Abstract
Fertility preservation is an important concern for young cancer patients. Oocyte or embryo cryopreservation prior to chemotherapy administration is desirable but often difficult for patients with hematopoietic and lymphoid tissue tumors. In this study, we examined the results of fertility preservation therapy in patients with hematopoietic and lymphoid tissue tumors. We retrospectively examined hematopoietic and lymphoid tissue tumors of five patients who underwent oocyte cryopreservation as a fertility preservation therapy after chemotherapy, at Showa University Hospital from February 2017 to September 2020. Eleven treatment cycles were administered (one of which was cancelled). The mean age of the patients was 28.6 years. The mean controlled ovarian stimulation duration for 10 cycles was 15.9 days, the mean total gonadotropin dose was 3705 IU, and the mean peak E2 was 502.8 (pg/mL). The mean number of eggs retrieved was 3.2, the mean number of mature oocytes was 2.1, and the mean maturation rate (mature oocytes/returned oocytes) was 70.7%. Fertility preservation procedures in the early period after chemotherapy may be viable because they allow for the acquisition of mature oocytes, even though the procedures may take longer and yield fewer oocytes.
1. Introduction
The five-year survival rate of children and young adolescent adults (YAAs) with cancer has recently increased, due to improved biological studies and treatment outcomes [1]. However, chemotherapy treatment, especially with alkylating agents and radiation therapy, affects ovarian function, increasing the risk of amenorrhea and premature ovarian failure [2,3]. The American Society of Clinical Oncology (ASCO) 2018 guidelines also indicate the risks of chemotherapy and radiation [4]. Currently, oocyte or embryo cryopreservation and ovarian tissue cryopreservation are used for fertility preservation to improve the quality of life of cancer patients after treatment [5]. Both fertility-preservation therapies should be performed prior to the initiation of chemotherapy or radiation therapy. This requirement is particularly important in oocyte or embryo cryopreservation, since oocyte retrieval requires approximately 2 weeks. However, since tumors of hematopoietic and lymphoid tissues, such as leukemia and malignant lymphoma, require immediate treatment, the maintenance of a 2-week interval before chemotherapy is practically difficult, in most cases. Moreover, ovarian tissue cryopreservation is still in the research stage, and the possibility of leukemia cell contamination in ovarian tissue has not been ruled out [6].
In the present study, we report multiple cases of hematopoietic and lymphoid tissue tumors treated with chemotherapy, followed by oocyte cryopreservation as a fertility preservation therapy, and discuss the course and results of the treatment.
2. Materials and Methods
2.1. Patients
The protocol for this study was reviewed and approved by the Ethics Committee of Showa University Hospital (#3307). We carried out a retrospective study of 5 patients and 11 cycles of fertility preservation therapy after chemotherapy initiation for hematopoietic and lymphoid tissue tumors between February 2017 and September 2020. Each cancer patient was examined by a primary care physician to obtain information for fertility-preservation therapy. We explained the fertility-preservation therapy and performed controlled ovarian stimulation (COS) and oocyte retrieval in patients who provided consent. To compare the treatment outcomes, the results were compared with those of 35 breast cancer patients who had undergone fertility preservation therapy prior to chemotherapy for 42 cycles.
2.2. Schedule of Chemotherapy and COS Protocol
After chemotherapy, COS was initiated on the first or second day after hospital discharge. We performed the gonadotropin-releasing hormone (GnRH) antagonist protocol or a random start protocol for the COS. Follicle-stimulating hormone (FSH, FOLYRMON®, FujiPharma, Tokyo, Japan) or human menopausal gonadotropin (hMG, HMG[FERRING], Ferring Pharma, Tokyo, Japan) were administered daily at 150–300 IU until ovulation triggering. Cetrorelix acetate (Cetrotide®, Merck Biopharma, Tokyo, Japan) was combined with the antagonist product after the leading follicle reached 14 mm. When multiple follicles reached 18–20 mm, oocytes were collected approximately 34 h later using recombinant human chorionic gonadotropin (hCG, OVIDREL®, Merck Biopharma, Tokyo, Japan) or urinary-hCG (GONATROPIN®, ASKA Pharma, Tokyo, Japan) 10,000 IU and a GnRH agonist (BUSERELIN, Fuji Pharma, Tokyo, Japan) as a double trigger. Patients who were scheduled for further chemotherapy were admitted for another chemotherapy session on the next day or 2 days after the oocyte retrieval.
2.3. Statistical Analysis
Statistical analysis was performed between the two groups using the Wilcoxon rank sum test and Fisher’s extract test; p < 0.05 was defined as a significant difference. The statistical software used was JMP Pro 15.
3. Results
Overall, we identified 5 women and 11 cycles with a mean age of 28.6 years. In all patients, anti-Müllerian hormone (AMH) levels were measured after the first chemotherapy was introduced, and although measurements could not be taken before the chemotherapy, the mean AMH level was 0.34 ng/mL (Table 1). Details of the chemotherapy given prior to the fertility preservation therapy are shown in Table 2. Although the chemotherapy used was different, all had a low or lower risk of ovarian toxicity, according to the ASCO classification. The results of the 11 cycles of treatment are shown in Table 3. Only one cycle was cancelled due to lack of response to controlled ovarian stimulation. The mean duration of controlled ovarian stimulation for the 10 cycles of fertility preservation therapy was 15.9 days, mean total gonadotropin dose was 3705 IU, and mean peak E2 was 502.8 (pg/mL). The mean number of retrieved oocytes was 3.2, mean number of mature oocytes was 2.1, and mean maturation rate (mature oocyte/retrieved oocyte) was 70.7%. Their AMH level was less than 1 ng/mL, which tended to be lower than the AMH values of the same generation previously reported [7]. As a comparison, the results of breast cancer patients who underwent fertility preservation therapy at our hospital before chemotherapy are shown (Supplemental Table S1). The breast cancer patients before chemotherapy are that the mean age tended to be significantly higher at 34.5 years than patients with hematopoietic and lymphoid tissue tumors after chemotherapy, but the mean AMH level was also significantly higher at 3.84 ng/mL. The treatment outcome was significantly shorter than that of after chemotherapy, with a controlled ovarian stimulation period of 8.9 days before chemotherapy, and the gonadotropin dose was significantly lower at 2298 IU. The number of eggs retrieved was 9.6, and the number of mature eggs (MII) retrieved was 7.4, both significantly higher (Supplemental Table S2).

Table 1.
Patient’s characteristics.
Table 2.
Chemotherapy protocols.
Table 3.
Oocyte cryopreservation results.
Individual Case Presentations
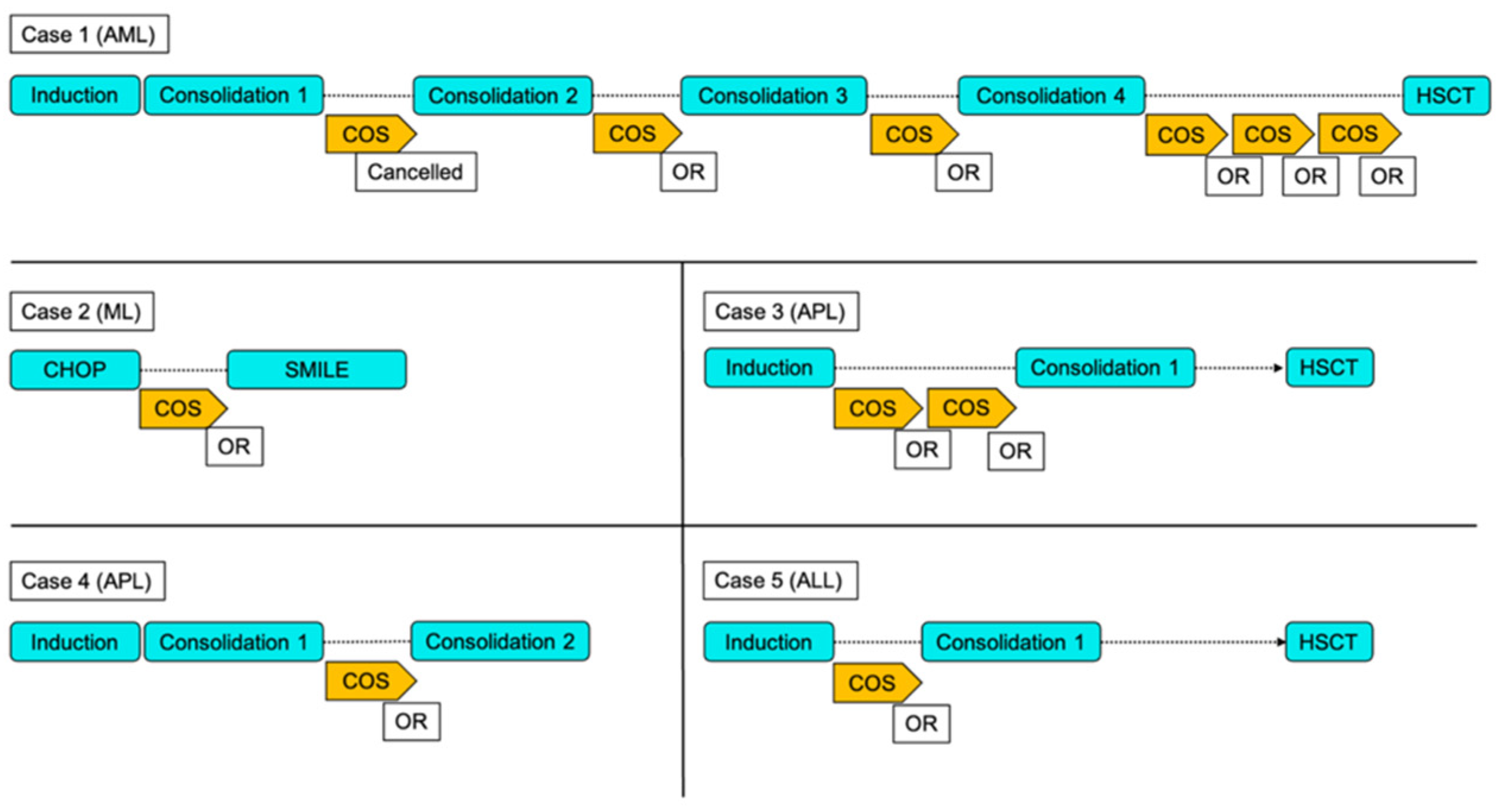
Figure 1 and Table 3 show the individual treatment progress and results. Case 1 involves a 27-year-old female diagnosed with acute myeloid leukemia (AML). The JALSG AML201 protocol by the JAPAN ADULT LEUKEMIA STUDY GROUP (JALSG) [8] was adopted as the chemotherapy regimen. Idarubicin (Idamycin®, Pfizer, New York, NY, USA) and cytarabine (Cylocide®, NIPPON SHINYAKU, Kyoto, Japan) were administered as remission induction therapy; cytarabine and mitoxantrone hydrochloride (NOVANTRON®, ASKA Pharma, Tokyo, Japan) were administered as the first round of consolidation therapy; cytarabine and daunorubicin (DAUNOMYCIN®, Meiji Seika, Tokyo, Japan) as the second round; cytarabine and aclarubicin (Aclacinon®, Astellas Pharma, Tokyo, Japan) as the third round; and cytarabine, etoposide (VePesid®, CLINIGEN, Burton On Trent, UK), vincristine (Oncovin®, Nippon Kayaku, Tokyo, Japan), and vindesine (Fildesin®, Nichi-Iko Pharma, Toyama, Japan) as the fourth round. Finally, future hematopoietic stem cell transplantation (HSCT) was planned. After the introduction and first consolidation therapy for the AML, we initiated COS. The initial ovarian stimulation was canceled due to lack of follicular development after 14 days of hMG/FSH administration, and there was no prospect of oocyte retrieval. However, she was scheduled to undergo another round of COS after the second consolidation therapy because the patient wished to undergo oocyte cryopreservation, when she was treated with Kaufman therapy. After the second consolidation therapy, the patient was started on COS with the antagonist protocol; two oocytes were retrieved, and one was cryopreserved. After the third round of consolidation, three oocytes were retrieved in the second round of oocyte retrieval and two were cryopreserved. In the fourth oocyte retrieval, five oocytes were retrieved and cryopreserved. For the fifth oocyte retrieval, two oocytes were retrieved, and one was cryopreserved.
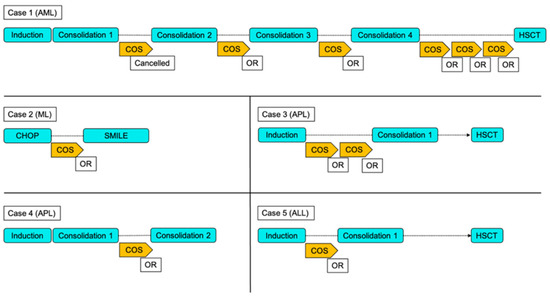
Figure 1.
Treatment course of individual chemotherapy and oocyte retrieval. AML: Acute myeloid leukemia ML:Malignant Lyphoma APL: Acute promyelocytic Leukemia ALL: Acute lymphocytic leukemia OR: oocyte retrieval COS: Controlled ovarian stimulation HSCT: Hematopoitic stem cell transplantation.
Case 2 involves a 30-year-old female with malignant lymphoma, who was referred during cyclophosphamide (Endoxan®, Shionogi pharma, Osaka, Japan), doxorubicin (Doxorubicin Hydrocholoride (NK), Nippon Kayaku, Tokyo, Japan), vincristine (Oncovin®, Nippon Kayaku, Tokyo, Japan), and prednisone (PREDONINE®, Shionogi pharma, Osaka, Japan) (CHOP) therapy. She was referred for fertility preservation therapy because she was scheduled to undergo dexamethasone (DEXART®, FujiPharma, Tokyo, Japan), methotrexate (METHOTREXATE®, Pfizer, New York, USA), ifosfamide (Ifomide®, Shionogi pharma, Osaka, Japan), L-asparaginase (Leunase®, Kyowa Kirin, Tokyo, Japan) and etoposide (SMILE) therapy and was concerned about irreversible ovarian dysfunction. Eight oocytes were retrieved and cryopreservation of four oocytes were performed in the COS with the random start protocol in the period before the start of SMILE therapy.
Case 3 involves a 30-year-old female with acute promyelocytic leukemia (APL). Idarubicin, cytarabine and tretinoin (VESANOID®, FujiPharma, Tokyo, Japan) were administered for remission induction therapy. A hematopoietic stem cell transplant was planned for the future. After the induction therapy, two cycles of COS with the random start protocol were performed. In the first oocyte retrieval cycle, one egg was retrieved and cryopreserved, and in the second cycle, two oocytes were retrieved, and one was cryopreserved.
Case 4 involves a 28-year-old female with acute promyelocytic leukemia (APL). Idarubicin, cytarabine and tretinoin were administered for remission induction therapy; mitoxantrone hydrochloride and cytarabine were administered as consolidation therapy. A hematopoietic stem cell transplant was planned for the future. After the induction and consolidation therapy, one cycle of COS with the random start protocol was performed and five oocytes were retrieved, and cryopreservation of four oocytes was performed.
Case 5 involves a 26-year-old female with acute lymphocytic leukemia (ALL). Daunorubicin, cyclophosphamide, vincristine, predonin, and L-asparaginase were administered as remission induction therapy. After the induction therapy, COS with random start protocol was performed for one cycle and two oocytes were retrieved, and cryopreservation of two oocytes was performed.
4. Discussion
The duration of controlled ovarian stimulation was longer, and the FSH/hMG dose was higher than patients with breast cancer who underwent fertility preservation therapy before chemotherapy. However, the number of oocytes retrieved tended to be lower. Unfortunately, we could not measure the AMH levels before chemotherapy introduction; thus, we could not determine how the AMH values changed, but five patients had no episodes of irregular menstruation, previous ovarian surgery, or other conditions that would affect AMH levels. We can assume that the values were originally age-appropriate and were likely altered by chemotherapy. Since AMH is a hormone produced by preantral follicles and small antral follicles, the present study results suggest that even low-risk chemotherapy may affect preantral follicles and small antral follicles. Several histologic studies on chemotherapy’s effects on human ovaries demonstrated increased ovarian atrophy and a reduced number of primordial follicles [9,10].
Although not yet definitive in human studies, data from animal studies indicate that chemotherapy/radiotherapy may be mutagenic to germ cells at various maturation stages [11,12,13,14,15,16]. Therefore, it may not be advisable to collect oocytes immediately after exposure to chemotherapy. However, the potential need for HSCT is another consideration in these patients. HSCT is indicated when chemotherapy does not result in an adequate response or when it is expected to yield better prognosis [17]. Chemotherapy and total-body irradiation, including treatment with alkylating agents prior to HSCT, is associated with a very high risk of amenorrhea and irreversible fertility impairment (>70%, according to the ASCO classification). Therefore, even though the effects of chemotherapy on the oocyte have not yet been fully clarified as mentioned above, if the patient wished to preserve fertility, fertility preservation therapy had to be performed before HSCT, including between chemotherapy and chemotherapy. In our study, three of five patients were scheduled for HSCT. Therefore, the short period between chemotherapy and HSCT was used to administer the fertility preservation therapy.
Anthracyclines (idarubicin, mitoxantrone hydrochloride, daunorubicin, aclarubicin, and doxorubicin) exhibit anticancer effects by inhibiting the activity of topoisomerase II, which is responsible for DNA synthesis [18]. Microvascular damage to the human ovary and necrosis of ovarian stromal tissue has also been reported [19]. Moreover, doxorubicin-associated female reproductive toxicity has recently been reported; it induces apoptosis in mammalian oocytes and significantly reduces oocyte viability in vitro [20]. Furthermore, anthracyclines produce reactive oxygen species (ROS) during the apoptosis induction process [21,22,23], resulting in decreased blood flow to the ovary [24], which may be involved in poor follicle development. Therefore, gonadotropin-dependent follicles may be less responsive to COS and are more easily induced into atretic follicles. Cytarabine is an antimetabolite that is considered to inhibit DNA synthesis at cytidine diphosphate reductase and DNA polymerase levels [25]. Cytarabine reportedly shows a concentration-dependent cytotoxic effect on leukemia cells in the stationary phase, with reduced DNA synthesis capacity [26]. Furthermore, it induces leukemia cell differentiation at concentrations below the cytotoxic effect [27], and it has limited effects on the ovary itself [28,29]. However, cytarabine also produces ROS [30], which, as is the case with anthracycline, may have interfered with follicle development. In addition to inhibiting DNA repair as a topoisomerase II inhibitor, etoposide induces double-stranded DNA breaks in cells. This leads to apoptosis via ataxia-telangiectasia-mutated protein kinase activation and subsequent phosphorylation of histone H2AX [31,32]. Increased DNA damage in granulosa cells and increased atretic follicles was reported in mice lacking topoisomerase [33].
Vincristine, a drug that belongs to the vinca alkaloid family, shows an antitumor effect by inhibiting mitotic spindles formation, necessary for cell division, proliferation, and apoptosis [34]. Although it does not affect primordial follicles, vincristine induces the development of atretic follicles [35].
These results suggest that even a low risk of amenorrhea (<30%, according to the ASCO classification) can temporarily decrease ovarian reserves. Since the chemotherapeutic drugs were not alkylating agents, they were considered to have affected the growing follicles, although their effect on primordial follicles was not significant. Thus, the patients showed a reduction in AMH levels and increased gonadotropins dose because of a poor response to COS. Thus, adult females who receive chemotherapy for leukemia may have a compromised ovarian reserve, even in the setting of regular menses [36]. In a study of AMH levels after chemotherapy in patients with lymphoma, AMH levels decreased rapidly after the introduction of chemotherapy, regardless of the regimen, and remained low until approximately 3 months after completing chemotherapy [37]. Therefore, we could have expected an increase in AMH levels that would have led to an increase in the number of developing follicles if we had waited for more than 3 months, although this was clinically difficult.
Only one patient underwent oocyte retrieval after each chemotherapy session. It was predicted that the response to COS would gradually worsen as the effects of chemotherapy on the ovaries accumulated. However, the stimulation period tended to shorten, and the number of retrieved and mature oocytes did not change significantly. This suggests that the effects of a low risk of amenorrhea (<30%, according to the ASCO classification) on the ovaries are limited in duration. Additionally, mature oocytes (MII) were obtained from the retrieved oocytes, indicating that follicles responding to COS had the potential to acquire mature oocytes.
This study had some limitations. The number of patients who received fertility preservation therapy after chemotherapy was small, and the timing and regimen of the fertility preservation therapy differed. Therefore, the effect of different regimens cannot be discussed. Furthermore, this study was conducted until the acquisition of mature oocytes, and none of the patients involved thawing and intracytoplasmic sperm injection of the cryopreserved oocytes. Few studies have reported on the outcome of fertilization rates after thawing cryopreserved oocytes after chemotherapy [38]. The effects of oocyte chemotherapy exposure on fertilization, embryo development, implantation, pregnancy course and delivery are topics for future studies.
5. Conclusions
In conclusion, the early period after chemotherapy fertility preservation therapy tends to induce apoptosis in developing follicles because of the effects of chemotherapy. This results in consequent effects on COS, and the number of retrieved oocytes. However, it does allow for the retrieval of mature oocytes. This makes it a viable option for patients who are expected to have irreversible ovarian dysfunction, such as those who will undergo hematopoietic stem cell transplantation, provided adequate informed consent is obtained. These data will be also useful for primary care physicians when explaining the effects of chemotherapy to patients undergoing fertility preservation therapy.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/reprodmed3020012/s1, Table S1: Breast cancer patients who underwent fertility preservation therapy before chemotherapy, Table S2: Oocyte cryopreservation results.
Author Contributions
R.A., S.N., M.S. (Miwa Sakamoto) and A.S. conceived and designed the experiments; K.O., M.S. (Megumi Saito) and T.K. analyzed the data; R.A. wrote the manuscript and prepared figures. All authors reviewed the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of Showa University Hospital (23 October 2020, #3307).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable requests.
Conflicts of Interest
The authors declare that the results of this manuscript have not been distorted by research funding or conflict of interest, and that there are no competing interests to declare.
References
- Van Dorp, W.; Mulder, R.L.; Kremer, L.C.M.; Hudson, M.M.; van den Heuvel-Eibrink, M.M.; van den Berg, M.H.; Levine, J.M.; van Dulmen-den Broeder, E.; di Iorgi, N.; Albanese, A.; et al. Recommendations for Premature Ovarian Insufficiency Surveillance for Female Survivors of Childhood, Adolescent, and Young Adult Cancer: A Report From the International Late Effects of Childhood Cancer Guideline Harmonization Group in Collaboration With the PanCareSurFup Consortium. J. Clin. Oncol. 2016, 34, 3440–3450. [Google Scholar] [PubMed]
- Barton, S.E.; Najita, J.S.; Ginsburg, E.S.; Leisenring, W.M.; Stovall, M.; E Weathers, R.; Sklar, C.A.; Robison, L.L.; Diller, L. Infertility, infertility treatment, and achievement of pregnancy in female survivors of childhood cancer: A report from the Childhood Cancer Survivor Study cohort. Lancet Oncol. 2013, 14, 873–881. [Google Scholar] [CrossRef] [Green Version]
- Sklar, C.A.; Mertens, A.C.; Mitby, P.; Whitton, J.; Stovall, M.; Kasper, C.; Mulder, J.; Green, D.; Nicholson, H.S.; Yasui, Y.; et al. Premature Menopause in Survivors of Childhood Cancer: A Report From the Childhood Cancer Survivor Study. JNCI J. Natl. Cancer Inst. 2006, 98, 890–896. [Google Scholar] [CrossRef]
- Oktay, K.; Harvey, B.; Loren, A.W. Fertility Preservation in Patients with Cancer: ASCO Clinical Practice Guideline Update Summary. J. Oncol. Pract. 2018, 14, 381–385. [Google Scholar] [CrossRef]
- Harada, M.; Osuga, Y. Fertility preservation for female cancer patients. Int. J. Clin. Oncol. 2018, 24, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Dolmans, M.-M.; Marinescu, C.; Saussoy, P.; Van Langendonckt, A.; Amorim, C.; Donnez, J. Reimplantation of cryopreserved ovarian tissue from patients with acute lymphoblastic leukemia is potentially unsafe. Blood 2010, 116, 2908–2914. [Google Scholar] [CrossRef] [PubMed]
- Asada, Y.; Morimoto, Y.; Nakaoka, Y.; Yamasaki, T.; Suehiro, Y.; Sugimoto, H.; Yoshida, M.; Irahara, M. Age-specific serum anti-Müllerian hormone concentration in Japanese women and its usefulness as a predictor of the ovarian response. Reprod. Med. Biol. 2017, 16, 364–373. [Google Scholar] [CrossRef] [Green Version]
- Kuwatsuka, Y.; Tomizawa, D.; Kihara, R.; Nagata, Y.; Shiba, N.; Iijima-Yamashita, Y.; Shimada, A.; Deguchi, T.; Miyachi, H.; Tawa, A.; et al. Prognostic value of genetic mutations in adolescent and young adults with acute myeloid leukemia. Int. J. Hematol. 2018, 107, 201–210. [Google Scholar] [CrossRef]
- Gürgen, S.G.; Erdoğan, D.; Elmas, Ç.; Kaplanoğlu, G.T.; Özer, Ç. Chemoprotective effect of ascorbic acid, α-tocopherol, and selenium on cyclophosphamide-induced toxicity in the rat ovarium. Nutrition 2013, 29, 777–784. [Google Scholar] [CrossRef]
- Familiari, G.; Caggiati, A.; Nottola, S.A.; Ermini, M.; di Benedetto, M.R.; Motta, P.M. Ultrastructure of human ovarian primordial follicles after combination chemotherapy for Hodgkin’s disease. Hum. Reprod. 1993, 8, 2080–2087. [Google Scholar] [CrossRef]
- Albanese, R. Induction and transmission of chemically induced chromosome aberrations in female germ cells. Environ. Mol. Mutagen. 1987, 10, 231–243. [Google Scholar] [CrossRef] [PubMed]
- Higdon, R.E.; Marchetti, F.; Mailhes, J.B.; Phillips, G.L. The effects of cisplatin on murine metaphase II oocytes. Gynecol. Oncol. 1992, 47, 348–352. [Google Scholar] [CrossRef]
- Mailhes, J.B.; Marchetti, F.; Young, D. Synergism between gonadotrophins and vinblastine relative to the frequencies of metaphase I, diploid and aneuploid mouse oocytes. Mutagenesis 1995, 10, 185–188. [Google Scholar] [CrossRef]
- Meirow, D.; Epstein, M.; Lewis, H.; Nugent, D.; Gosden, R. Administration of cyclophosphamide at different stages of follicular maturation in mice: Effects on reproductive performance and fetal malformations. Hum. Reprod. 2001, 16, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Levis, A. Detection of aneuploidy in male germ cells of mice by means of a meiotic micronucleus assay. Mutat. Res. Lett. 1992, 281, 187–191. [Google Scholar] [CrossRef]
- Sudman, P.; Rutledge, J.; Bishop, J.; Generoso, W. Bleomycin: Female-specific dominant lethal effects in mice. Mutat. Res. Genet. Toxicol. 1992, 296, 143–156. [Google Scholar] [CrossRef]
- Takami, A. Hematopoietic stem cell transplantation for acute myeloid leukemia. Int. J. Hematol. 2018, 107, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Meirow, D.; Schiff, E. Appraisal of chemotherapy effects on reproductive outcome according to animal studies and clinical data. J. Natl. Cancer Inst. Monogr. 2005, 2005, 21–25. [Google Scholar] [CrossRef] [Green Version]
- Soleimani, R.; Heytens, E.; Darzynkiewicz, Z.; Oktay, K. Mechanisms of chemotherapy-induced human ovarian aging: Double strand DNA breaks and microvascular compromise. Aging 2011, 3, 782–793. [Google Scholar] [CrossRef] [Green Version]
- Ting, A.Y.; Petroff, B.K. Tamoxifen decreases ovarian follicular loss from experimental toxicant DMBA and chemotherapy agents cyclophosphamide and doxorubicin in the rat. J. Assist. Reprod. Genet. 2010, 27, 591–597. [Google Scholar] [CrossRef] [Green Version]
- Mizutani, H.; Tada-Oikawa, S.; Hiraku, Y.; Kojima, M.; Kawanishi, S. Mechanism of apoptosis induced by doxorubicin through the generation of hydrogen peroxide. Life Sci. 2005, 76, 1439–1453. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Gupta, S.; Sharma, R.K. Role of oxidative stress in female reproduction. Reprod. Biol. Endocrinol. 2005, 3, 28–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizzo, A.; Roscino, M.; Binetti, F.; Sciorsci, R. Roles of Reactive Oxygen Species in Female Reproduction. Reprod. Domest. Anim. 2012, 47, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Sugino, N. Reactive oxygen species in ovarian physiology. Reprod. Med. Biol. 2005, 4, 31–44. [Google Scholar] [PubMed]
- Kimball, A.P.; Wilson, M.J. Inhibition of DNA polymerase by beta-D-arabinosylcytosine and reversal of inhibition by deoxycytidine-5′-triphosphate. Proc. Soc. Exp. Biol. Med. 1968, 127, 429–432. [Google Scholar] [CrossRef]
- A Smets, L.; Homan-Blok, J. S1-phase cells of the leukemic cell cycle sensitive to 1-beta-D-arabinofuranosylcytosine at a high-dose level. Cancer Res. 1985, 45, 3113–3117. [Google Scholar]
- Chomienne, C.; Abita, J.P.; Balitrand, N.; Degos, L. Drug association including ara-C in myeloid leukemia cell differentiation: In vitro studies. Semin. Oncol. 1985, 12 (Suppl. S3), 60–64. [Google Scholar]
- Azem, F.; Amit, A.; Merimsky, O.; Lessing, J.B. Successful transfer of frozen-thawed embryos obtained after subtotal colectomy for colorectal cancer and before fluorouracil-based chemotherapy. Gynecol. Oncol. 2004, 93, 263–265. [Google Scholar] [CrossRef]
- Twelves, C.; Wong, A.; Nowacki, M.P.; Abt, M.; Burris, H.; Carrato, A.; Cassidy, J.; Cervantes, A.; Fagerberg, J.; Georgoulias, V.; et al. Capecitabine as Adjuvant Treatment for Stage III Colon Cancer. N. Engl. J. Med. 2005, 352, 2696–2704. [Google Scholar] [CrossRef]
- Burt, R.; Dey, A.; Aref, S.; Aguiar, M.; Akarca, A.; Bailey, K.; Day, W.; Hooper, S.; Kirkwood, A.; Kirschner, K.; et al. Activated stromal cells transfer mitochondria to rescue acute lymphoblastic leukemia cells from oxidative stress. Blood 2019, 134, 1415–1429. [Google Scholar] [CrossRef]
- Morgan, S.; Anderson, R.A.; Gourley, C.; Wallace, W.H.; Spears, N. How do chemotherapeutic agents damage the ovary? Hum. Reprod. Update 2012, 18, 525–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefansdottir, A.; Johnston, Z.C.; Powles-Glover, N.; Anderson, R.A.; Adams, I.R.; Spears, N. Etoposide damages female germ cells in the developing ovary. BMC Cancer 2016, 16, 482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.-L.; Yu, C.; Ji, S.-Y.; Li, X.-M.; Zhang, Y.-P.; Zhang, D.; Zhou, D.; Fan, H.-Y. TOP2β is essential for ovarian follicles that are hypersensitive to chemotherapeutic drugs. Mol. Endocrinol. 2013, 27, 1678–1691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moudi, M.; Go, R.; Yien, C.Y.S.; Nazre, M. Vinca alkaloids. Int. J. Prev. Med. 2013, 4, 1231–1235. [Google Scholar]
- Winship, A.; Carpenter, M.; Griffiths, M.; Hutt, K.J. Vincristine Chemotherapy Induces Atresia of Growing Ovarian Follicles in Mice. Toxicol. Sci. 2019, 169, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Rossi, B.V.; Missmer, S.; Correia, K.F.; Wadleigh, M.; Ginsburg, E.S. Ovarian Reserve in Women Treated for Acute Lymphocytic Leukemia or Acute Myeloid Leukemia with Chemotherapy, but Not Stem Cell Transplantation. ISRN Oncol. 2012, 2012, 956190. [Google Scholar] [CrossRef]
- Decanter, C.; Morschhauser, F.; Pigny, P.; Lefebvre, C.; Gallo, C.; Dewailly, D. Anti-Müllerian hormone follow-up in young women treated by chemotherapy for lymphoma: Preliminary results. Reprod. Biomed. Online 2010, 20, 280–285. [Google Scholar] [CrossRef] [Green Version]
- Chan, J.L.; Johnson, L.N.C.; Efymow, B.L.; Sammel, M.D.; Gracia, C.R. Outcomes of ovarian stimulation after treatment with chemotherapy. J. Assist. Reprod. Genet. 2015, 32, 1537–1545. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).