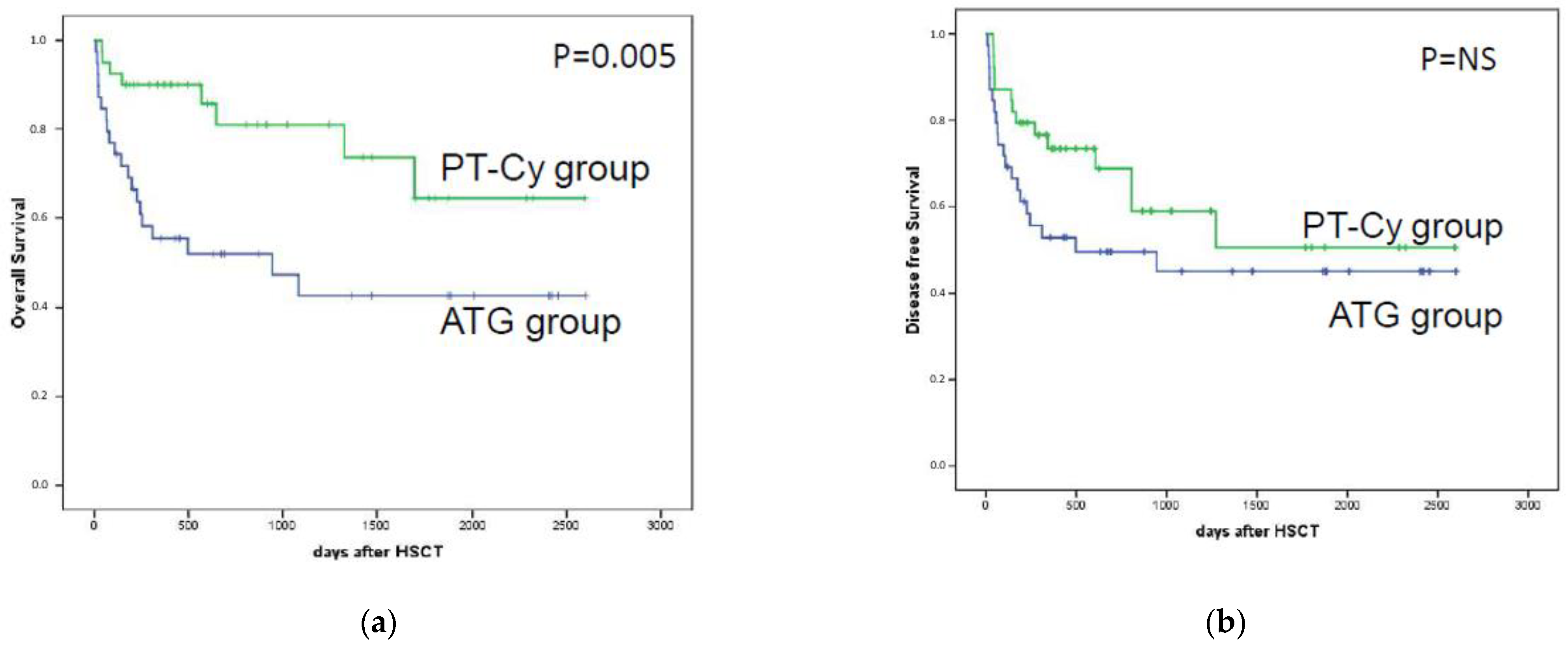
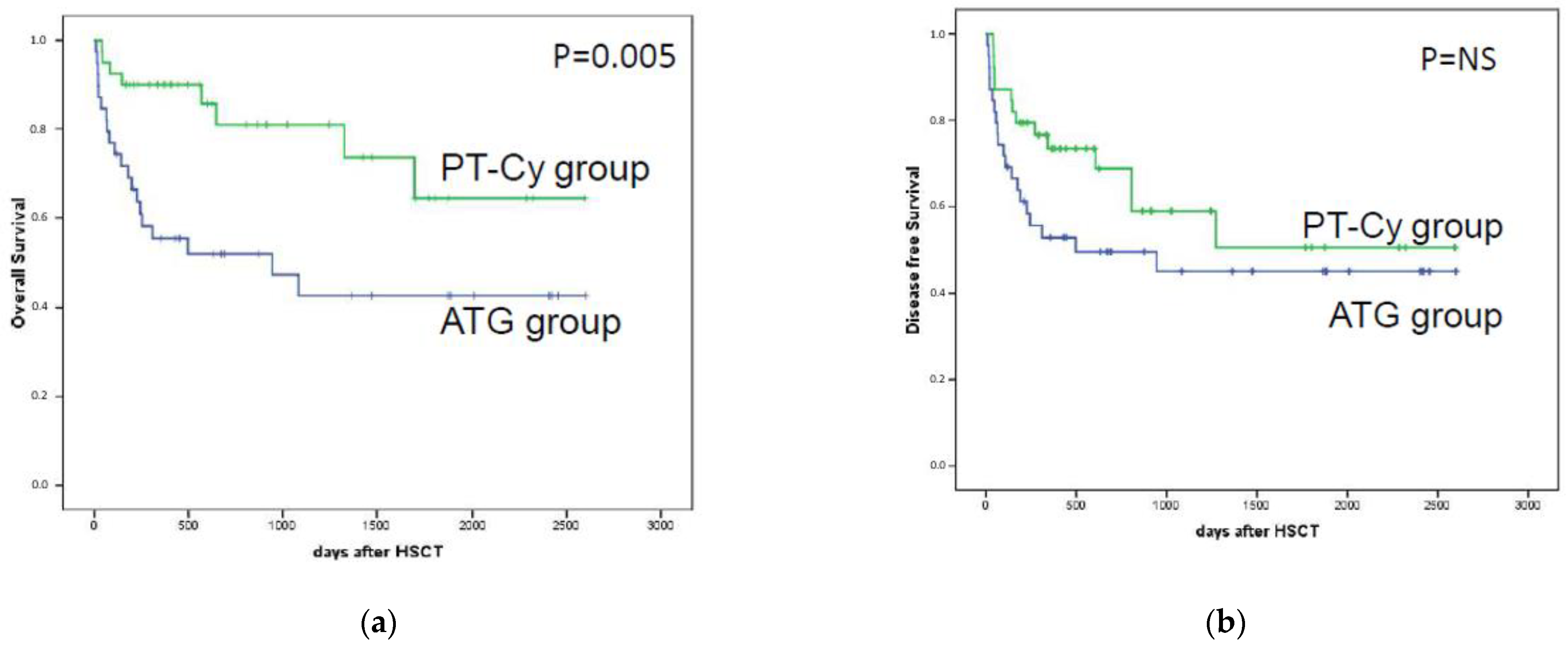
3.6. Overall Survival
3.7. Transplant-Related Mortality
3.8. Relapse Incidence
3.9. Cause of Death
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ballen, K.K.; King, R.J.; Chitphakdithai, P.; Bolan, C.D., Jr.; Agura, E.; Hartzman, R.J.; Kernan, N.A. The national marrow donor program 20 years of unrelated donor hematopoietic cell transplantation. Biol. Blood Marrow Transplant. 2008, 14, 2–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kekre, N.; Antin, J.H. Hematopoietic stem cell transplantation donor sources in the 21st century: Choosing the ideal donor when a perfect match does not exist. Blood 2014, 124, 334–343. [Google Scholar] [CrossRef]
- Ciurea, S.O.; Saliba, R.M.; Rondon, G.; Patah, P.A.; Aung, F.; Cano, P.; Andersson, B.S.; Kebriaei, P.; Popat, U.; Fernandez-Vina, M.; et al. Outcomes of patients with myeloid malignancies treated with allogeneic hematopoietic stem cell transplantation from matched unrelated donors compared with one human leukocyte antigen mismatched related donors using HLA typing at 10 loci. Biol. Blood Marrow Transplant. 2011, 17, 923–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamae, H.; Storer, B.E.; Storb, R.; Storek, J.; Chauncey, T.R.; Pulsipher, M.A.; Petersen, F.B.; Wade, J.C.; Maris, M.B.; Bruno, B.; et al. Low-dose total body irradiation and fludarabine conditioning for HLA class I-mismatched donor stem cell transplantation and immunologic recovery in patients with hematologic malignancies: A multicenter trial. Biol. Blood Marrow Transplant. 2010, 16, 384–394. [Google Scholar] [CrossRef] [Green Version]
- Mehta, J.; Singhal, S.; Gee, A.P.; Chiang, K.Y.; Godder, K.; van Rhee, F.; DeRienzo, S.; O’Neal, W.; Lamb, L.; Henslee-Downey, P.J. Bone marrow transplantation from partially HLA-mismatched family donors for acute leukemia: Single-center experience of 201 patients. Bone Marrow Transplant. 2004, 33, 389–396. [Google Scholar] [CrossRef] [Green Version]
- Hauzenberger, D.; Schaffer, M.; Ringdén, O.; Hassan, Z.; Omazic, B.; Mattsson, J.; Wikström, A.-C.; Remberger, M. Outcome of haematopoietic stem cell transplantation in patients transplanted with matched unrelated donors vs allele-mismatched donors: A single centre study. Tissue Antigens 2008, 72, 549–558. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Klein, J.; Haagenson, M.; Baxter-Lowe, L.A.; Confer, D.L.; Eapen, M.; Fernandez-Vina, M.; Flomenberg, N.; Horowitz, M.; Hurley, C.K.; et al. High-resolution donor-recipient HLA matching contributes to the success of unrelated donor marrow transplantation. Blood 2007, 110, 4576–4583. [Google Scholar] [CrossRef] [Green Version]
- Woolfrey, A.; Klein, J.P.; Haagenson, M.; Spellman, S.; Petersdorf, E.; Oudshoorn, M.; Gajewski, J.; Hale, G.A.; Horan, J.; Battiwalla, M.; et al. HLA-C antigen mismatch is associated with worse outcome in unrelated donor peripheral blood stem cell transplantation. Biol. Blood Marrow Transplant. 2011, 17, 885–892. [Google Scholar] [CrossRef] [Green Version]
- Ruutu, T.; van Biezen, A.; Hertenstein, B.; Henseler, A.; Garderet, L.; Passweg, J.; Mohty, M.; Sureda, A.; Niederwieser, D.; Gratwohl, A.; et al. Prophylaxis and treatment of GVHD after allogeneic haematopoietic SCT: A survey of centre strategies by the European Group for Blood and Marrow Transplantation. Bone Marrow Transplant. 2012, 47, 1459–1464. [Google Scholar] [CrossRef]
- Ruutu, T.; Gratwohl, A.; Niederwieser, D.; de Witte, T.; van der Werf, S.; van Biezen, A.; Mohty, M.; Kröger, N.; Rambaldi, A.; McGrath, E.; et al. The EBMT-ELN working group recommendations on the prophylaxis and treatment of GvHD: A change-control analysis. Bone Marrow Transplant. 2017, 52, 357–362. [Google Scholar] [CrossRef]
- Scheinberg, P.; Nunez, O.; Weinstein, B.; Scheinberg, P.; Biancotto, A.; Wu, C.O.; Young, N.S. Horse versus rabbit antithymocyte globulin in acquired aplastic anemia. N. Engl. J. Med. 2011, 365, 430–438. [Google Scholar] [CrossRef] [Green Version]
- Kekre, N.; Zhang, Y.; Zhang, M.J.; Carreras, J.; Ahmed, P.; Anderlini, P.; Atta, E.H.; Ayas, M.; Boelens, J.J.; Bonfim, C.; et al. Effect of antithymocyte globulin source on outcomes of bone marrow transplantation for severe aplastic anemia. Haematologica 2017, 102, 1291–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Wei, J.; Huang, Y.; He, Y.; Yang, D.; Zhang, R.; Jiang, E.; Ma, Q.; Zhai, W.; Yao, J.; et al. Effect of antithymocyte globulin source on outcomes of HLA-matched sibling allogeneic hematopoietic stem cell transplantation for patients with severe aplastic anemia. Biol. Blood Marrow Transplant. 2018, 24, 86–90. [Google Scholar] [CrossRef] [Green Version]
- Kröger, N.; Solano, C.; Wolschke, C.; Bandini, G.; Patriarca, F.; Pini, M.; Nagler, A.; Selleri, C.; Risitano, A.; Messina, G.; et al. Antilymphocyte Globulin for Prevention of Chronic Graft-versus-Host Disease. N. Engl. J. Med. 2016, 374, 43–53. [Google Scholar] [CrossRef]
- Kanakry, C.G.; O’Donnell, P.V.; Furlong, T.; De Lima, M.J.; Wei, W.; Medeot, M.; Mielcarek, M.; Champlin, R.E.; Jones, R.J.; Thall, P.F.; et al. Multi-institutional study of post-transplantation cyclophosphamide as single-agent graft-versus-host disease prophylaxis after allogeneic bone marrow transplantation using myeloablative busulfan and fludarabine conditioning. J. Clin. Oncol. 2014, 32, 3497–3505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanakry, C.G.; Fuchs, E.J.; Luznik, L. Modern approaches to HLA-haploidentical blood or marrow transplantation. Nat. Rev. Clin. Oncol. 2016, 13, 10–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanakry, C.G.; Ganguly, S.; Zahurak, M.; Bolaños-Meade, J.; Thoburn, C.; Perkins, B.; Fuchs, E.J.; Jones, R.J.; Hess, A.D.; Luznik, L. Aldehyde dehydrogenase expression drives human regulatory T cell resistance to post-transplantation cyclophosphamide. Sci. Transl. Med. 2013, 5, 211ra157. [Google Scholar] [CrossRef] [Green Version]
- Carnevale-Schianca, F.; Caravelli, D.; Gallo, S.; Coha, V.; D’Ambrosio, L.; Vassallo, E.; Fizzotti, M.; Nesi, F.; Gioeni, L.; Berger, M.; et al. Post-Transplant Cyclophosphamide and Tacrolimus–Mycophenolate Mofetil Combination Prevents Graft-versus-Host Disease in Allogeneic Peripheral Blood Hematopoietic Cell Transplantation from HLA-Matched Donors. Biol. Blood Marrow Transplant. 2017, 23, 459–466. [Google Scholar] [CrossRef] [Green Version]
- Al-Homsi, A.S.; Roy, T.S.; Cole, K.; Feng, Y.; Duffner, U. Post-transplant high-dose cyclophosphamide for the prevention of graft-versus-host disease. Biol. Blood Marrow Transplant. 2015, 21, 604–611. [Google Scholar] [CrossRef] [Green Version]
- Berger, M.; Lanino, E.; Cesaro, S.; Zecca, M.; Vassallo, E.; Faraci, M.; De Bortoli, M.; Barat, V.; Prete, A.; Fagioli, F. Feasibility and Outcome of Haploidentical Hematopoietic Stem Cell Transplantation with Post-Transplant High-Dose Cyclophosphamide for Children and Adolescents with Hematologic Malignancies: An AIEOP-GITMO Retrospective Multicenter Study. Biol. Blood Marrow Transplant. 2016, 22, 902–909. [Google Scholar] [CrossRef] [Green Version]
- Saglio, F.; Berger, M.; Spadea, M.; Pessolano, R.; Carraro, F.; Barone, M.; Quarello, P.; Vassallo, E.; Fagioli, F. Haploidentical HSCT with post transplantation cyclophosphamide versus unrelated donor HSCT in pediatric patients affected by acute leukemia. Bone Marrow Transplant. 2020, 56, 586–595. [Google Scholar] [CrossRef] [PubMed]
- Battipaglia, G.; Labopin, M.; Kröger, N.; Vitek, A.; Afanasyev, B.; Hilgendorf, I.; Schetelig, J.; Ganser, A.; Blaise, D.; Itälä-Remes, M.; et al. Posttransplant cyclophosphamide vs antithymocyte globulin in HLA-mismatched unrelated donor transplantation. Blood 2019, 134, 892–899. [Google Scholar] [CrossRef] [PubMed]
- Nagler, A.; Kanate, A.S.; Labopin, M.; Ciceri, F.; Angelucci, E.; Koc, Y.; Gülbas, Z.; Arcese, W.; Tischer, J.; Pioltelli, P.; et al. Post-transplant cyclophosphamide versus antithymocyte globulin for graft-versus-host disease prevention in haploidentical transplantation for adult acute lymphoblastic leukemia. Haematologica 2021, 106, 1591. [Google Scholar] [CrossRef] [PubMed]
- Shaw, B.E.; Jimenez-Jimenez, A.M.; Burns, L.J.; Logan, B.R.; Khimani, F.; Shaffer, B.C.; Shah, N.N.; Mussetter, A.; Tang, X.-Y.; McCarty, J.M.; et al. National Marrow Donor Program–Sponsored Multicenter, Phase II Trial of HLA-Mismatched Unrelated Donor Bone Marrow Transplantation Using Post-Transplant Cyclophosphamide. J. Clin. Oncol. 2021, 39, 1971–1982. [Google Scholar] [CrossRef]
- Bailén, R.; Kwon, M.; Pascual-Cascón, M.J.; Ferrà, C.; Sanz, J.; Gallardo-Morillo, A.; García-Sola, A.; Torrent, A.; Jiménez-Lorenzo, M.J.; Piñana, J.L.; et al. Post-transplant cyclophosphamide for GVHD prophylaxis compared to ATG-based prophylaxis in unrelated donor transplantation. Ann. Hematol. 2021, 100, 541–553. [Google Scholar] [CrossRef]
- Gao, F.; Zhang, J.; Hu, J.; Lin, L.; Xu, Y. Post-transplant cyclophosphamide versus antithymocyte globulin in allogeneic hematopoietic cell transplantation: A meta-analysis. Ann. Hematol. 2021, 100, 529–540. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, S.; Hattori, N.; Matsui, T.; Nakata, A.; Sasaki, Y.; Shimada, S.; Murai, S.; Abe, M.; Baba, Y.; Watanuki, M.; et al. Refined Disease Risk Index for Hematological Malignancies, Including Rare Disorders, After Allogeneic Stem Cell Transplantation. Transplant. Proc. 2019, 51, 3437–3443. [Google Scholar] [CrossRef]
- Armand, P.; Gibson, C.J.; Cutler, C.; Ho, V.T.; Koreth, J.; Alyea, E.P.; Ritz, J.; Sorror, M.L.; Lee, S.J.; Deeg, H.J.; et al. A disease risk index for patients undergoing allogeneic stem cell transplantation. Blood 2012, 120, 905–913. [Google Scholar] [CrossRef] [Green Version]
- Gratwohl, A. The EBMT risk score. Bone Marrow Transplant. 2012, 47, 749–756. [Google Scholar] [CrossRef]
- Tiercy, J.M. How to select the best available related or unrelated donor of hematopoietic stem cells? Haematologica 2016, 101, 680–687. [Google Scholar] [CrossRef] [Green Version]
- Fürst, D.; Neuchel, C.; Tsamadou, C.; Schrezenmeier, H.; Mytilineos, J. HLA Matching in Unrelated Stem Cell Transplantation up to Date. Transfus. Med. Hemother. 2019, 46, 326–336. [Google Scholar] [CrossRef] [PubMed]
- Fleischhauer, K. Selection of matched unrelated donors moving forward: From HLA allele counting to functional matching. Hematol. Am. Soc. Hematol. Educ. Program. 2019, 2019, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Oran, B.; Saliba, R.M.; Carmazzi, Y.; de Lima, M.; Rondon, G.; Ahmed, S.; Alousi, A.; Andersson, B.S.; Anderlini, P.; Alvarez, M.; et al. Effect of nonpermissive HLA-DPB1 mismatches after unrelated allogeneic transplantation with in vivo T-cell depletion. Blood 2018, 131, 1248–1257. [Google Scholar] [CrossRef] [PubMed]
- Pidala, J.; Wang, T.; Haagenson, M.; Spellman, S.R.; Askar, M.; Battiwalla, M.; Baxter-Lowe, L.A.; Bitan, M.; Fernandez-Viña, M.; Gandhi, M.; et al. Amino acid substitution at peptide-binding pockets of HLA class I molecules increases risk of severe acute GVHD and mortality. Blood 2013, 122, 3651–3658. [Google Scholar] [CrossRef] [Green Version]
- Glucksberg, H.; Storb, R.; Fefer, A.; Buckner, C.D.; Neiman, P.E.; Clift, R.A.; Lerner, K.G.; Thomas, E.D. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-A-matched sibling donors. Transplantation 1974, 18, 295–304. [Google Scholar] [CrossRef]
- Shulman, H.M.; Sullivan, K.M.; Weiden, P.L.; McDonald, G.B.; Striker, G.E.; Sale, G.E.; Sale, G.E.; Hackman, R.; Tsoi, M.-S.; Storb, R.; et al. Chronic graft-versus-host syndrome in man. A long-term clinicopathologic study of 20 Seattle patients. Am. J. Med. 1980, 69, 204–217. [Google Scholar] [CrossRef]
- Spyridonidis, A.; Labopin, M.; Savani, B.N.; Niittyvuopio, R.; Blaise, D.; Craddock, C.; Socié, G.; Platzbecker, U.; Beelen, D.; Milpied, N.; et al. Redefining and measuring transplant conditioning intensity in current era: A study in acute myeloid leukemia patients. Bone Marrow Transplant. 2020, 55, 1114–1125. [Google Scholar] [CrossRef]
- Conover, W.J. Practical Nonparametric Statistics, 2nd ed.; Wiley: New York, NY, USA, 1980; p. 493. [Google Scholar]
- Walpole, R.E.; Myers, R.H.; Myers, S.L.; Ye, K.E. Probability and Statistics for Engineers and Scientists, 9th ed.; Pearson: London, UK, 2012. [Google Scholar]
- Kaplan, E.L.; Meier, P. Nonparametric estimation from incomplete observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. The logrank test. BMJ 2004, 328, 1073. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.T. Cumulative incidence in competing risks data and competing risks regression analysis. Clin. Cancer Res. 2007, 13 Pt 1, 559–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verneris, M.R.; Lee, S.J.; Ahn, K.W.; Wang, H.L.; Battiwalla, M.; Inamoto, Y.; Fernandez-Vina, M.A.; Gajewski, J.; Pidala, J.; Munker, R.; et al. HLA-mismatch is associated with worse outcomes after unrelated donor reduced intensity conditioning hematopoietic cell transplantation: An analysis from the CIBMTR. Biol. Blood Marrow Transplant. 2015, 21, 1783–1789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jagasia, M.H.; Greinix, H.T.; Arora, M.; Williams, K.M.; Wolff, D.; Cowen, E.W.; Palmer, J.; Weisdorf, D.; Treister, N.S.; Cheng, G.-S.; et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group report. Biol. Blood Marrow Transplant. 2015, 21, 389–401.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katovich Hurley, C.; Woolfrey, A.; Wang, T.; Haagenson, M.; Umejiego, J.; Aljurf, M.; Battiwalla, M.; Dehn, J.; Horan, J.; Oudshoorn, M.; et al. The impact of HLA unidirectional mismatches on the outcome of myeloablative hematopoietic stem cell transplantation with unrelated donors. Blood 2013, 121, 4800–4806. [Google Scholar] [CrossRef] [PubMed]
- Gaballa, S.; Ge, I.; El Fakih, R.; Brammer, J.E.; Kongtim, P.; Tomuleasa, C.; Wang, S.A.; Lee, D.; Petropoulos, D.; Cao, K.; et al. Results of 2-arm, phase 2 clinical trial using post-transplantation Cyclophopshamide for the prevention of graft-versus-host disease in haploidentical donor and mismatched unrelated donor hematopoietic stem cell transplantation. Cancer 2016, 123, 3316–3326. [Google Scholar] [CrossRef]
- Crocchiolo, R.; Ciceri, F.; Fleischhauer, K.; Oneto, R.; Bruno, B.; Pollichieni, S.; Sacchi, N.; Sormani, M.P.; Fanin, R.; Bandini, G.; et al. HLA matching affects clinical outcome of adult patients undergoing haematopoietic SCT from unrelated donors: A study from the Gruppo Italiano Trapianto di Midollo Osseo and Italian Bone Marrow Donor Registry. Bone Marrow Transplant. 2009, 44, 571–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasegawa, W.; Lipton, J.H.; Messner, H.A.; Jamal, H.; Yi, Q.L.; Daly, A.S.; Kotchetkova, N.; Kiss, T.L. Influence of one human leukocyte antigen mismatch on outcome of allogeneic bone marrow transplantation from related donors. Hematology 2003, 8, 27–33. [Google Scholar] [CrossRef]
- Kekre, N.; Mak, K.S.; Stopsack, K.H.; Binder, M.; Ishii, K.; Brånvall, E.; Cutler, C.S. Impact of HLA-Mismatch in Unrelated Donor Hematopoietic Stem Cell Transplantation: A Meta-Analysis. Am. J. Hematol. 2016, 91, 551–555. [Google Scholar] [CrossRef] [Green Version]
- Modi, D.; Kondrat, K.; Kim, S.; Deol, A.; Ayash, L.; Ratanatharathorn, V.; Uberti, J.P. Post-transplant Cyclophosphamide Versus Thymoglobulin in HLA-Mismatched Unrelated Donor Transplant for Acute Myelogenous Leukemia and Myelodysplastic Syndrome. Transplant. Cell. Ther. 2021, 27, 760–767. [Google Scholar] [CrossRef]
- Luznik, L.; O’Donnell, P.V.; Symons, H.J.; Chen, A.R.; Leffell, M.S.; Zahurak, M.; Gooley, T.A.; Piantadosi, S.; Kaup, M.; Ambinder, R.F.; et al. HLA-haploidentical bone marrow transplantation for hematological malignancies using nomyeloablative conditioning and high-dose post transplantation Cyclophosphamide. Biol. Blood Marrow Transplant. 2008, 14, 641–650. [Google Scholar] [CrossRef] [Green Version]
- Mehta, R.S.; Saliba, R.M.; Chen, J.; Rondon, G.; Hammerstrom, A.E.; Alousi, A.; Qazilbash, M.; Bashir, Q.; Ahmed, S.; Popat, U.; et al. Post-transplantation cyclophosphamide versus conventional graft-versus-host disease prophylaxis in mismatched unrelated donor haematopoietic cell transplantation. Br. J. Haematol. 2016, 173, 444–455. [Google Scholar] [CrossRef] [Green Version]
- Jorge, A.S.; Lledo, M.S.; Pereira, A.; Gutierrez, G.; Fernández-Avilés, F.; Rosiñol, L.; Llobet, N.; Solano, T.; Urbano-Ispízua, A.; Rovira, M.; et al. Single antigen-mismatched unrelated hematopoietic stem cell transplantation using high-dose post-transplantation cyclophosphamide is a suitable alternative for patients lacking HLA-matched donors. Biol. Blood Marrow Transplant. 2018, 24, 1196–1202. [Google Scholar] [CrossRef] [Green Version]
- Arora, M.; Weisdorf, D.J.; Spellman, S.; Haagenson, M.D.; Klein, J.P.; Hurley, C.K.; Selby, G.B.; Antin, J.H.; Kernan, N.A.; Kollman, C.; et al. HLA-identical sibling compared with 8/8 matched and mismatched unrelated donor bone marrow transplant for chronic phase chronic myeloid leukemia. J. Clin. Oncol. 2009, 27, 1644–1652. [Google Scholar] [CrossRef] [Green Version]
- Ruutu, T.; Gratwohl, A.; de Witte, T.; Afanasyev, B.; Apperley, J.; Bacigalupo, A.; Dazzi, F.; Dreger, P.; Duarte, R.; Finke, J.; et al. Prophylaxis and treatment of GVHD: EBMT-ELN working group recommendations for a standardized practice. Bone Marrow Transplant. 2014, 49, 168–173. [Google Scholar] [CrossRef] [Green Version]
- Clausen, J.; Böhm, A.; Straßl, I. HLA-C KIR-Ligands Determine the Impact of Anti-Thymocyte Globulin (ATG) on Graft versus Host and Graft versus Leukemia Effects Following Hematopoietic Stem Cell Transplantation. Biomedicines 2017, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, P.; Lang, A.M.; Matela, M.; Horrer, A.; Schilling, A.; Joechner, A.; Wiedenmann, M.; Seitz, C.; Döring, M.; Feuchtinger, T.; et al. Ex vivo expansion of autologous, donor-derived NK-, γδT-, and cytokine induced killer (CIK) cells post haploidentical hematopoietic stem cell transplantation results in increased antitumor activity. Bone Marrow Transplant. 2019, 54, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Solomon Scott, R.; Aubrey Michael, T.; Zhang, X. Selecting the Best Donor for Haploidentical Transplant: Impact of HLA, Killer Cell Immunoglobulin-Like Receptor Genotyping, and Other Clinical Variables. Biol. Blood Marrow Transplant. 2018, 24, 789–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narayan, R.; Benjamin, J.E.; Shah, O.; Tian, L.; Tate, K.; Armstrong, R.; Xie, B.J.; Lowsky, R.; Laport, G.; Negrin, R.S.; et al. Donor-Derived Cytokine-Induced Killer Cell Infusion as Consolidation after Nonmyeloablative Allogeneic Transplantation for Myeloid Neoplasms. Biol. Blood Marrow Transplant. 2019, 25, 1293–1303. [Google Scholar] [CrossRef]
- Zhang, C.; Ma, Y.Y.; Liu, J.; Liu, Y.; Gao, L.; Gao, L.; Kong, P.-Y.; Xiong, Q.-H.; Mei, W.-L.; Liu, J.; et al. Preventive infusion of donor-derived CAR-T cells after haploidentical transplantation: Two cases report. Medicine 2019, 98, e16498. [Google Scholar] [CrossRef] [PubMed]
- Ayuk, F.; Fehse, B.; Janson, D.; Berger, C.; Riecken, K.; Kröger, N. Excellent proliferation and persistence of allogeneic donor-derived 41-BB based CAR-T cells despite immunosuppression with cyclosporine A. Haematologica 2020, 105, 322–324. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| CSA+MTX+ATG N = 39 | Tacrolimus+MMF+PTCy N = 40 | p | ||
|---|---|---|---|---|
| Patient gender | Male | 24 (61%) | 25 (62%) | NS |
| Female | 15 (38%) | 15 (37%) | ||
| Patient age | ≥60 | 17 (43%) | 8 (20%) | 0.02 |
| <60 | 22 (56%) | 32 (80%) | ||
| Disease | ALL | 8 (20%) | 6 (15%) | NS |
| AML | 19 (49%) | 18 (45%) | ||
| CLL | 2 (5%) | 1 (2%) | ||
| CML | 1 (2%) | 0 | ||
| MDS | 5 (13%) | 2 (5%) | ||
| MM | 2 (5%) | 7 (17%) | ||
| NHL | 1 (2%) | 2 (5%) | ||
| HL | 0 | 3 (7%) | ||
| MF | 1 (2%) | 1 (2%) | ||
| Disease risk index | Low | 3 (8%) | 9 (22%) | 0.04 |
| Intermediate | 26 (67%) | 16 (40%) | ||
| High | 10 (25%) | 15 (37%) | ||
| Very high | 0 | 0 | ||
| EBMT score | 2 | 0 | 3 (7%) | NS |
| 3 | 8 (20%) | 6 (15%) | ||
| 4 | 8 (20%) | 12 (30%) | ||
| 5 | 16 (41%) | 7 (17%) | ||
| 6 | 6 (15%) | 12 (30%) | ||
| 7 | 1 (2%) | 0 | ||
| Interval diagnosis–HSCT | >1 year | 17 (43%) | 27 (67%) | 0.04 |
| <1 year | 22 (56%) | 13 (32%) | ||
| Conditioning | TBI-based | 9 (23%) | 2 (5%) | 0.02 |
| Chemo-based | 30 (77%) | 38 (95%) | ||
| Intensity of conditioning | RIC | 8 (20%) | 2 (5%) | 0.04 |
| MAC | 31 (80%) | 38 (95%) | ||
| Donor gender | Male | 23 (59%) | 27 (%) | |
| Female | 16 (41%) | 13 (67%) | ||
| Donor age | >30 | 15 (38%) | 20 (50%) | NS |
| <30 | 24 (61%) | 20 (50%) | ||
| Gender relation | F > M | 16 (41%) | 16 (40%) | NS |
| other | 23 (59%) | 24 (60%) | ||
| PBSC CD34+ cells | >median | 19 (49%) | 18 (45%) | NS |
| <median | 20 (51%) | 22 (55%) | ||
| HLA-A mismatch | 18 (46%) | 23 (57%) | NS | |
| HLA-B mismatch | 8 (20%) | 6 (15%) | ||
| HLA-C mismatch | 12 (31%) | 9 (22%) | ||
| HLA-DQB1 mismatch | 8 (20%) | 10 (25%) | ||
| Double class 1 mismatch | 3 (7%) | 2 (5%) | ||
| Double class I and class II mismatch | 4 (10%) | 6 (15%) |
| (a) | |||||||
|---|---|---|---|---|---|---|---|
| DAY-100 aGvHD II–IV (95% CI) | p | DAY-100 aGvHD III–IV (95% CI) | p | 3-y cGvHD (95% CI) | p | ||
| Patient’s gender | M | 22% (12–38) | NS | 8% (3–22) | 0.14 | 37% (25–55) | 0.04 |
| F | 22% (11–45) | 0% | 12% (4–36) | ||||
| Patient’s age | >60 year | 18% (7–44) | NS | 0% | 0.17 | 28% (13–58) | NS |
| <60 year | 23% (14–38) | 8% (3–20) | 28% (18–44) | ||||
| Donor | M | 18% (9–33) | NS | 4% (1–16) | NS | 24% (14–42) | NS |
| F | 30% (16–53) | 7% (2–28) | 32% (18–57) | ||||
| GvHD prophylaxis | ATG-based | 39% (26–60) | 0.0006 | 11% (4–28) | 0.014 | 48% (33–70) | 0.0005 |
| PTCy-based | 7% (2–22) | 0% | 13% (6–30) | ||||
| Donor’s age | >30 | 13% (5–32) | 0.06 | 0% | 0.054 | 20% (10–41) | 0.09 |
| <30 | 28% (18–46) | 9% (4–24) | 35% (23–54) | ||||
| Gender relation | F>M | 21% (10–42) | NS | 6% (2–25) | NS | 27% (14–51) | NS |
| other | 23% (13–39) | 4% (1–17) | 29% (18–47) | ||||
| Conditioning | TBI | 50% (27–93) | 0.01 | 9% (1–59) | NS | 22% (6–75) | NS |
| Chemo | 17% (10–30) | 5% (1–14) | 29% (20–44) | ||||
| Intensity of conditioning | RIC | 52% (16–80) | 0.008 | 10% (0–28) | NS | 60% (30–90) | 0.007 |
| MAC | 17% (8–26) | 5% (0–10) | 28% (13–43) | ||||
| DRI | low | 17% (5–59) | NS | 8% (1–54) | NS | 25% (9–67) | NS |
| intermediate | 22% (13–40) | 5% (1–19) | 30% (18–49) | ||||
| high | 24% (11–51) | 4% (1–28) | 28% (13–58) | ||||
| EBMT score | 2 | 0% | 0% | 33% (7–100) | |||
| 3 | 36% (17–72) | 14% (4–51) | 43% (23–78) | ||||
| 4 | 15% (5–42) | 5% (1–34) | 20% (8–48) | ||||
| 5 | 22% (9–53) | 0% | 21% (8–58) | ||||
| 6 | 23% (10–55) | 6% (1–37) | 31% (14–69) | ||||
| 7 | 0% | 0% | 100% | ||||
| HLA-A | mismatch | 24% (13–42) | NS | 5% (1–20) | NS | 31% (18–52) | NS |
| match | 20% (10–39) | 5% (1–21) | 27% (16–48) | ||||
| HLA-B | mismatch | 38% (19–76) | NS | 14% (4–51) | 0.05 | 46% (26–83) | 0.0003 |
| match | 18% (11–31) | 3% (1–13) | 25% (16–40) | ||||
| HLA-C | mismatch | 11% (3–41) | NS | 0% | NS | 25% (11–58) | NS |
| match | 25% (16–49) | 7% (3–18) | 31% (20–47) | ||||
| HLA-DQB1 | mismatch | 17% (6–49) | NS | 6% (1–37) | NS | 28% (13–58) | NS |
| match | 24% (15–38) | 5% (2–16) | 30% (19–46) | ||||
| (b) | |||||||
| 3-y OS (95% CI) | p | 3-y TRM (95% CI) | p | 3-y RI (95% CI) | p | ||
| Patient’s gender | M | 52% (33–70) | NS | 20% (12–35) | NS | 26% (17–42) | NS |
| F | 58% (35–91) | 24% (12–46) | 14% (5–34) | ||||
| Patient’s age | >60 year | 27% (4–50) | 0.005 | 40% (25–64) | 0.0021 | 20% (9–44) | NS |
| <60 year | 67% (52–83) | 13% (7–26) | 23% (14–37) | ||||
| Donor | M | 55% (37–74) | NS | 21% (12–36) | NS | 23% (14–38) | NS |
| F | 51% (29–74) | 24% (13–46) | 21% (10–42) | ||||
| GvHD prophylaxis | ATG-based | 42% (25–60) | 0.005 | 36% (24–55) | 0.0033 | 15% (7–32) | NS |
| PTCy-based | 64% (41–88) | 8% (2–23) | 28% (17–46) | ||||
| Donor’s age | >30 | 62% (41–83) | 0.11 | 17% (8–35) | NS | 28% (17–48) | NS |
| <30 | 44% (24–65) | 26% (15–42) | 16% (8–32) | ||||
| Gender relation | F>M | 47% (26–77) | NS | 28% (16–49) | NS | 25% (14–45) | NS |
| other | 57% (36–77) | 17% (9–33) | 19% (11–35) | ||||
| Conditioning | TBI | 51% (19–83) | NS | 9% (1–59) | 0.33 | 36% (17–79) | NS |
| Chemo | 55% (38–71) | 24% (15–37) | 19% (12–32) | ||||
| Intensity of conditioning | RIC | 64% (30–98) | NS | 20% () | NS | 0% | 0.06 |
| MAC | 52% (36–68) | 39% (24–56) | |||||
| DRI | low | 92% (76–100) | 0.01 | 8% (1–54) | 0.21 | 8% (1–54) | 0.015 |
| intermediate | 56% (36–76) | 21% (12–38) | 17% (8–33) | ||||
| high | 26% (0–53) | 29% (16–54) | 37% (22–63) | ||||
| EBMT score | 2 | 100% | 0.02 | 0% | 0% | <0.00001 | |
| 3 | 68% (32–100) | 7% (1–47) | 14% (4–51) | ||||
| 4 | 71% (49–93) | 10% (3–37) | 20% (8–48) | ||||
| 5 | 46% (26–67) | 43% (27–69) | 26% (13–52) | ||||
| 6 | 49% (16–81) | 23% (10–55) | 23% (10–55) | ||||
| 7 | 100% | 0% | 0% | ||||
| HLA-A | mismatch | 59% (41–79) | NS | 22% (12–40) | NS | 20% (11–37) | NS |
| match | 64% (47–81) | 21% (11–39) | 21% (11–39) | ||||
| HLA-B | mismatch | 60% (33–87) | NS | 21% (8–58) | NS | 14% (4–51) | NS |
| match | 60% (46–75) | 22% (14–35) | 22% (14–35) | ||||
| HLA-C | mismatch | 37% (13–61) | NS | 28% (14–56) | NS | 28% (14–56) | NS |
| match | 66% (52–80) | 19% (11–33) | 17% (10–31) | ||||
| HLA-DQB1 | mismatch | 88% (73–100) | 0.02 | 6% (1–37) | 0.04 | 17% (6–47) | NS |
| match | 54% (39–68) | 27% (17–40) | 23% (15–37) | ||||
| GvHD II–IV (95% CI) | 3-y cGvHD (95% CI) | 3-y OS (95% CI) | 3-y TRM (95% CI) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Risk factor | OR | p | OR | p | RR | p | OR | p | |
| GvHD prophylaxis | ATG | 1.28 (1.1–3.9) | 0.05 | 1 | 0.001 | 1 | 0.025 | 1 | 0.031 |
| PT-Cy | 1 | 0.143 (0.07–0.4) | 0.342 (0.18–0.56) | 0.231 (0.09–0.4) | |||||
| Patient’s age | <60 year | 0.210 (0.09–0.6) | 0.028 | — | NS | 1 | 0.002 | 1 | 0.01 |
| >60 year | 1 | 3.5 (1.9–7.6) | 4.24 (3.6–6.3) | ||||||
| DRI | low-intermediate | — | NS | — | NS | 1 | 0.005 | 1 | 0.05 |
| high | 2.90 (1.2–4.9) | 2.552 (1.9–5.1) | |||||||
| DQB1 mismatch | no | — | NS | — | NS | — | NS | 1 | 0.037 |
| yes | 0.112 (0.08–0.5) | ||||||||
| Intensity of conditioning | MAC | 1 | 0.008 | — | NS | — | NS | — | NS |
| RIC | 6.404 (3.4–10.8) | ||||||||
| HLA-class 1 and DQB1 mismatches | no | — | NS | 1 | 0.012 | — | NS | — | NS |
| yes | 4.170 (2.9–8.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berger, M.; Barone, M.; Carnevale-Schianca, F.; De Gobbi, M.; Nicoli, P.; Caravelli, D.; Cilloni, D.; Paruzzo, L.; Spadea, M.; Mareschi, K.; et al. HSCT with Mismatched Unrelated Donors (MMUD): A Comparison of Different Platforms for GvHD Prophylaxis. Transplantology 2022, 3, 51-67. https://doi.org/10.3390/transplantology3010006
Berger M, Barone M, Carnevale-Schianca F, De Gobbi M, Nicoli P, Caravelli D, Cilloni D, Paruzzo L, Spadea M, Mareschi K, et al. HSCT with Mismatched Unrelated Donors (MMUD): A Comparison of Different Platforms for GvHD Prophylaxis. Transplantology. 2022; 3(1):51-67. https://doi.org/10.3390/transplantology3010006
Chicago/Turabian StyleBerger, Massimo, Marta Barone, Fabrizio Carnevale-Schianca, Marco De Gobbi, Paolo Nicoli, Daniela Caravelli, Daniela Cilloni, Luca Paruzzo, Manuela Spadea, Katia Mareschi, and et al. 2022. "HSCT with Mismatched Unrelated Donors (MMUD): A Comparison of Different Platforms for GvHD Prophylaxis" Transplantology 3, no. 1: 51-67. https://doi.org/10.3390/transplantology3010006
APA StyleBerger, M., Barone, M., Carnevale-Schianca, F., De Gobbi, M., Nicoli, P., Caravelli, D., Cilloni, D., Paruzzo, L., Spadea, M., Mareschi, K., Aglietta, M., & Fagioli, F. (2022). HSCT with Mismatched Unrelated Donors (MMUD): A Comparison of Different Platforms for GvHD Prophylaxis. Transplantology, 3(1), 51-67. https://doi.org/10.3390/transplantology3010006