Abstract
Fibromuscular dysplasia is a non-atherosclerotic, non-inflammatory arteriopathy, considered a rare cause of coronary artery disease. Although familial cases have been described, no specific gene association has been detected so far. When the coronary vessels are involved, the main clinical scenarios are stable angina, acute coronary syndromes, left ventricular dysfunction, and sudden death. Specific clinical and angiographic findings may suggest this as the underlying disease, but certain diagnosis histological. The involvement of the lower and upper limbs is unusual; however, it may have decisive clinical implications for the most appropriate revascularization method and the selection of the arterial graft to be used.
1. Introduction
Fibromuscular dysplasia (FMD) is a rare non-inflammatory and non-atherosclerotic arterial disease that affects multiple vascular beds with a female to male ratio of 9:1 [1], and mainly in middle-aged women. The most affected arterial vessels are the renal arteries, extracranial carotid circulation, and vertebral arteries [1]. However, in the literature, numerous cases have been reported with coronary [2] and peripheral [3,4] involvement. The angiographic aspect is polymorphic and includes focal stenosis, occlusions, and aneurysms up to the classic “string-of-beads” lesions. Both pediatric cases and late adult manifestations have been described [1], with clinical features strictly depending on the affected vascular system. When coronary branches are involved, spontaneous coronary dissection (SCAD) is the most typical manifestation.
2. Clinical Case
A 32-year-old male patient, a current smoker with dyslipidemia and previous cocaine abuse, came to the emergency department with recent typical chest pain on exertion. Six months prior to admission, angioplasty and bilateral external iliac artery stenting had been performed for critical stenosis attributed to atherosclerotic disease. The electrocardiogram on admission showed negative T waves in anterolateral leads consistent with the electrocardiographic evolution of a transient ischemic event (Figure 1A). Blood tests revealed an increase in myocytolysis enzymes (peak troponin T 193 ng/L on day 1, normal values: <14 ng/L). Normal size and thickness of the left ventricle with apical and lateral hypokinesia and preserved global systolic function in the absence of valvular disease or pulmonary hypertension were found in the ultrasound examination. Single antiplatelet therapy, antithrombotic therapy with fondaparinux, antianginal therapy, and high-dose statins were immediately administered, planning an early invasive strategy.
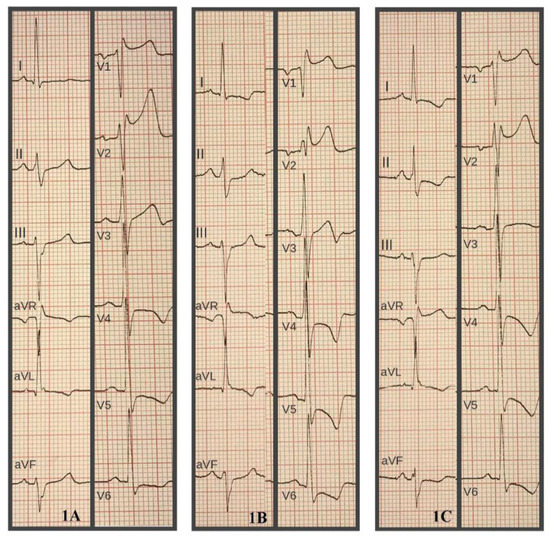
Figure 1.
Dynamic electrocardiographic changes. (A): Electrocardiogram on admission. (B): Recurrence of chest pain; note the ST segment depression in V4-V5-V6. 1 (C): After therapy with beta-blockers and nitrates; modest regression of ischemic alterations.
Because of the recurrence of symptoms at rest with electrocardiographic changes consistent with acute ischemia (Figure 1B), which were responsive to sublingual nitroglycerin and intravenous beta-blockers (Figure 1C), an urgent coronary angiography was performed. Angiography showed multivessel coronary artery disease with critical stenosis of the ostium and middle tract of the left anterior descending artery (LAD) and proximal critical stenosis of the circumflex and marginal branch (Figure 2A). Coronary artery bypass grafting was therefore successfully performed, using left internal mammary artery (LIMA) and single radial graft (Y graft: LIMA to the LAD and radial graft to the circumflex).
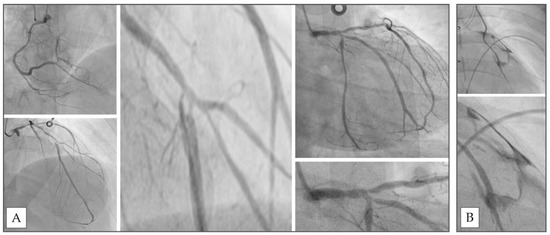
Figure 2.
Coronary angiography. (A): Multivessel disease on admission. (B): Detachment of radial graft with pericardial blush of contrast medium.
On the first postoperative day, a recurrence of chest pain immediately followed by cardiac arrest occurred with electromechanical dissociation. Resuscitation attempts were immediately initiated, and an emergency coronary angiography was performed, showing early graft failure with a spread of contrast medium into the pericardium. Emergency redo surgery was unsuccessfully attempted, and the patient died after several days of mechanical circulatory support. An autopsy was not performed, and a heart specimen was not taken for further histological examination. The left radial artery used as arterial graft was collected for histological analysis; macroscopic examination revealed sub-occlusive nodularities inside the vessel lumen, and fibrointimal thickening with deposition of myxoid matrix consistent with fibrointimal dysplasia was confirmed by microscopic examination (Figure 3).
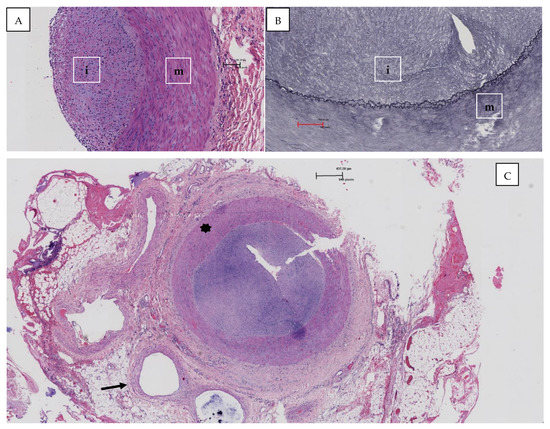
Figure 3.
(A): The microscopic image of the radial artery shows thickening of the intima due to the deposition of myxoid matrix (Hematoxylin and Eosin, magnification 100×, i: intima, m: tunica media); (B): the staining for the elastic fibers shows duplication of the elastic lamina (Weighert, magnification 100×, i: intima, m: tunica media, arrow: elastic lamina); (C): the image shows the vessel affected by intimal fibroplasia with a marked reduction of the lumen (star) in comparison with an adjacent artery (arrow) (Hematoxylin and Eosin, magnification 20×).
3. Discussion
Coronary involvement in FMD is a rare phenomenon, and stable angina, acute coronary syndrome, left ventricular dysfunction, and sudden death are the main disease manifestations [2].
The most unusual differential diagnoses to consider are type IV Ehler Danlos syndrome, Takayasu arteritis, and cocaine vasculitis, which have specific clinical and instrumental features [2,5]. The etiology of FDM is currently unknown; although there is a significant family component, no specific gene association has yet been detected [1,6,7]. To date, there is no specific therapy. If chronic coronary syndrome occurs, a conservative approach seems to be the most advantageous, but in cases of myocardial ischemia refractory to therapies, percutaneous or surgical revascularization is required depending on the anatomical characteristics [8].
Despite the young age of the patient, the history of smoking, untreated dyslipidemia, cocaine abuse, and critical peripheral lower limb artery disease made the likelihood of atherosclerotic disease very high; moreover, no diagnosis of FMD or cocaine vasculitis was detectable in the clinical analysis. Angiography showed multivessel coronary artery disease mainly involving the bifurcation of the left coronary branches and left main non-critical disease. Although SCAD is the most frequent coronary manifestation of FMD, the angiographic images did not present the typical findings, and a diagnosis of multiple dissection was initially ruled out. The patient’s young age, ischemic LAD territory, and anatomical complexity prompted the choice of arterial bypass, despite a Syntax score of 19. Clinical instability occurred in the hours following the angiographic examination, requiring urgent surgical intervention. It is important to note that the radial graft did not show macroscopic changes when it was harvested, and the subocclusive nodularities of the lumen were noticed only afterward by histological examination.
The histological diagnosis performed on the radial graft harvested during redo surgery identified the typical characteristics of FMD, suggesting the presence of coronary artery involvement. Furthermore, the finding of FMD in the arterial graft could justify early postoperative graft detachment complicated by fatal cardiac tamponade.
FMD is a cause of non-atherosclerotic and non-inflammatory vascular disease, with three different histopathological patterns, depending on the predominant site of dysplasia in the artery wall, based on the classification proposed by Harrison and McCormack [8] in 1971 and modified by Stanley et al. [9,10] in 1975. Intimal fibroplasia, which is presented in our case, represents only 2% to 5% of cases of FMD and is angiographically identical to medial hyperplasia. In the literature, only five cases of brachial artery involvement have been described [11], and radial artery involvement seems to have a similar frequency and has been described in association with renal artery FMD [12,13,14,15,16]. These data may be remarkable when choosing which arterial graft to use, especially in young patients with multisite vasculopathy or renal FMD.
When FMD is known or the clinical suspicion of FMD is high, SCAD should always be excluded using invasive imaging techniques if the typical angiographical findings are not present. Moreover, a careful anatomical evaluation of the vessels chosen as grafts must be made, possibly supported by an angiography before sampling.
4. Conclusions
FMD is a rare, non-atherosclerotic, and non-inflammatory arterial disease; coronary vessels can be affected together with other vascular beds. The clinical and angiographic presentation mimics atherosclerosis; definitive diagnosis is histological and can be supported by invasive imaging techniques. SCAD is the most frequent form of presentation and peripheral disease localization is not infrequent, and it can have decisive clinical implications both for the most appropriate revascularization method and the selection of the arterial graft to be used.
Author Contributions
A.L.V. and R.M.: conception, literature review, drafting of the manuscript; F.S.: pathologist, revision of manuscript; C.B.: surgeon, revision of manuscript; R.D.P.: revision of manuscript; B.C.: hemodynamist, revision of manuscript. All authors actively contributed to the review and drafting of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from the subject involved in the study.
Data Availability Statement
No new data were created or analyzed in this study.
Conflicts of Interest
All authors declare no conflict of interest.
References
- Olin, J.W.; Froehlich, J.; Gu, X.; Bacharach, J.M.; Eagle, K.; Gray, B.H.; Jaff, M.R.; Kim, E.S.; Mace, P.; Matsumoto, A.H.; et al. The United States Registry for Fibromuscular Dysplasia: Results in the first 447 patients. Circulation 2012, 125, 3182–3190. [Google Scholar] [CrossRef] [PubMed]
- Michelis, K.C.; Olin, J.W.; Kadian-Dodov, D.; d’Escamard, V.; Kovacic, J.C. Coronary artery manifestations of fibromuscular dysplasia. J. Am. Coll. Cardiol. 2014, 64, 1033–1046. [Google Scholar] [CrossRef] [PubMed]
- Brinza, E.; Grabinski, V.; Durga, S.; O’Connor, S.; Yesenko, S.L.; Kim, E.S.H.; Gornik, H.L. Lower Extremity Fibromuscular Dysplasia: Clinical Manifestations, Diagnostic Testing, and Approach to Management. Angiology 2017, 68, 722–727. [Google Scholar] [CrossRef] [PubMed]
- Antonescu, I.; Knowles, M.; Wirtz, E.; Pascarella, L. An Unusual Case of Bilateral Upper Extremity Ischemia Caused by Forearm Vessel Fibromuscular Dysplasia. Ann. Vasc. Surg. 2019, 56, 353.e7–353.e11. [Google Scholar] [CrossRef] [PubMed]
- Bachi, K.; Mani, V.; Jeyachandran, D.; Fayad, Z.A.; Goldstein, R.Z.; Alia-Klein, N. Vascular disease in cocaine addiction. Atherosclerosis 2017, 262, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Pannier-Moreau, I.; Grimbert, P.; Fiquet-Kempf, B.; Vuagnat, A.; Jeunemaitre, X.; Corvol, P.; Plouin, P.F. Possible familial origin of multifocal renal artery fibromuscular dysplasia. J. Hypertens. 1997, 15 Pt 2, 1797–1801. [Google Scholar] [CrossRef]
- Suzuki, H.; Daida, H.; Sakurai, H.; Yamaguchi, H. Familial fibromuscular dysplasia of bilateral brachial arteries. Heart 1999, 82, 251–252. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Harrison, E.G., Jr.; McCormack, L.J. Pathologic classification of renal arterial disease in renovascular hypertension. Mayo Clin. Proc. 1971, 46, 161–167. [Google Scholar]
- Stanley, J.C.; Gewertz, B.L.; Bove, E.L.; Sottiurai, V.; Fry, W.J. Arterial fibrodysplasia. Histopathologic character and current etiologic concepts. Arch. Surg. 1975, 110, 561–566. [Google Scholar] [CrossRef]
- Lüscher, T.F.; Lie, J.T.; Stanson, A.W.; Houser, O.W.; Hollier, L.H.; Sheps, S.G. Arterial fibromuscular dysplasia. Mayo Clin. Proc. 1987, 62, 931–952. [Google Scholar] [CrossRef]
- Lin, W.W.; McGee, G.S.; Patterson, B.K.; Yao, J.S.; Pearce, W.H. Fibromuscular dysplasia of the brachial artery: A case report and review of the literature. J. Vasc. Surg. 1992, 16, 66–70. [Google Scholar] [CrossRef][Green Version]
- Zucker, M.I.; Craven, J.D.; Eisenman, J.I.; Lynch, K. A problem in hemodialysis management: Fibromuscular dysplasia of radial and ulnar arteries—Report of a case. J. Urol. 1976, 115, 606–607. [Google Scholar] [CrossRef]
- Khatri, V.P.; Gaulin, J.C.; Amin, A.K. Fibromuscular dysplasia of distal radial and ulnar arteries: Uncommon cause of digital ischemia. Ann. Plast Surg. 1994, 33, 652–655. [Google Scholar] [CrossRef] [PubMed]
- Boutouyrie, P.; Gimenez-Roqueplo, A.P.; Fine, E.; Laloux, B.; Fiquet-Kempf, B.; Plouin, P.F.; Jeunemaitre, X.; Laurent, S. Evidence for carotid and radial artery wall subclinical lesions in renal fibromuscular dysplasia. J. Hypertens. 2003, 21, 2287–2295. [Google Scholar] [CrossRef] [PubMed]
- Gharib, B.; Ghareh Zadeh Shirazi, A.; Moradi, E.; Yaghmaei, B.; Ziaee, V. A rare disease with a rare presentation: Hemi-atrophy caused by fibromuscular dysplasia in a 27 month old girl. Reumatismo 2019, 71, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Kesler, W.W., 3rd; Maleszewski, J.J.; Payatakes, A.H. Spontaneous radial artery pseudoaneurysm in an infant due to idiopathic medial hypoplasia—A case report. Case Rep. Plast Surg. Hand Surg. 2019, 6, 69–73. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).