
Biophysical Markers of Suspected Preeclampsia, Fetal Growth Restriction and The Two Combined—How Accurate They Are?

 , , ,
, , ,
Abstract
:1. Introduction
2. Sample and Methods
2.1. Sample
2.2. Immunodiagnostic Test of Angiogenic Markers
2.3. Biophysical Markers
2.3.1. Blood Pressure
2.3.2. Endo PAT
2.3.3. Ultrasound
2.4. Clinical Definition of the Study Groups
2.5. Statistical Analyses
3. Results
3.1. Cohort Characteristics
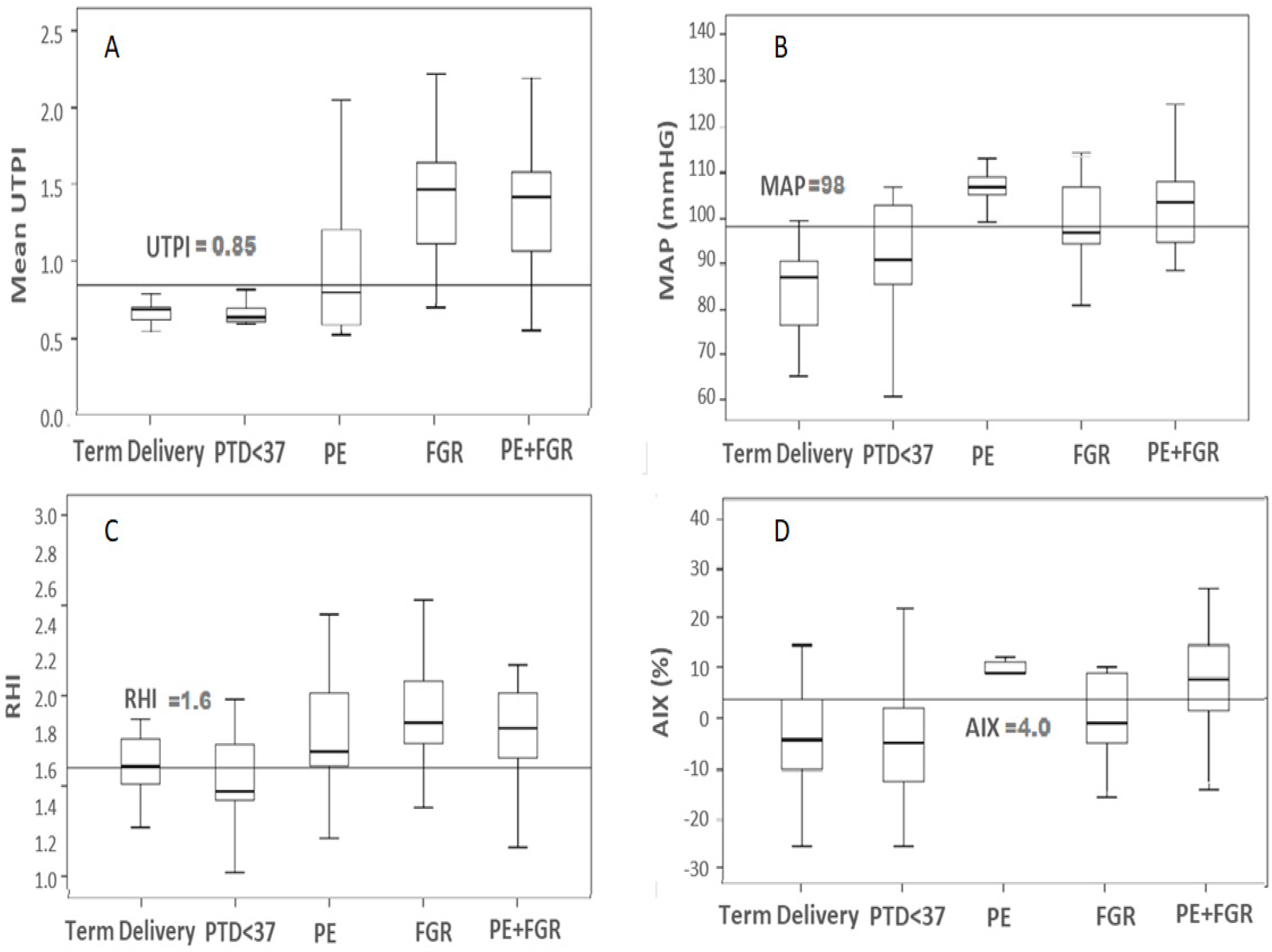
3.2. Biophysical Marker, Medians and Inter Quartiles for the Outcome Groups
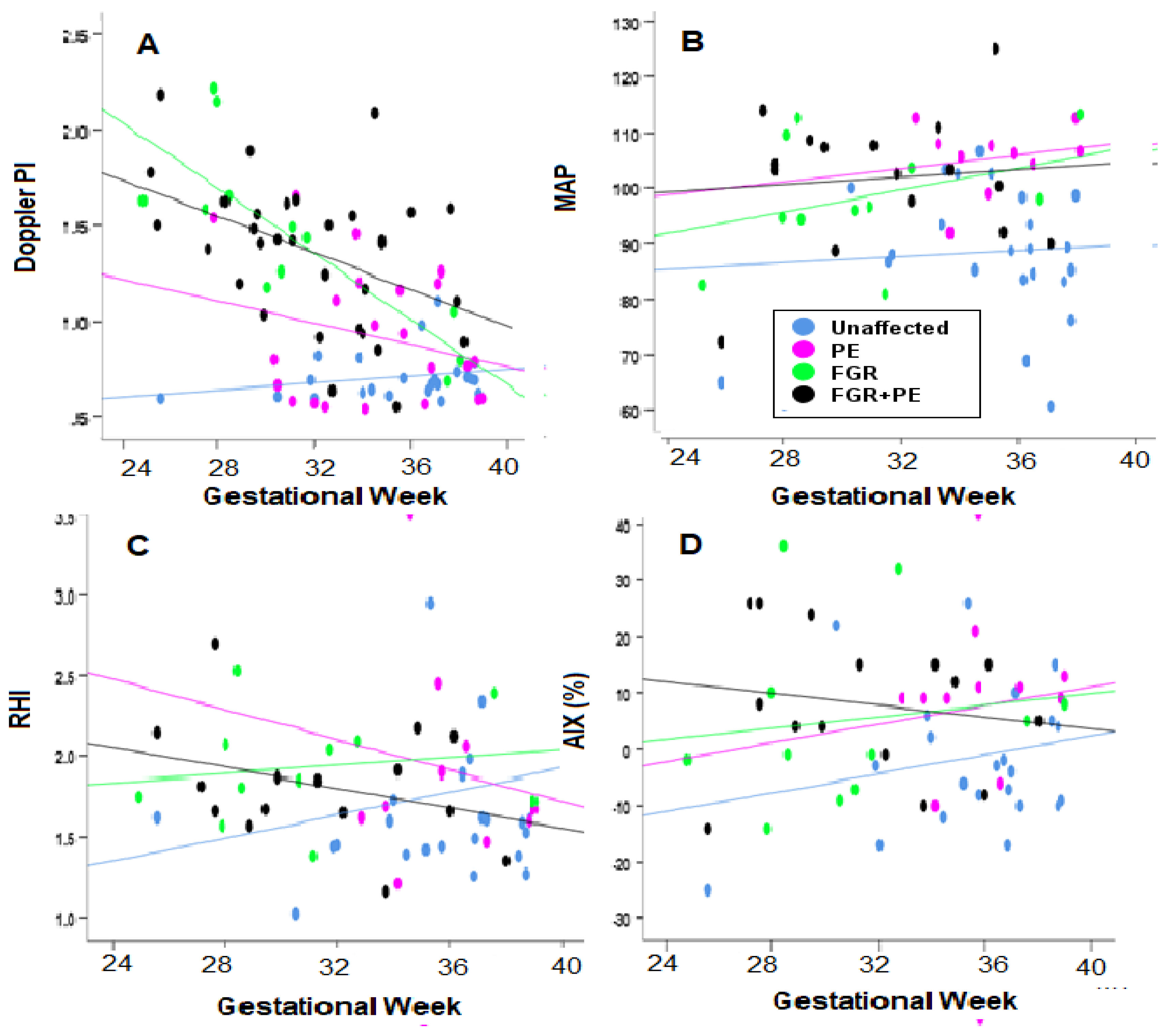
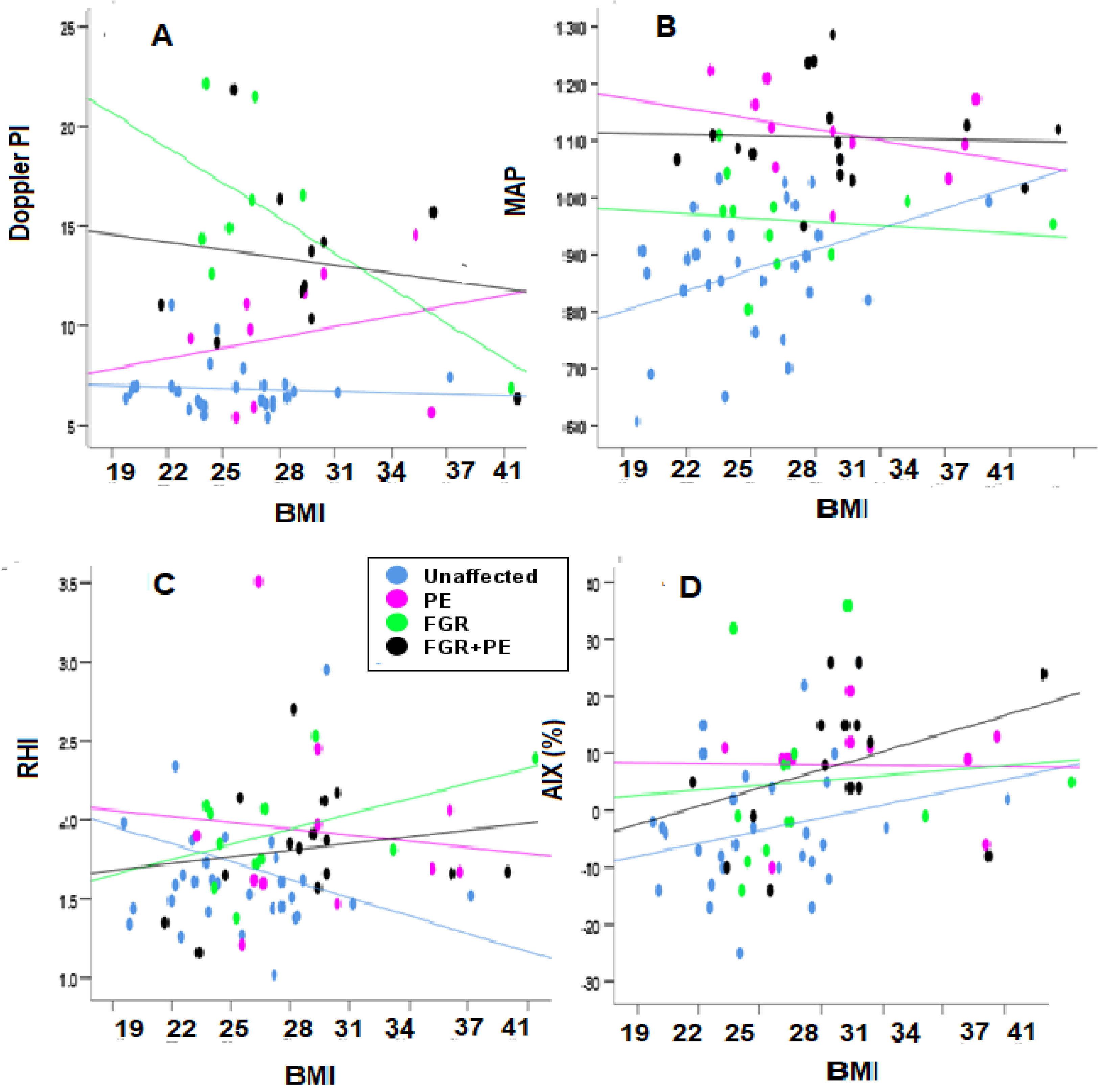
3.3. Spearman’s Coefficient of the Biophysical Markers against Gestational Week and Body Mass Index
3.3.1. Gestational Week (GA)
3.3.2. Body Mass Index (BMI)
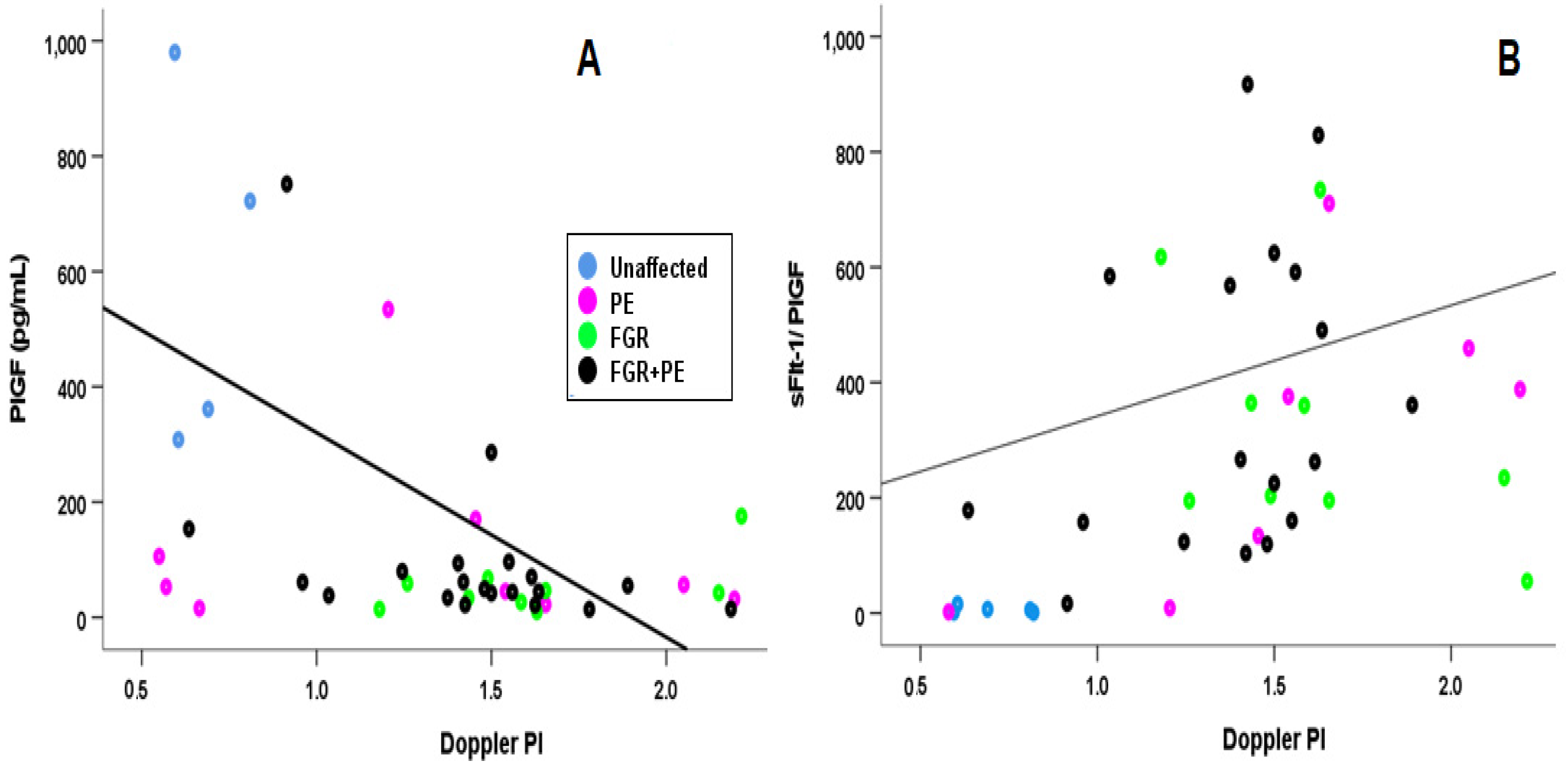
3.3.3. Angiogenic Markers
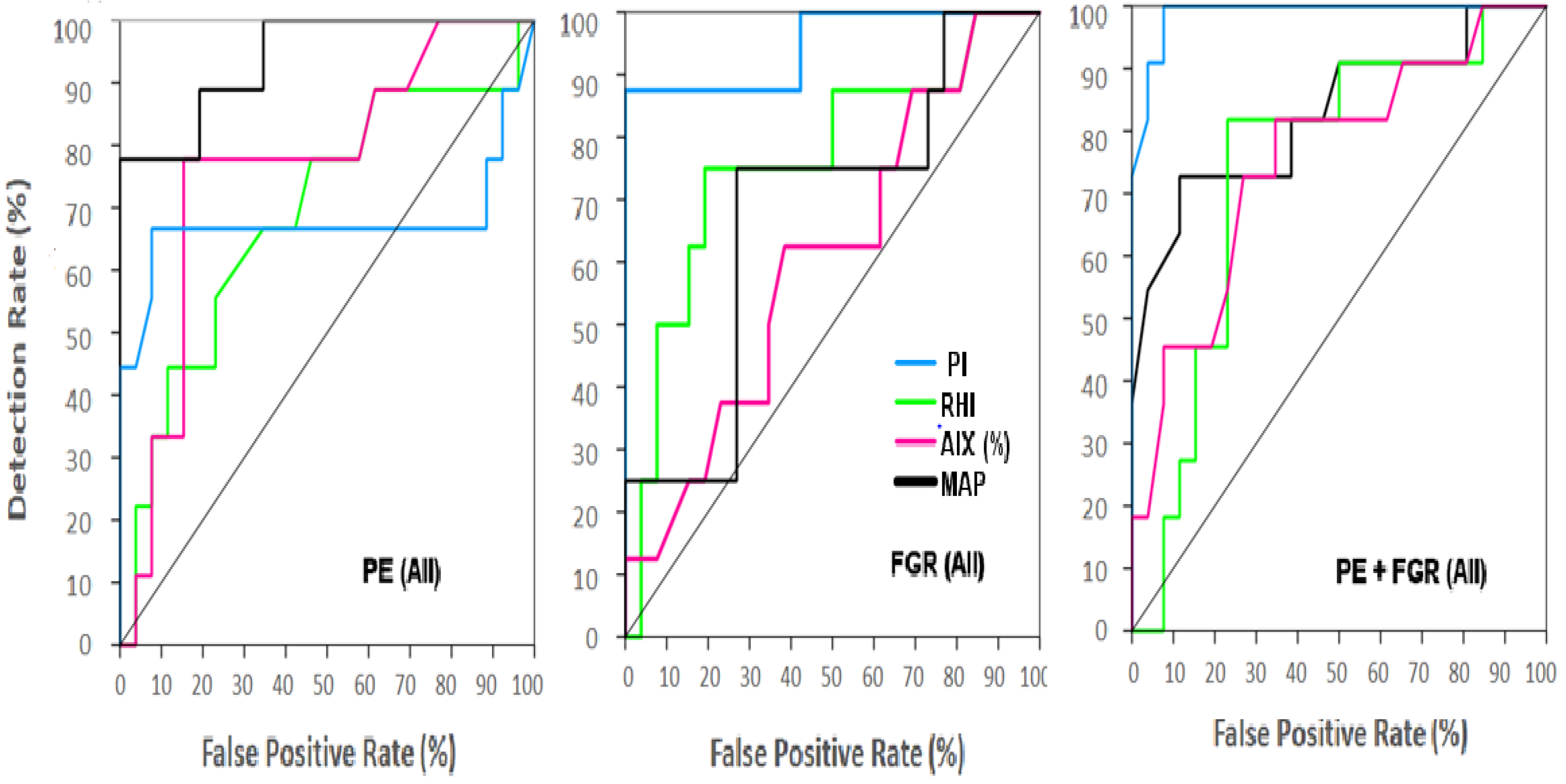
3.4. AUC Analysis
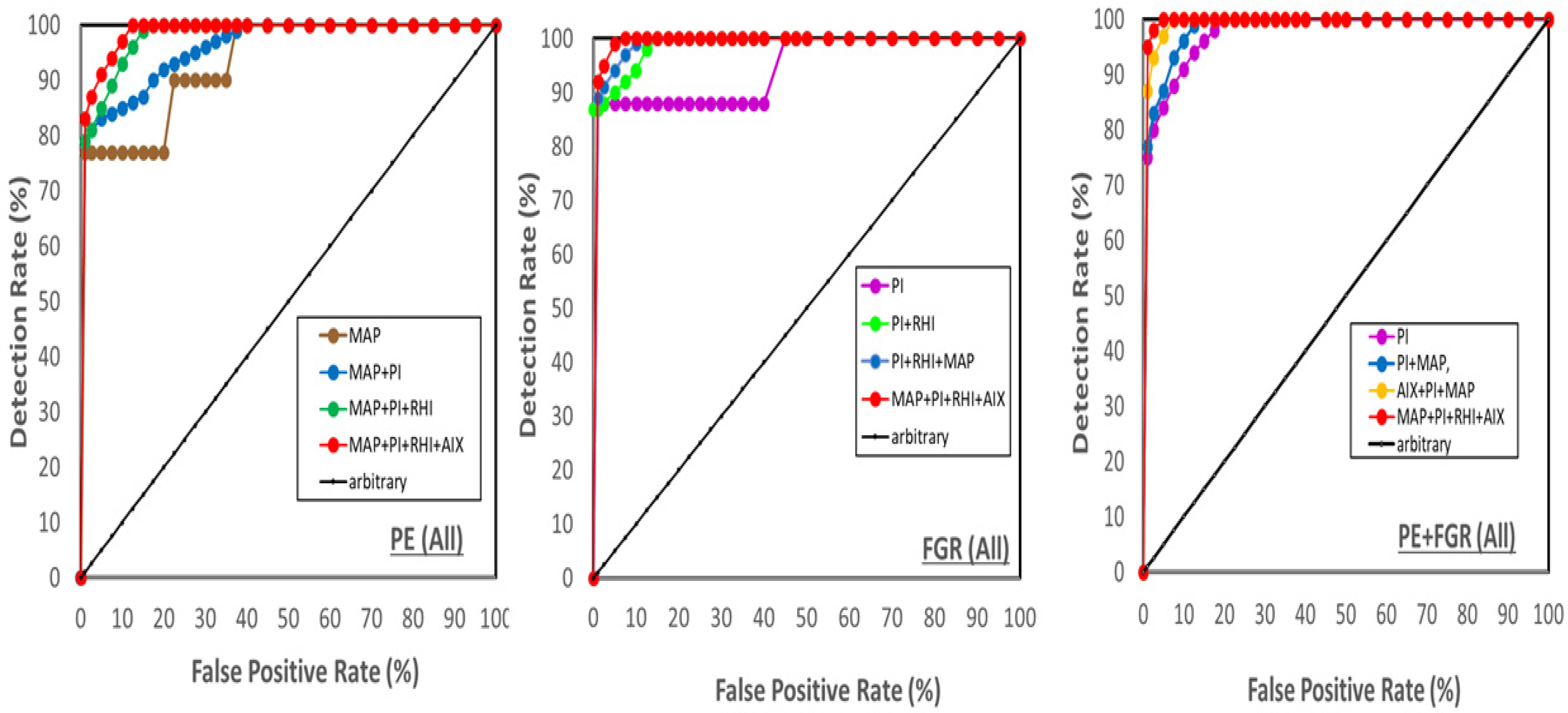
Combined Biophysical Marker Analysis
3.5. Multiple Regression
3.5.1. All Cases
- MAP = 92.82 − 0.41 × MA + 0.20 × GA + 19.31 × PE + 12.63 × FGR +17.33 × (FGR + PE)
- UtA PI = 2.42 + 0.01 × MA − 0.05 × GA + 0.17 × PE + 0.47 × FGR + 0.44 × (FGR + PE)
- RHI = 1.51 + 0.01 × MA − 0.01 × GA + 0.19 × PE + 0.19 × FGR + 0.05 × (FGR + PE)
- AIX = 2.36 − 0.19 × MA + 0.01 × GA + 11.58 × PE + 8.71 × FGR + 12.19 × (FGR + PE)
3.5.2. Early Cases (<34 wks of Gestation) (Equations Not Shown)
- MAP: R2 = 0.46, F(6,63)= 6.16 (p < 0.001), β’s = 0.49, 0.29 and 0.38 for PE, FGR and PE + FGR, respectively, p < 0.001 for any.
- UtA Doppler PI: R2 = 0.45, F = 7.29, p < 0.001, β’s = 0.62 for PE + FGR, and non-significant for other complications. (p < 0.001).
- AIX: R2 = 0.27, F = 2.63 and p < 0.05, and β = 0.38 and 0.35 for PE and PE + FGR (p < 0.001) but insignificant for FGR alone.
- RHI: R2 = 0.1703, F = 1.52 and all β’s were non-significant for any of the complications.
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACOG | American College of Obstetricians and Gynecologists |
| AIX (%) | Augmentation index (percent). |
| APGAR | Newborn score of Appearance (skin color), Pulse (heart rate), Grimace (reflex irritability), Activity (tone), and Respiration |
| AUC- | Area under the c of the receiver operation characteristic curve |
| BMI | Body mass index |
| BP | Blood pressure |
| dBP | diastolic blood pressure |
| DR | Detection rate (sensitivity) |
| FGR | Fetal growth restriction |
| FPR | False positive rate (1-specificity) |
| ISSHP | International Society for the Study of Hypertension Disorders in Pregnancy |
| ISUOG | International Society for Ultrasound in Obstetrics and Gynecology |
| IVF | In-vitro fertilization |
| MAP | Mean arterial blood pressure |
| MCA | Middle cerebral artery |
| MoM | Multiples of the medians |
| NICE | National Institute of Clinical Excellence |
| NPV | Negative predictive value |
| PE | Preeclampsia |
| UtA PI | Uterine artery pulsatility index assessed by Doppler |
| PPV | Positive predictive value |
| PlGF | Placental growth factor |
| PTD | Preterm delivery |
| sFlt-1 | Soluble FMS (oncogene for Feline McDonough Sarcoma) like tyrosine kinase 1 |
References
- Chappell, L.C.; Duckworth, S.; Seed, T.; Griffin, M.; Myers, J.; Mackillop, L.; Simpson, N.; Waugh, J.; Anumba, D.; Kenny, L.C.; et al. Diagnostic accuracy of placental growth factor in women with suspected preeclampsia—A prospective multicenter study. Circulation 2013, 128, 2121–2131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verlohren, S.; Dröge, L.-A. The diagnostic value of angiogenic and antiangiogenic factors in differential diagnosis of preeclampsia. Am. J. Obstet. Gynecol. 2020, 226, S1048–S1058. [Google Scholar] [CrossRef] [PubMed]
- Bello, N.A.; Woolley, J.J.; Cleary, K.L.; Falzon, L.; Alpert, B.S.; Oparil, S.; Cutter, G.; Wapner, R.; Muntner, P.; Tita, A.T.; et al. Accuracy of Blood Pressure Measurement Devices in Pregnancy. Hypertension 2018, 71, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Mayrink, J.; Souza, R.T.; Feitosa, F.E.; Rocha Filho, E.A.; Leite, D.F.; Vettorazzi, J.; Calderon, I.M.; Costa, M.; Kenny, L.; Baker, P.; et al. Mean arterial blood pressure: Potential predictive tool for preeclampsia in a cohort of healthy nulliparous pregnant women. BMC Pregnancy Childbirth 2019, 19, 460. [Google Scholar] [CrossRef]
- Tagetti, A.; Fava, C. Diagnosis of hypertensive disorders in pregnancy: An update. J. Lab. Precis. Med. 2020, 5, 8. Available online: https://jlpm.amegroups.com/article/view/5239/html (accessed on 20 January 2020). [CrossRef]
- Wojtowicz, A.; Zembala-Szczerb, M.; Babczyk, D.; Kołodziejczyk-Pietruszka, M.; Lewaczynska, O.; Huras, H. Early- and Late-Onset Preeclampsia: A Comprehensive Cohort Study of Laboratory and Clinical Findings according to the New ISHHP Criteria. Int. J. Hypertens. 2019, 2019, 4108271. [Google Scholar] [CrossRef]
- Magee, L.A.; Brown, M.A.; Hall, D.R.; Gupte, S.; Hennessy, A.; Karumanchi, S.A.; Kenny, L.C.; McCarthy, F.; Myers, J.; Poon, L.C.; et al. The 2021 International Society for the Study of Hypertension in Pregnancy classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2021, 27, 148–169. [Google Scholar] [CrossRef] [PubMed]
- WHO. Managing Complications in Pregnancy and Childbirth. Available online: http:///www.who.int/publications/i/item/9789241565493 (accessed on 1 February 2017).
- American College of Obstetricians and Gynecologists. Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin, Number 222. Obstet. Gynecol. 2020, 135, e237–e260. [Google Scholar] [CrossRef]
- Hypertension in Pregnancy: Diagnosis and Management NICE Guideline [NG133]. Published Date: 25 June 2019. Available online: https://www.nice.org.uk/guidance/ng133/resources/hypertension-in-pregnancy-diagnosis-and-management-pdf-66141717671365 (accessed on 25 June 2019).
- Kumer, K.; Premru-Srsen, T.; Fabjan-Vodušek, V.; Tul, N.; Fabjan, T.; Osredkar, J. Peripheral arterial tonometry and angiogenic biomarkers in preeclampsia. Hypertens. Pregnancy 2018, 37, 197–203. [Google Scholar] [CrossRef]
- Sharabi-Nov, A.; Kumer, K.; Vodušek, V.F.; Sršen, T.P.; Tul, N.; Fabjan, T.; Meiri, H.; Nicolaides, K.H.; Osredkar, J. Establishing a differential marker profile for pregnancy complications near delivery. Fetal Diagn. Ther. 2019, 47, 471–484. [Google Scholar] [CrossRef]
- Kumer, K.; Sharabi-Nov, A.; Fabjan Vodušek, V.; Premru Sršen, T.; Tul, N.; Fabjan, T.; Meiri, H.; Nicolaides, K.H.; Osredkar, J. Pro- and Anti-Angiogenic Markers as Clinical Tools for Suspected Preeclampsia with and without FGR near Delivery—A Secondary Analysis. Reprod. Med. 2021, 2, 12–25. [Google Scholar] [CrossRef]
- Sharabi-Nov, A.; Premru Sršen, T.; Kumer, K.; Fabjan Vodušek, V.; Fabjan, T.; Tul, N.; Meiri, H.; Nicolaides, K.H.; Osredkar, J. Maternal Serum Inhibin-A Augments the Value of Maternal Serum PlGF and of sFlt-1/PlGF Ratio in the Prediction of Preeclampsia and/or FGR Near Delivery—A Secondary Analysis. Reprod. Med. 2021, 2, 35–49. [Google Scholar] [CrossRef]
- Saleh, L.; Vergouwe, Y.; van den Meiracker, A.H.; Verdonk, K.; Russcher, H.; Bremer, H.A.; Versendaal, H.J.; Steegers, E.A.P.; Danser, J.A.H.; Visser, W. Angiogenic markers predict pregnancy complications and prolongation in preeclampsia continuous versus cut-off values. Hypertension 2017, 70, 1025–1033, Epub 28 August 2017. [Google Scholar] [CrossRef] [Green Version]
- Levine, R.J.; Lam, C.; Qian, C.; Yu, K.F.; Maynard, S.E.; Sachs, B.P.; Sibai, B.M.; Epstein, F.H.; Romero, R.; Thadhani, R.; et al. Soluble endoglin and other circulating antiangiogenic factors in preeclampsia. N. Engl. J. Med. 2006, 355, 992–1005. [Google Scholar] [CrossRef]
- Zeisler, J.; Llurba, E.; Chantraine, F.; Vatish, M.; Phil, D.; Staff, A.D.; Sennström, M.; Olovsson, M.; Brennecke, S.P.; Stepan, H. Predictive value of the sFlt-1: PlGF ratio in women with suspected preeclampsia. N. Engl. J. Med. 2016, 374, 13–22. [Google Scholar] [CrossRef]
- Schlembach, D.; Hund, M.; Schroer, A.; Wolf, C. Economic assessment of the use of the sFlt-1/PlGF ratio test to predict preeclampsia in Germany. BMC Health Serv. Res. 2018, 18, 603, PMCID: PMC6080558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rana, S.; Burke, S.D.; Karumanchi, S.A. Imbalances in circulating angiogenic factors in the pathophysiology of preeclampsia and related disorders. Am. J. Obstet. Gynecol. 2022, 226, S1019–S1034, Epub 20 October 2020. PMCID: PMC888416. [Google Scholar] [CrossRef] [PubMed]
- Suresh, S.; Mueller, A.; Salahuddin, S.; Naseem, H.; Dhir, R.; Rana, S. Evaluation of angiogenic factors in the decision to admit women with suspected preeclampsia. Pregnancy Hypertens. 2020, 21, 124–131. [Google Scholar] [CrossRef]
- Thilaganathan, B. Maternal Cardiac Dysfunction Precedes Development of Preeclampsia. Hypertension 2020, 76, 321–322. [Google Scholar] [CrossRef] [PubMed]
- Pijnenborg, R.; Vercruysse, L.; Hanssens, M. Fetal-maternal conflict, trophoblast invasion, preeclampsia, and the red queen. Hypertension 2008, 27, 183–196. [Google Scholar] [CrossRef]
- Osol, G.; Ko, N.L.; Mandalà, M. Plasticity of the Maternal Vasculature During Pregnancy. Annu. Rev. Physiol. 2019, 81, 89–111. [Google Scholar] [CrossRef] [PubMed]
- Valiño, N.; Giunta, G.; Gallo, D.M.; Akolekar, R.; Nicolaides, K.H. Biophysical and biochemical markers at 30–34 weeks’ gestation in the prediction of adverse perinatal outcome. Ultrasound Obstet. Gynecol. 2016, 47, 194–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciobanu, A.; Rouvali, A.; Syngelaki, A.; Akolekar, R.; Nicolaides, K.H. Prediction of small for gestational age neonates: Screening by maternal factors, fetal biometry, and biomarkers at 35–37 weeks’ gestation. Am. J. Obstet. Gynecol. 2019, 220, 486.e1–486.e11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perry, H.; Gutierrez, J.; Binder, J.; Thilaganathan, B.; Khalil, A. Maternal arteria stiffness in hypertensive pregnancies with and without small-for-gestational-age neonate. Ultrasound Obstet. Gynecol. 2020, 56, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Redman, C.W.G.; Staff, A.C.; Roberts, J.M. Syncytiotrophoblast stress in preeclampsia: The convergence point for multiple pathways. Am. J. Obstet. Gynecol. 2022, 226, S907–S927, Epub 2021 Feb 2. [Google Scholar] [CrossRef] [PubMed]
- Salomon, L.; Alfirevic, Z.; Costa, F.D.S.; Deter, R.; Figueras, F.; Ghi, T.; Glanc, P.; Khalil, A.; Lee, W.; Napolitano, R.; et al. ISUOG practice guidelines: Ultrasound assessment of fetal biometry and growth. Ultrasound Obstet. Gynecol. 2019, 53, 715–723. [Google Scholar] [CrossRef]
- Khalil, A.; Gordijn, S.J.; Beune, I.M.; Wynia, K.; Ganzevoort, W.; Figueras, F.; Kingdom, J.; Marlow, N.; Papageorghiou, A.; Sebire, N.; et al. Essential variables for reporting research studies on fetal growth restriction: A Delphi consensus. Ultrasound Obstet. Gynecol. 2019, 53, 609–614. [Google Scholar] [CrossRef] [Green Version]
- Figueras, F.; Gratacos, E. An integrated approach to fetal growth restriction. Best Pract. Res. Clin. Obstet. Gynaecol. 2017, 38, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Poon, L.; Kametas, N.A.; Valencia, C.; Chelemen, T.; Nicolaides, K.H. Hypertensive disorders in pregnancy: Screening by systolic diastolic and mean arterial pressure at 11–13 weeks. Hypertens. Pregnancy 2010, 30, 93–107. [Google Scholar] [CrossRef]
- Hamburg, N.M.; Benjamin, E.J. Assessment of Endothelial Function Using Digital Pulse Amplitude Tonometry. Trends Cardiovasc. Med. 2009, 19, 6–11. [Google Scholar] [CrossRef] [Green Version]
- Moerland, M.; Kales, A.J.; Schrier, L.; van Dongen, M.G.; Bradnock, D.; Burggraaf, J. Evaluation of the EndoPAT as a Tool to Assess Endothelial Function. Int. J. Vasc. Med. 2012, 2012, 904141, Epub 14 February 2012. PMCID: PMC3303545. [Google Scholar] [CrossRef] [PubMed]
- Arrebola-Moreno, A.L.; Laclaustra, M.; Kaski, J.C. Non-invasive Assessment of Endothelial Function in Clinical Practice. Rev. Esp. Cardiol. 2012, 65, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Carty, D.M.; Anderson, L.A.; Duncan, C.N.; Baird, D.P.; Rooney, L.K.; Dominiczak, A.F.; Delles, C. Peripheral arterial tone: Assessment of microcirculatory function in pregnancy. J. Hypertens. 2012, 30, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Kuvin, J.; Patel, A.; Sliney, K.; Pandian, N.; Sheffy, J. Assessment of peripheral vascular endothelial function with finger arterial pulse wave amplitude. Am. Heart J. 2003, 146, 168–174. [Google Scholar] [CrossRef]
- Flammer, A.J.; Anderson, T.; Celermajer, D.S.; Creager, M.A.; Deanfield, J.; Ganz, P.; Hamburg, N.M.; Lüscher, T.F.; Shechter, M.; Taddei, S.; et al. The assessment of endothelial function: From research into clinical practice. Circulation 2012, 126, 753–767. [Google Scholar] [CrossRef]
- Koo, B.K.; Chung, W.Y.; Moon, M.K. Peripheral arterial endothelial dysfunction predicts future cardiovascular events in diabetic patients with albuminuria: A prospective cohort study. Cardiovasc Diabetol. 2020, 13, 82, PMCID: PMC7293773. [Google Scholar] [CrossRef] [PubMed]
- Hadlock, F.P.; Shah, Y.P.; Kanon, D.J.; Lindsey, J.V. Fetal crown-rump length: Reevaluation of relation to menstrual age (5–18 weeks) with high-resolution real-time US. Radiology 1992, 182, 501–505. [Google Scholar] [CrossRef]
- Hadlock, F.P.; Harrist, R.B.; Martinez-Poyer, J. In utero analysis of fetal growth: A sonographic weight standard. Radiology 1991, 181, 129–133. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Meertens, L.J.; Van Montfort, P.; Scheepers, H.C.; Van Kuijk, S.M.; Aardenburg, R.; Langenveld, J.; Van Dooren, I.M.; Zwaan, I.M.; Spaanderman, M.E.; Smits, L.J. Prediction models for the risk of spontaneous preterm birth based on maternal characteristics: A systematic review and independent external validation. Acta Obstet. Gynecol. Scand. 2018, 97, 907–920. [Google Scholar] [CrossRef]
- Erez, O.; Romero, R.; Jung, E.; Chaemsaithong, P.; Bosco, M.; Suksai, M.; Gallo, D.M.; Gotsch, F. Preeclampsia and eclampsia: The conceptual evolution of a syndrome. Am. J. Obstet. Gynecol. 2022, 226 (Suppl. S2), S786–S803. [Google Scholar] [CrossRef] [PubMed]
- Cnossen, J.S.; Vollebregt, K.C.; de Vrieze, N.; ter Riet, G.; Mol, B.W.; Franx, A.; Khan, K.S.; van der Post, J.A. Accuracy of mean arterial pressure and blood pressure measurements in predicting pre-eclampsia: Systematic review and meta-analysis. BMJ 2008, 336, 1117–1120, Epub 2008 May 14. PMCID: PMC2386627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rolnik, D.A.; Wright, D.; Poon, L.L.; O’Gorman, N.N.; Syngelaki, A.A.; Matallana, C.C.D.P.; Akolekar, R.R.; Cicero, S.S.; Janga, D.D.; Singh, M.M.; et al. Aspirin versus placebo in pregnancies at high risk for preterm preeclampsia. N. Engl. J. Med. 2017, 377, 613–622. [Google Scholar] [CrossRef]
- Tan, M.Y.; Wright, D.; Syngelaki, A.; Akolekar, R.; Cicero, S.; Janga, D.; Singh, M.; Greco, E.; Wright, A.; Maclagan, K.; et al. Comparison of diagnostic accuracy of early screening for pre-eclampsia by NICE guidelines and a method combining maternal factors and biomarkers: Results of SPREE. Ultrasound Obstet. Gynecol. 2018, 51, 743–750, Epub 14 March 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helgadottir, H.; Tropea, T.; Gizurarson, S.; Meiri, H.; Mandalà, M. Aspirin causes endothelium-dependent vasodilation of resistance arteries from non-gravid and gravid rats. Pregnancy Hypertens. 2019, 15, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Jung, E.; Romero, R.; Yeo, L.; Gomez-Lopez, N.; Chaemsaithong, P.; Jaovisidha, A.; Gotsch, F.; Erez, O. The etiology of preeclampsia. Am. J. Obstet. Gynecol. 2022, 226 (Suppl. S2), S844–S866. [Google Scholar] [CrossRef] [PubMed]
- Tarca, A.L.; Romero, R.; Benshalom-Tirosh, N.; Than, N.G.; Gudicha, D.W.; Done, B.; Pacora, P.; Chaiworapongsa, T.; Panaitescu, B.; Tirosh, D.; et al. The prediction of early preeclampsia: Results from a longitudinal proteomics study. PLoS ONE 2019, 14, e0217273, PMCID: PMC6548389. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.D.; Malinowski, A.; Zhou, Q.; Yusuf, S.; Devereaux, P.J. Cardiovascular sequelae of preeclampsia/eclampsia: A systematic review and meta-analyses. Am. Heart J. 2008, 156, 918–930. [Google Scholar] [CrossRef]
- Rodriguez-Fernandez, J.J.; Martinez-Garza, L.E.; Sepulveda-Gonzalez, G.; Hernandez-Castro, F.; Gaston-Locsin, T. Serum biomarkers and Doppler pulsatile index increases likelihood ratio for prediction of preeclampsia in the second trimester of pregnancy. J. Obstet. Gynaecol. 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Melchiorre, K.; Thilaganathan, B.; Giorgione, V.; Ridder, A.; Memmo, A.; Khalil, A. Hypertensive Disorders of Pregnancy and Future Cardiovascular Health. Front. Cardiovasc. Med. 2020, 15, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwala, A.; Michos, E.D.; Samad, Z.; Ballantyne, C.M.; Virani, S.S. The Use of Sex-Specific Factors in the Assessment of Women’s Cardiovascular Risk. Circulation 2020, 141, 592–599, PMCID: PMC7032610. [Google Scholar] [CrossRef] [PubMed]
- Qu, H.; Khalil, R.A. Vascular mechanisms and molecular targets in hypertensive pregnancy and preeclampsia. Am. J. Physiol. Heart Circ. Physiol. 2020, 319, H661–H681, PMCID: PMC7509272. [Google Scholar] [CrossRef] [PubMed]
- Schlembach, D.; Wallner, W.; Sengenberger, R.; Stieglere, E.; Mortl, M.; Beckmann, M.W.; Lang, U. Angiogenic growth factor levels in maternal and fetal blood: Correlation with Doppler ultrasound parameters in pregnancies complicated by pre-eclampsia and intrauterine growth restriction. Ultrasound Obstet. Gynecol. 2007, 29, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Guerby, P.; Tasta, O.; Swiader, A.; Pont, F.; Bujold, E.; Parant, O.; Vayssiere, C.; Salvayre, R.; Negre-Salvayre, A. Role of oxidative stress in the dysfunction of the placental endothelial nitric oxide synthase in preeclampsia. Redox Biol. 2021, 40, 101861. [Google Scholar] [CrossRef] [PubMed]
- Verlohren, S.; Melchiorre, K.; Khalil, A.; Thilaganathan, B. Uterine artery Doppler, birth weight and timing of onset of pre-eclampsia: Providing insights into the dual etiology of late-onset pre-eclampsia. Ultrasound Obstet. Gynecol. 2014, 44, 293–298. [Google Scholar] [CrossRef] [Green Version]
- Klabunde, R.E. Cardiovascular Physiology Concepts, 2nd ed.; Walter Kluwer, Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012; 256p. [Google Scholar]
- Riise, H.K.; Sulo, G.; Tell, G.S.; Igland, J.; Nygård, O.; Vollset, S.E.; Iversen, A.; Austgulen, R.; Daltveit, A.K. Incident coronary heart disease after preeclampsia: Role of reduced fetal growth, preterm delivery, and parity. J. Am. Heart Assoc. 2017, 6, e004158. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unaffected | PTD (<37 wks) | PE | FGR | FGR + PE | p | |
|---|---|---|---|---|---|---|
| A. All Participants | ||||||
| (n = 21) | (n = 15) | (n = 31) | (n = 16) | (n = 42) | ||
| Enrollment | ||||||
| Gestational Age (wks) | 34.0 [32.0–35.9] | 31.2 [29.4–32.9] * | 33.9 [32.3–35.6] | 31.4 [29.1–33.6] * | 31.8 [30.7–32.8] * | 0.027 |
| Maternal Age (years) | 31.6 [29.5–33.8] | 31.3 [29.7–32.9] | 32.0 [29.9–34.1] | 31.7 [29.7–33.7] | 32.9 [31.1–34.7] | 0.792 |
| Body Mass Index | 25.8 [23.7–27.9] | 24.6 [22.9–26.4] | 29.5 [26.5–32.6] | 27.6 [24.2–31.0] | 29.6 [26.9–32.4] | 0.011 |
| Previous PE (%) | 4.8 | 6.7 | 6.5 | 6.3 | 9.5 | 0.965 |
| Chronic Hypertension (%) | 0 | 0 | 19.4 * | 0 | 16.7 * | 0.032 |
| Diabetes (%) | 0 | 0 | 3.2 | 0 | 4.8 | 0.787 |
| Polycystic Ovary (%) | 0 | 0 | 0 | 0 | 7.1 * | 0.204 |
| Parity | 1.7 [1.3–2.0] | 1.6 [1.2–2.1] | 1.4 [1.0–1.8] | 1.5 [1.1–1.9] | 1.5 [1.2–1.8] | 0.806 |
| Conception by IVF (%) | 4.8 | 0 | 6.5 | 0 | 11.9 * | 0.361 |
| Biophysical Markers | ||||||
| MAP | 85 [80–90] | 90 [82–98] | 106 [102–110] * | 98 [91–106] | 102 [95–108] * | <0.001 |
| PI | 0.68 [0.66–0.70] | 0.70 [0.64–0.61] | 0.80 [0.60–1.17] * | 1.35 [1.05–1.66] ** | 1.42 [1.25–1.56] ** | <0.001 |
| RHI | 1.61 [1.59–1.65] | 1.47 [1.44–1.62] | 1.69 [1.67–1.97] | 1.85 [1.81–2.07] * | 1.82 [1.66–1.91] * | 0.048 |
| AIX(%) | −4.0 [(−8.0)−(5.0)] | −4.5 v[(−12.0)–(2.0)] | 9.0 [(8.9)–(12.0)] * | −1.0 [(−7.0)–(10.0) | 8.0 [(4.0)–(15.0)] * | 0.035 |
| Delivery | ||||||
| Gestational age (wks) | 39.1 [38.5–39.7] | 33.8 [32.1–35.5] * | 34.2 [32.6–35.9] * | 31.7 [29.4–34.0] ** | 32.0 [31.0–33.1] ** | <0.001 |
| Delivery by C-Section | 23.8 | 30.8 | 54.8 ** | 60.0 * | 83.4 ** | <0.001 |
| Baby’s birthweight(grams) | 3330 [3133–3528] | 2207 [1872–2542] * | 2306 [1906–2705] * | 2306 [1906–2705] * | 1449 [1247–1651] ** | <0.001 |
| B. Early Cases (<34 wks) | ||||||
| (n = 6) | (n = 10) | (n = 12) | (n = 28) | |||
| Enrollment | ||||||
| Gestational Age (wks) | 29.2 [26.8–31.6] | 29.9 [27.5–32.3] | 29.3 [27.7–30.8] | 29.9 [28.9–30.9] | 0.805 | |
| Maternal age (years) | 31.3 [27.8–34.8] | 33.8 [33.0–37.7] | 31.5 [29.2–33.8] | 33.1 [30.7–35.5] | 0.668 | |
| Body Mass Index (kg/m2) | 24.7 [21.0–28.4] | 30.7 [26.2–35.2] | 26.3 [23.9–28.8] | 29.7 [26.1–33.4] | 0.123 | |
| Previous PE (%) | 0 | 0 | 0 | 7.1 | 0.591 | |
| Chronic Hypertension (%) | 0 | 7.7 | 0 | 21.4 * | 0.146 | |
| Diabetes (%) | 0 | 0 | 0 | 3.6 | 0.771 | |
| Polycystic Ovary (%) | 0 | 0 | 0 | 3.6 | 0.771 | |
| Parity | 1.8 [1.0–2.6] | 1.5 [0.7–2.4] | 1.3 [0.9–1.7] | 1.6 [1.2–2.0] | 0.807 | |
| Conception by IVF (%) | 0 | 15.4 * | 0 | 10.7 | 0.805 | |
| Biophysical Markers | ||||||
| MAP | 87 [70–103] | 110 [81–140] * | 97 [89–105] * | 102 [94–110] * | 0.041 | |
| UTPI | 0.69 [0.57–0.80] | 1.20 [0.83–1.57] * | 1.62 [1.35–1.90] ** | 1.43 [1.27–1.58] ** | 0.003 | |
| RHI | 1.5 [1.4–1.6] | 1.7 [1.6–1.7] | 1.9 [1.8–2.1] * | 1.7 [1.7–1.9] | 0.047 | |
| AIX (%) | −3.0 [(−17.0)–(22.0)] | 9.0 [8.9–9.1] | 3.0 [(−12.0)–(32.0)] | 6.0 [(−15.0)–(25.0)] | 0.048 | |
| Delivery | ||||||
| GA at delivery (wks) | 31.0 [28.0–34.0] | 30.2 [27.8–32.6] | 29.5 [28.0–31.1] | 30.2 [29.2–31.2] | 0.805 | |
| Delivery by C-Section (%) | 20.0 | 77.9 * | 72.7 * | 92.6 ** | 0.003 | |
| Baby birthweight (grams) | 1669 [1318–2020] | 1276 [923–1628] * | 874 [627–1121] ** | 1171 [995–1346] * | 0.018 | |
| Unaffected + PTD | PE | FGR | FGR + PE | p | |
|---|---|---|---|---|---|
| (n = 37) | (n = 31)) | (n = 16) | (n = 42) | ||
| All Participants | |||||
| Markers over GA | |||||
| UtA Doppler PI | 0.002 | −0.350 | −0.811 *** | −0.412 * | <0.001 |
| MAP | −0.212 | −0.162 | 0.108 | −0.266 | <0.05 |
| RHI | 0.136 | 0.027 | 0.164 | −0.199 | <0.05 |
| AIX | −0.110 | 0.485 * | 0.305 | −0.130 | <0.001 |
| Markers over BMI | |||||
| UtA Doppler PI | −0.038 | 0.367 * | −0.095 | 0.001 | <0.05 |
| MAP | 0.288 | −0.487 * | −0.392 * | −0.071 | <0.05 |
| RHI | −0.157 | 0.146 | 0.282 | 0.273 | <0.05 |
| AIX (%) | 0.183 | 0.262 | 0.273 | 0.273 | <0.05 |
| UtA Doppler PI over Angiogenic Markers | |||||
| sFlt-1/PlGF ratio | −0.116 | 0.09 | −0.367 ** | 0.550 ** | <0.001 |
| PlGF | 0.319 | −0.354 | 0.317 * | −0.484 * | <0.005 |
| GA < 34 wks | |||||
| sFlt-1/PlGF ratio | 0.327 * | 0.05 | |||
| PlGF | −0.497 *** | 0.001 | |||
| Continuous Model | Cut-Off Model | PPV (%) | NPV (%) | |||||
|---|---|---|---|---|---|---|---|---|
| Complication | Marker | AUC (95% CI) | DR at 10% FPR | Cut-Off | AUC (95% CI) | DR at 10% FPR | ||
| A. All Cases | ||||||||
| PE (n = 31) | MAP | 0.94 [0.85–1.00) | 82 | 98 mm Hg | 0.81 [0.65–0.97) | 35 | 58 | 83 |
| UtAPI | 0.68 [0.39–0.96) | 85 | 0.85 | 0.80 [0.60–0.99) | 50 | 87 | 71 | |
| RHI | 0.69 [0.48–0.91) | 27 | 1.6 | 0.62 [0.41–0.84) | 15 | 65 | 85 | |
| AIX | 0.76 [0.58–0.95) | 46 | 4.0 | 0.77 [0.59–0.96) | 35 | 56 | 92 | |
| FGR (n = 16) | MAP | 0.68 [0.46–0.90] | 36 | 0.85 | 0.49 [0.26–0.72] | 15 | 33 | 37 |
| UtAPI | 0.95 [0.85–1.00] | 83 | 0.85 | 0.90 [0.75–1.00] | 84 | 83 | 94 | |
| RHI | 0.76 [0.56–0.97] | 46 | 1.6 | 0.66 [0.45–0.88] | 17 | 63 | 89 | |
| AIX | 0.61 [0.38–0.83] | 18 | 4.0 | 0.57 [0.34–0.81] | 42 | 80 | ||
| PE + FGR (n = 41) | MAP | 0.83 [0.66–0.99] | 60 | 98 mm Hg | 0.73 [0.54–0.91] | 27 | 58 | 83 |
| UtAPI | 0.99 [0.96–1.00] | 88 | 0.85 | 0.96 [0.90–1.00] | 81 | 94 | 91 | |
| RHI | 0.74 [0.58–0.93] | 27 | 1.60 | 0.70 [0.52–0.88] | 16 | 88 | 85 | |
| AIX | 0.75 [0.59–0.90] | 46 | 4.0 | 0.66 [0.46–0.86] | 26 | 56 | 80 | |
| B. Early Cases < 34 weeks | ||||||||
| PE (n = 10) | MAP | 1.00 [1.00–1.00] | 100 | 98 mm Hg | 0.90 [0.65–1.00] | 50 | 67 | 100 |
| UtAPI | 0.68 [0.43–0.93] | 58 | 0.85 | 0.79 [0.59–1.00] | 63 | 100 | 53 | |
| RHI | 0.95 [0.78–1.00] | 16 | 1.6 | 0.90 [0.65–1.00] | 50 | 67 | 100 | |
| AIX | 0.80 [0.45–1.00] | 0 | 4.0 | 0.80 [0.47–1.00] | 25 | 50 | 100 | |
| FGR (n = 12) | MAP | 0.73 [0.45–1.00] | 34 | 98 mm Hg | 0.57 [0.25–0.89] | 17 | 75 | 40 |
| UtA PI | 1.00 [1.00–1.00] | 100 | 0.85 | 1.00 [1.00–1.00] | 100 | 100 | 100 | |
| RHI | 0.87 [0.67–1.00] | 78 | 1.6 | 0.79 [0.52–1.00] | 38 | 88 | 89 | |
| AIX | 0.64 [0.31–0.98] | 23 | 4.0 | 0.47 [0.14–0.79] | 8 | 40 | 33 | |
| PE + FGR (n = 28) | MAP | 0.87 [0.70–1.00] | 73 | 98 mm Hg | 0.76 [0.50–1.00] | 35 | 89 | 57 |
| UtAPI | 0.98 [0.92–1.00] | 95 | 0.85 | 0.98 [0.92–1.00] | 95 | 100 | 86 | |
| RHI | 0.88 [0.70–1.00] | 80 | 1.6 | 0.80 [0.54–1.00] | 40 | 67 | 67 | |
| AIX | 0.72 [0.43–1.00] | 30 | 4.0 | 0.55 [0.23–0.87] | 13 | 71 | 63 | |
| Condition | Marker | AUC (95% CI) | p | DR at 10% FPR |
|---|---|---|---|---|
| All PE (n = 31) | MAP | 0.94 [0.85–1.00] | <0.006 | 82 |
| MAP + UtA PI | 0.95 [0.89–1.00] | <0.002 | 91 | |
| MAP + PI + RHI | 0.97 [0.88–1.00] | <0.001 | 95 | |
| MAP + UtA PI + RHI + AIX | 0.98 [0.91–1.00] | <0.001 | 100 | |
| All FGR (n = 16) | PI | 0.95 [0.88–1.00] | <0.001 | 83 |
| UtA PI + RHI | 0.98 [0.90–1.00] | 0.002 | 93 | |
| UtA UtA PI + RHI + MAP | 0.98 [0.92–1.00] | <0.001 | 93 | |
| MAP + UtA PII + RHI + AIX | 0.99 [0.94–1.00] | <0.001 | 99 | |
| All PE + FGR (n = 42) | UtA PI | 0.94 [0.87–1.00] | <0.001 | 88 |
| UtA PI + MAP | 0.98 [0.91–0.99] | <0.001 | 90 | |
| UtA PI + MAP + RHI | 0.98 [0.93–1.00] | <0.001 | 93 |
| MAP | UtA PI | RHI | AIX | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All Participants | ||||||||||||
| Variables | B | S.E. | Β | B | S.E. | Β | B | S.E. | Β | B | S.E. | β |
| MA (years) | −0.41 | 0.29 | −0.15 | 0.01 | 0.01 | 0.01 | 0.01 | 0.02 | 0.08 | −0.19 | 0.33 | −0.07 |
| GA (weeks)) | 0.20 | 0.39 | 0.06 | −0.05 | 0.01 | −0.46 | −0.01 | 0.02 | −0.01 | 0.01 | 0.45 | 0.00 |
| PE (vs. unaffected) | 19.31 | 3.90 | 0.53 *** | 0.17 | 0.09 | 0.16 * | 0.19 | 0.20 | 0.12 | 11.58 | 4.42 | 0.32 * |
| FGR (vs. unaffected) | 12.63 | 4.52 | 0.35 ** | 0.47 | 0.12 | 0.33 *** | 0.19 | 0.24 | 0.12 | 8.71 | 5.10 | 0.24 |
| FGR + PE (vs. unaffected) | 17.33 | 4.11 | 0.55 *** | 0.44 | 0.09 | 0.44 *** | 0.05 | 0.22 | 0.04 | 12.19 | 4.69 | 0.39 * |
| F | 7.19 *** | 24.74 *** | 0.39 | 2.53 * | ||||||||
| R2 | 0.36 | 0.57 | 0.03 | 0.17 | ||||||||
| Birth < 34 wks | ||||||||||||
| Variables | B | S.E. | Β | B | S.E. | Β | B | S.E. | Β | B | S.E. | β |
| MA (years) | −0.41 | 0.45 | −0.18 | 0.00 | 0.01 | −0.01 | −0.03 | 0.01 | −0.48 * | 0.06 | 0.74 | 0.02 |
| GA (weeks)) | 1.74 | 0.88 | 0.37 | −0.08 | 0.02 | −0.47 *** | −0.04 | 0.03 | −0.28 | 0.73 | 1.41 | 0.12 |
| PE (vs. unaffected) | 23.06 | 10.22 | 0.49 * | 0.44 | 0.17 | 0.40 * | 0.63 | 0.28 | 0.47 * | 10.03 | 16.06 | 0.17 |
| FGR (vs. unaffected) | 13.08 | 6.25 | 0.50 * | 0.78 | 0.18 | 0.64 *** | 0.45 | 0.17 | 0.60 * | 9.29 | 9.67 | 0.28 |
| FGR + PE (vs. unaffected) | 18.72 | 6.32 | 0.74 ** | 0.66 | 0.16 | 0.69 *** | 0.45 | 0.17 | 0.61 * | 12.45 | 9.84 | 0.39 |
| F | 2.74 * | 10.23 *** | 3.57 * | 0.40 | ||||||||
| R2 | 0.40 | 0.55 | 0.47 | 0.09 | ||||||||
| Birth > 34 wks | ||||||||||||
| Variables | B | S.E. | Β | B | S.E. | Β | B | S.E. | Β | B | S.E. | β |
| MA (years) | −0.71 | 0.39 | −0.24 | 0.00 | 0.01 | 0.03 | 0.05 | 0.02 | 0.31 | −0.46 | 0.38 | −0.19 |
| GA (weeks)) | −1.13 | 0.96 | −0.16 | −0.03 | 0.02 | −0.15 | −0.09 | 0.06 | −0.27 | −0.63 | 0.93 | −0.11 |
| PE (vs. unaffected) | 16.30 | 4.38 | 0.49 ** | 0.11 | 0.09 | 0.14 | 0.12 | 0.26 | 0.07 | 10.29 | 4.21 | 0.38 * |
| FGR (vs. unaffected) | 18.60 | 7.94 | 0.29 * | 0.13 | 0.16 | 0.10 | 0.33 | 0.48 | 0.11 | 9.88 | 7.64 | 0.19 |
| FGR + PE (vs. unaffected) | 15.76 | 5.87 | 0.38 * | 0.50 | 0.11 | 0.62 *** | −0.33 | 0.35 | −0.16 | 11.89 | 5.66 | 0.35 * |
| F | 6.16 *** | 7.29 *** | 1.52 | 2.63 * | ||||||||
| R2 | 0.46 | 0.45 | 0.17 | 0.27 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharabi-Nov, A.; Tul, N.; Kumer, K.; Premru Sršen, T.; Fabjan Vodušek, V.; Fabjan, T.; Osredkar, J.; Nicolaides, K.H.; Meiri, H. Biophysical Markers of Suspected Preeclampsia, Fetal Growth Restriction and The Two Combined—How Accurate They Are? Reprod. Med. 2022, 3, 62-84. https://doi.org/10.3390/reprodmed3020007
Sharabi-Nov A, Tul N, Kumer K, Premru Sršen T, Fabjan Vodušek V, Fabjan T, Osredkar J, Nicolaides KH, Meiri H. Biophysical Markers of Suspected Preeclampsia, Fetal Growth Restriction and The Two Combined—How Accurate They Are? Reproductive Medicine. 2022; 3(2):62-84. https://doi.org/10.3390/reprodmed3020007
Chicago/Turabian StyleSharabi-Nov, Adi, Nataša Tul, Kristina Kumer, Tanja Premru Sršen, Vesna Fabjan Vodušek, Teja Fabjan, Josko Osredkar, Kypros H. Nicolaides, and Hamutal Meiri. 2022. "Biophysical Markers of Suspected Preeclampsia, Fetal Growth Restriction and The Two Combined—How Accurate They Are?" Reproductive Medicine 3, no. 2: 62-84. https://doi.org/10.3390/reprodmed3020007
APA StyleSharabi-Nov, A., Tul, N., Kumer, K., Premru Sršen, T., Fabjan Vodušek, V., Fabjan, T., Osredkar, J., Nicolaides, K. H., & Meiri, H. (2022). Biophysical Markers of Suspected Preeclampsia, Fetal Growth Restriction and The Two Combined—How Accurate They Are? Reproductive Medicine, 3(2), 62-84. https://doi.org/10.3390/reprodmed3020007