1. Introduction
Mullerian malformations are a group of congenital abnormalities that affect the development of the reproductive system in females. These malformations occur due to an incomplete or abnormal fusion of the two Mullerian ducts, which form the uterus, fallopian tubes and upper part of the vagina during fetal development. The prevalence of uterine anomalies in the unselected population is approximately 5.5% [
1]. One type of Mullerian malformation is the didelphic uterus, characterized by two separate uterus cavities with their own cervix and vaginal canal. Each uterus cavity may have its own fallopian tube and ovary [
2].
Diagnosis of uterus didelphys typically occurs during a routine gynecological exam. Further diagnostic tests, such as an ultrasound or MRI, may be performed to confirm the diagnosis and assess the size and shape of the uteri.
In the general population, the true incidence of Mullerian defects is not accurately known. In a review of the prevalence of different types of uterine malformations performed by Grimbizis et al., the mean incidence of uterus didelphys was found to be at 8.3% of all Mullerian defects [
3]. Didelphic uterus is associated in 15–30% of cases with unilateral anomalies, i.e., obstructed hemivagina and ipsilateral renal agenesia. This condition, initially described in 1971 by Herlyn and Werner, is known as Herlyn–Werner–Wunderlich syndrome, also identified as “obstructed hemivagina with uterus didelphys and ipsilateral renal anomaly” (OHVIRA).
The most common signs and symptoms are pain, dysmenorrhea, a palpable mass in the lower abdomen secondary to haematocolpos and/or haematometra and recurrent urinary tract infections.
There are few sporadic case reports in the literature about this condition and its related management, indicating its rarity.
We present a case of symptomatic Herlyn–Werner–Wunderlich syndrome in a symptomatic 19-year-old patient. A two-dimensional/three-dimensional ultrasound and abdominopelvic MRI were performed to confirm the diagnosis. The patient was successfully treated with a laparoscopic-assisted hysteroscopic vaginal septum resection using 5 Fr hysteroscopic bipolar electrodes.
2. Case
A 19-year-old Chinese woman G0P0 was presented to the Emergency Department (ED) of Obstetrics and Gynecology Unit with complaints of increasing dysmenorrhea and pain in the right iliac fossa, associated with foul-smelling discharge.
The anamnesis was negative for significant pathologies and for previous surgery. The patient had undergone a single routine gynecological check-up some years before with no abnormal findings. She had menarche at 12 years and a normal menstrual cycle of 5/28 days.
She had regular sexual activity, and her menstruations were described as regular in terms of quantity and duration, characterized by intense dysmenorrhea (VAS 9/10) treated with non-steroidal inflammatory drugs.
The specular examination showed a regular vaginal canal, a single portio with normal epithelization and slightly malodorous discharge.
Vaginal examination showed a swelling at the level of the upper-third of the left vaginal wall. The vagina appeared continuous, with no detectable septa.
Transabdominal/transvaginal ultrasound revealed a didelphys uterus with two fully developed unfused cervices and two vaginas, one of which (the left one) was blind, inaccessible from the outside and full of blood material. The imaging also showed an associated urinary tract malformation characterized by left renal agenesia, ipsilateral to the vagina presenting hematocolpo.
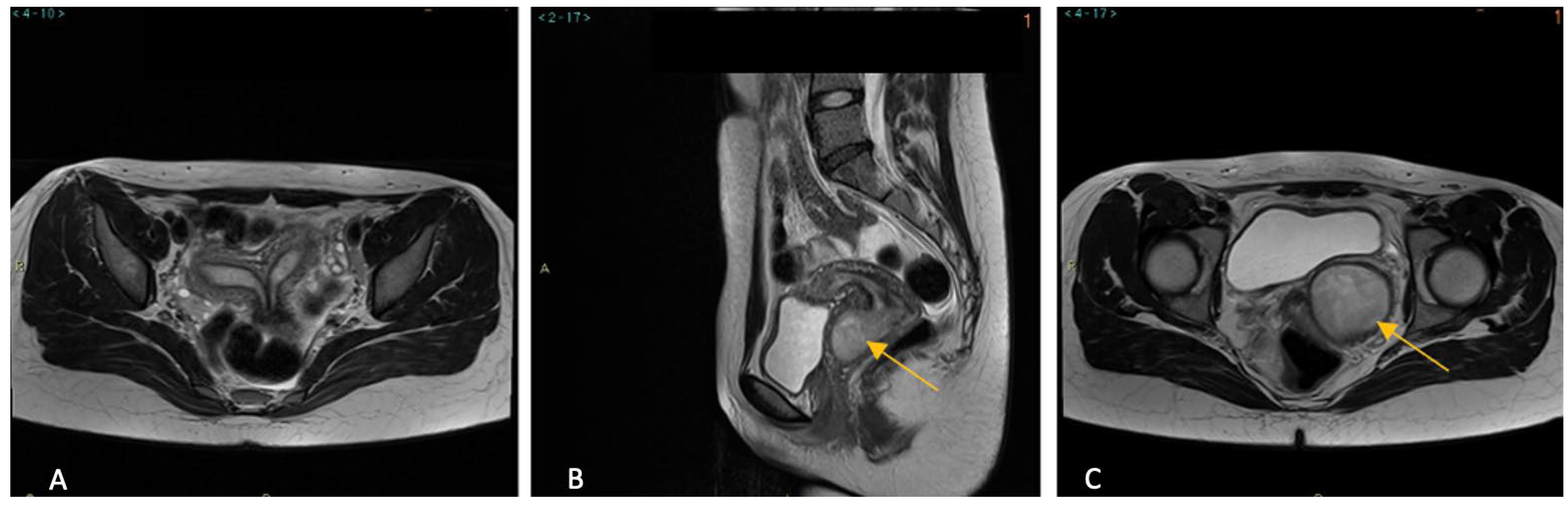
CT scan and MRI confirmed the findings. In addition, MRI clearly demonstrated two vaginal cavities. The right hemivagina was seen to communicate with the right cervix and corresponding uterine horn. Instead, the left hemivagina was markedly distended, suggestive of a left hematocolpos (
Figure 1). No evidence of focal implants of endometriosis were detected. All these findings were consistent with obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome.
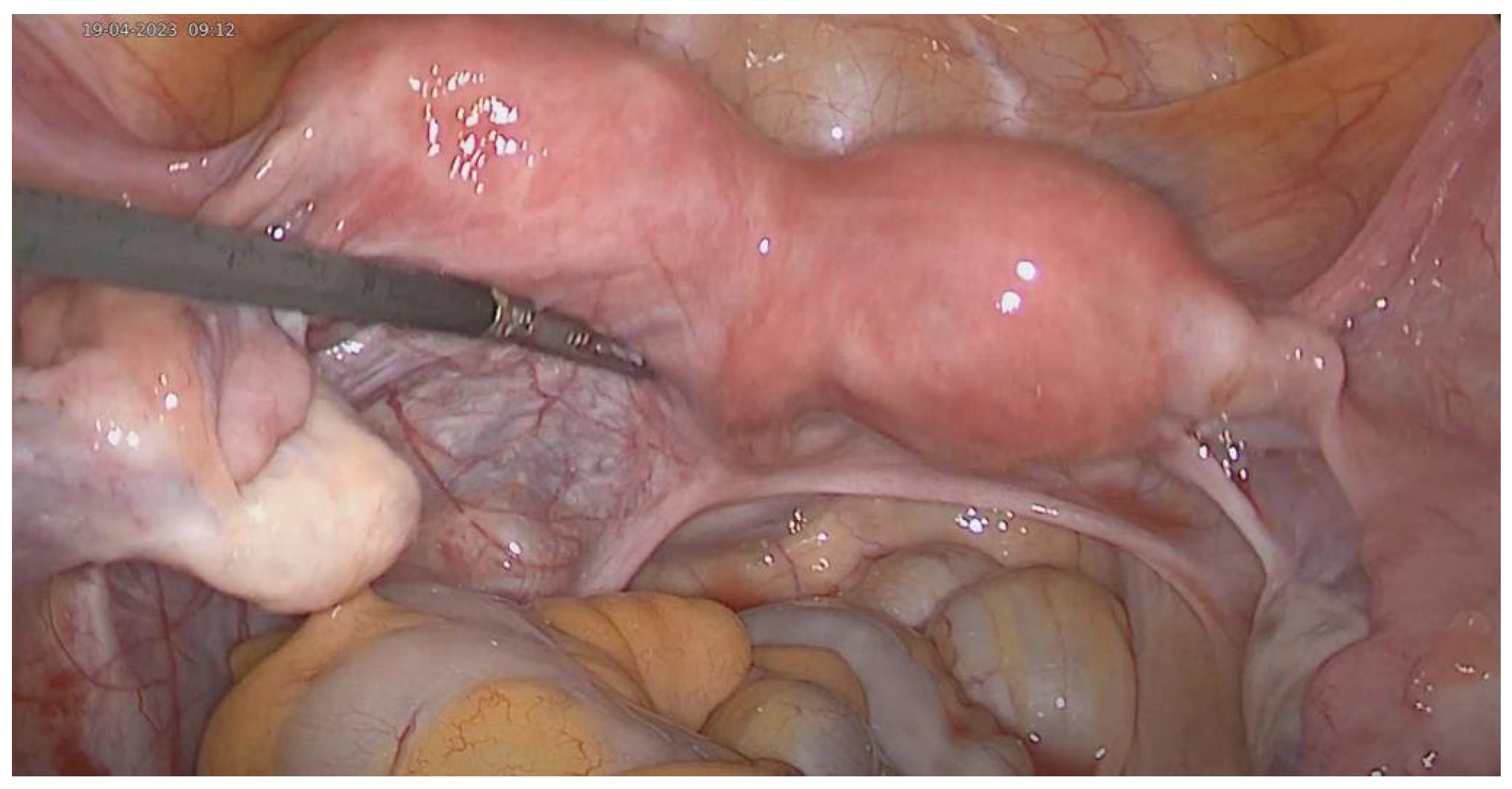
The patient underwent diagnostic laparoscopy prior to the hysteroscopic approach (
Figure 2). Upon inspection of the pelvic cavity, a bicornuate uterus with symmetric equally sized uterine bodies, bilateral normal-shaped tubes and regular ovaries were observed. There was no evidence of formations attributable to cysts or inflammatory collections or other macroscopically visible lesions in the abdomen.
A Bettocchi hysteroscope was introduced through vaginoscopy. The vagina, the portio of the right hemiuterus and the right cervical canal appeared regular. The right uterine hemicavity was normal and only the right tubal ostium was visible.
During vaginoscopy, a longitudinal incision of about 2 cm was made using a bipolar loop in the vaginal wall, laterally to the left of the cervix of the right hemiuterus. The cervical canal of the left hemiuterus was crossed with the hysteroscope, which appeared regular. Similar to the right hemicavity, only the left tubal ostium was visible. The endometrium showed a micro-papillary pattern, neovascularized and friable to the touch. A wide biopsy was performed using 5 Fr mechanical instruments.
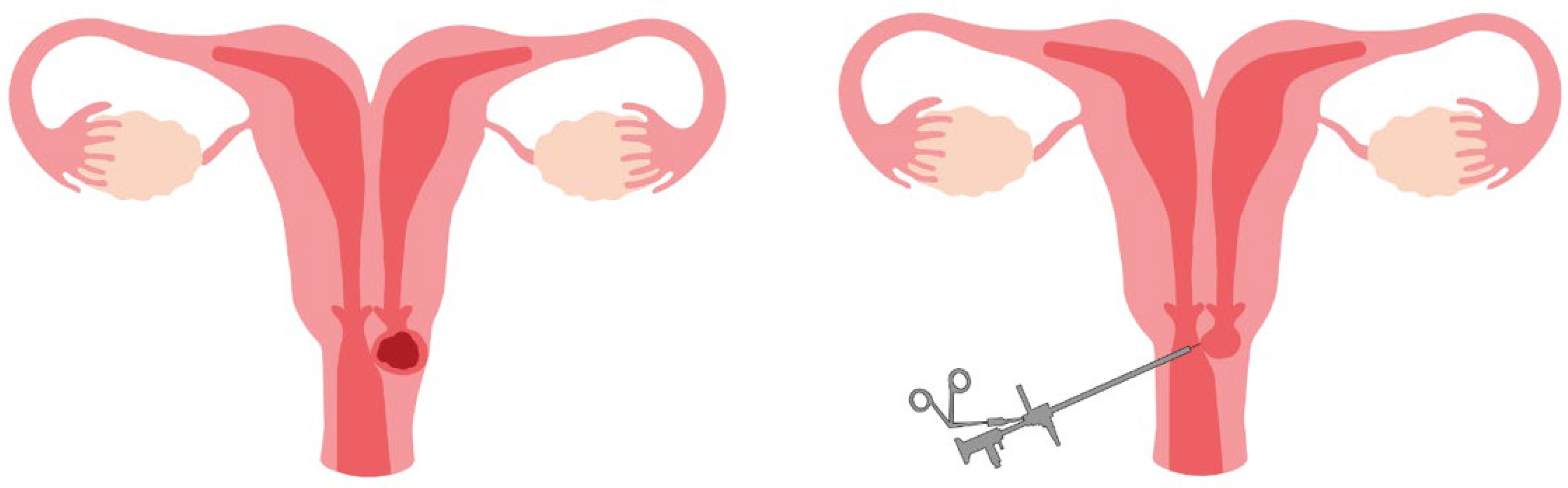
Using the hysteroscope, the vaginal recess about 3 cm to the left of the cervix of the left hemiuterus was visualized through the continuous vaginal solution (
Figure 3). Part of the vaginal wall (about 1 cm) forming the above-mentioned recess was resected using a monopolar electrode and sent for histological examination. A 10 cc cuffed Foley catheter was placed into the cavity of the residual vaginal recess to assure patency.
The patient was discharged after three days of hospitalization with a regular postoperative course and no pelvic pain. The vaginal foley catheter was left in place until reassessment.
The patient returned for a follow-up visit 14 days after the initial surgical procedure; the vaginal foley catheter had been spontaneously extruded the day before (13 day after surgery).
Upon gynecologycal examination, there were no atypical discharges; the cervix of the right hemiuterus and suture points were visible on the left vaginal wall, corresponding to the created continuous solution of the vaginal recess. Histological results were negative for malignancy and other conditions.
After 12 months postoperative, the patient was asymptomatic with regular, unpainful menstrual cycles.
3. Summary
Herlyn–Werner–Wunderlich syndrome, also known as “obstructed hemivagina with uterus didelphys and ipsilateral renal anomaly” (OHVIRA), is a Mullerian malformation consisting of an obstructed hemivagina in a didelphic uterus, usually associated with ipsilateral renal and ureteral agenesis.
In 1971, Herlyn and Werner initially described a condition consisting of renal agenesis and an ipsilateral blind hemivagina. Five years later, Wunderlich reported a case featuring right renal aplasia alongside a bicornuate uterus and a normal vagina, where there was an isolated hematocervix due to a lack of communication between the right hemiuterus and the vagina.
Interestingly, these conditions give an input to better understand the embryological origin of the upper vaginal portion. In fact, according to the classic theory, the uterus and upper vagina would originate from the paramesonephric (Mullerian) ducts, which fuse to form a single and midline primordial uterovaginal canal [
4]. However, this theory is not appropriate to explain the complex Mullerian malformation associated with renal anomalies.
Thus, another theory hypothesized that the vagina forms entirely from the cavitation and fusion of the sinuvaginal bulbs, i.e., enlargements of the caudal segments of the mesonephric ducts (Wolffian).
In OHVIRA syndrome, the developmental abnormality of ipsilateral mesonephric ducts results in the failure of its opening into the uro-genital sinus, leading to obstruction of the hemivagina and the absence of the ureteral bud, thereby resulting in ipsilateral renal agenesis.
From a clinical perspective, numerous classifications for female genital tract malformations have been proposed. OHVIRA syndrome is categorized as class III in the American Fertility Society (AFS) of congenital uterine anomalies, typically involving uterine duplication, though a complete longitudinal vaginal septum (Class V) occurs in 75% of cases of this anomaly [
5]. The ESHRE/ESGE classification system describes OHVIRA with an embryological defect image as U3b C2 V2, indicating a ‘complete bicorporeal, with double cervix and longitudinal obstructing vaginal septum’ [
1].
In 2015, Zhu et al. proposed a new classification for this syndrome based on the clinical characteristics that differ significantly between the completely and incompletely obstructed vaginal septum [
6]. Classification 1 (1.1—with blind hemivagina; 1.2—cervicovaginal atresia without communicating uteri) describes case of a completely obstructed hemivagina clinically characterized by a large distended hematocolpos that causes acute onset of abdominal pain, fever and vomiting. Differently, in Classification 2 (2.1—partial resorption of the vaginal septum; 2.2—with communicating uteri), due to limited communication between the two vaginas, the vaginal cavity behind the septum is incompletely obstructed. In these cases, symptoms often appear several periods after menarche and ascending genital system infection can be present.
In a recent multicenter study including 255 HWWS patients, Song et al. reported that 80.8% presented with dysmenorrhea or periodic lower abdominal pain, and 45.5% complained of vaginal bloody/purulent discharge [
7].
In a large institutional case series of 87 patients with double uterus, unilateral cervico-vaginal obstruction and ipsilateral renal anomalies, Fedele et al. found an incidence of didelphys uterus in 77% of patients (67/87). Of these 67 patients, 63 (72%) presented an obstructed hemivagina, not communicant, communicant and septatae in 49, 11 and 3 cases, respectively [
8]. This study, performed in a referral center for the treatment of genital anomalies, showed the different possible variants of the syndrome, increasing the awareness of heterogeneity of the anatomic variants among health-care providers. For example, although the presence of didelphys uterus with unilateral renal agenesis associated with a pelvic hematic mass is commonly associated with an obstructed hemivagina (72% of cases), there are also rare variants of this syndrome that must be considered (e.g., unilateral cervical atresia) with all their therapeutic implications. If, for the classic variant, the preferred surgical approach is the full hysteroscopic excision of the vaginal septum, for rare variants, a more complex surgical approach could be required.
In our case, since MRI confirmed our diagnostic suspect, we planned surgical management performing a single-stage procedure. Ultrasonography was performed before surgery to see the extent of the hematocolpo and a histological examination was also requested to rule out malignancy. MRI findings were subsequently confirmed intraoperatively.
Ultrasound is a reasonable initial imaging study for the investigation of anatomic anomalies. However, MRI has proven to be the golden-standard technique for diagnosing Mullerian abnormalities; it provides useful detailed information for preoperative planning regarding uterine morphology, its continuity with each vaginal channel, and the nature of the uterovaginal content. Ultrasound and MRI can also contribute to the early and accurate diagnosis of endometriosis. A previous study showed that the rate of endometriosis among patients with HWWS was 17–19% [
9].
Due to the anatomical distortion from the hematocervix and chronic inflammation, as well as the narrow vagina in adolescent girls, a laparoscopically assisted hysteroscopical excision of the septum was selected. While the optimal treatment of HWWS remains debated, most experts agree that an explorative laparoscopy with vaginal septotomy and the drainage of the hematocervix is enough to restore the obstruction for a blind hemivagina, avoiding hemi-hysterectomy.
The use of laparoscopy to assess exact uterine anatomy at the time of resection of the vaginal septum has also been discussed; although some authors concluded that its use is not essential to management, this type of surgical procedure also allowed us to perform a successful and safe treatment. Indeed, laparoscopy allows for the direct visualization of the external structures of the uterus, fallopian tubes and ovaries, also examining any associated pelvic pathology, such as endometriosis and/or other pelvic abnormalities. The combination of laparoscopy and hysteroscopy provides information for the anatomical status of the vagina, cervical canal, uterine cavity, tubal ostia, external contour of the uterus and the intra-peritoneal structures for diagnosis and differential diagnosis.
In a retrospective case review of patients diagnosed with HWWS from 2010 to 2017, Tan et al. showed that most prepubertal patients with HWWS do not need early gynecological surgery [
10]. The authors also recommended pelvic ultrasound screening for HWWS in patients with renal agenesis or multicystic dysplastic kidney.
In cases of pregnancy, there are increased rates of infertility associated with HWWS. It has also been associated with preterm labor, with preterm premature rupture of membranes (pPROM) and with fetal abnormal presentation. Additionally, didelphys uterus is associated with fetal growth restriction.


 ,
, 
{kind=link}
{kind=link}
{kind=link}