
Automatic Classification of Melanoma Skin Cancer with Deep Convolutional Neural Networks


Abstract
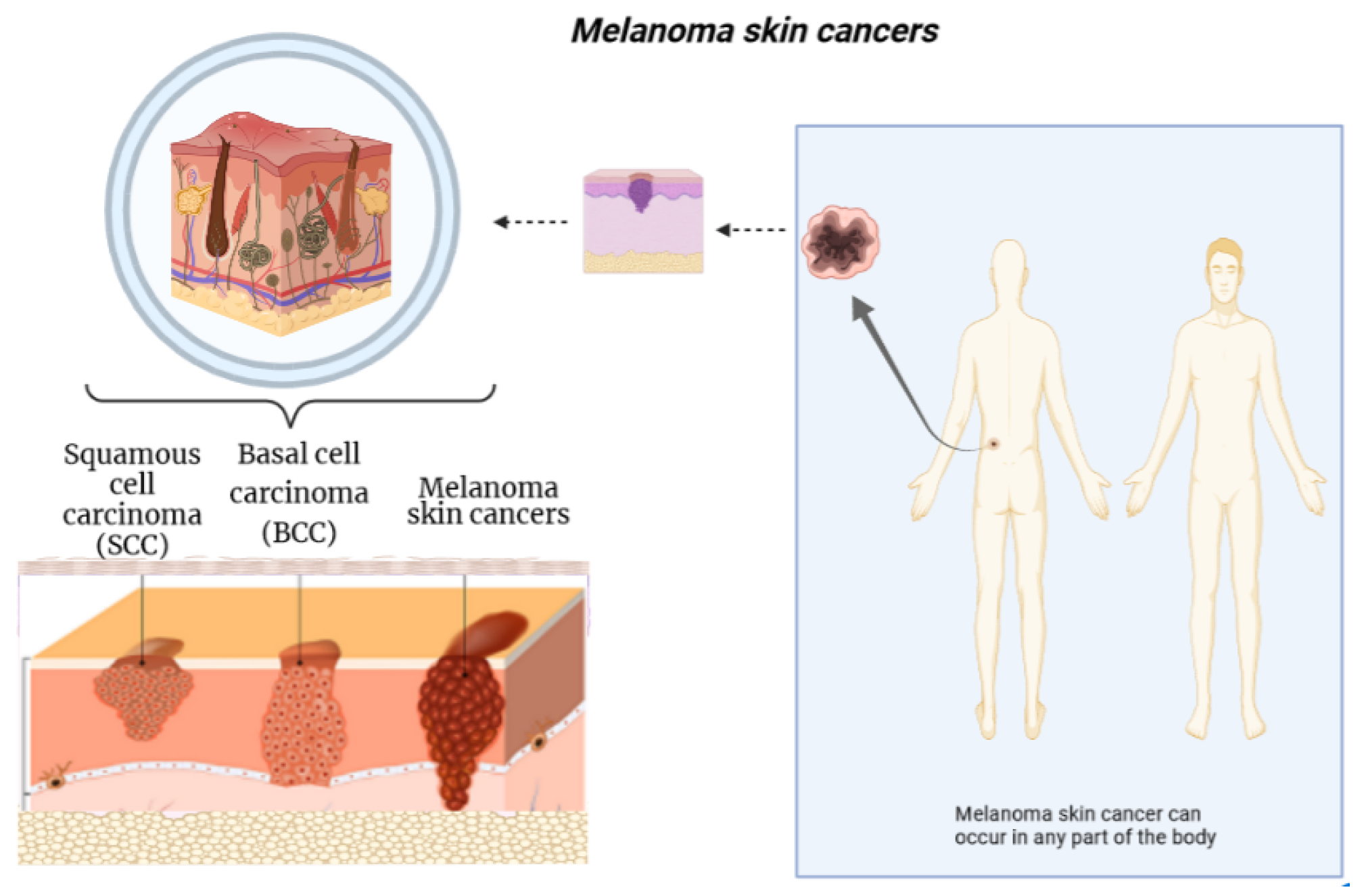
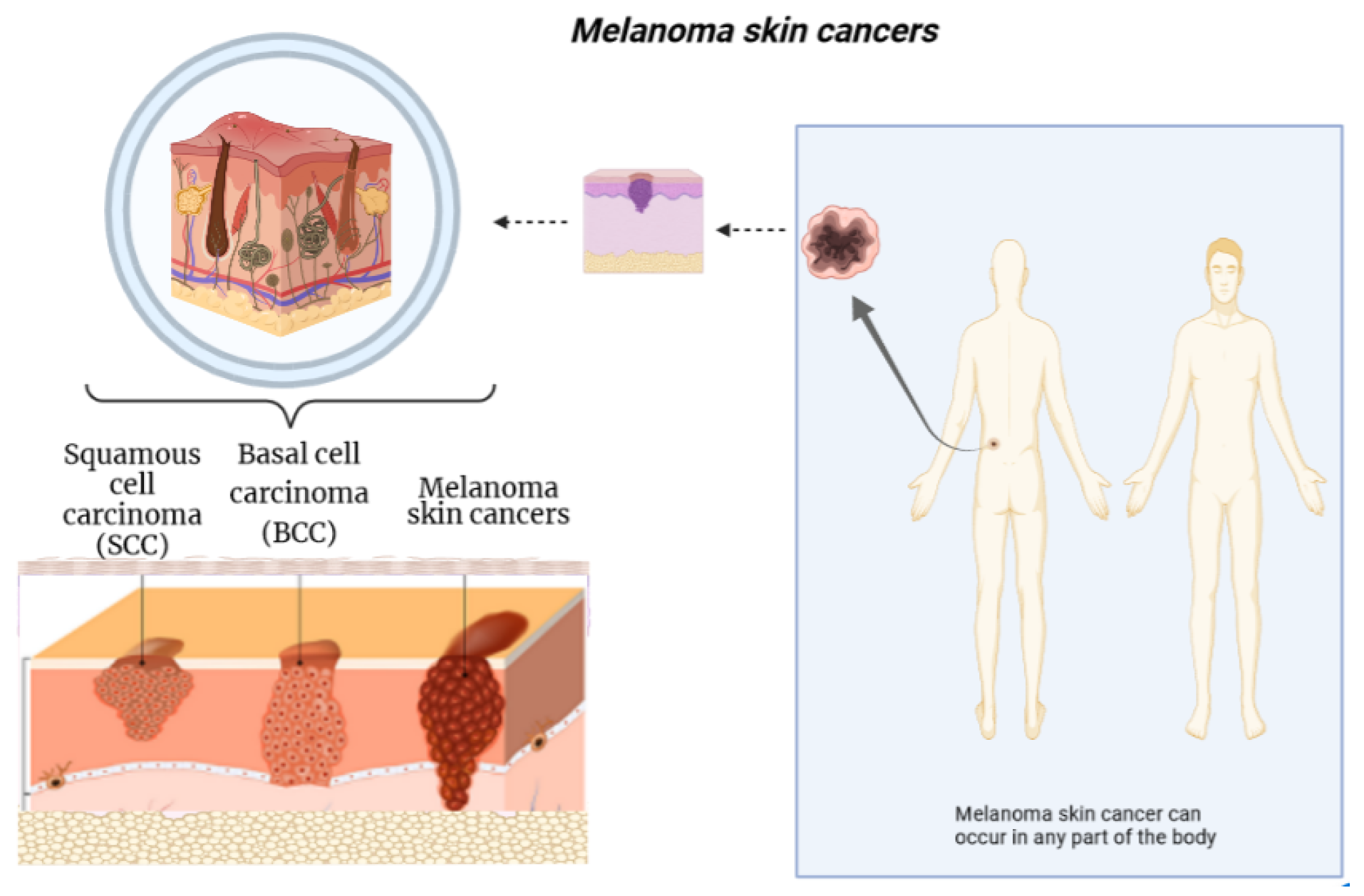
:1. Background
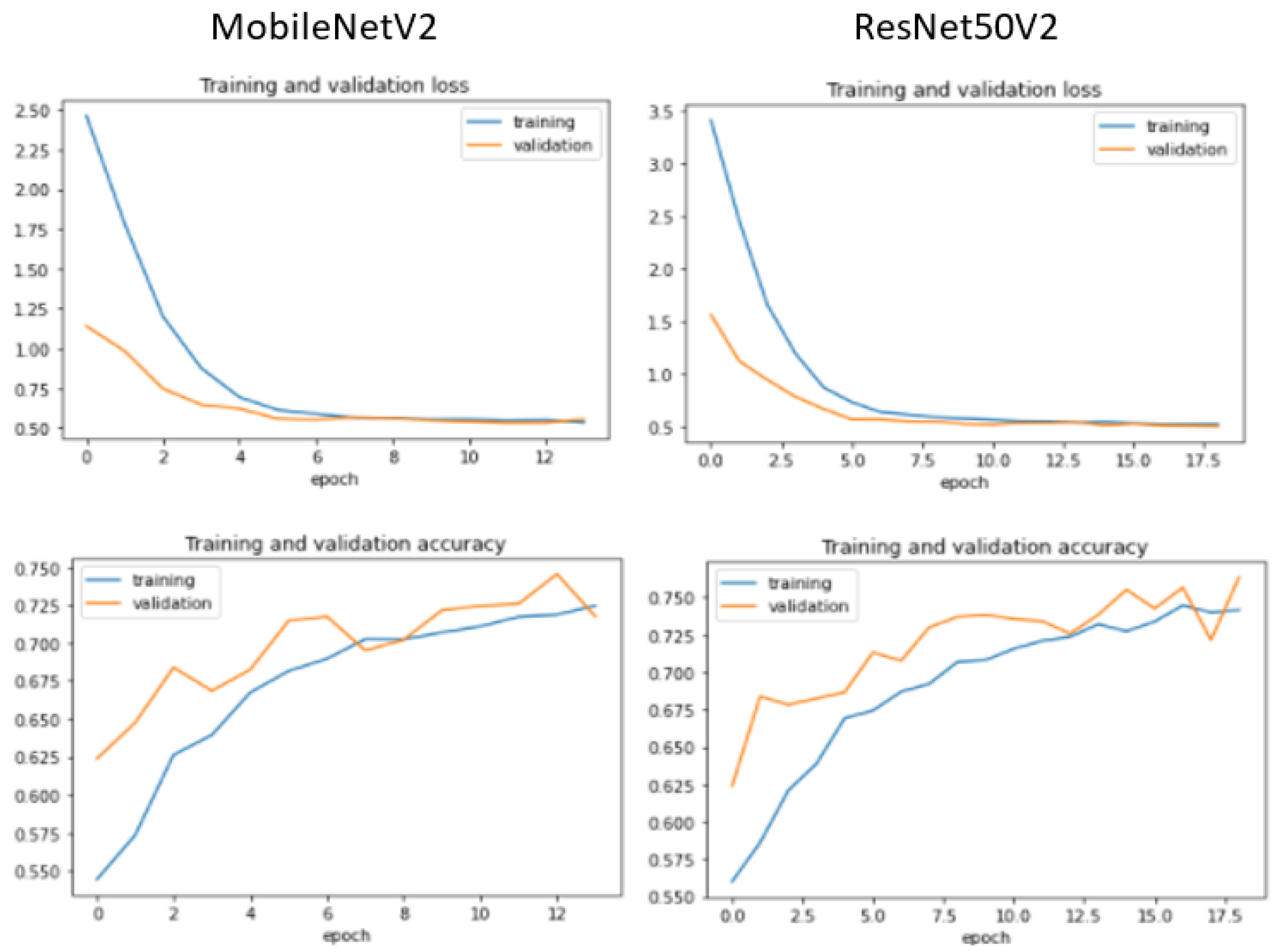
- Unlike existing studies, we include recent (and previous state-of-the-art) deep learning (DL) architectures to comprehensively investigate their performance differences. The utilized DL architectures in this study include DenseNet201, MobileNetV2, ResNet50V2, ResNet152V2, Xception, VGG16, VGG19, and GoogleNet.
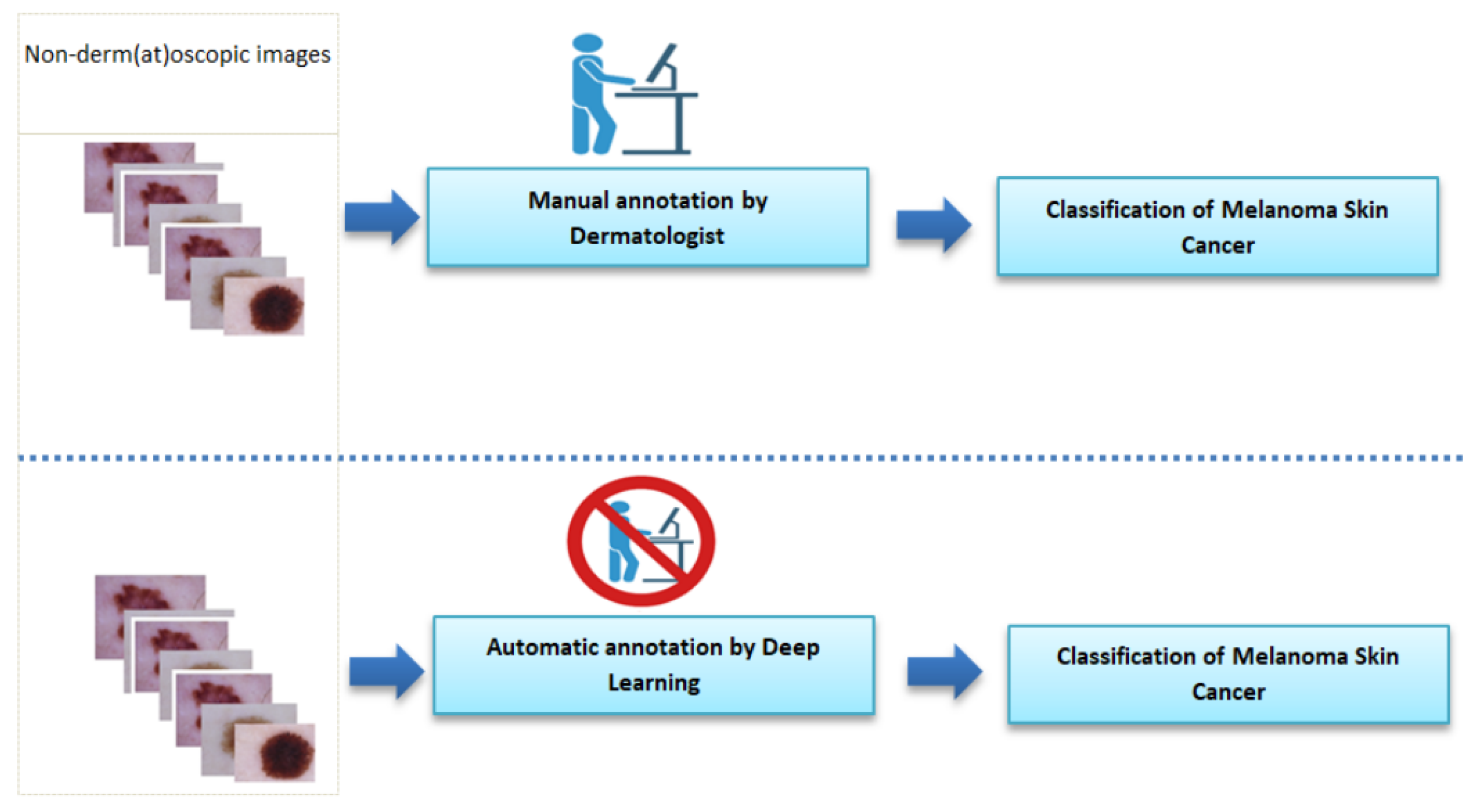
- As the accurate prediction performance is of great importance in the melanoma skin cancer classification task, therefore, we aimed to identify the best-performing deep learning model to assist dermatologists in finding the appropriate AI tool.
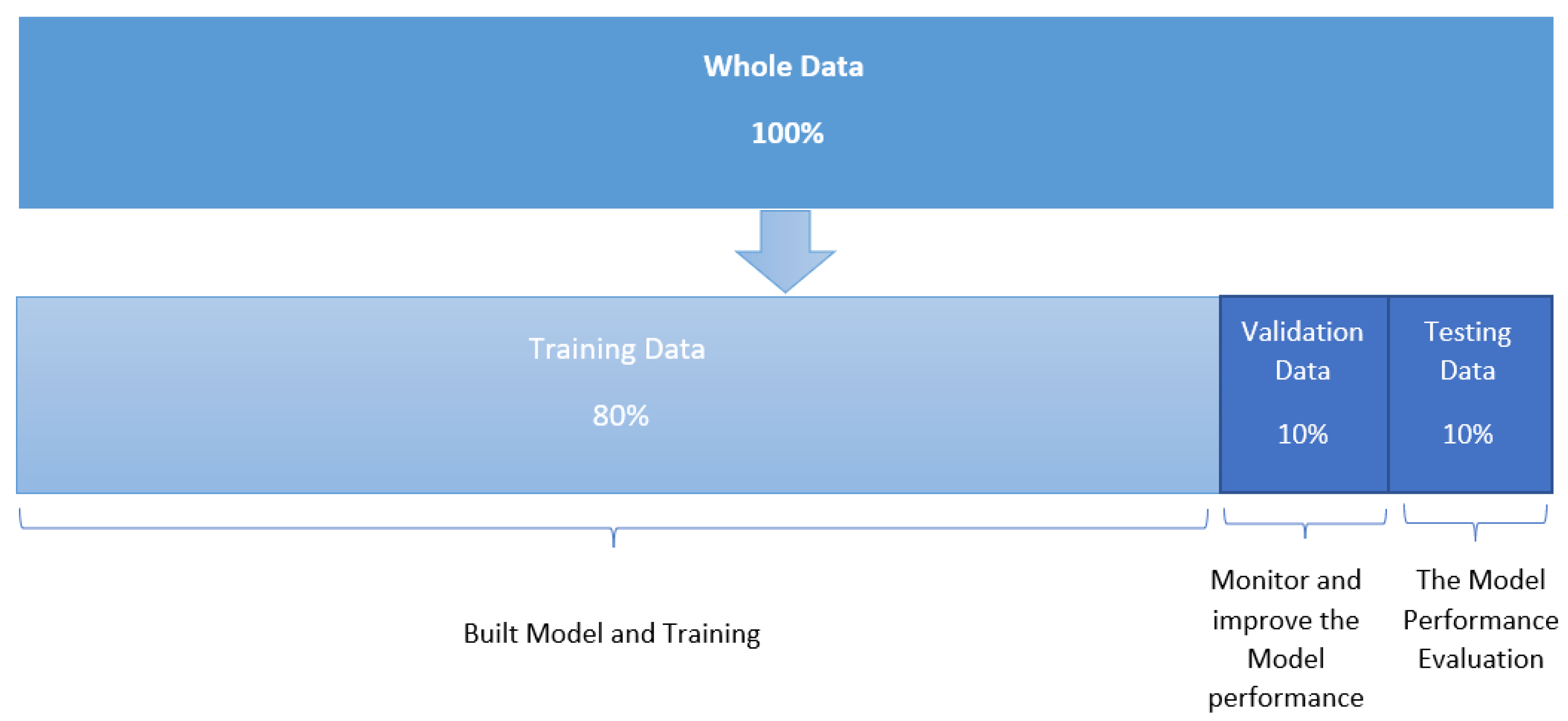
- We report training results of all DL architectures in this study. Moreover, we record the generalization performance results using the ISIC benchmark dataset pertaining to the melanoma skin cancer classification task.
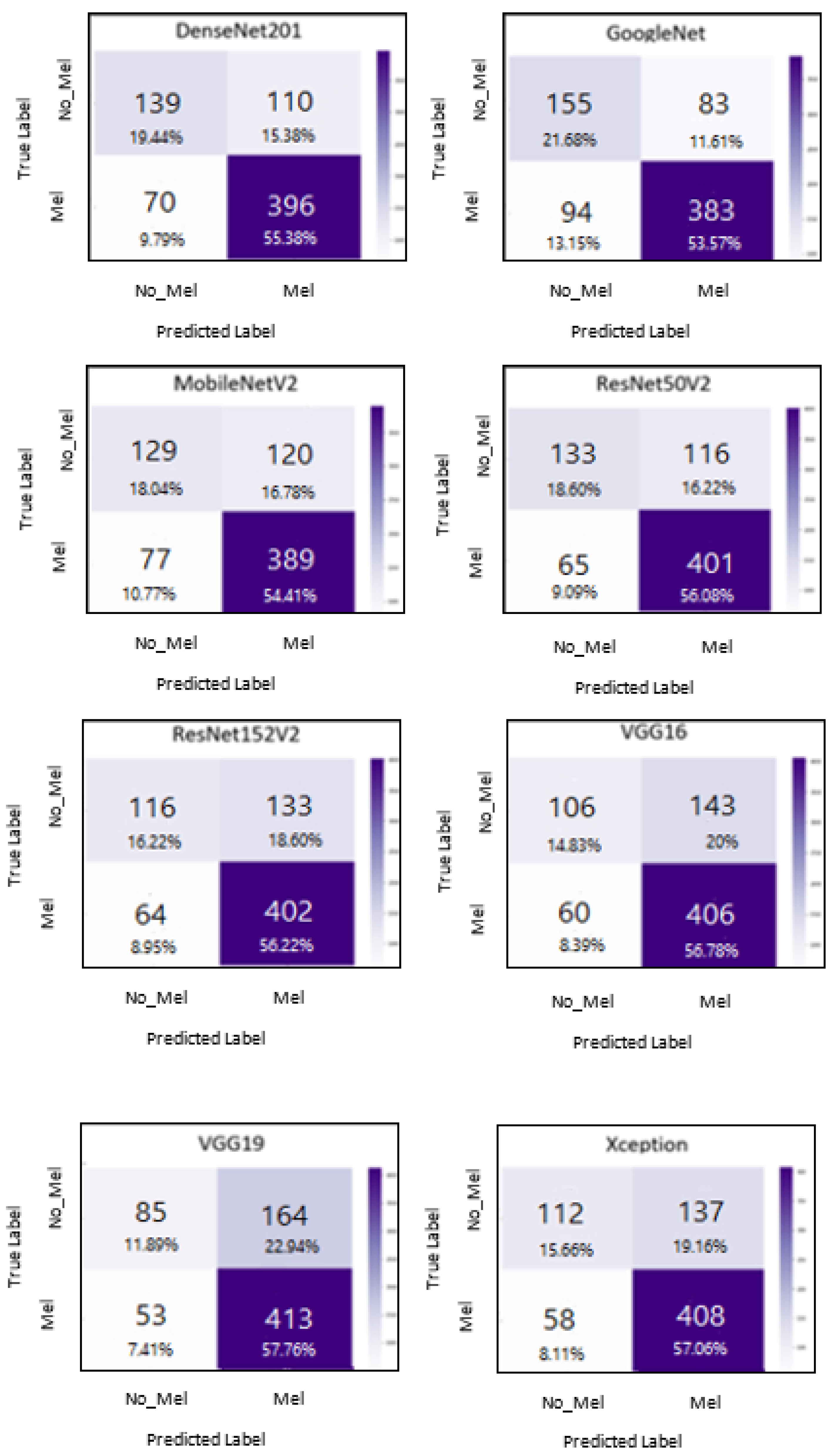
- Although large networks such as DenseNet201 and ResNet152V2 have notably more deep layers than GoogleNet and the other ones, experimental results demonstrate that GoogleNet generated the best performance results when measured using the standard performance measures. These results show the superiority of GoogleNet when tackling the melanoma skin cancer classification task.
2. Materials and Methods
2.1. Dataset
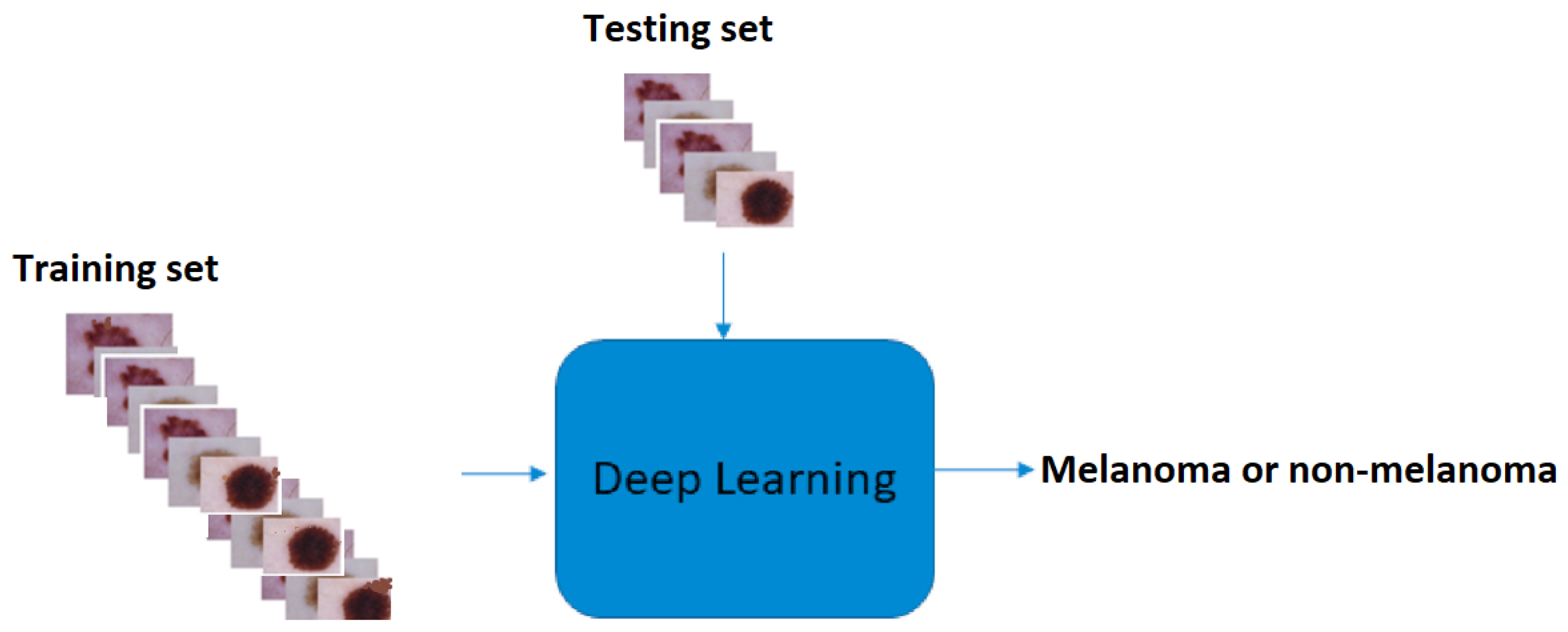
2.2. Deep Learning Approach
3. Results
3.1. Classification Methodology
3.2. Implementation Details
3.3. Classification Results
4. Discussion
5. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Argenziano, G.; Longo, C.; Cameron, A.; Cavicchini, S.; Gourhant, J.Y.; Lallas, A.; McColl, I.; Rosendahl, C.; Thomas, L.; Tiodorovic-Zivkovic, D.; et al. Blue-black rule: A simple dermoscopic clue to recognize pigmented nodular melanoma. Br. J. Dermatol. 2011, 165, 1251–1255. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, M.; Macaskill, P.; Holt, P.; Menzies, S. Dermoscopy compared with naked eye examination for the diagnosis of primary melanoma: A meta-analysis of studies performed in a clinical setting. Br. J. Dermatol. 2008, 159, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Charoenpong, J.; Pimpunchat, B.; Amornsamankul, S.; Triampo, W.; Nuttavut, N. A Comparison of Machine Learning Algorithms and their Applications. Int. J. Simul.–Syst. Sci. Technol. 2019, 20, 1–17. [Google Scholar]
- Rezayi, S.; Mohammadzadeh, N.; Bouraghi, H.; Saeedi, S.; Mohammadpour, A. Timely Diagnosis of Acute Lymphoblastic Leukemia Using Artificial Intelligence-Oriented Deep Learning Methods. Comput. Intell. Neurosci. 2021, 2021, 5478157. [Google Scholar] [CrossRef]
- Tufail, A.B.; Ma, Y.K.; Kaabar, M.K.; Martínez, F.; Junejo, A.; Ullah, I.; Khan, R. Deep learning in cancer diagnosis and prognosis prediction: A minireview on challenges, recent trends, and future directions. Comput. Math. Methods Med. 2021, 2021, 9025470. [Google Scholar] [CrossRef]
- Li, X.; Jiao, H.; Wang, Y. Edge detection algorithm of cancer image based on deep learning. Bioengineered 2020, 11, 693–707. [Google Scholar] [CrossRef]
- Gheisari, M.; Wang, G.; Bhuiyan, M.Z.A. A survey on deep learning in big data. In Proceedings of the 2017 IEEE International Conference on Computational Science and Engineering (CSE) and IEEE International Conference on Embedded and Ubiquitous Computing (EUC), Guangzhou, China, 21–24 July 2017; Volume 2, pp. 173–180. [Google Scholar]
- Banka, A.A.; Mir, R.N. Current Big Data Issues and Their Solutions via Deep Learning: An Overview. Iraqi J. Electr. Electron. Eng. 2018, 14, 127–138. [Google Scholar] [CrossRef]
- Alzubaidi, L.; Zhang, J.; Humaidi, A.J.; Al-Dujaili, A.; Duan, Y.; Al-Shamma, O.; Santamaría, J.; Fadhel, M.A.; Al-Amidie, M.; Farhan, L. Review of deep learning: Concepts, CNN architectures, challenges, applications, future directions. J. Big Data 2021, 8, 1–74. [Google Scholar] [CrossRef]
- Chen, X.; Weng, J.; Lu, W.; Xu, J.; Weng, J. Deep manifold learning combined with convolutional neural networks for action recognition. IEEE Trans. Neural Netw. Learn. Syst. 2017, 29, 3938–3952. [Google Scholar] [CrossRef]
- Ghods, A.; Cook, D.J. A survey of deep network techniques all classifiers can adopt. Data Min. Knowl. Discov. 2021, 35, 46–87. [Google Scholar] [CrossRef]
- Liu, W.; Wang, Z.; Liu, X.; Zeng, N.; Liu, Y.; Alsaadi, F.E. A survey of deep neural network architectures and their applications. Neurocomputing 2017, 234, 11–26. [Google Scholar] [CrossRef]
- Yamashita, R.; Nishio, M.; Do, R.K.G.; Togashi, K. Convolutional neural networks: An overview and application in radiology. Insights Imaging 2018, 9, 611–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, A.; Sohail, A.; Zahoora, U.; Qureshi, A.S. A survey of the recent architectures of deep convolutional neural networks. Artif. Intell. Rev. 2020, 53, 5455–5516. [Google Scholar] [CrossRef] [Green Version]
- Dong, Y.N.; Liang, G.S. Research and discussion on image recognition and classification algorithm based on deep learning. In Proceedings of the 2019 International Conference on Machine Learning, Big Data and Business Intelligence (MLBDBI), Taiyuan, China, 8–10 November 2019; pp. 274–278. [Google Scholar]
- Sharma, O. Deep challenges associated with deep learning. In Proceedings of the 2019 International Conference on Machine Learning, Big Data, Cloud and Parallel Computing (COMITCon), Faridabad, India, 14–16 February 2019; pp. 72–75. [Google Scholar]
- Rajput, D.S.; Reddy, T.S.K.; Raju, D.N. Investigation on Deep Learning Approach for Big Data: Applications and Challenges. In Deep Learning and Neural Networks: Concepts, Methodologies, Tools, and Applications; IGI Global: Hershey, PA, USA, 2020; pp. 1016–1029. [Google Scholar]
- Jan, B.; Farman, H.; Khan, M.; Imran, M.; Islam, I.U.; Ahmad, A.; Ali, S.; Jeon, G. Deep learning in big data analytics: A comparative study. Comput. Electr. Eng. 2019, 75, 275–287. [Google Scholar] [CrossRef]
- Zhang, Q.; Yang, L.T.; Chen, Z.; Li, P. A survey on deep learning for big data. Inf. Fusion 2018, 42, 146–157. [Google Scholar] [CrossRef]
- Qian, Y. Exploration of machine algorithms based on deep learning model and feature extraction. Math. Biosci. Eng. 2021, 18, 7602–7618. [Google Scholar] [CrossRef]
- Pouyanfar, S.; Sadiq, S.; Yan, Y.; Tian, H.; Tao, Y.; Reyes, M.P.; Shyu, M.L.; Chen, S.C.; Iyengar, S.S. A survey on deep learning: Algorithms, techniques, and applications. ACM Comput. Surv. (CSUR) 2018, 51, 1–36. [Google Scholar] [CrossRef]
- Cullell-Dalmau, M.; Otero-Viñas, M.; Manzo, C. Research techniques made simple: Deep learning for the classification of dermatological images. J. Investig. Dermatol. 2020, 140, 507–514. [Google Scholar] [CrossRef] [Green Version]
- Schadendorf, D.; van Akkooi, A.C.; Berking, C.; Griewank, K.G.; Gutzmer, R.; Hauschild, A.; Stang, A.; Roesch, A.; Ugurel, S. Melanoma. Lancet 2018, 392, 971–984. [Google Scholar] [CrossRef]
- Chassagnon, G.; Vakalopolou, M.; Paragios, N.; Revel, M.P. Deep learning: Definition and perspectives for thoracic imaging. Eur. Radiol. 2020, 30, 2021–2030. [Google Scholar] [CrossRef]
- Hekler, A.; Utikal, J.S.; Enk, A.H.; Berking, C.; Klode, J.; Schadendorf, D.; Jansen, P.; Franklin, C.; Holland-Letz, T.; Krahl, D.; et al. Pathologist-level classification of histopathological melanoma images with deep neural networks. Eur. J. Cancer 2019, 115, 79–83. [Google Scholar] [CrossRef] [Green Version]
- Acosta, M.F.J.; Tovar, L.Y.C.; Garcia-Zapirain, M.B.; Percybrooks, W.S. Melanoma diagnosis using deep learning techniques on dermatoscopic images. BMC Med. Imaging 2021, 21, 6. [Google Scholar] [CrossRef] [PubMed]
- Brinker, T.J.; Hekler, A.; Enk, A.H.; Berking, C.; Haferkamp, S.; Hauschild, A.; Weichenthal, M.; Klode, J.; Schadendorf, D.; Holland-Letz, T.; et al. Deep neural networks are superior to dermatologists in melanoma image classification. Eur. J. Cancer 2019, 119, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bisla, D.; Choromanska, A.; Berman, R.S.; Stein, J.A.; Polsky, D. Towards automated melanoma detection with deep learning: Data purification and augmentation. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition Workshops, Long Beach, CA, USA, 16–20 June 2019. [Google Scholar]
- Abbas, Q.; Celebi, M.E. DermoDeep-A classification of melanoma-nevus skin lesions using multi-feature fusion of visual features and deep neural network. Multimed. Tools Appl. 2019, 78, 23559–23580. [Google Scholar] [CrossRef]
- Tognetti, L.; Bonechi, S.; Andreini, P.; Bianchini, M.; Scarselli, F.; Cevenini, G.; Moscarella, E.; Farnetani, F.; Longo, C.; Lallas, A.; et al. A new deep learning approach integrated with clinical data for the dermoscopic differentiation of early melanomas from atypical nevi. J. Dermatol. Sci. 2020, 101, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Pennig, L.; Shahzad, R.; Caldeira, L.; Lennartz, S.; Thiele, F.; Goertz, L.; Zopfs, D.; Meißner, A.K.; Fürtjes, G.; Perkuhn, M.; et al. Automated Detection and Segmentation of Brain Metastases in Malignant Melanoma: Evaluation of a Dedicated Deep Learning Model. Am. J. Neuroradiol. 2021, 42, 655–662. [Google Scholar] [CrossRef]
- Zhou, Q.; Shi, Y.; Xu, Z.; Qu, R.; Xu, G. Classifying melanoma skin lesions using convolutional spiking neural networks with unsupervised stdp learning rule. IEEE Access 2020, 8, 101309–101319. [Google Scholar] [CrossRef]
- Pollastri, F.; Bolelli, F.; Paredes, R.; Grana, C. Augmenting data with GANs to segment melanoma skin lesions. Multimed. Tools Appl. 2020, 79, 15575–15592. [Google Scholar] [CrossRef] [Green Version]
- Winkler, J.K.; Fink, C.; Toberer, F.; Enk, A.; Deinlein, T.; Hofmann-Wellenhof, R.; Thomas, L.; Lallas, A.; Blum, A.; Stolz, W.; et al. Association between surgical skin markings in dermoscopic images and diagnostic performance of a deep learning convolutional neural network for melanoma recognition. JAMA Dermatol. 2019, 155, 1135–1141. [Google Scholar] [CrossRef]
- Almaraz-Damian, J.A.; Ponomaryov, V.; Sadovnychiy, S.; Castillejos-Fernandez, H. Melanoma and nevus skin lesion classification using handcraft and deep learning feature fusion via mutual information measures. Entropy 2020, 22, 484. [Google Scholar] [CrossRef] [Green Version]
- Combalia, M.; Codella, N.C.; Rotemberg, V.; Helba, B.; Vilaplana, V.; Reiter, O.; Carrera, C.; Barreiro, A.; Halpern, A.C.; Puig, S.; et al. BCN20000: Dermoscopic lesions in the wild. arXiv 2019, arXiv:1908.02288. [Google Scholar]
- Tschandl, P.; Rosendahl, C.; Kittler, H. The HAM10000 dataset, a large collection of multi-source dermatoscopic images of common pigmented skin lesions. Sci. Data 2018, 5, 180161. [Google Scholar] [CrossRef] [PubMed]
- Codella, N.C.; Gutman, D.; Celebi, M.E.; Helba, B.; Marchetti, M.A.; Dusza, S.W.; Kalloo, A.; Liopyris, K.; Mishra, N.; Kittler, H.; et al. Skin lesion analysis toward melanoma detection: A challenge at the 2017 international symposium on biomedical imaging (isbi), hosted by the international skin imaging collaboration (isic). In Proceedings of the 2018 IEEE 15th international symposium on biomedical imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018; pp. 168–172. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Ragab, D.A.; Attallah, O.; Sharkas, M.; Ren, J.; Marshall, S. A framework for breast cancer classification using multi-DCNNs. Comput. Biol. Med. 2021, 131, 104245. [Google Scholar] [CrossRef]
- Chollet, F. Xception: Deep learning with depthwise separable convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1251–1258. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Identity mappings in deep residual networks. In Computer Vision—ECCV 2016, Proceedings of the European Conference on Computer Vision, Amsterdam, The Netherlands, 11–14 October 2016; Springer: Cham, Switzerland, 2016; pp. 630–645. [Google Scholar]
- Howard, A.G.; Zhu, M.; Chen, B.; Kalenichenko, D.; Wang, W.; Weyand, T.; Andreetto, M.; Adam, H. Mobilenets: Efficient convolutional neural networks for mobile vision applications. arXiv 2017, arXiv:1704.04861. [Google Scholar]
- Najafabadi, M.M.; Villanustre, F.; Khoshgoftaar, T.M.; Seliya, N.; Wald, R.; Muharemagic, E. Deep learning applications and challenges in big data analytics. J. Big Data 2015, 2, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Christin, S.; Hervet, É.; Lecomte, N. Applications for deep learning in ecology. Methods Ecol. Evol. 2019, 10, 1632–1644. [Google Scholar] [CrossRef]
- Angermueller, C.; Pärnamaa, T.; Parts, L.; Stegle, O. Deep learning for computational biology. Mol. Syst. Biol. 2016, 12, 878. [Google Scholar] [CrossRef]
- Szegedy, C.; Zaremba, W.; Sutskever, I.; Bruna, J.; Erhan, D.; Goodfellow, I.; Fergus, R. Intriguing properties of neural networks. arXiv 2013, arXiv:1312.6199. [Google Scholar]
- Khan, S.; Muhammad, K.; Mumtaz, S.; Baik, S.W.; de Albuquerque, V.H.C. Energy-efficient deep CNN for smoke detection in foggy IoT environment. IEEE Internet Things J. 2019, 6, 9237–9245. [Google Scholar] [CrossRef]
- Turki, T.; Wei, Z. Improved Deep Convolutional Neural Networks via Boosting for Predicting the Quality of In Vitro Bovine Embryos. Electronics 2022, 11, 1363. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors and Year | Datasets | Architecture | Images | Results |
|---|---|---|---|---|
| Hekler et al., 2019 [25] | The largest regional dermatohistopathological institute in Germany | ResNet50 | 350 nevi and 345 melanomas | Misclassification rates of the trained CNN were 0.18 for melanomas 95%, 0.20 for nevi 95%, and 0.19 for the full set of images 95% |
| Jojoa et al., 2021 [26] | ISIC 2017 challenge | ResNet152 | Training: 1995, validation: 149 | eVida M6 model accuracy = 90.4%, sensitivity = 82%, specificity = 0.925 |
| Brinker et al., 2019 [27] | ISIC | ResNet50 | Training: 1888 mel, 10,490 nevi; validation: 210 mel, 1049 nevi; test: 20 mel, 80 nevi | sensitivity = 84.5%, chief physician’s sensitivity: 73.3% |
| Bisla et al., 2019 [28] | ISIC 2017–2018, PH2, Edinburgh | U-Net, ResNet50 | ISIC 2017 (803,2107,288); PH2 (40,80,0); Edinburgh (76,331,257); Testing: ISIC 2017–2018 (147,470,182) (mel, nevus, and seborrheic keratosis, respectively) | The accuracy was 81.6%, while two dermatologists had accuracies of 65.56% and 66.0% |
| Jose et al., 2020 [35] | ISIC 2018 | VGG-16, VGG-19, MobileNet, ResNet50, Xception, DenseNet201 | HAM10000 10,015 (actinic keratosis, basal cell carcinoma, dermatofibroma, mel, nevus, pigmented benign keratosis, vascular) | accuracy of 92.4%, IBA of 0.80, and MCC of 0.7953 |
| Architecture | Training Accuracy | Test Accuracy | Training Loss | Test Loss |
|---|---|---|---|---|
| DenseNet201 | 0.7396 | 0.7468 | 0.5167 | 0.5174 |
| MobileNetV2 | 0.7188 | 0.7398 | 0.5371 | 0.5325 |
| ResNet50V2 | 0.7374 | 0.7342 | 0.5187 | 0.5090 |
| ResNet152V2 | 0.7039 | 0.7384 | 0.5950 | 0.5601 |
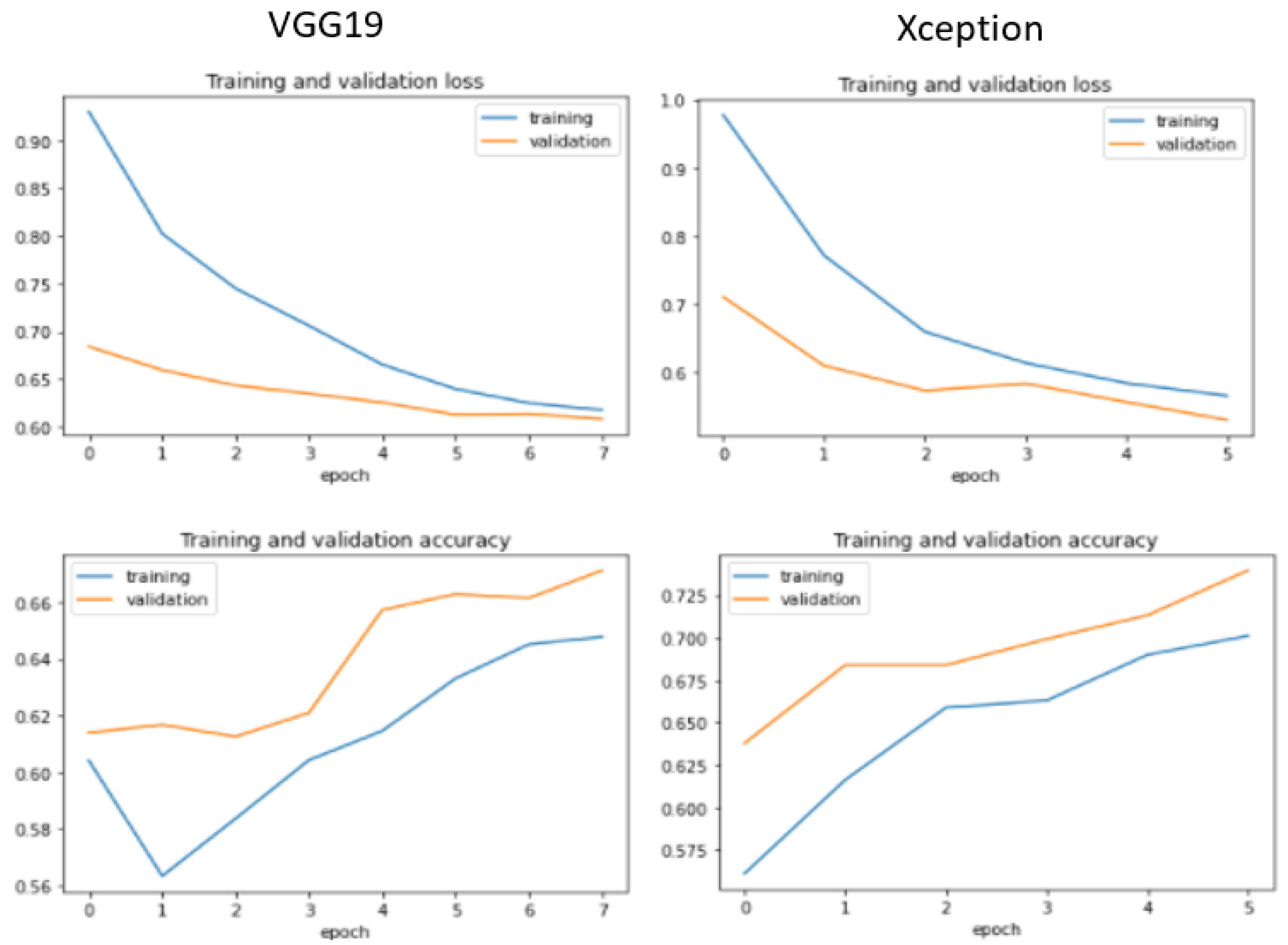
| Xception | 0.708 | 0.7062 | 0.5555 | 0.5419 |
| VGG16 | 0.6436 | 0.7146 | 0.6325 | 0.5547 |
| VGG19 | 0.6550 | 0.6867 | 0.6095 | 0.5793 |
| GoogleNet | 0.7491 | 0.7608 | 0.4991 | 0.5015 |
| Architecture | TN | FN | TP | FP | Total | TN&TP | FN&FP |
|---|---|---|---|---|---|---|---|
| DenseNet201 | 139 | 70 | 396 | 110 | 715 | 535 | 180 |
| MobileNetV2 | 129 | 77 | 389 | 120 | 715 | 518 | 197 |
| ResNet50V2 | 133 | 65 | 401 | 116 | 715 | 534 | 181 |
| ResNet152V2 | 116 | 64 | 402 | 133 | 715 | 518 | 197 |
| Xception | 112 | 58 | 408 | 137 | 715 | 520 | 195 |
| VGG16 | 106 | 60 | 406 | 143 | 715 | 512 | 203 |
| VGG19 | 85 | 53 | 413 | 164 | 715 | 498 | 217 |
| GoogleNet | 155 | 94 | 383 | 83 | 715 | 538 | 177 |
| Architecture | Balanced Accuracy | F1-score | Precision | Recall |
|---|---|---|---|---|
| DenseNet201 | 0.70 | 0.81 | 0.78 | 0.85 |
| MobileNetV2 | 0.68 | 0.80 | 0.76 | 0.83 |
| ResNet50V2 | 0.70 | 0.82 | 0.78 | 0.86 |
| ResNet152V2 | 0.66 | 0.80 | 0.75 | 0.86 |
| Xception | 0.66 | 0.81 | 0.75 | 0.88 |
| VGG16 | 0.65 | 0.80 | 0.74 | 0.87 |
| VGG19 | 0.61 | 0.79 | 0.72 | 0.89 |
| GoogleNet | 0.73 | 0.81 | 0.82 | 0.80 |
| Architecture | Best Epoch |
|---|---|
| DenseNet201 | 16 |
| MobileNetV2 | 14 |
| ResNet50V2 | 19 |
| ResNet152V2 | 9 |
| Xception | 6 |
| VGG16 | 5 |
| VGG19 | 8 |
| GoogleNet | 29 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aljohani, K.; Turki, T. Automatic Classification of Melanoma Skin Cancer with Deep Convolutional Neural Networks. AI 2022, 3, 512-525. https://doi.org/10.3390/ai3020029
Aljohani K, Turki T. Automatic Classification of Melanoma Skin Cancer with Deep Convolutional Neural Networks. AI. 2022; 3(2):512-525. https://doi.org/10.3390/ai3020029
Chicago/Turabian StyleAljohani, Khalil, and Turki Turki. 2022. "Automatic Classification of Melanoma Skin Cancer with Deep Convolutional Neural Networks" AI 3, no. 2: 512-525. https://doi.org/10.3390/ai3020029
APA StyleAljohani, K., & Turki, T. (2022). Automatic Classification of Melanoma Skin Cancer with Deep Convolutional Neural Networks. AI, 3(2), 512-525. https://doi.org/10.3390/ai3020029