1. Introduction
Cytomegalovirus (CMV) infection is an important cause of morbidity and mortality in lung transplantation and is associated with impaired allograft function, development of bronchiolitis obliterans syndrome, and decreased long-term survival [
1]. Current guidelines recommend antiviral prophylaxis against CMV for 6–12 months after lung transplant, typically with valganciclovir [
2]. Bone marrow suppression and leukopenia are well-known adverse effects of valganciclovir and, if severe enough, can limit its utility [
2]. The incidence of valganciclovir-associated leukopenia has been reported to be as high as 20% in kidney transplant recipients and 58% in bone marrow transplant patients [
3].
Letermovir, a novel antiviral agent approved for CMV prophylaxis in hematopoietic cell transplantation (HCT) [
4], preferentially targets and inhibits the CMV viral terminase, a virus-specific enzyme complex encoded by genes UL51, UL56, and UL89 and responsible for cleavage and translocation of CMV progeny DNA into capsids [
5]. The risk of side effects, including myelosuppression, is expected to be lower with letermovir. Reports have described treatment of resistant CMV retinitis and pneumonitis with letermovir and use of letermovir for secondary prophylaxis after ganciclovir-resistant CMV infections [
6,
7]. Recently, a series of nine thoracic organ transplant patients receiving letermovir for CMV prophylaxis was reported [
8]. Although letermovir was well-tolerated, the rate of treatment failure defined as breakthrough CMV DNAemia appeared to be higher than previously reported. Herein, we describe our single-center experience with letermovir for CMV prophylaxis in 17 lung transplant patients who developed severe leukopenia due to valganciclovir.
2. Materials and Methods
We retrospectively reviewed the electronic medical record of lung transplant patients who were administered letermovir for CMV prophylaxis at our center between 1 January 2018 and 1 January 2020. Collected data included indication for transplant, transplant type (single vs. bilateral), age at time of transplant, sex, CMV serostatus, history of CMV infection, baseline induction and maintenance immunosuppression regimen, antifungal prophylaxis, time from transplant to initiation of letermovir, duration of letermovir use, and reason for letermovir discontinuation (if applicable). Information on plasma CMV DNA polymerase chain reaction (PCR) testing (Abbott RealTime CMV assay), white blood cell (WBC) count, serum creatinine (SCr), serum tacrolimus trough level, and tacrolimus dose adjustments were also collected. Leukopenia was defined as serum white blood cell (WBC) count less than 4.0 K/uL. The Ohio State University Institutional Review Board approved the study.
2.1. Institutional Protocol
All lung transplant recipients received basiliximab and methylprednisolone for induction immunosuppression, and tacrolimus, mycophenolate, and prednisone as maintenance. Patients with donor or recipient CMV seropositive status received antiviral prophylaxis with valganciclovir started on post-operative day (POD) 0 and continued for twelve months. Patients with donor and recipient CMV seronegative status received antiviral prophylaxis with valacyclovir and were excluded from this study. Antifungal prophylaxis, typically with voriconazole, was started on POD 0 and continued for six to twelve months. Patients were transitioned to letermovir at different times post-transplant due to the development of leukopenia while on valganciclovir. Letermovir was dosed at 480 mg by mouth once daily based on manufacturer recommendations for use in hematopoietic stem cell transplantation. The decision to switch to letermovir was made by a multidisciplinary team including a transplant pulmonologist, infectious disease specialist, and pharmacist. Adjustments in immunosuppression dosing, including temporarily holding mycophenolate, were done prior to transition to letermovir.
2.2. Data Analysis
The effect of letermovir on WBC count was analyzed using a repeated measures mixed model and descriptive statistics, while secondary outcomes (incidence of breakthrough CMV DNAemia defined as any quantifiable CMV level while on letermovir, incidence of CMV disease defined as CMV infection requiring treatment, letermovir interactions with tacrolimus, change in SCr level, change in the need for human granulocyte colony stimulating factor (filgrastim) administration, incidence of acute rejection, change in pulmonary function testing (PFT), and patient reported side effects) were analyzed with descriptive statistics. In addition to analysis of data for the entire study period (approximately twelve months), a period of 60 days prior to and 60 days after letermovir initiation was also reviewed. As patients developed leukopenia at different times post-transplant, the ±60-day period was utilized to capture acute changes in laboratory parameters that triggered the change from valganciclovir to letermovir.
3. Results
Seventeen patients developed valganciclovir-induced leukopenia and were switched to letermovir between 1 January 2018 and 1 January 2020.
Table 1 highlights baseline patient characteristics (see also
Table S1). All but two patients underwent bilateral lung transplantation. One patient (#14) received a retransplant for chronic lung allograft dysfunction. Eleven patients were CMV donor positive, recipient negative (D+/R−), four patients were CMV D-/R+, and the remaining two patients were CMV D+/R+. All but four patients concurrently received letermovir with azole antifungal prophylaxis (12/17 voriconazole; 1/17 itraconazole for histoplasma in explant), whereas the other four patients had completed a 6–12 month course of voriconazole prophylaxis prior to letermovir initiation. Median time from transplant to letermovir initiation was 185 days (range: 77–767 days), and median duration of letermovir usage was 180 days (range: 55–689 days).
All 17 patients had developed leukopenia while taking valganciclovir, with 13 patients requiring filgrastim administration. While we used a WBC cutoff of <4.0 K/uL to define leukopenia, all patients had a WBC nadir well below 4.0 K/uL, with a median nadir of 1.1 K/uL (range < 0.30–2.19 K/uL) (
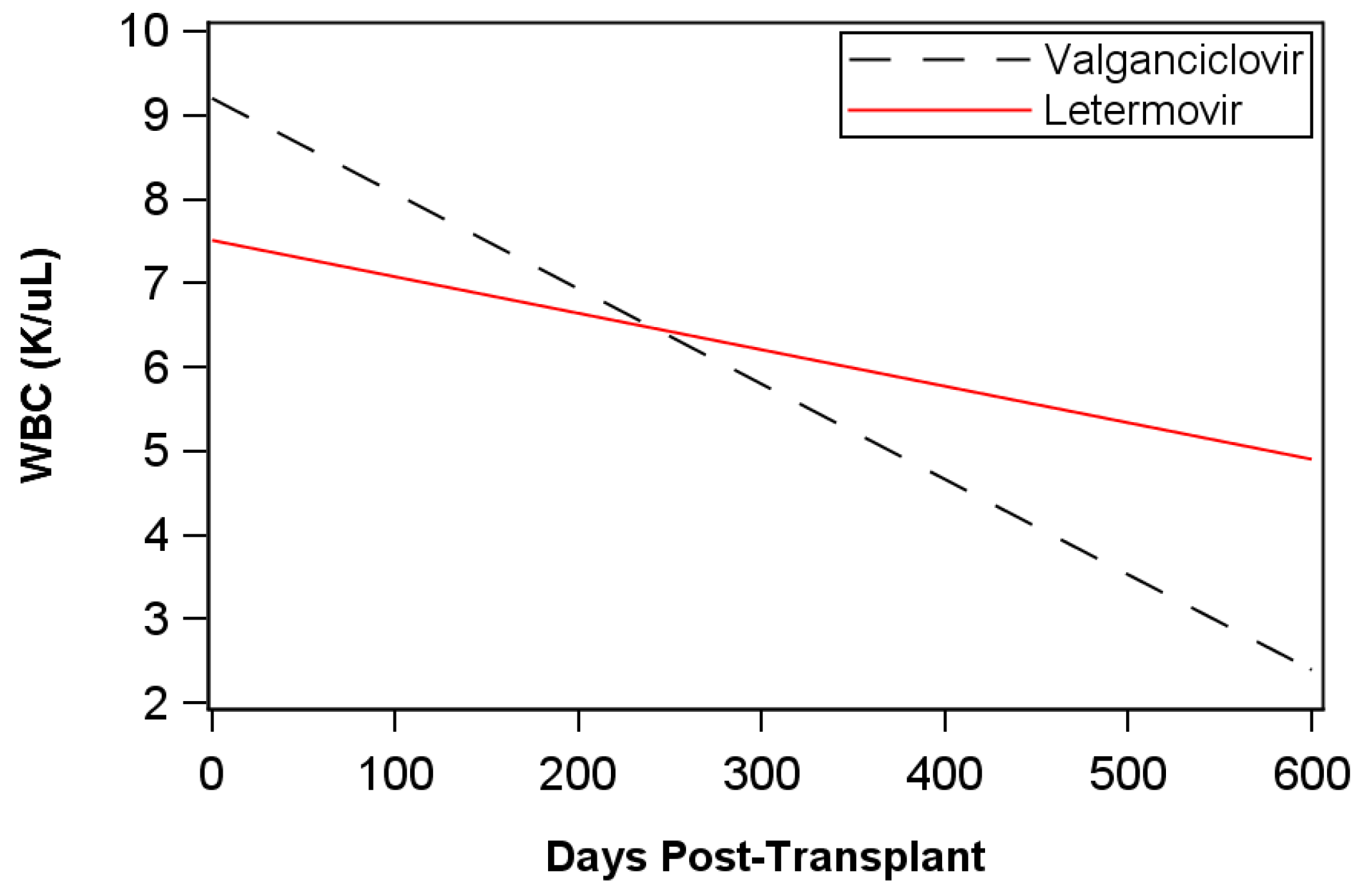
Table S1). A repeated measures mixed model was developed and fitted to WBC to compare WBC trends relative to letermovir and valganciclovir (
Figure 1). Patients receiving valganciclovir +/− filgrastim experienced a decrease in WBC by an average of −0.0113 K/uL/day. Following transition from valganciclovir to letermovir, the rate of decrease in WBC significantly improved to −0.0043 K/uL/day (
p < 0.0001,
Figure 1 and
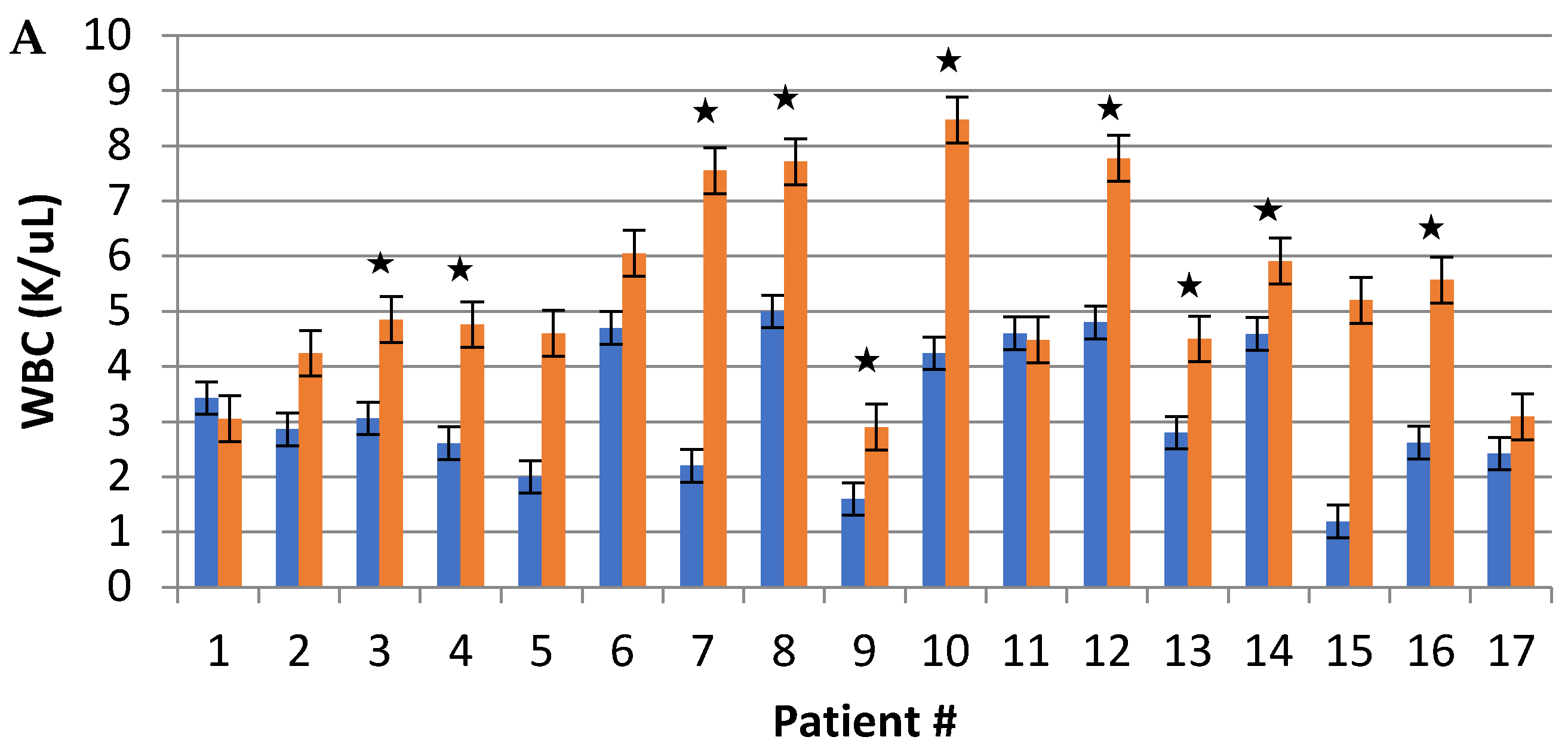
Table S2). After letermovir initiation, 15 patients (88.2%) demonstrated improvement in median WBC (
Figure 2A). Of the 15 patients who received filgrastim at any point, a decrease in the number of required filgrastim doses was noted in 13 patients after letermovir initiation, with the remaining two patients each receiving two doses of filgrastim within the first week following the switch to letermovir (
Table S3). Two patients did not require any filgrastim administration. Median time to leukopenia resolution after starting letermovir was 11.5 days (range 5–77 days,
Table 1).
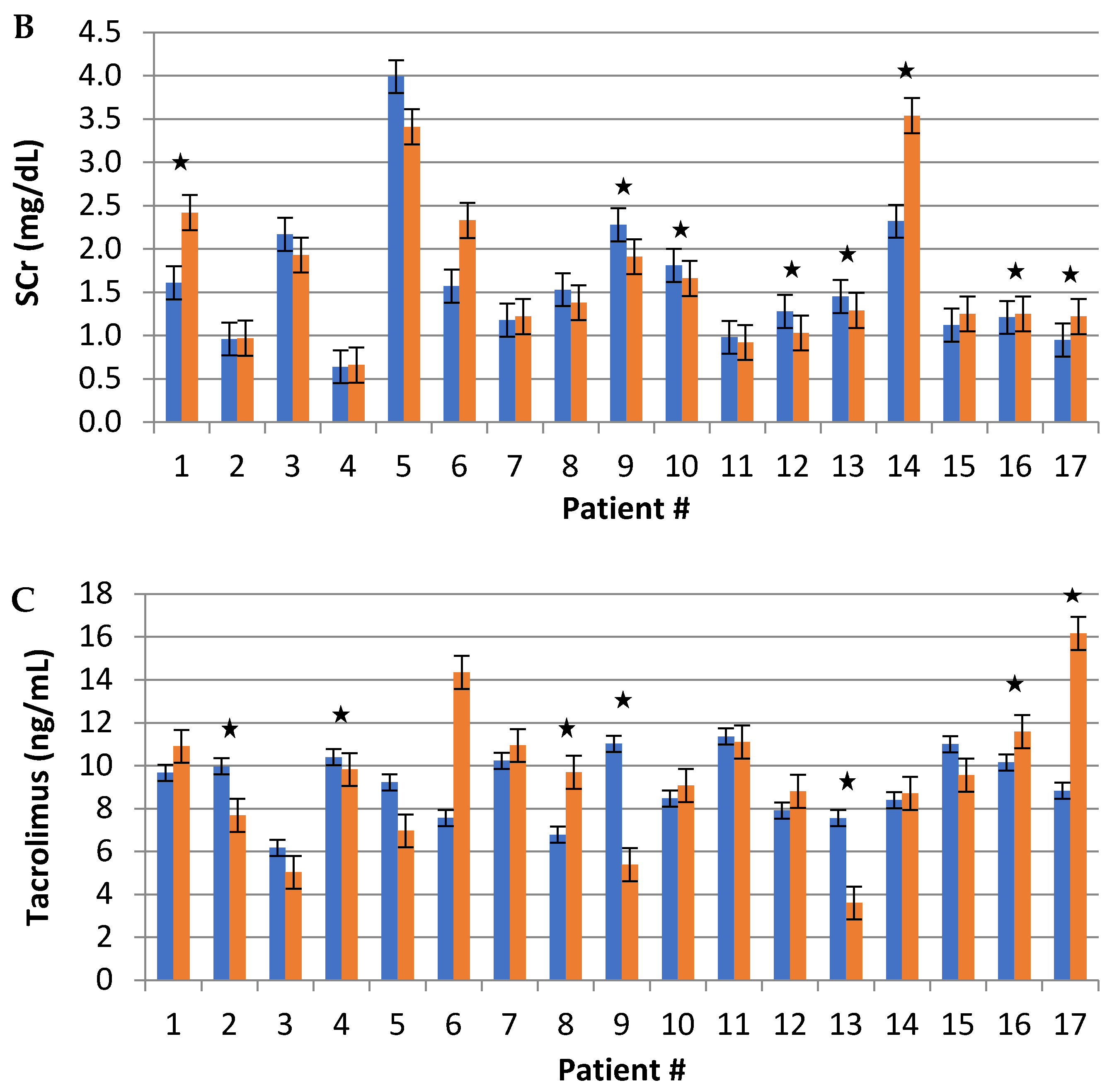
Eight (47.1%) patients experienced breakthrough CMV DNAemia while still on the gold-standard valganciclovir (
Figure S1), with six of these patients demonstrating CMV DNAemia in the 60 days immediately prior to the switch to letermovir (
Figure 3). All eight patients required enhanced antiviral treatment, with increased doses of valganciclovir in six patients and intravenous ganciclovir in the other two patients. Improvement in CMV DNAemia was noted in all cases before transition to letermovir, with all but patient #2 having undetectable CMV viral load at time of letermovir initiation. CMV DNAemia was noted in patient #2 for 100 days post-transplant while on valganciclovir prophylaxis. Once her serum CMV DNA level declined with the use of treatment-dose valganciclovir, she was transitioned to letermovir prophylaxis. At time of letermovir initiation, her CMV DNA level was 129 IU/mL.
Similar to valganciclovir, eight (47.1%) patients developed quantifiable breakthrough CMV DNAemia while on letermovir (
Figure S1). In 75% of these cases, the peak level of CMV DNAemia breakthrough was lower on letermovir than valganciclovir (
Figure 3 and
Figure S1). The median time to breakthrough CMV DNAemia after starting letermovir was 52 days (range: 4–376 days). Of the eight instances of letermovir breakthrough, two (#1 and #16) were de novo CMV DNAemia, and six (#2, #3, #6, #8 #12, and #13) were recurrent breakthrough CMV DNAemia events in patients who previously broke through valganciclovir. Episodes of de novo CMV DNAemia occurred later after letermovir initiation than did recurrent CMV DNAemia (de novo: median 69 days (range: 55–82 days) vs. recurrent: median 44 days (range: 4–376 days)). Peak de novo CMV DNAemia values were 476 and 22,090 IU/mL (patients #1 and #16, respectively). Patient #1 exhibited no clinical signs or symptoms of CMV disease and was maintained on letermovir with rapid resolution of CMV DNAemia for the duration of letermovir prophylaxis. Patient #16 self-discontinued letermovir after 57 days of treatment for unknown reasons, and his CMV viremia was determined to be a result of medication noncompliance rather than treatment failure. Patient #16 was treated with valganciclovir (900 mg oral twice daily) and then maintained on valganciclovir for prophylaxis (450 mg oral once daily, adjusted for renal function) once the serum CMV viral load was undetectable. In terms of recurrent CMV DNAemia, five of the six patients exhibited no clinical signs or symptoms of CMV disease, and CMV levels remained low. As a result, none required enhanced antiviral treatment, and all remained on letermovir prophylaxis. The remaining patient, #8, developed recurrent CMV DNAemia-associated gastrointestinal symptoms while on letermovir. This patient was treated with valganciclovir (450 mg oral twice daily, adjusted for renal function) and then transitioned to valganciclovir prophylaxis (450 mg oral once daily, adjusted for renal function) once the serum CMV viral load was undetectable.
Our institution’s protocol is to stop antiviral prophylaxis one year after lung transplant, irrespective of CMV serostatus. Letermovir was therefore discontinued in nine patients at 1 year post-transplant or when insurance approval of medication coverage ended, whichever came first. In four of these nine patients, CMV DNAemia was noted following stoppage of letermovir prophylaxis but not during letermovir use. One other patient, patient #1, received 13 months of letermovir prophylaxis and developed CMV DNAemia following discontinuation of antiviral prophylaxis. In all these patients, median time from stopping letermovir antiviral prophylaxis to CMV DNAemia onset was 42 days (range: 36–92 days,
Figure S1).
CMV resistance testing was not routinely performed in our institution except for in patients #2 and #8 who developed CMV DNAemia at 376 and 54 days, respectively, after starting letermovir and had persistently elevated levels of serum CMV DNA. In these patients, resistance testing revealed mutations at C325Y of CMV UL56 gene in patient #2 and C325F of CMV UL56 gene in patient #8. Patient #8 was transitioned to valganciclovir as mentioned above. Patient #2 was maintained on letermovir as her CMV viral load remained low without evidence of CMV disease.
Letermovir use was not associated with allograft dysfunction. Mean forced expiratory volume in 1 s (FEV1) of the group 60 days pre- and post-letermovir was 72% and 76% predicted, respectively. Mean FEV1 of the group both during letermovir therapy and at the end of the study period was 70% predicted. Mean forced vital capacity (FVC) of the group 60 days pre- and post-letermovir was 65% and 67% predicted, respectively. Mean FVC of the group during letermovir therapy and at the end of the study period was 63% and 64% predicted, respectively. None of these changes were statistically significant. All patients underwent routine rejection surveillance with transbronchial biopsy and peripheral blood screens for donor-specific antibodies. There was no evidence of acute cellular rejection, antibody-mediated rejection, or chronic lung allograft dysfunction in any patient during the study period.
No fungal infections were identified in patients while taking letermovir, and no patients discontinued letermovir due to side effects. There was a statistically significant increase in serum creatinine in four patients (23.5%), while four other patients (23.5%) demonstrated a significant decrease in serum creatinine after starting letermovir (
Figure 2B). Patient #6 developed acute kidney injury associated with high tacrolimus trough levels within 3 weeks of starting letermovir. Of note, this patient was not concurrently on an azole antifungal at the time of letermovir initiation. Two patients (11.8%) had statistically significant increases in serum tacrolimus trough levels, while five patients (29.4%) had significant decreases in serum tacrolimus trough levels while on letermovir (
Figure 2C). The lower tacrolimus trough levels in these five patients were intentional and due to reductions in tacrolimus dosing related to time from transplant and, in the cases of patients #9 and #13, addition of sirolimus to their immunosuppression regimen. No differences were noted in the number of tacrolimus dose adjustments required to maintain target trough levels in patients taking letermovir.
4. Discussion
Lung transplant patients are at increased risk of leukopenia from valganciclovir, a risk accentuated by other myelosuppressive agents required for allograft preservation [
9]. In an effort to minimize the risk of leukopenia in our patients due to valganciclovir, we utilized letermovir, a novel CMV antiviral, for prophylaxis in patients with valganciclovir-induced leukopenia. Consistent with a recent report [
8], letermovir was well-tolerated by our patients with relatively minimal side effects. Furthermore, the myelosuppressive effect of valganciclovir improved soon after withdrawal of the offending agent and transition to letermovir (median time to leukopenia resolution of 11.5 days). Most importantly, we found that letermovir exhibited better efficacy than valganciclovir in preventing CMV disease and similar efficacy in controlling asymptomatic CMV DNAemia.
In terms of CMV disease, eight patients (47%) developed CMV disease on valganciclovir prophylaxis necessitating enhanced antiviral therapy. In contrast, only two patients (11.8%) developed CMV disease requiring enhanced treatment while taking letermovir. Of these two cases, one was related to medication noncompliance rather than letermovir treatment failure, leaving only one patient (5.9%) with CMV disease while taking letermovir prophylaxis as prescribed. All patients with CMV disease were successfully treated with valganciclovir without further recurrence of CMV disease.
Consistent with a recent report [
10], letermovir had similar efficacy to the gold-standard valganciclovir in preventing CMV DNAemia breakthrough in our cohort. There were eight cases of quantifiable CMV breakthrough with each drug. Of these cases, six patients demonstrated breakthrough with both drugs. Whether CMV that breaks through valganciclovir prophylaxis is also more likely to break through letermovir prophylaxis is unknown, though it may be possible based on our findings. Furthermore, the fact that our cohort was selected from patients with valganciclovir-induced leukopenia may have artificially increased the rates of CMV breakthrough we observed. Alternatively, the detected CMV DNAemia during letermovir prophylaxis may simply be the result of an abortive infection as recently reported [
11]. We did not perform viral culture so we cannot know for sure, but this will be important to evaluate in future studies.
Several studies have reported a 10–12% CMV breakthrough rate with the gold-standard valganciclovir over 12 months of use in solid organ transplant recipients [
12,
13,
14]. While the rate of breakthrough CMV DNAemia with letermovir prophylaxis in lung transplant patients is not yet established, it should be noted that 75% of the patients who broke through letermovir had previously demonstrated CMV breakthrough of valganciclovir prophylaxis as well. In HCT patients on letermovir prophylaxis, approximately 38% developed clinically significant CMV infection requiring treatment [
8], much higher than what we observed in our cohort. In the majority of instances of letermovir breakthrough CMV DNAemia in our study, viral levels remained low, and letermovir was continued with spontaneous resolution of CMV DNAemia. The numerical viral load values that reliably predict CMV disease risk compared with asymptomatic infection are not well-defined. However, a previous meta-analysis indicated that high initial viral load and rapid rise in CMV levels are predictors of CMV disease [
15]. We felt that continuing letermovir prophylaxis was justified given the low levels of circulating CMV DNA, lack of a sharp increase in CMV DNA level, and the absence of any evidence of end organ dysfunction or any symptoms consistent with CMV disease.
Development of CMV resistance to letermovir is a concern and has been reported both in experimental and clinical settings [
16,
17,
18,
19,
20,
21]. Mutations conferring letermovir resistance most commonly map to genes encoding the viral terminase complex (UL56, UL51, and UL89), with mutations in UL56 being the most common [
17,
18]. In our cohort, we detected letermovir resistance in two subjects, both in the CMV UL56 gene, but we did not routinely check for resistance in the remaining subjects. To better evaluate whether a relationship exists between letermovir resistance and breakthrough viremia, future studies should include broader screening for viral resistance mutations. Interestingly, one of the two patients with letermovir resistance, patient #2, had cystic fibrosis (CF) and was not on pancreatic enzyme supplementation while on letermovir. As letermovir has been documented to be highly lipophilic, in disease states with impaired gastrointestinal absorption such as CF, letermovir absorption may be altered [
22,
23]. Further investigation is required to determine whether letermovir absorption is, indeed, impaired in CF patients and whether pancreatic enzyme supplementation improves letermovir absorption.
There is some concern that letermovir may possess a low genetic barrier to resistance as seen in some in vitro studies [
17,
18]. Clinically, emergence of resistance has been seen with use of letermovir as salvage therapy for ganciclovir- or valganciclovir-resistant CMV infections [
19,
20,
24]. Whether the risk of letermovir resistance seen in treatment of CMV infection extends to its use for prophylaxis is less clear. Interestingly, a recent report indicated that in HCT patients, the emergence of resistance during prophylaxis with letermovir is relatively low [
21]. Nevertheless, further research investigating the rate of resistance emergence in treatment vs. prophylaxis with letermovir is warranted.
Drug interactions, especially co-administration of letermovir with calcineurin inhibitors (CNI) and azole antifungals, are also a concern due to letermovir’s metabolism through the cytochrome P450 system. Letermovir confers moderate inhibition of cytochrome P450 3A4 (CYP3A4) and induction of CYP2C9 and CYP2C19 and is a substrate of p-glycoprotein [
4,
25,
26,
27]. In pharmacokinetic trials of healthy adults, letermovir resulted in higher tacrolimus and lower voriconazole plasma levels [
25,
26]. In our cohort, one patient (#6) who was not on an azole antifungal had a dramatic increase in tacrolimus trough level along with a rise in serum creatinine within 3 weeks of starting letermovir. We did not observe an abrupt change in plasma tacrolimus levels or the need for more frequent tacrolimus dose adjustments following letermovir initiation in patients who were concurrently taking both tacrolimus and an azole antifungal. Although robust in vivo data of letermovir–CNI–azole interactions in transplant recipients do not exist, a small observational study in HCT patients demonstrated higher serum CNI concentrations in subjects receiving co-administered letermovir [
28]. The authors also suggested voriconazole therapeutic drug monitoring while on letermovir. We hypothesize that concurrent azole antifungal therapy may abrogate letermovir’s effect on tacrolimus metabolism; however, due to the small number of patients in our study, the drug effects may not be representative. Based on our experience, it is imperative to closely monitor anticipated drug interactions and serum creatinine and tacrolimus levels in patients on letermovir, especially if other agents such as azole antifungals are added to or removed from the treatment regimen.
Our study has some limitations. This was a single-center, retrospective study, and given the small sample size, rare side effects may have been missed. Our cohort was selected based on valganciclovir-induced leukopenia, patients who may be more susceptible to CMV, and therefore the true incidence of breakthrough DNAemia may have been overestimated. The observational nature of the study is another limitation. In the absence of randomization and comparison with a control arm, it is difficult to compare the incidence of CMV DNAemia on letermovir with standard valganciclovir therapy. While most CMV PCR testing was completed at our hospital laboratory, some testing was performed at local community laboratories with assays that had varying thresholds for CMV DNA detection. For example, at our institution the threshold for CMV PCR detection is 50 IU/mL while an outside laboratory using a different assay had a threshold for detection of 200 IU/mL. This variability could have led to under-reporting of low-level serum CMV DNA. Additionally, letermovir was initiated in patients at varying times post-transplant, with some patients in the outpatient setting and others still hospitalized following transplant. As a result, there was variability in severity of illness among patients, which may have impacted the risk of CMV DNAemia and/or CMV disease. Finally, letermovir is a fairly new drug on the market, and, in certain cases, we faced significant barriers limiting its use including cost and access to the drug. Letermovir is not universally covered by insurance, and in cases where it is covered, high copays and limitations on the number of days covered make its routine use challenging. Despite these limitations, this is the largest study to date in lung transplantation to evaluate the efficacy and tolerability of letermovir for CMV prophylaxis. While we believe our study captures the real-world challenges faced by transplant physicians in managing these complex patients, a large multicenter prospective trial is needed to confirm our findings.
In conclusion, our data suggest that letermovir is a generally safe and effective alternative to valganciclovir for CMV prophylaxis in lung transplant recipients unable to tolerate the standard of care valganciclovir due to leukopenia. Letermovir is well-tolerated with a favorable side effect profile when used in conjunction with other myelosuppressive agents. Close monitoring for drug interactions is necessary, and calcineurin inhibitor dose adjustment may be required based on the pharmacokinetics of other co-administrated drugs such as voriconazole. Further studies are warranted to confirm letermovir’s safety and efficacy in CMV prophylaxis in solid organ transplantation.









{kind=link}
{kind=link}
{kind=link}
{kind=link}