

Effect of Different Dental Implant Prosthetic Joints on Marginal Bone Loss: Emerging Findings from a Bayesian Network Meta-Analysis (NMA) and Systematic Review

 ,
, 
 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
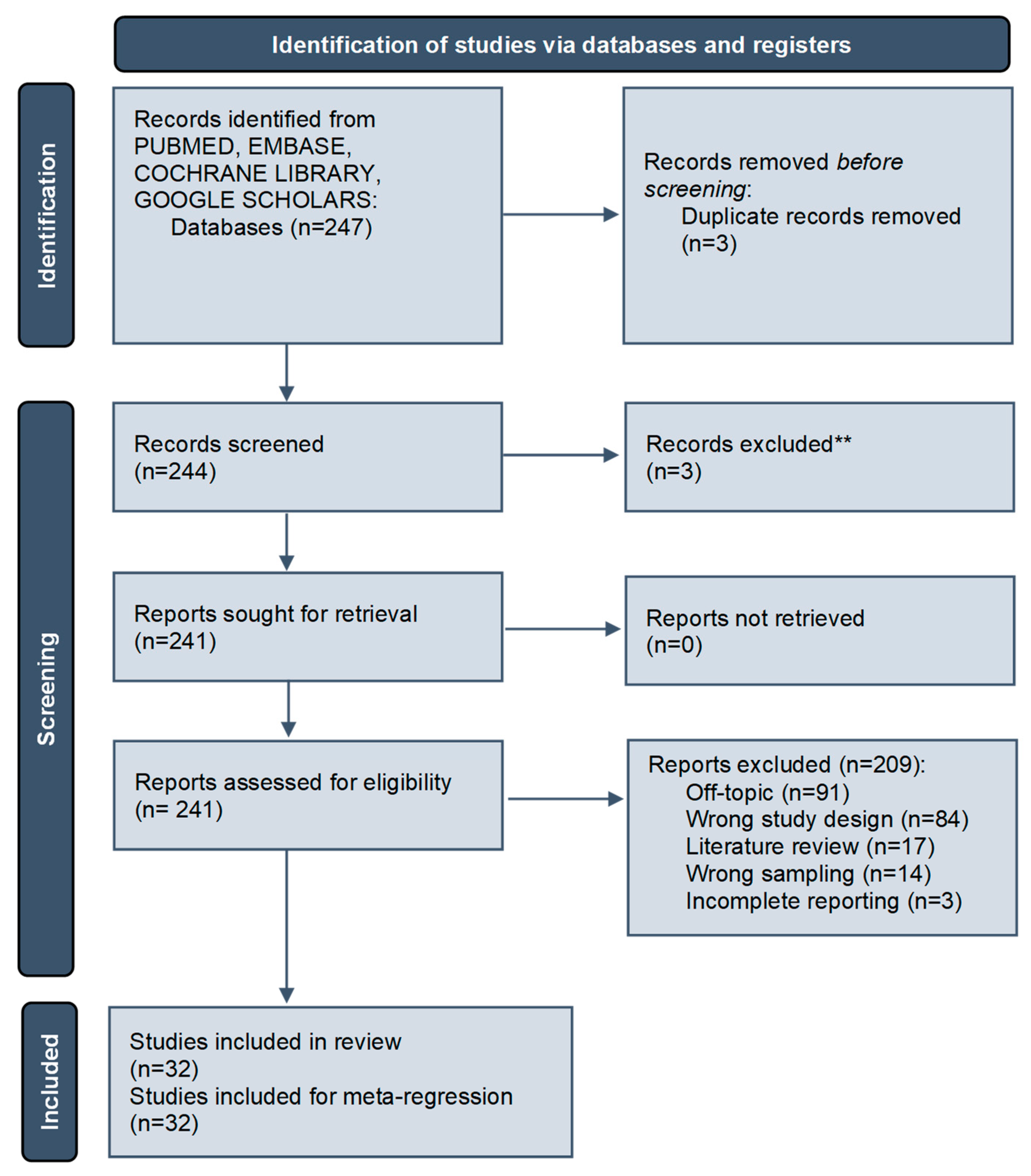
2.1. Search Strategy
- (1)
- P = Population/Patient/Problem—Subjects needing dental implant for prosthetic rehabilitations;
- (2)
- I = Intervention—dental implant treatment positioning and fixed oral rehabilitation;
- (3)
- C = Comparison—comparison between different internal, external and conical prosthetic joint;
- (4)
- O = Outcome—Marginal bone loss, major prosthetic complications.
2.2. Inclusion Criteria
2.3. Study Data Extraction
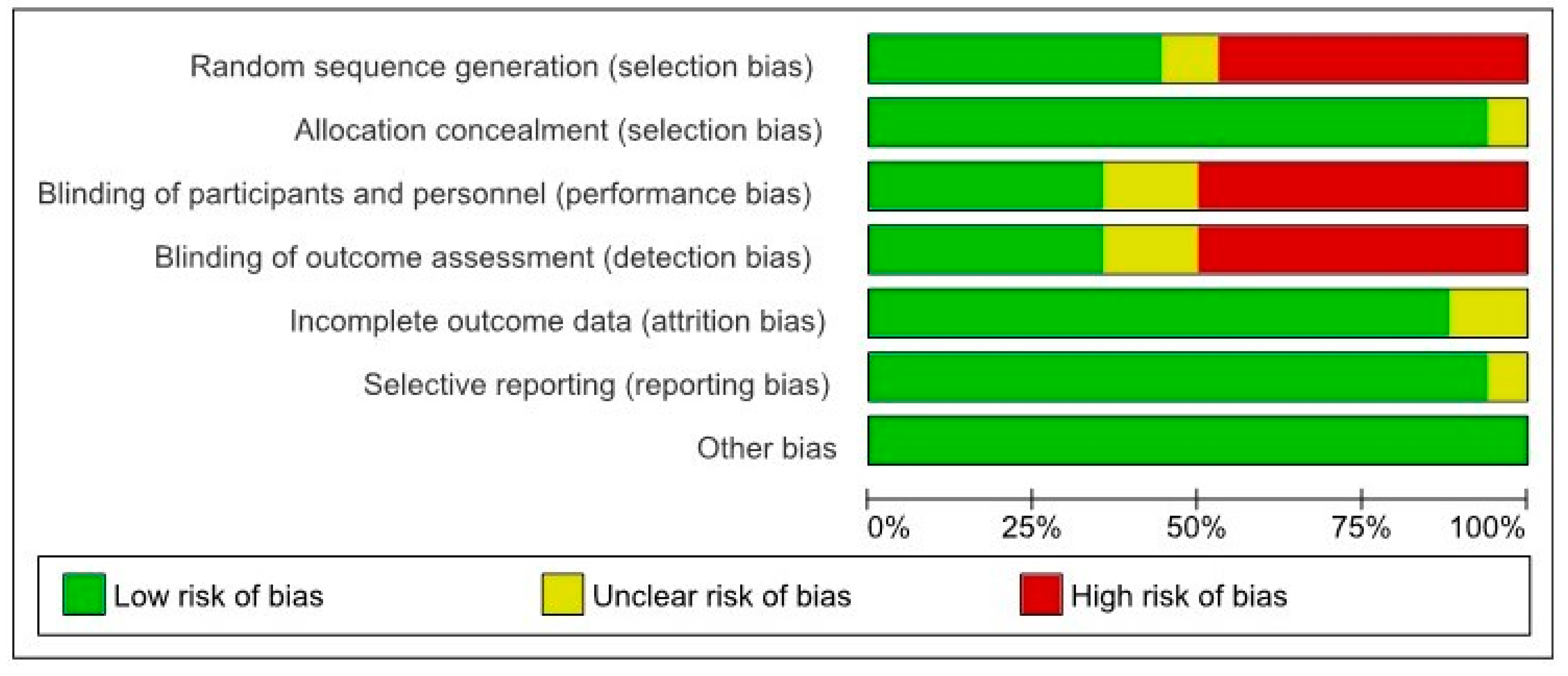
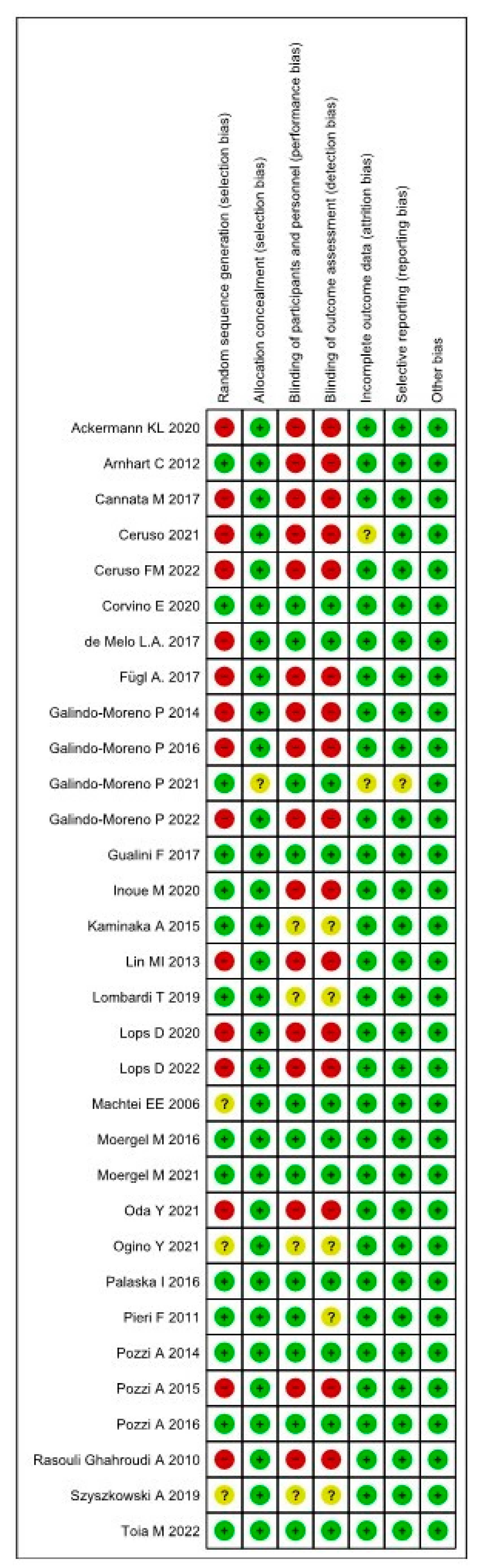
2.4. Risk of Bias (RoB)
2.5. Heterogeneity and Meta-Analysis Assessment
2.6. Inconsistency Assessment
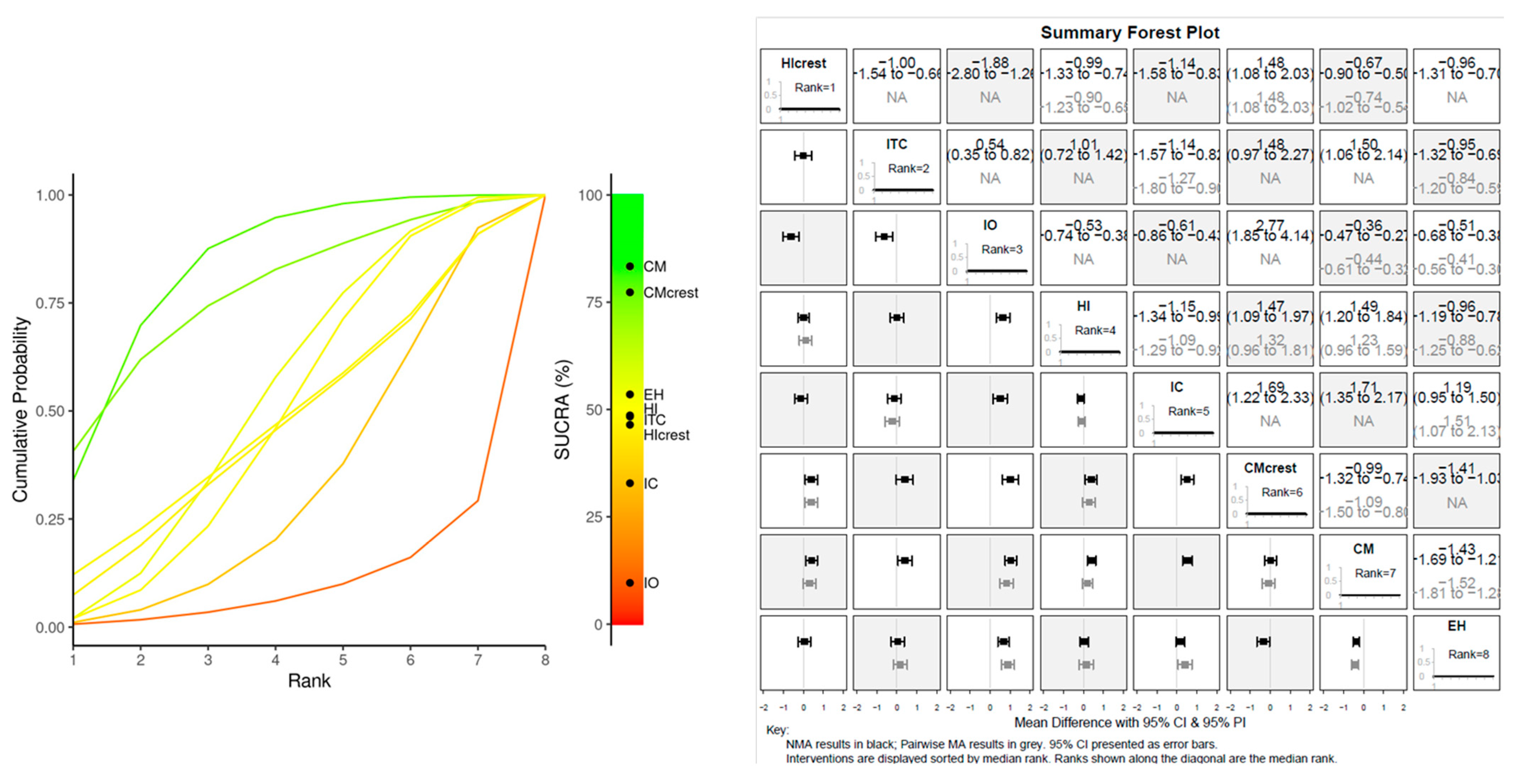
2.7. Study Data Analysis
3. Results
3.1. General Parameters
3.2. Prosthetic Complications and Joint Failure
3.3. Risk of Bias Assessment
3.4. Meta-Regression MBL
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hamada, Y.; Shin, D.; John, V. Peri-Implant Disease--A Significant Complication of Dental Implant Supported Restorative Treatment. J. Indiana Dent. Assoc. 2016, 95, 31–38. [Google Scholar]
- Koutouzis, T. Implant-abutment Connection as Contributing Factor to Peri-implant Diseases. Periodontology 2000 2019, 81, 152–166. [Google Scholar] [CrossRef] [PubMed]
- Bernardes, S.R.; da Gloria Chiarello de Mattos, M.; Hobkirk, J.; Ribeiro, R.F. Loss of Preload in Screwed Implant Joints as a Function of Time and Tightening/Untightening Sequences. Int. J. Oral Maxillofac. Implant. 2014, 29, 89–96. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, J. Influences of Microgap and Micromotion of Implant–Abutment Interface on Marginal Bone Loss around Implant Neck. Arch. Oral Biol. 2017, 83, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.R. The Long-Term Efficacy of Currently Used Dental Implants: A Review and Proposed Criteria of Success. Int. J. Oral Maxillofac. Implant. 1986, 1, 11–25. [Google Scholar]
- Romeo, E.; Ghisolfi, M.; Murgolo, N.; Chiapasco, M.; Lops, D.; Vogel, G. Therapy of Peri-Implantitis with Resective Surgery: A 3-Year Clinical Trial on Rough Screw-Shaped Oral Implants. Part I: Clinical Outcome. Clin. Oral Implant. Res. 2004, 16, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-H.; Kim, H.J.; Kim, S.; Koo, K.-T.; Kim, T.-I.; Seol, Y.-J.; Lee, Y.-M.; Ku, Y.; Rhyu, I.-C. Comparison of Marginal Bone Loss between Internal- and External-Connection Dental Implants in Posterior Areas without Periodontal or Peri-Implant Disease. J. Periodontal Implant. Sci. 2018, 48, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Ellakany, P.; Mahrous, A.; Eraky, D.; Albarrak, A.; AlJindan, R.; Fouda, S. Evaluation of Bacterial Leakage in Platform-Switching Dental Implant with Morse Taper Connection Under Thermocycling and Loading Effects: In Vitro Study. Int. J. Oral Maxillofac. Implant. 2021, 36, 68–74. [Google Scholar] [CrossRef]
- Assenza, B.; Tripodi, D.; Scarano, A.; Perrotti, V.; Piattelli, A.; Iezzi, G.; D’Ercole, S. Bacterial Leakage in Implants with Different Implant-Abutment Connections: An in Vitro Study. J. Periodontol. 2012, 83, 491–497. [Google Scholar] [CrossRef]
- Fernandes, P.F.; Grenho, L.; Fernandes, M.H.; Sampaio-Fernandes, J.C.; Gomes, P.S. Microgap and Bacterial Microleakage during the Osseointegration Period: An in Vitro Assessment of the Cover Screw and Healing Abutment in a Platform-Switched Implant System. J. Prosthet. Dent. 2021, 130, 87–95. [Google Scholar] [CrossRef]
- Larrucea, C.; Conrado, A.; Olivares, D.; Padilla, C.; Barrera, A.; Lobos, O. Bacterial Microleakage at the Abutment-Implant Interface, in Vitro Study. Clin. Implant Dent. Relat. Res. 2018, 20, 360–367. [Google Scholar] [CrossRef]
- Sahin, C.; Ayyildiz, S. Correlation between Microleakage and Screw Loosening at Implant-Abutment Connection. J. Adv. Prosthodont. 2014, 6, 35. [Google Scholar] [CrossRef]
- Norton, M.R. An in Vitro Evaluation of the Strength of an Internal Conical Interface Compared to a Butt Joint Interface in Implant Design. Clin. Oral Implant. Res. 1997, 8, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-Analyses of Health Care Interventions: Checklist and Explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Owen, R.K.; Bradbury, N.; Xin, Y.; Cooper, N.; Sutton, A. MetaInsight: An Interactive Web-Based Tool for Analyzing, Interrogating, and Visualizing Network Meta-Analyses Using R-Shiny and Netmeta. Res. Synth. Methods 2019, 10, 569–581. [Google Scholar] [CrossRef]
- Nikolakopoulou, A.; Higgins, J.P.T.; Papakonstantinou, T.; Chaimani, A.; Del Giovane, C.; Egger, M.; Salanti, G. CINeMA: An Approach for Assessing Confidence in the Results of a Network Meta-Analysis. PLoS Med. 2020, 17, e1003082. [Google Scholar] [CrossRef]
- Papakonstantinou, T.; Nikolakopoulou, A.; Higgins, J.P.T.; Egger, M.; Salanti, G. CINeMA: Software for Semiautomated Assessment of the Confidence in the Results of Network Meta-Analysis. Campbell Syst. Rev. 2020, 16, e1080. [Google Scholar] [CrossRef]
- Ceruso, F.M.; Ieria, I.; Tallarico, M.; Meloni, S.M.; Lumbau, A.I.; Mastroianni, A.; Zotti, A.; Gargari, M. Comparison between Early Loaded Single Implants with Internal Conical Connection or Implants with Transmucosal Neck Design: A Non-Randomized Controlled Trial with 1-Year Clinical, Aesthetics, and Radiographic Evaluation. Materials 2022, 15, 511. [Google Scholar] [CrossRef]
- Ceruso, F.M.; Ieria, I.; Martelli, M.; Lumbau, A.I.; Xhanari, E.; Gargari, M. New Generation of Fixture–Abutment Connection Combining Soft Tissue Design and Vertical Screw-Retained Restoration: 1-Year Clinical, Aesthetics and Radiographic Preliminary Evaluation. Dent. J. 2021, 9, 35. [Google Scholar] [CrossRef]
- Inoue, M.; Nakano, T.; Shimomoto, T.; Kabata, D.; Shintani, A.; Yatani, H. Multivariate Analysis of the Influence of Prosthodontic Factors on Peri-Implant Bleeding Index and Marginal Bone Level in a Molar Site: A Cross-Sectional Study. Clin. Implant Dent. Relat. Res. 2020, 22, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Corvino, E.; Pesce, P.; Camodeca, F.; Moses, O.; Iannello, G.; Canullo, L. Clinical and Radiological Outcomes of Implants with Two Different Connection Configurations: A Randomised Controlled Trial. Int. J. Oral Implantol. 2020, 13, 355–368. [Google Scholar]
- Kaminaka, A.; Nakano, T.; Ono, S.; Kato, T.; Yatani, H. Cone-Beam Computed Tomography Evaluation of Horizontal and Vertical Dimensional Changes in Buccal Peri-Implant Alveolar Bone and Soft Tissue: A 1-Year Prospective Clinical Study. Clin. Implant Dent. Relat. Res. 2015, 17, e576–e585. [Google Scholar] [CrossRef] [PubMed]
- Pieri, F.; Aldini, N.N.; Marchetti, C.; Corinaldesi, G. Influence of Implant-Abutment Interface Design on Bone and Soft Tissue Levels around Immediately Placed and Restored Single-Tooth Implants: A Randomized Controlled Clinical Trial. Int. J. Oral Maxillofac. Implant. 2011, 26, 169–178. [Google Scholar]
- Oda, Y.; Mori, G.; Honma, S.; Ito, T.; Iijima, T.; Yajima, Y. Marginal Bone Loss and the Risk Indicators of Fixed Screw-Retained Implant-Supported Prostheses and Fixed Telescopic-Retained Implant-Supported Prostheses in Full Arch: A Retrospective Case-Control Study. Clin. Oral Implant. Res. 2021, 32, 818–827. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.-I.; Shen, Y.-W.; Huang, H.-L.; Hsu, J.-T.; Fuh, L.-J. A Retrospective Study of Implant–Abutment Connections on Crestal Bone Level. J. Dent. Res. 2013, 92, 202S–207S. [Google Scholar] [CrossRef] [PubMed]
- Cannata, M.; Grandi, T.; Samarani, R.; Svezia, L.; Grandi, G. A Comparison of Two Implants with Conical vs Internal Hex Connections: 1-Year Post-Loading Results from a Multicentre, Randomised Controlled Trial. Eur. J. Oral Implantol. 2017, 10, 161–168. [Google Scholar]
- Arnhart, C.; Kielbassa, A.M.; Martinez-de Fuentes, R.; Goldstein, M.; Jackowski, J.; Lorenzoni, M.; Maiorana, C.; Mericske-Stern, R.; Pozzi, A.; Rompen, E.; et al. Comparison of Variable-Thread Tapered Implant Designs to a Standard Tapered Implant Design after Immediate Loading. A 3-Year Multicentre Randomised Controlled Trial. Eur. J. Oral Implantol. 2012, 5, 123–136. [Google Scholar]
- Melo, L.A.; Souza, M.B.C.; Barbosa, G.A.S.; Carreiro, A.D.F.P. Peri-Implant Bone Loss of External Hexagon and Morse Taper in Patients Wearing Immediately Loaded Overdentures. Braz. Dent. J. 2017, 28, 694–698. [Google Scholar] [CrossRef]
- Machtei, E.E.; Oved-Peleg, E.; Peled, M. Comparison of Clinical, Radiographic and Immunological Parameters of Teeth and Different Dental Implant Platforms. Clin. Oral Implant. Res. 2006, 17, 658–665. [Google Scholar] [CrossRef]
- Pozzi, A.; Agliardi, E.; Tallarico, M.; Barlattani, A. Clinical and Radiological Outcomes of Two Implants with Different Prosthetic Interfaces and Neck Configurations: Randomized, Controlled, Split-Mouth Clinical Trial. Clin. Implant Dent. Relat. Res. 2014, 16, 96–106. [Google Scholar] [CrossRef]
- Lops, D.; Stocchero, M.; Motta Jones, J.; Freni, A.; Palazzolo, A.; Romeo, E. Five Degree Internal Conical Connection and Marginal Bone Stability around Subcrestal Implants: A Retrospective Analysis. Materials 2020, 13, 3123. [Google Scholar] [CrossRef]
- Galindo-Moreno, P.; León-Cano, A.; Ortega-Oller, I.; Monje, A.; Suárez, F.; ÓValle, F.; Spinato, S.; Catena, A. Prosthetic Abutment Height Is a Key Factor in Peri-Implant Marginal Bone Loss. J. Dent. Res. 2014, 93, 80S–85S. [Google Scholar] [CrossRef]
- Szyszkowski, A.; Kozakiewicz, M. Effect of Implant-Abutment Connection Type on Bone Around Dental Implants in Long-Term Observation: Internal Cone Versus Internal Hex. Implant Dent. 2019, 28, 430–436. [Google Scholar] [CrossRef]
- Galindo-Moreno, P.; Ravidà, A.; Catena, A.; O’Valle, F.; Padial-Molina, M.; Wang, H.L. Limited Marginal Bone Loss in Implant-Supported Fixed Full-Arch Rehabilitations after 5 Years of Follow-Up. Clin. Oral Implant. Res. 2022, 33, 1224–1232. [Google Scholar] [CrossRef] [PubMed]
- Moergel, M.; Rocha, S.; Messias, A.; Nicolau, P.; Guerra, F.; Wagner, W. Clinical and Radiographic Performance of Self-Locking Conical Connection Implants in the Posterior Mandible: Five-Year Results of a Two-Centre Prospective Study. Clin. Oral Implant. Res. 2021, 32, 998–1007. [Google Scholar] [CrossRef]
- Moergel, M.; Rocha, S.; Messias, A.; Nicolau, P.; Guerra, F.; Wagner, W. Radiographic Evaluation of Conical Tapered Platform-Switched Implants in the Posterior Mandible: 1-Year Results of a Two-Center Prospective Study. Clin. Oral Implant. Res. 2016, 27, 686–693. [Google Scholar] [CrossRef] [PubMed]
- Galindo-Moreno, P.; Concha-Jeronimo, A.; Lopez-Chaichio, L.; Rodriguez-Alvarez, R.; Sanchez-Fernandez, E.; Padial-Molina, M. Marginal Bone Loss around Implants with Internal Hexagonal and Internal Conical Connections: A 12-Month Randomized Pilot Study. J. Clin. Med. 2021, 10, 5427. [Google Scholar] [CrossRef]
- Toia, M.; Stocchero, M.; Galli, S.; Papia, E.; Wennerberg, A.; Becktor, J.P. The Use of Implant-Level Connection in Screw-Retained Fixed Partial Dentures: A 3-Year Randomised Clinical Trial. Clin. Oral Implant. Res. 2022, 33, 78–93. [Google Scholar] [CrossRef]
- Pozzi, A.; Tallarico, M.; Moy, P.K. Immediate Loading with a Novel Implant Featured by Variable-Threaded Geometry, Internal Conical Connection and Platform Shifting: Three-Year Results from a Prospective Cohort Study. Eur. J. Oral Implantol. 2015, 8, 51–63. [Google Scholar] [PubMed]
- Lombardi, T.; Berton, F.; Salgarello, S.; Barbalonga, E.; Rapani, A.; Piovesana, F.; Gregorio, C.; Barbati, G.; Di Lenarda, R.; Stacchi, C. Factors Influencing Early Marginal Bone Loss around Dental Implants Positioned Subcrestally: A Multicenter Prospective Clinical Study. J. Clin. Med. 2019, 8, 1168. [Google Scholar] [CrossRef] [PubMed]
- Gualini, F.; Salina, S.; Rigotti, F.; Mazzarini, C.; Longhin, D.; Grigoletto, M.; Trullenque-Eriksson, A.; Sbricoli, L.; Esposito, M. Subcrestal Placement of Dental Implants with an Internal Conical Connection of 0.5 Mm versus 1.5 Mm: Outcome of a Multicentre Randomised Controlled Trial 1 Year after Loading. Eur. J. Oral Implantol. 2017, 10, 73–82. [Google Scholar] [PubMed]
- Pozzi, A.; Mura, P. Immediate Loading of Conical Connection Implants: Up-to-2-Year Retrospective Clinical and Radiologic Study. Int. J. Oral Maxillofac. Implant. 2016, 31, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Lops, D.; Romeo, E.; Stocchero, M.; Palazzolo, A.; Manfredi, B.; Sbricoli, L. Marginal Bone Maintenance and Different Prosthetic Emergence Angles: A 3-Year Retrospective Study. J. Clin. Med. 2022, 11, 2014. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, K.L.; Barth, T.; Cacaci, C.; Kistler, S.; Schlee, M.; Stiller, M. Clinical and Patient-Reported Outcome of Implant Restorations with Internal Conical Connection in Daily Dental Practices: Prospective Observational Multicenter Trial with up to 7-Year Follow-Up. Int. J. Implant. Dent. 2020, 6, 14. [Google Scholar] [CrossRef]
- Fügl, A.; Zechner, W.; Pozzi, A.; Heydecke, G.; Mirzakhanian, C.; Behneke, N.; Behneke, A.; Baer, R.A.; Nölken, R.; Gottesman, E.; et al. An Open Prospective Single Cohort Multicenter Study Evaluating the Novel, Tapered, Conical Connection Implants Supporting Single Crowns in the Anterior and Premolar Maxilla: Interim 1-Year Results. Clin. Oral Investig. 2017, 21, 2133–2142. [Google Scholar] [CrossRef][Green Version]
- Galindo-Moreno, P.; León-Cano, A.; Monje, A.; Ortega-Oller, I.; O’Valle, F.; Catena, A. Abutment Height Influences the Effect of Platform Switching on Peri-Implant Marginal Bone Loss. Clin. Oral Implant. Res. 2016, 27, 167–173. [Google Scholar] [CrossRef]
- Ogino, Y.; Matsushita, Y.; Sasaki, M.; Ayukawa, Y.; Koyano, K. A 3-Year Prospective Study on Radiographic Marginal Bone Evaluation Around Platform-Shifting Implants with Internal Conical Connections. Int. J. Oral Maxillofac. Implant. 2021, 36, 574–580. [Google Scholar] [CrossRef]
- Palaska, I.; Tsaousoglou, P.; Vouros, I.; Konstantinidis, A.; Menexes, G. Influence of Placement Depth and Abutment Connection Pattern on Bone Remodeling around 1-Stage Implants: A Prospective Randomized Controlled Clinical Trial. Clin. Oral Implant. Res. 2016, 27, e47–e56. [Google Scholar] [CrossRef] [PubMed]
- Romanos, G.E.; Biltucci, M.T.; Kokaras, A.; Paster, B.J. Bacterial Composition at the Implant-Abutment Connection under Loading in Vivo: Bacteria at Implant-Abutment Interface under in Vivo Loading Conditions. Clin. Implant. Dent. Relat. Res. 2016, 18, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Camps-Font, O.; Rubianes-Porta, L.; Valmaseda-Castellón, E.; Jung, R.E.; Gay-Escoda, C.; Figueiredo, R. Comparison of External, Internal Flat-to-Flat, and Conical Implant Abutment Connections for Implant-Supported Prostheses: A Systematic Review and Network Meta-Analysis of Randomized Clinical Trials. J. Prosthet. Dent. 2021, 130, 327–340. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Perrotti, V.; Piattelli, A.; Iaculli, F.; Iezzi, G. Sealing Capability of Implant-Abutment Junction under Cyclic Loading: A Toluidine Blue in Vitro Study. J. Appl. Biomater. Funct. Mater. 2015, 13, e293–e295. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Mortellaro, C.; Mavriqi, L.; Pecci, R.; Valbonetti, L. Evaluation of Microgap With Three-Dimensional X-Ray Microtomography: Internal Hexagon Versus Cone Morse. J. Craniofacial Surg. 2016, 27, 682–685. [Google Scholar] [CrossRef] [PubMed]
- Naser Mostofy, S.; Jalalian, E.; Valaie, N.; Mohtashamrad, Z.; Haeri, A.; Bitaraf, T. Study of the Effect of GapSeal on Microgap and Microleakage in Internal Hex Connection After Cyclic Loading. J. Res. Dentomaxillofac. Sci. 2019, 4, 36–42. [Google Scholar] [CrossRef]
- Orsini, G.; Fanali, S.; Scarano, A.; Petrone, G.; di Silvestro, S.; Piattelli, A. Tissue Reactions, Fluids, and Bacterial Infiltration in Implants Retrieved at Autopsy: A Case Report. Int. J. Oral Maxillofac. Implant. 2000, 15, 283–286. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search Strategies | |
|---|---|
| Keywords search: | (dental implant* OR dental prosth* OR implant-supported prosth* OR endosseous implant*) AND (conical OR tapper OR tapered OR fractional OR locking)) and (internal connection OR internal hexagon OR non conical OR non tapered OR internal tri-channel OR butt-joint)) AND (survival OR success OR bone loss OR bone level OR complications) |
| Timespan | No limitations (1995–2023) |
| Electronic Databases | Pubmed/Medline, EMBASE, Google scholars |
| Author | Journal | Year | Population | Implant | Connection |
|---|---|---|---|---|---|
| Arnhart C | Eur J Oral Implantol. | 2012 | 177 patients | 325 implants | Internal Conical Prosthetic Joint W/Index External Hexagon Internal Tri-Channel Connection |
| Ackermann KL | Int J Implant Dent | 2020 | 94 patients | 130 implants | Internal Conical Connection W/Index |
| Cannata M | Eur J Oral Implantol | 2017 | 90 patients | 90 implants | Internal Hexagon Internal Conical Prosthetic Joint W/Index |
| Ceruso FM | Materials | 2022 | 30 patients | 30 Implants | Internal Hexagon Internal Conical Prosthetic Joint W/Index |
| Ceruso FM | Dent J (Basel) | 2021 | 13 patients | 13 implants | Internal Hexagon Connection |
| Corvino E | Int J Oral Implantol (Berl) | 2020 | 33 patients | 53 implants | Internal Hexagon Internal Conical Prosthetic Joint W/Index |
| de Melo L.A. | Braz Dent J | 2017 | 20 patients | 40 implants | External Hexagon Cone Morse |
| Fügl A. | Clin Oral Invest | 2017 | 97 patients | 102 implants | Internal Conical Connection W/Index |
| Galindo-Moreno P | Clin Oral Implants Res | 2022 | 19 patients | 160 implants | Internal Conical Prosthetic Joint W/Index |
| Galindo-Moreno P | J Clin Med | 2021 | 30 patients | 30 implants | Internal Conical Prosthetic Joint W/Index |
| Galindo-Moreno P | Clin Oral Implants Res | 2016 | 108 patients | 228 implants | Cone Morse |
| Galindo-Moreno P | J Dent Res | 2014 | 131 patients | 315 implants | Internal Conical Prosthetic Joint W/Index |
| Gualini F. | Eur J Oral Implantol | 2017 | 60 patients | 120 implants | Internal Conical Connection W/Index |
| Inoue M | Clin Implant Dent Relat Res | 2020 | 140 patients | 310 implants | Internal Hexagon Internal Conical Prosthetic Joint W/Index |
| Kaminaka A | Clin Implant Dent Relat Res | 2015 | 33 patients | 34 implants | Internal Hexagon External Hexagon Cone Morse |
| Lin MI | J Dent Res | 2013 | 63 patients | 103 implants | External Hexagon Internal Octagon Cone Morse |
| Lombardi T. | J. Clin. Med. | 2019 | 55 patients | 83 implants | Internal Conical Connection W/Index |
| Lops D | J Clin Med | 2022 | 80 patients | 312 implants | Internal Conical Prosthetic Joint W/Index |
| Lops D | Materials | 2020 | 93 patients | 410 implants | Internal Conical Prosthetic Joint W/Index |
| Machtei EE | Clin Oral Implants Res | 2006 | 27 patients | 73 implants | External Hexagon Cone Morse |
| Moergel M | Clin Oral Implants Res | 2021 | 24 patients | 52 implants. | Internal Conical Connection W/Index |
| Moergel M | Clin Oral Implants Res | 2016 | 24 patients | 52 implants | Internal Conical Connection W/Index |
| Oda Y | Clin Oral Implants Res | 2021 | 60 patients | 592 implants | Internal Hexagon External Hexagon Cone Morse |
| Ogino Y | Int J Oral Maxillofac Implants | 2021 | 25 patients | 30 implants | Cone Morse |
| Palaska I | Clin Oral Implants Res | 2016 | 81 patients | 105 implants | Internal Polygonal Butt-Joint Cone Morse |
| Pieri F | Int J Oral Maxillofac Implants | 2011 | 40 patients | 40 implants | Internal Hexagon Cone Morse |
| Pozzi A | Int J Oral Maxillofac Implants | 2016 | 64 patients | 148 implants | Internal Conical Connection W/Index |
| Pozzi A | Eur J Oral Implantol | 2015 | 54 patients | 118 implants | Internal Conical Connection W/Index |
| Pozzi A | Clin Implant Dent Relat Res | 2014 | 34 patients | 68 implants | External Hexagon Internal Conical Prosthetic Joint W/Index |
| Rasouli Ghahroudi A | J Dent (Tehran) | 2010 | 31 patients | 170 implants | Internal Conical Prosthetic Joint W/Index |
| Szyszkowski A | Implant Dent | 2019 | 184 patients | 540 implants | Internal Conical Connection W/Index |
| Toia M | Clin Oral Implants Res | 2022 | 50 patients | 119 implants | Internal Conical Prosthetic Joint W/Index |
| Author | Journal | Year | Prosthetic Complications | Follow Up | Marginal Bone Loss | Outcomes |
|---|---|---|---|---|---|---|
| Arnhart C | Eur J Oral Implantol. | 2012 | prov. debonding (n = 9) prov. Abut. screw loose (n = 5) prov. framework fracture (n = 3) chipping veneering mat. (n = 7) restoration debonding (n = 2) screw loosening (n = 1) occlusal adjustments (n = 1) | 3 years | (a) baseline IC: −0.60 ± 0.83 mm; EH: −1.01 ± 1.02 mm; ITC: −0.84 ± 1.09 mm; (b) 1 year: IC: −1.48 ± 1.26 mm; EH: −1.66 ± 1.04 mm; ITC: −1.49 ± 0.96 mm; (c) 2 year: IC: −1.41 ± 1.54 mm; EH: −1.18 ± 0.91 mm; ITC: −1.71 ± 1.28 mm; | Stable or improving bone levels for all implant groups after the initial tissue remodelling. |
| Ackermann KL | Int J Implant Dent | 2020 | Crown loosening (3) Ceramic chipping (1) | 5 years | (a) baseline: −0.52 ± 0.55 mm (b) 1 year: −0.04 ± 0.37 mm (c) 2 years: −0.04 ± 0.40 mm (d) 5 yars: −0.09 ± 0.43 mm | High peri-implant tissue stability over the 5 to 7 years of follow up. |
| Cannata M | Eur J Oral Implantol | 2017 | Screw loosening (2) [HI group] | 1 year | (a) baseline: IC: 0.03 ± 0.06 mm; HI: 0.02 ± 0.05 mm (b) 1 year: IC:0.59 ± 0.61 mm; HI. 0.56 ± 0.53 mm | No significant differences concerning ICC and HI concerning marginal bone loss. |
| Ceruso FM | Materials | 2022 | None | 1 year | (a) Baseline: IC: 0.04 ± 0.06; HI: 0.01 ± 0.02 (b) 1 year: IC: 0.99 ± 0.71; HI: 0.65 ± 0.48 | Similar findings regarding marginal bone levels, implant survival, and periodontal parameter |
| Ceruso FM | Dent J (Basel) | 2021 | - | 1 year | (a) 1 year: 0.65 ± 0.48 mm | The IH implants showed no mechanical complications. |
| Corvino E | Int J Oral Implantol (Berl) | 2020 | - | 1 year | (a) baseline: CS: 0.33 ± 0.34 mm; HI: 0.43 ± 0.37 (b) 1 year: CS: 0.48 ± 0.18 mm; HI: 0.57 ± 0.24 mm | ICC seems to be correlated to lower level of MBL after the loading. |
| de Melo L.A. | Braz Dent J | 2017 | - | 1 year | (a) baseline: EH: −0.34 ± 1.90; CS: 0.12 ± 1.83 (b) 1 year: EH: −1.28 ± 1.68; CS: −0.73 ± 2.54 | Significantly higher marginal bone loss of HE compared to CM. Success rate in the groups EH of 100% and MT of 94.4%. |
| Fügl A. | Clin Oral Invest | 2017 | - | 1 year | (a) baseline: −0.37 ± 0.75 mm (b) 6 months: −1.35 ± 1.16 mm (c) 1 year: −1.25 ± 1.15 mm | Marginal bone levels followed the expected initial bone loss, and soft-tissue outcomes improved suggesting favorable tissue response. |
| Galindo-Moreno P | Clin Oral Implants Res | 2022 | 14 implants > 2 mm of MBL (8.75%) | 5 years | baseline: −0.423 ± 0.069 | Abutment height 1 mm more MBL than 2, 4 and 6 mm. Narrow implant more MBL then wider diameter implant |
| Galindo-Moreno P | J Clin Med | 2021 | Ceramic chipping (1) [HI] | 12 months | (a) 1 year: IC: −0.25 (0.12) HI: −0.70 (0.43) | HI implants produce higher MBL after 12 months of follow-up |
| Galindo-Moreno P | Clin Oral Implants Res | 2016 | - | 18 months | (a) baseline: −Implant diam. 4.5: Short abutment: 0.562 ± 0.09 mm Long abutment: 0.195 ± 0.05 mm −Implant diam.Short abutment: 5.0 mm: 0.557 ± 0.21 mm Long abutment: 0.549 ± 0.06 mm | Abutment height seems to affect MBL at the short/medium term period. |
| Galindo-Moreno P | J Dent Res | 2014 | - | 18 months | (a) baseline: SA: 0.210 ± 0.025 mm LA: 0.068 ± 0.015 (b) 1 year: SA: 0.681 ± 0.051 mm LA: 0.316 ± 0.042 | Higher MBL associated with short abutment height. butment height is a key factor in MBL. MBL is higher during the first 6 months post-loading. |
| Gualini F. | Eur J Oral Implantol | 2017 | Crown loosening (1) | 1 year | (a) baseline: 0.5 mm subcrestal: 0.07 ± 0.21 mm; 1.5 mm subcrestal: 0 04 ± 0.13 mm (b) 2 months: 0.5 mm subcrestal: 0.16 ± 0.30 mm; 1.5 mm subcrestal: 0 10 ± 0.38 mm (c) 1 year: 0.5 mm subcrestal: 0.21 ± 0.51 mm; 1.5 mm subcrestal: 0 11 ± 0.36 mm | No significant differences concerning implants positioned 0.5 mm or 1.5 mm subcrestally |
| Inoue M | Clin Implant Dent Relat Res | 2020 | - | 1 year | (a) baseline: 0.61 ± 0.43 mm | ICC showed lower MBR compared to internal connection. No significant difference in mBI and MBL comparing cement and screw crowns. |
| Kaminaka A | Clin Implant Dent Relat Res | 2015 | - | 1 year | (a) baseline: EH: −0.08 ± 0.33 mm; IH: 0.21 ± 0.32; CM:−0.04 ± 0.84 (a) 1 year: EH:−1.94 ± 0.87 mm; IH: −0.79 ± 1.30; CM: 0.25 ± 0.87 | Implants with a conical connection preserve peri-implant alveolar bone and soft tissue more effectively than other connection types. |
| Lin MI | J Dent Res | 2013 | - | 6 months | (a) baseline: EH: –0.45 ± 0.19 mm IO: 0.44 ± 0.15 mm; CM: –0.38 ± 0.14 mm (b) 3 months: EH: –0.21 ± 0.13 mm IO: –0.18 ± 0.12 mm; CM: –0.19 ± 0.11 mm (c) 6 months: EH: −0.32 ± 0.19 mm IO: –0.38 ± 0.22 mm; CM: –0.32 ± 0.14 mm | Implant–abutment connection appears to have no significant impact on short-term MBL. |
| Lombardi T. | J. Clin. Med. | 2019 | - | 1 year | (a) baseline: 0.46 ± 0.59 mm (b) 2 months: 0.5 ± 0.34 mm (c) 3 months: 0.18 ± 0.22 mm (d) 9 months: 0.11 ± 0.20 mm (e) 15 months: 0.00 ± 0.19 mm | Peri-implant bone levels seems to be stabilized over long-term loading. |
| Lops D | J Clin Med | 2022 | None | 3 years | Emergency angle > 30°: MBL: 0.25 ± 0.3 mm Emergency angle < 30°: MBL: 0.4 ± 0.3 mm | The emergency angle seems to play no significant effect on MBL at 3-year follow up |
| Lops D | Materials | 2020 | 9 years | (a) Baseline: −1.09 ± 0.65 mm (b) 9 years: −1.00 ± 0.37 mm | MBL are correlated to the implant’s vertical position and the of type-2 controlled diabetes comorbidity | |
| Machtei EE | Clin Oral Implants Res | 2006 | - | 2.9 years | (a) baseline: EH: 2.15 ± 0.67 mm; CM: 0.95 ± 0.21 mm | Similar clinical and MBL response. Non-submerged implants might suggest future higher bone resorption compared to submerged healing protocol. |
| Moergel M | Clin Oral Implants Res | 2021 | Screw fracture (1): | 5-year | (a) Baseline: −0.5, ± 0.4 mm (b) 60 months: 0.27 ± 0.47 mm | Conical abutment-joint connection was associated with a marginal bone levels maintainment after 5 years of loading |
| Moergel M | Clin Oral Implants Res | 2016 | Screw fracture (1) | 1 year | (a) Baseline:0.53 ± 0.40 mm; (b) 1 year: 0.12 ± 0.42 mm (c) 18 months: 0.11 ± 0.36 mm | No implant loss after 1 year of loading |
| Oda Y | Clin Oral Implants Res | 2021 | - | 13 years | (a) FSI: 0.60 ± 0.51; FTI: 0.41 ± 1.03 mm | FSI and FTI implants showed similar MBL. HI and HE showed higher MBL compared to Cone Morse abutment joint connection |
| Ogino Y | Int J Oral Maxillofac Implants | 2021 | - | 3 years | (a) Baseline: −0.41 ± 0.61 mm (b) 1 year: −0.08 ± 0.54 mm (c) 3 years: −0.04 ± 0.95 mm | ICC are able to prevent marginal bone loss after 3 years of follow up |
| Palaska I | Clin Oral Implants Res | 2016 | - | 3 months | (a) baseline: Group 1HI [subcrestal]: 0.68 ± 0.07 mm, Group 2 HI [crestal]: 0.79 ± 0.06 mm, Group 3 CM [subcrestal]: 0.49 ± 0.06 mm, Group 4CM [subcrestal]: 0.40 ± 0.07 mm. | The fixture/abutment joint rather than vertical implant placement in relation to marginal bone level seems to affect peri-implant marginal bone resorption |
| Pieri F | Int J Oral Maxillofac Implants | 2011 | - | 1 year | (a) baseline: HI: 0.51 ± 0.24 mm; CM: 0.2 ± 0.17 mm | Slight difference in MBL in favour of cone morse joint group. |
| Pozzi A | Int J Oral Maxillofac Implants | 2016 | - | 2 years | (a) baseline: 0.42 ± 1.16 mm 1 year: 0.71 ± 1.53 mm 2 years: 0.17 ± 1.01 mm | Immediately loaded implants revealed well-maintained MBL, and soft tissue conditions. |
| Pozzi A | Eur J Oral Implantol | 2015 | Crown failure (1) | 3 years | (a) baseline: 0.42 ± 0.29 mm (b) 1 year: 0.19 ± 0.21 mm (c) 2 years: 0.07 mm ± 0.13 mm | Prosthetic Cumulative Success Rate (CSR) of 98.15 for ICC. |
| Pozzi A | Clin Implant Dent Relat Res | 2014 | 1 year | (a) baseline: CM: 0.37 ± 0.23 mm EH: 0.95 ± 0.56 mm (b) 1 year: 0.14 ± 0.20 mm EH: 0.16 ± 0.19 mm | Lower MBL of back-tapered neck compared to external hexagon joint. | |
| Rasouli Ghahroudi A | J Dent (Tehran) | 2010 | - | 1 year | (a) baseline: 0.935 ± 0.905 mm | ICC seems to provide a useful maintenance of the peri-implant bone levels at 1 year follow-up. |
| Szyszkowski A | Implant Dent | 2019 | - | 2 years | (a) baseline: 0.99 ± 0.79 (b) 1 year: 1.12 ± 1.00 (c) 2 years: 1.22 ± 1.03 (d) 3 years: 1.30 ± 1.15 | ICC revealed lower MBL compared to internal hexagon joint connection. Both of implant groups revealed 100% survival rate. |
| Toia M | Clin Oral Implants Res | 2022 | (a) Screw loosening (2): [Abutment level Group (AL) (1)/Implant level Group (IG) (1)] (b) Screw fracture (2): [Abutment level Group (AL)] | 3 years | (a) Baseline: AL: 0.11 ± 0.24; IC: 0.15 ± 0.31 (b) 1 year: AL: 0.12 ± 0.31; IC: 0.23 ± 0.26 (c) 2 years: A(L: 0.15 ± 0.34; IC: 0.17 ± 0.22 (d) 3 years: AL: 0.18 ± 0.39; 0.15; IC: 0.21 | The MBL change was similar in the groups. No relevant complicaitons were detected in the soft tissue. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorusso, F.; Alla, I.; Gehrke, S.A.; Carmine, M.D.; Tari, S.R.; Scarano, A. Effect of Different Dental Implant Prosthetic Joints on Marginal Bone Loss: Emerging Findings from a Bayesian Network Meta-Analysis (NMA) and Systematic Review. Prosthesis 2024, 6, 186-205. https://doi.org/10.3390/prosthesis6010015
Lorusso F, Alla I, Gehrke SA, Carmine MD, Tari SR, Scarano A. Effect of Different Dental Implant Prosthetic Joints on Marginal Bone Loss: Emerging Findings from a Bayesian Network Meta-Analysis (NMA) and Systematic Review. Prosthesis. 2024; 6(1):186-205. https://doi.org/10.3390/prosthesis6010015
Chicago/Turabian StyleLorusso, Felice, Iris Alla, Sergio Alexandre Gehrke, Mariastella Di Carmine, Sergio Rexhep Tari, and Antonio Scarano. 2024. "Effect of Different Dental Implant Prosthetic Joints on Marginal Bone Loss: Emerging Findings from a Bayesian Network Meta-Analysis (NMA) and Systematic Review" Prosthesis 6, no. 1: 186-205. https://doi.org/10.3390/prosthesis6010015
APA StyleLorusso, F., Alla, I., Gehrke, S. A., Carmine, M. D., Tari, S. R., & Scarano, A. (2024). Effect of Different Dental Implant Prosthetic Joints on Marginal Bone Loss: Emerging Findings from a Bayesian Network Meta-Analysis (NMA) and Systematic Review. Prosthesis, 6(1), 186-205. https://doi.org/10.3390/prosthesis6010015