Review of Studies Reporting the Incidence of Acute Type B Aortic Dissection


Abstract
1. Introduction
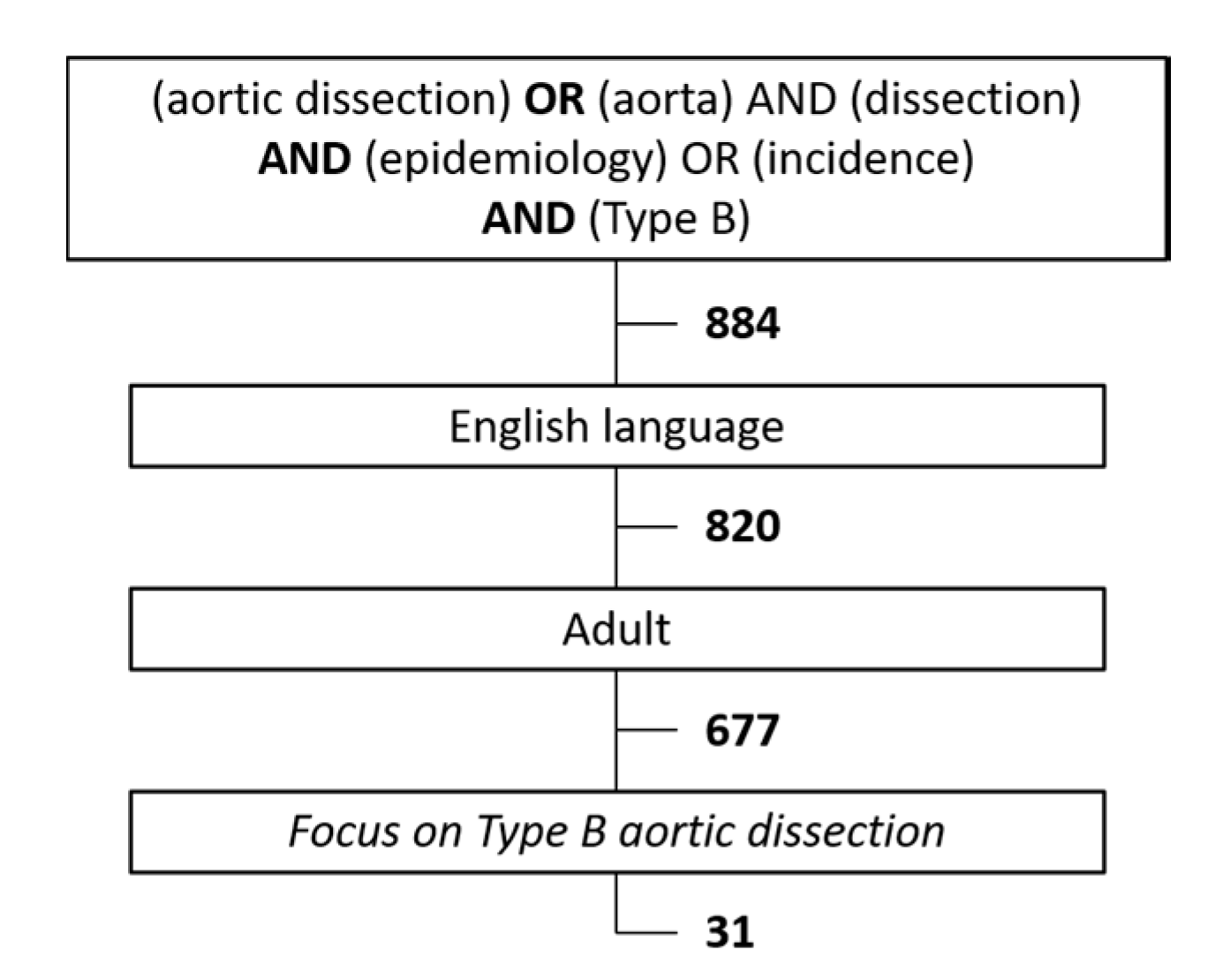
2. Materials and Methods
3. Results
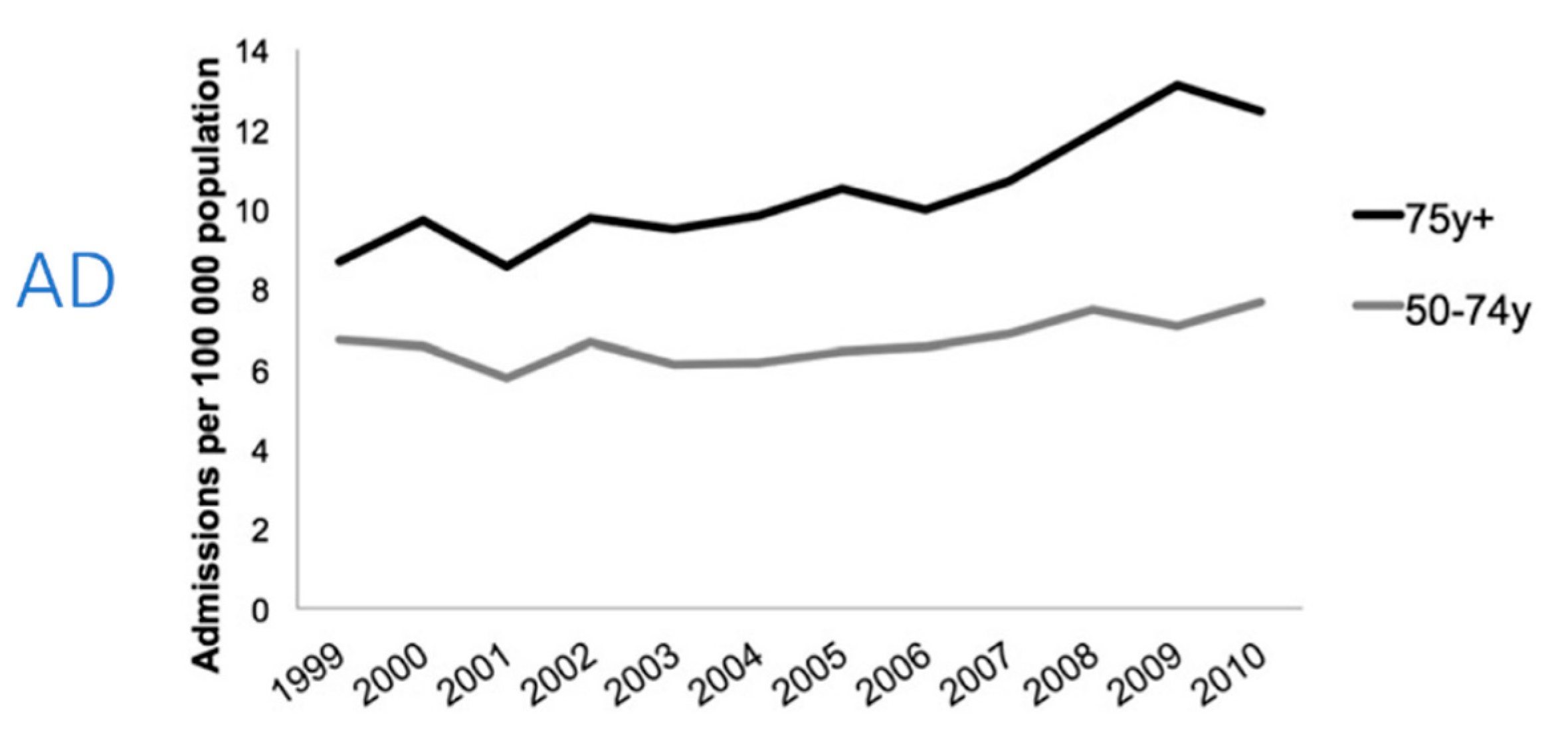
3.1. Health Episode Statistics
3.2. Prospective Epidemiological Studies
3.3. Disease Specific Registries
3.4. Clinical Studies (Hospitalisation)
3.4.1. Sweden
3.4.2. Italy
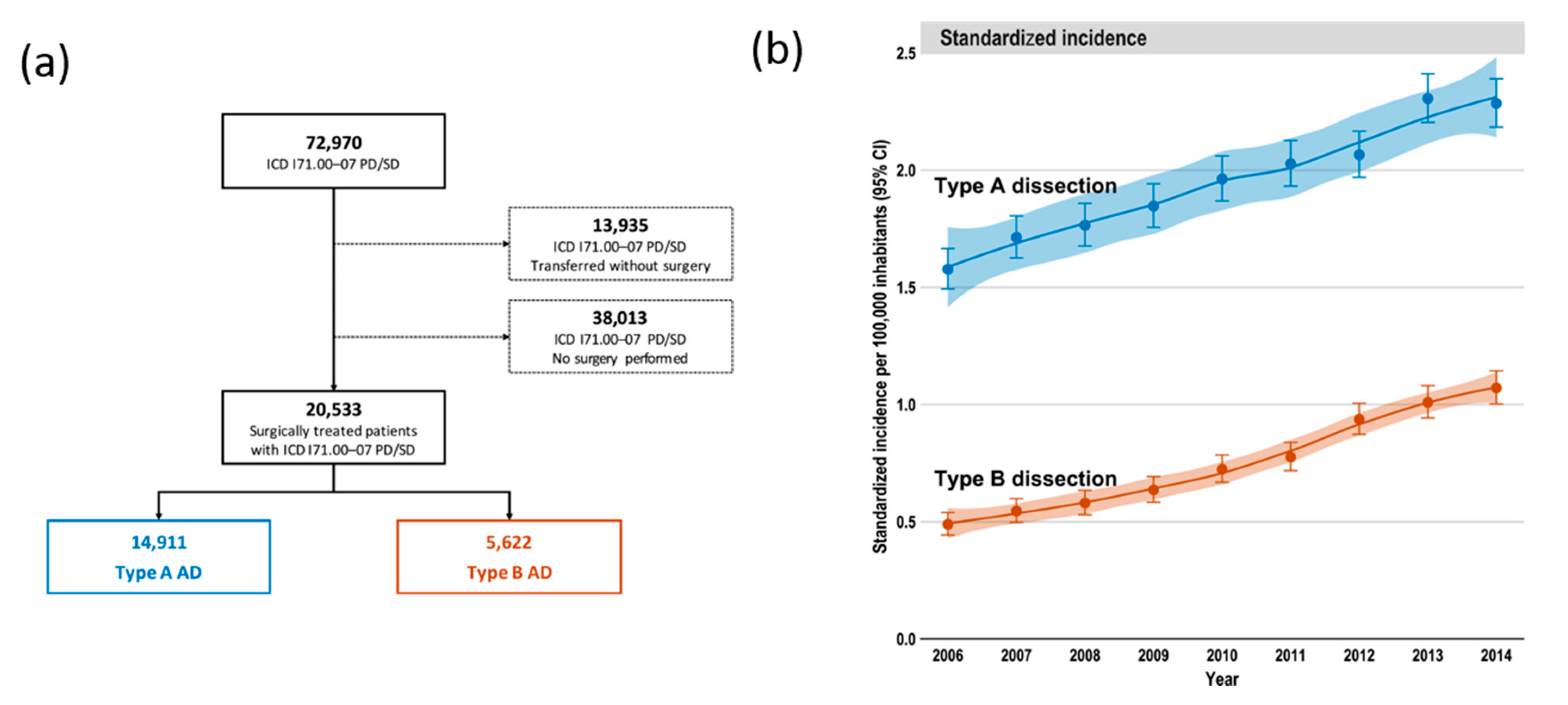
3.4.3. Germany
3.4.4. Hungary
3.4.5. Canada
3.4.6. Mainland China
3.4.7. Japan
4. Discussion
Funding
Conflicts of Interest
References
- Howard, D.P.J.; Banerjee, A.; Fairhead, J.F.; Perkins, J.; Silver, L.E.; Rothwell, P.M. Population-based study of incidence and outcome of acute aortic dissection and premorbid risk factor control clinical perspective: 10-year results from the Oxford vascular study. Circulation 2013, 127, 2031–2037. [Google Scholar] [CrossRef] [PubMed]
- Bottle, A.; Mariscalco, G.; Shaw, M.A.; Benedetto, U.; Saratzis, A.; Mariani, S.; Bashir, M.; Aylin, P.; Jenkins, D.; Oo, A.Y.; et al. Unwarranted Variation in the Quality of Care for Patients with Diseases of the Thoracic Aorta. J. Am. Heart Assoc. 2017, 6, e004913. [Google Scholar] [CrossRef] [PubMed]
- Waton, S. (Royal College of Surgeons of England, London, UK). Personal communication, 2019.
- National Vascular Regsitry 2019 Annual Report. Available online: https://www.vsqip.org.uk/content/uploads/2019/12/NVR-2019-Annual-Report.pdf (accessed on 15 October 2020).
- Brunkwall, J.; Kasprzak, P.; Verhoeven, E.; Heijmen, R.; Taylor, P.; Alric, P.; Canaud, L.; Janotta, M.; Raithel, D.; Malina, M.; et al. Endovascular repair of acute uncomplicated aortic type B dissection promotes aortic remodelling: 1 year results of the ADSORB trial. Eur. J. Vasc. Endovasc. Surg. 2014, 48, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Nienaber, C.A.; Kische, S.; Rousseau, H.; Eggebrecht, H.; Rehders, T.C.; Kundt, G.; Glass, A.; Scheinert, D.; Czerny, M.; Kleinfeldt, T.; et al. Endovascular repair of type B aortic dissection: Long-term results of the randomized investigation of stent grafts in aortic dissection trial. Circ. Cardiovasc. Interv. 2013, 6, 407–416. [Google Scholar] [CrossRef] [PubMed]
- von Allmen, R.S.; Anjum, A.; Powell, J.T. Incidence of descending aortic pathology and evaluation of the impact of thoracic endovascular aortic repair: A population-based study in England and Wales from 1999 to 2010. Eur. J. Vasc. Endovasc. Surg. 2013, 45, 154–159. [Google Scholar] [CrossRef][Green Version]
- Olsson, C.; Thelin, S.; Ståhle, E.; Ekbom, A.; Granath, F. Thoracic aortic aneurysm and dissection: Increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation 2006, 114, 2611–2618. [Google Scholar] [CrossRef]
- Reutersberg, B.; Salvermoser, M.; Trenner, M.; Geisbüsch, S.; Zimmermann, A.; Eckstein, H.-H.; Kuehnl, A. Hospital Incidence and In-Hospital Mortality of Surgically and Interventionally Treated Aortic Dissections: Secondary Data Analysis of the Nationwide German Diagnosis-Related Group Statistics From 2006 to 2014. J. Am. Heart Assoc. 2019, 8, e011402. [Google Scholar] [CrossRef]
- Mody, P.S.; Wang, Y.; Geirsson, A.; Kim, N.; Desai, M.M.; Gupta, A.; Dodson, J.A.; Krumholz, H.M. Trends in aortic dissection hospitalizations, interventions, and outcomes among Medicare beneficiaries in the United States, 2000–2011. Circ. Cardiovasc. Qual. Outcomes 2014, 7, 920–992. [Google Scholar] [CrossRef]
- Jones, D.W.; Goodney, P.P.; Nolan, B.W.; Brooke, B.S.; Fillinger, M.F.; Powell, R.J.; Stone, D.H. National trends in the utilization, mortality, and survival after repair of type B aortic dissection in the Medicare population. JVS 2014, 60, 11–19. [Google Scholar] [CrossRef]
- Wang, G.J.; Jackson, B.M.; Foley, P.J.; Damrauer, S.M.; Goodney, P.P.; Kelz, R.R.; Wirtalla, C.; Fairman, R.M. National trends in admissions, repair, and mortality for thoracic aortic aneurysm and type B dissection in the National Inpatient Sample. J. Vasc. Surg. 2018, 67, 1649–1658. [Google Scholar] [CrossRef]
- Xia, L.; Li, J.H.; Zhao, K.; Wu, H.Y. Incidence and in-hospital mortality of acute aortic dissection in China: Analysis of China Health Insurance Research (CHIRA) Data 2011. J. Geriatr. Cardiol. 2015, 12, 502–506. [Google Scholar] [PubMed]
- Yu, H.Y.; Chen, Y.S.; Huang, S.C.; Chiu, C.C.; Lai, W.T.; Huang, B. Late outcome of patients with aortic dissection: Study of a national database. Eur. J. Cardiothorac. Surg. 2004, 25, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Yeh, T.Y.; Chen, C.Y.; Huang, J.W.; Chiu, C.C.; Lai, W.T.; Huang, Y.B. Epidemiology and Medication Utilization Pattern of Aortic Dissection in Taiwan. A Population-Based Study. Medicine 2015, 94, e1522. [Google Scholar] [CrossRef] [PubMed]
- Dias, R.R.; Mejia, O.A.V.; Fernandes, F.; Ramires, F.J.A.; Mady, C.; Stolf, N.A.G.; Jatene, F.B. Mortality impact of thoracic aortic disease in São Paulo state from 1998 to 2007. Arquivos Brasileiros Cardiol. 2013, 101, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Trujillo, I.; González-Pascual, M.; Jiménez-García, R.; Hernández-Barrera, V.; Miguel-Yanes, J.M.; Méndez-Bailón, M.; de Miguel-Diez, J.; Salino-Fort, M.A.; Perez-Farinos, N.; Carrosco-Garrido, P.; et al. Type 2 Diabetes Mellitus and Thoracic Aortic Aneurysm and Dissection. An Observational Population-Based Study in Spain from 2001 to 2012. Medicine 2016, 95, e3618. [Google Scholar]
- Smedberg, C.; Steuer, J.; Leander, K.; Hultgren, R. Sex differences and temporal trends in aortic dissection: A population-based study of incidence, treatment strategies, and outcome in Swedish patients during 15 years. Eur. Heart J. 2020, 41, 2430–2438. [Google Scholar] [CrossRef]
- Avdic, T.; Franzén, S.; Zarrouk, M.; Acosta, S.; Nilsson, P.; Gottsäter, A.; Svensson, A.-M.; Gudbjörnsdottir, S.; Eliassön, B. Reduced Long-Term Risk of Aortic Aneurysm and Aortic Dissection Among Individuals with Type 2 Diabetes Mellitus: A Nationwide Observational Study. J. Am. Heart Assoc. 2018, 7, e007618. [Google Scholar] [CrossRef]
- Clouse, W.D.; Hallett, J.W.; Schaff, H.V.; Spittell, P.C.; Rowland, C.M.; Ilstrup, D.M.; Melton, L.J. Acute aortic dissection: Population-based incidence compared with degenerative aortic aneurysm rupture. Mayo Clin. Proc. 2004, 79, 176–180. [Google Scholar] [CrossRef]
- DeMartino, R.R.; Sen, I.; Huang, Y.; Bower, T.C.; Oderich, G.S.; Pochettino, A.; Greason, K.; Kalra, M.; Johnstone, J.; Shuja, F.; et al. A Population-Based Assessment of the Incidence of Aortic Dissection, Intramural Hematoma and Penetrating Ulcer, and Its Associated Mortality from 1995 to 2015. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004689. [Google Scholar] [CrossRef]
- Melvinsdottir, I.H.; Lund, S.H.; Agnarsson, B.A.; Sigvaldason, K.; Gudbjartsson, T.; Geirsson, A. The incidence and mortality of acute thoracic aortic dissection: Results from a whole nation study. Eur. J. Cardiothorac. Surg. 2016, 50, 1111–1117. [Google Scholar] [CrossRef]
- Landenhed, M.; Engström, G.; Gottsäter, A.; Caulfield, M.P.; Hedblad, B.; Newton-Cheh, C.; Melander, O.; Smith, J.G. Risk profiles for aortic dissection and ruptured or surgically treated aneurysms: A prospective cohort study. J. Am. Heart Assoc. 2015, 4, e001513. [Google Scholar] [CrossRef]
- Hagan, P.G.; Nienaber, C.A.; Isselbacher, E.M.; Bruckman, D.; Karavite, D.J.; Russman, P.L.; Evangelista, A.; Fattori, R.; Suzuki, T.; Oh, J.K.; et al. The International Registry of Acute Aortic Dissection (IRAD): New insights into an old disease. JAMA 2000, 283, 897–903. [Google Scholar] [CrossRef]
- Pape, L.A.; Awais, M.; Woznicki, E.M.; Suzuki, T.; Trimarchi, S.; Evangelista, A.; Myrmel, T.; Larsen, M.; Harris, K.M.; Greason, K.; et al. Presentation, diagnosis, and outcomes of acute aortic dissection: 17-year trends from the International Registry of Acute Aortic Dissection. J. Am. Coll. Cardiol. 2015, 66, 350–358. [Google Scholar] [CrossRef]
- Wang, D.J.; Fan, F.D.; Wang, Q.; Li, Q.G.; Zhou, Q.; Wu, Q.; Shi, G.F. Preliminary Characterization of Acute Aortic Dissection in the Mainland of China. Med. J. 2011, 124, 1726–1730. [Google Scholar]
- Yamaguchi, T.; Nakai, M.; Sumita, Y.; Miyamoto, Y.; Matsuda, H.; Inoue, Y.; Yoshino, H.; Okita, Y.; Minatoya, K.; Ueda, Y.; et al. Current Status of the Management and Outcomes of Acute Aortic Dissection in Japan: Analyses of Nationwide Japanese Registry of All Cardiac and Vascular Diseases-Diagnostic Procedure Combination Data. Eur. Heart J. Acute Cardiovasc. Care 2019. [Google Scholar] [CrossRef]
- Acosta, S.; Gottsäter, A. Stable population-based incidence of acute type A and B aortic dissection. Scand. Cardiovasc. J. 2019, 53, 274–279. [Google Scholar] [CrossRef]
- Pacini, D.; Di Marco, L.; Fortuna, D.; Belotti, L.M.B.; Gabbieri, D.; Zussa, C.; Pigini, F.; Contini, A.; Barattoni, M.C.; De Palma, R.; et al. Acute aortic dissection: Epidemiology and outcomes. Int. J. Cardiol. 2013, 167, 2806–2812. [Google Scholar] [CrossRef]
- Ante, M.; Mylonas, S.; Bischoff, M.; Rengier, F.; Brunkwall, J.; Bockler, D. Prevalence of the Computed Tomographic Morphological DISSECT Predictors in Uncomplicated Stanford Type B Aortic Dissection. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 525–533. [Google Scholar] [CrossRef]
- Mészáros, I.; Mórocz, J.; Szlávi, J.; Schmidt, J.; Tornóci, L.; Nagy, L.; Szép, L. Epidemiology and clinicopathology of aortic dissection. Chest 2000, 117, 1271–1278. [Google Scholar] [CrossRef]
- McClure, R.S.; Brogly, S.B.; Lajkosz, K.; Payne, D.; Hall, S.F.; Johnson, A.P. Epidemiology and management of thoracic aortic dissections and thoracic aortic aneurysms in Ontario, Canada: A population-based study. J. Thorac. Cardiovasc. Surg. 2018, 155, 2254–2264. [Google Scholar] [CrossRef]
- Li, Y.; Yang, N.; Duan, W.; Liu, S.; Yi, D. Acute aortic dissection in China. Am. J. Cardiol. 2012, 110, 1056–1061. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Chen, C.; Wu, Z.; Chen, D.; Guo, W. Recent evolution in use and effectiveness in mainland China of thoracic endovascular aortic repair of type B aortic dissection. Sci. Rep. 2017, 7, 17350. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Duan, W.; Xue, Y.; Wang, L.; Liu, J.; Yu, S.; Yi, D.; Registry of Aortic Dissection in China Sino-RAD Investigators. Clinical features of acute aortic dissection from the Registry of Aortic Dissection in China. J. Thorac. Cardiovasc. Surg. 2014, 148, 2995–3000. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Chan, Y.C.; Cheng, S.W. Contemporary endovascular treatment of type B aortic dissection in China. Asian Cardiovasc. Thorac. Ann. 2016, 24, 739–749. [Google Scholar] [CrossRef] [PubMed]
- Xia, L.; Huang, L.; Feng, X.; Xiao, J.; Wei, X.; Yu, X. Chronobiological patterns of acute aortic dissection in central China. Heart 2020. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, T.; Adachi, H.; Ohuchida, M.; Nakamura, T.; Satoh, A.; Jacobs, D.R.; Imaizumi, T. A case-control study found that low albumin and smoking were associated with aortic dissection. J. Clin. Epidemiol. 2004, 57, 386–391. [Google Scholar] [CrossRef]
- Rylski, B.; Hoffmann, I.; Beyersdorf, F.; Suedkamp, M.; Siepe, M.; Nitsch, B.; Blettner, M.; Borger, M.A.; Weigang, E. Acute aortic dissection type A: Age-related management and outcomes reported in the German Registry for Acute Aortic Dissection Type A (GERAADA) of over 2000 patients. Ann. Surg. 2014, 259, 598–604. [Google Scholar] [CrossRef]
- Takeuchi, S.; Yamaguchi, Y.; Soejima, K.; Yoshino, H. Incidence and characteristics of acute aortic dissection in patients with out-of-hospital cardiopulmonary arrest evaluated by non-contrast computed tomography. Eur. Heart J. Acute Cardiovasc. Care 2020. [Google Scholar] [CrossRef]
- Chen, Y.; Zhang, S.; Liu, L.; Lu, Q.; Zhang, T.; Jing, T. Retrograde Type A Aortic Dissection after Thoracic Endovascular Aortic Repair: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2017, 6, e004649. [Google Scholar] [CrossRef]
- Hossack, M.; Patel, S.; Gambardella, I.; Neequaye, S.; Antoniou, G.A.; Torella, F. Endovascular vs. Medical Management for Uncomplicated Acute and Sub-acute Type B Aortic Dissection: A Meta-analysis. JVEVS 2020, 59, 794–807. [Google Scholar] [CrossRef]
- Zhao, X.; Chen, J.; Cui, Y.; Wu, F.; Hu, D. Current status of primary hypertension in China: An epidemiological study of 12 provinces, 1 autonomous region and 1 municipality. Natl. Med. J. China 2006, 86, 1148–1152. [Google Scholar]
- World Health Organisation: Prevalence of Tobacco Smoking. Available online: http://gamapserver.who.int/gho/interactive_charts/tobacco/use/atlas.html (accessed on 15 October 2020).
- Herrett, E.; Shah, A.D.; Boggon, R.; Denaxas, S.; Smeeth, L.; van Staa, T.; Timmis, A.; Hemingway, H. Completeness and diagnostic validity of recording acute myocardial infarction events in primary care, hospital care, disease registry, and national mortality records: Cohort study. BMJ 2013, 346, f2350. [Google Scholar] [CrossRef]
- Bright, R.A.; Avorn, J.; Everitt, D.E. Medicaid data as a resource for epidemiologic studies: Strengths and limitations. J. Clin. Epidemiol. 1989, 42, 937–945. [Google Scholar] [CrossRef]
- Schneeweiss, S.; Avorn, J. A review of uses of health care utilization databases for epidemiologic research on therapeutics. J. Clin. Epidemiol. 2005, 58, 323–337. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, A.; Begaj, I.; Thorne, S. Aortic dissection in pregnancy in England: An incidence study using linked national databases. BMJ Open 2015, 5, e008318. [Google Scholar] [CrossRef] [PubMed]
- Erbel, R.; Aboyans, V.; Boileau, C.; Bossone, E.; Bartolomeo, R.; Eggebrecht, H.; Evangelista, A.; Falk, V.; Frank, H.; Gaemperli, O.; et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases. Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2015, 36, 2779–2926. [Google Scholar] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (http://creativecommons.org/licenses/by/4.0/).Authors | Years Studied | Study Size (n) | Age | Male (%) | Incidence Per 100,000 Person Years | Operated TBAD (%) | Trend Over time | |
|---|---|---|---|---|---|---|---|---|
| AD | TBAD | |||||||
| Population based studies 1 | ||||||||
| Landenhead, et al. [23] | 1991–2011 | 70 | 62 | 66% | 15 | 6.3 | - | - |
| Mészáros, et al. [31] | 1973–2000 | 84 | 66 | 64% | 2.9 | - | - | - |
| Olsson, et al. [8] | 1987–2002 | 4425 | 70 | 62% | - | - | - | ↑ |
| Dias, et al. [16] | 1998–2007 | 10,019 | - | 58% | - | - | - | ↑ |
| Howard, et al. [1] | 2002–2012 | 59 | 72 | 60% | 6.0 | 1.7 | 26% | - |
| Melvinsdottir, et al. [22] | 1992–2013 | 153 | 67 | 61% | 2.5 | 1.0 | 26% | → |
| Clouse, et al. [20] DeMartino, et al. [21] | 1980–1994 | 39 | 67 | 64% | 2.6–3.5 | 0.5 | - | ↑ |
| 1995–2015 | 77 | 72 | 57% | 4.4 | - | - | → | |
| Acosta & Gottsäter [28] | 2000–2004 2014–2016 | 73 32 | 73 61 | 55% 56% | 5.5 3.3 | 2.1 0.9 | - 18% | - ↓ |
| Smedberg, et al. [18] | 2002–2016 | 8057 | 68 | 64% | 7.2 | - | - | ↓ |
| Hospital based studies | ||||||||
| Yu, et al. [14] | 1996–2001 | 5654 | 64 | 69% | 4.3 | - | - | - |
| Pacini, et al. [29] | 2000–2008 | 1449 | 68 | 64% | 4.7 | - | - | ↑ |
| von Allmen, et al. [7] | 1999–2010 | - | - | - | 7.2–8.8 | - | 53% | ↑ |
| Mody, et al. [10] | 2000–2011 | 32,057 | 77 | 48–53% | 10 | - | 30% | → |
| Li, et al. [33] | 2008–2011 | 1812 | 51 | 77% | - | - | 76% | - |
| Xia, et al. [13] | 2011 | 65 | 59 | 72% | 2.0 1 | - | 35% | - |
| Wang, et al. [12] | 2000–2012 | 46,869 | 67 | 58% | - | - | 23% | ↑ |
| Yeh, et al. [15] | 2005–2012 | 9092 | 64 | 72% | 5.6 | - | 13% | ↑ |
| McClure, et al. [32] | 2002–2014 | 5966 | 66 | 61% | 4.6 | 2.8 | 17% | ↑ |
| Reutersberg, et al. [9] Operated Type A: Operated Type B: | 2006–2014 | - 72,970 148,115,622 | - 64 66 | - 65% 71% | 2.8 - - | - - - | 27% - - | ↑ |
| Xia et al. [37] | 2011–2018 | 2048 | 53 | 81% | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brooks, M. Review of Studies Reporting the Incidence of Acute Type B Aortic Dissection. Hearts 2020, 1, 152-165. https://doi.org/10.3390/hearts1030016
Brooks M. Review of Studies Reporting the Incidence of Acute Type B Aortic Dissection. Hearts. 2020; 1(3):152-165. https://doi.org/10.3390/hearts1030016
Chicago/Turabian StyleBrooks, Marcus. 2020. "Review of Studies Reporting the Incidence of Acute Type B Aortic Dissection" Hearts 1, no. 3: 152-165. https://doi.org/10.3390/hearts1030016
APA StyleBrooks, M. (2020). Review of Studies Reporting the Incidence of Acute Type B Aortic Dissection. Hearts, 1(3), 152-165. https://doi.org/10.3390/hearts1030016