
Computer-Guided Osteotomy with Simultaneous Implant Placement and Immediately Loaded Full-Arch Fixed Restoration: A Case Report

 ,
,  ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
3. Discussion
- (a)
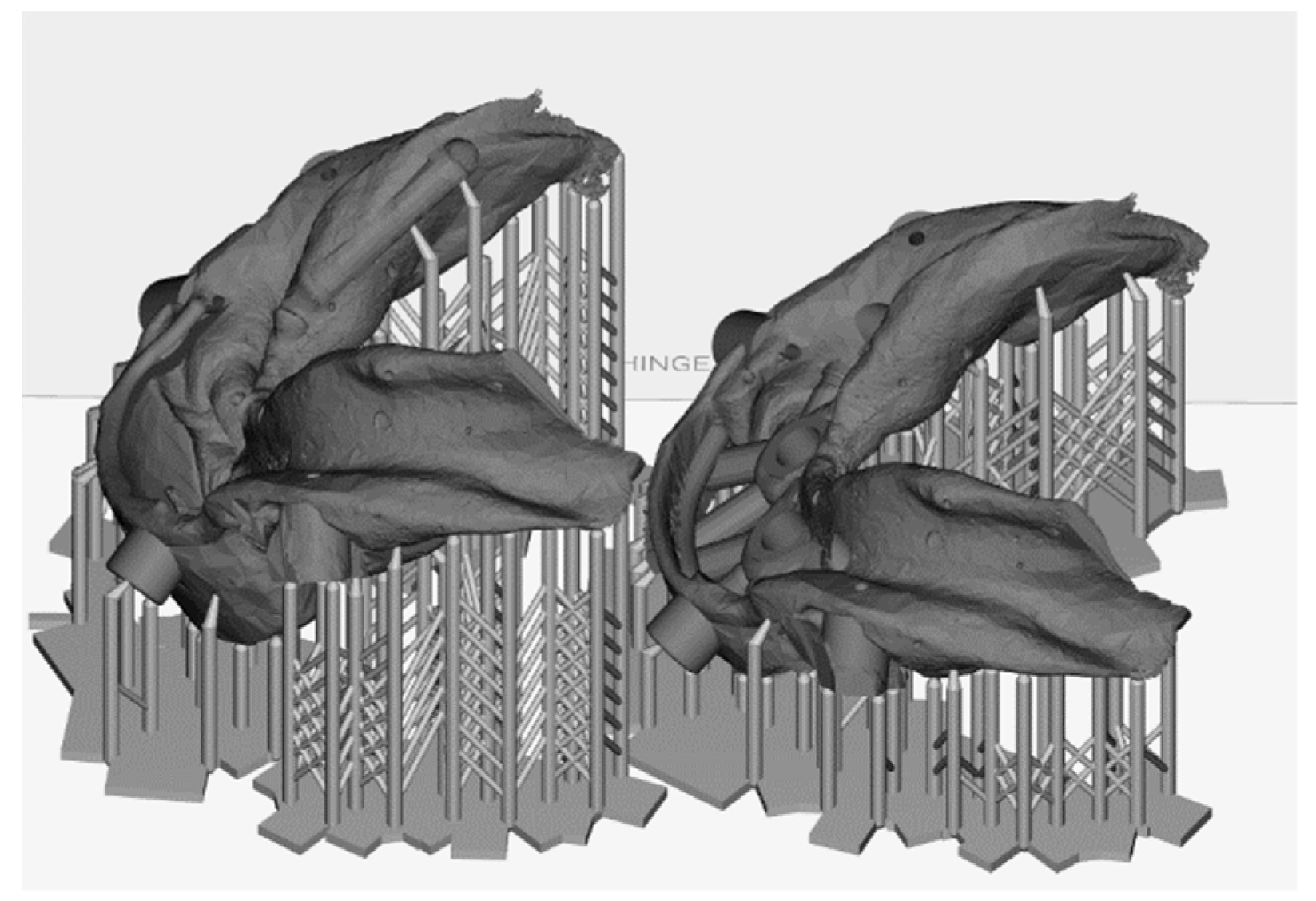
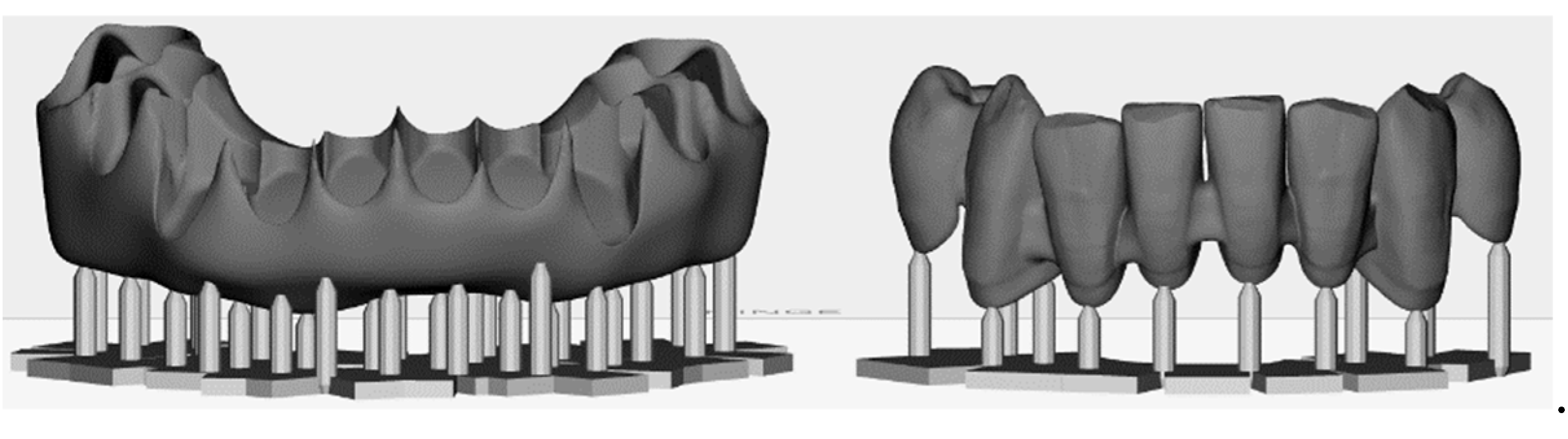
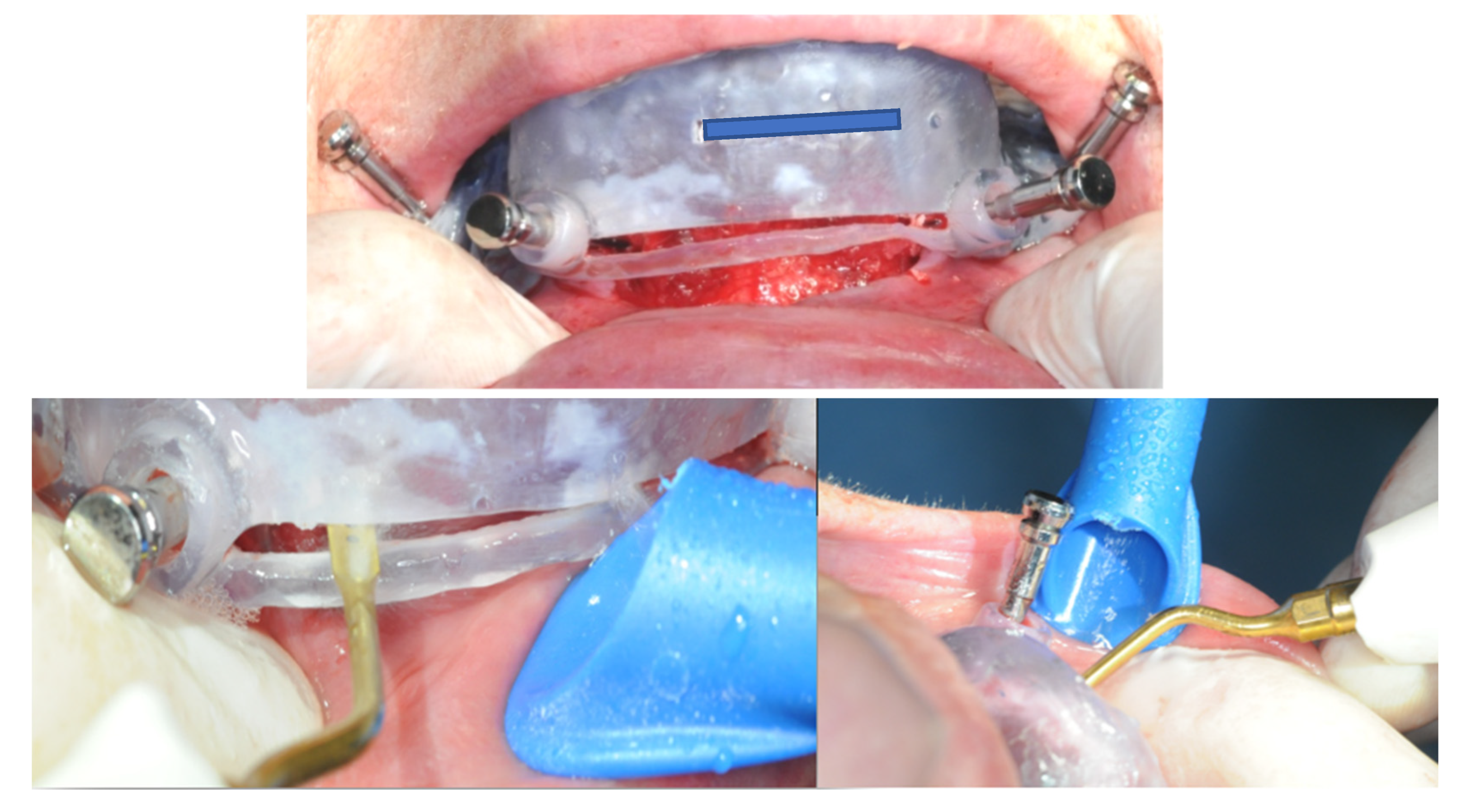
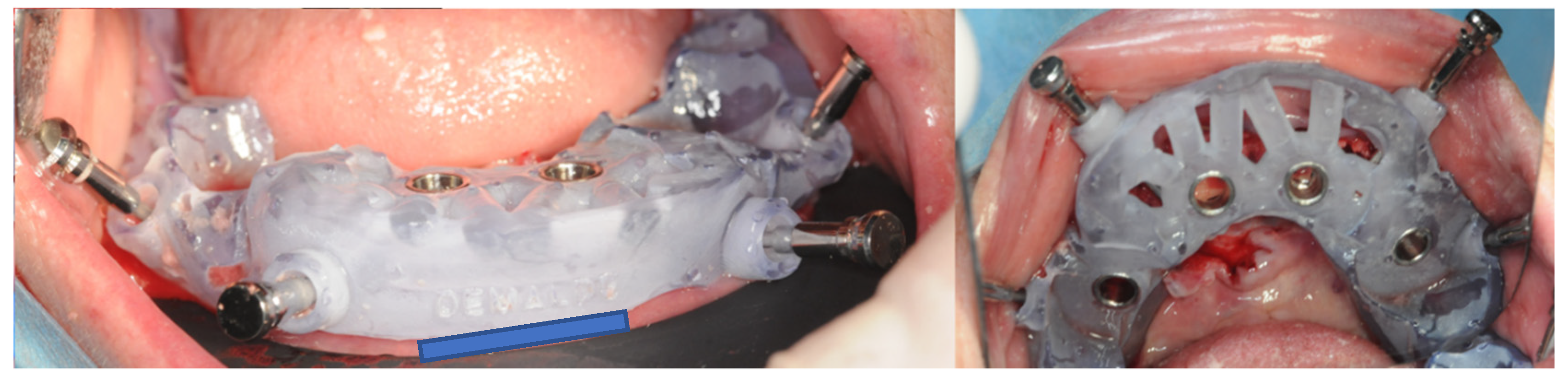
- Support of the osteotomy and surgical guide (valence of the dental support). The design of the osteotomy positioning template provided support for all the dental elements present in the arch, from element 3.3 to element 4.4. The operative choice to keep the support elements for the osteotomy’s cutting template is supported by the literature. Currently, scientific studies such as that of Kholy et al. conducted in 2019 [41] have shown that the support provided by four stable elements or an entire arch is comparable in terms of implant positioning deviation with respect to the plan itself [33,42,43]. On the other hand, the positioning of implants starting from a template that has fewer dental elements as support is less predictable. The operative and design choice of the case was directed towards the realization of a first osteotomy guide template with dental support. However, in our experience, the amount of dental support is not a significant variable when the template is designed and stabilized by means of stabilization pins specially placed on the buccal side [44,45]. Any positioning discrepancies that could occur in full-arch rehabilitations due to the lack of dental elements or the presence of some of them with high mobility are bypassed by the presence of stable stabilization pins or landmarks. In the first instance, the creation of a predetermined bone plane provided greater predictability for the subsequent implant’s positioning, despite the fact that, due to the clinical needs of the case, the implant surgical guide was exclusively supported in a bone-mucosal fashion. Greater stability, positioning effectiveness, and design adherence were achieved by using the same positioning pins as the osteotomy guide as a reference point.
- (b)
- Arrangement of the slit for osteotomy and the role of piezosurgery. The slit prepared in the osteotomy guide was designed on the basis of the thickness of the inserts used with the piezosurgery approach in order to reduce the risk of the inclination of the drill in the surgical preparation of the osteotomy plane. The piezo-surgical approach to osteotomy has been extensively studied and, subsequently, validated in the literature on orthognathic surgery; it is more conservative with respect to the surrounding tissues, causing less bleeding and less severe damage to nerve structures [36]. In addition, regarding oral surgery, the piezosurgical technique was advanced above all for maxillary sinus lift and the extraction of impacted wisdom teeth, thus confirming its lower risk of postoperative complications compared to the traditional method using rotating burs [46,47,48].
- (c)
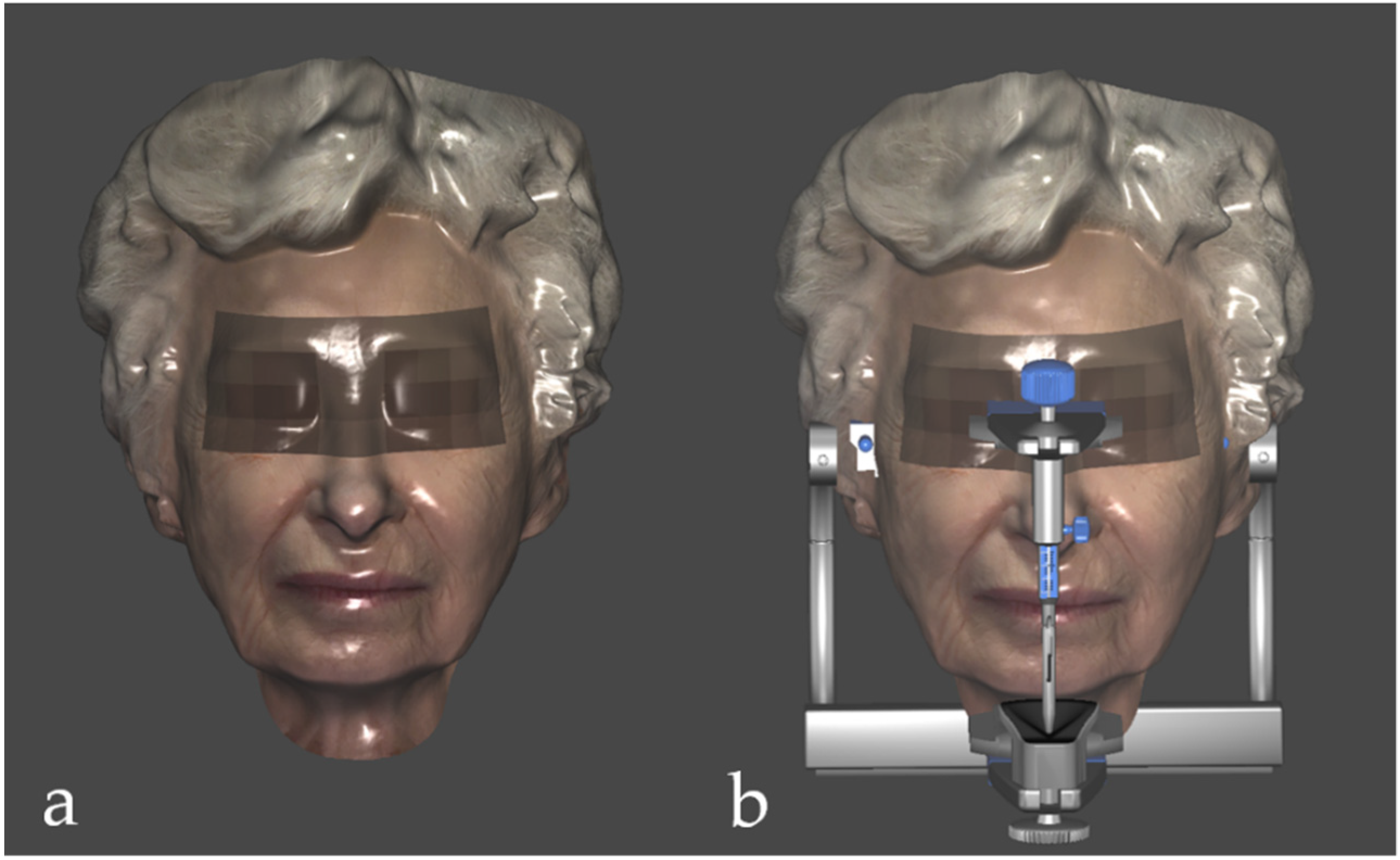
- Facial scanning as an additional tool. Facial scanning represents a recent and innovative method with significant advantages in terms of the investigation and clinical planning of complex cases [49]. From an aesthetic perspective, this technique allows the clinician to program the digital smile design in a three-dimensional way, with a greater and more precise number of landmarks available [50,51]. From a functional perspective, the face scan combined with the scan of the arches, the CBCT, and the virtual articulator allow for the evaluation of the gnathological aspects of complex rehabilitation [52], which will be the subject of future research. Furthermore, it is offered as a means of making doctor–patient communication more effective [53].
4. Materials and Methods
4.1. Selection of the Case
4.2. Data Acquisition
4.3. Diagnostic Wax-Up
4.4. Design and 3D Printing of the Templates
4.5. Prosthesis
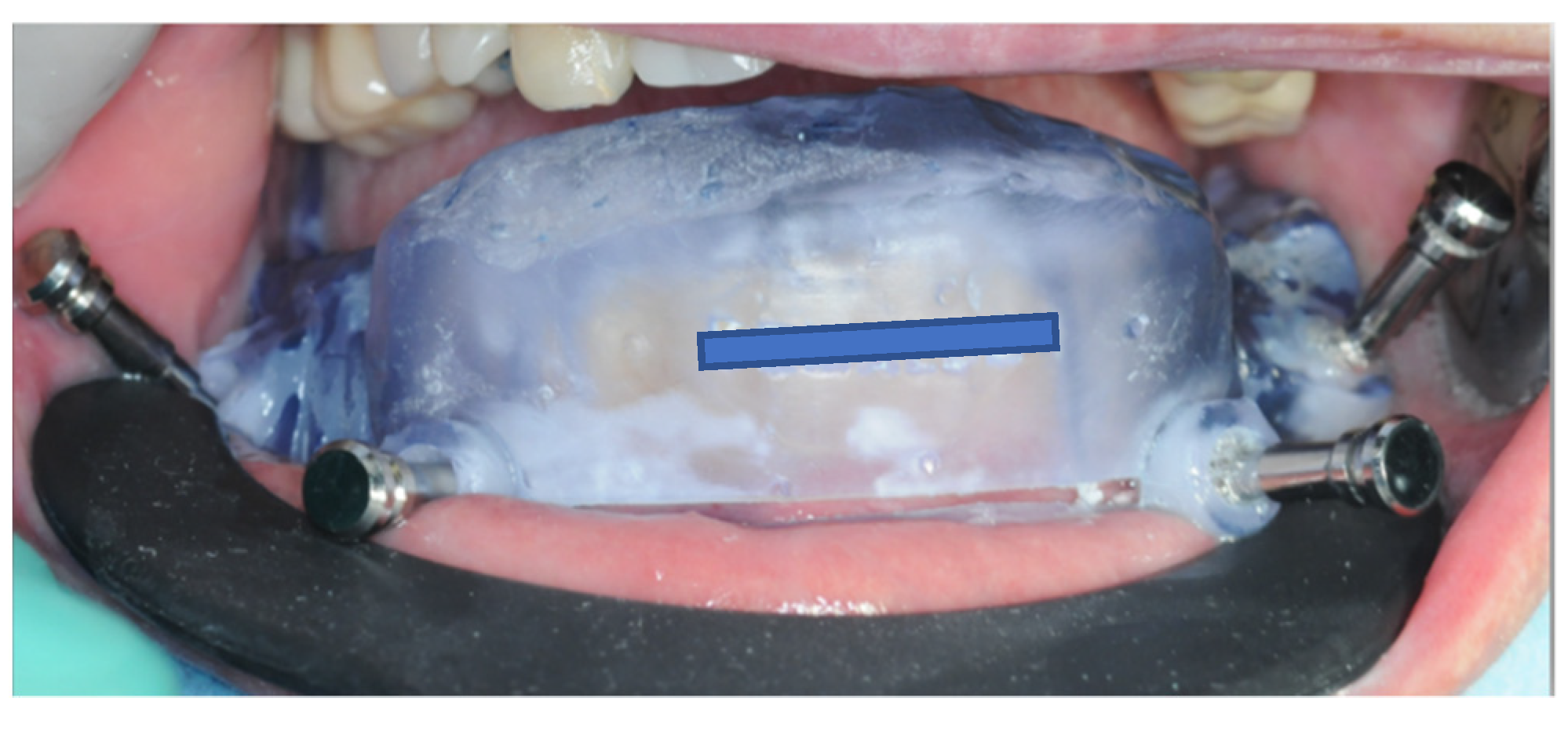
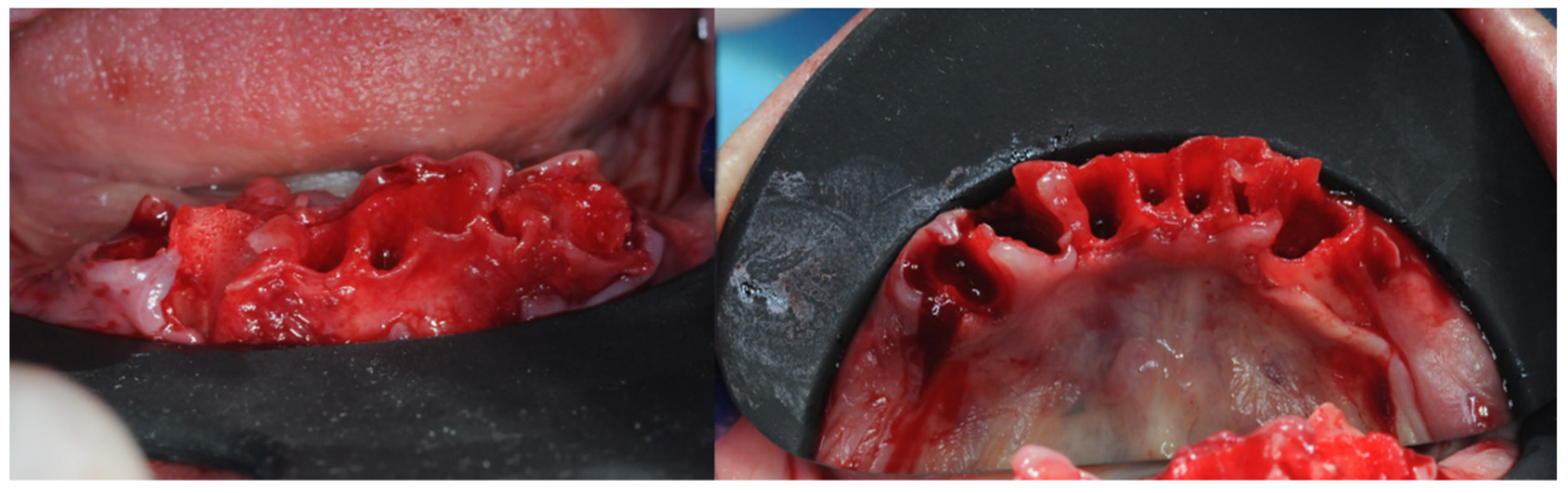
4.6. Surgical Procedure
4.7. Evaluation of the Clinical Effect Immediately after the Operation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chan, M.H.; Nudell, Y.A. All-on-4 Concept Update. Dent. Clin. N. Am. 2020, 65, 211–227. [Google Scholar] [CrossRef] [PubMed]
- Beretta, M.; Poli, P.P.; Tansella, S.; Maiorana, C. Virtually guided alveolar ridge reduction combined with computer-aided implant placement for a bimaxillary implant-supported rehabilitation: A clinical report. J. Prosthet. Dent. 2018, 120, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Nikoyan, L. Guided Implant Surgery. Dent. Clin. N. Am. 2021, 65, 67–80. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.Y.; Yu, J.Y.; Xie, C.Y.; Gao, J.; Yu, H.Y. Immediate precision of the digital osteotomy template in the digital stackable template: A clinical study. Hua Xi Kou Qiang Yi Xue Za Zhi 2021, 39, 732–738. [Google Scholar] [CrossRef]
- Sun, H.; Zhang, J.; Li, B.; Liu, Z.; Shen, S.; Wang, X. Accuracy of a new custom-made bone-supported osteotomy and repositioning guide system for reconstruction of the mandibular ramus using costochondral grafts: A preliminary study. Br. J. Oral Maxillofac. Surg. 2020, 58, 51–56. [Google Scholar] [CrossRef]
- Gangwani, K.D.; Shetty, L.; Kulkarni, D.; Seshagiri, R.; Chopra, R. Piezosurgery versus conventional method alveoloplasty. Ann. Maxillofac. Surg. 2018, 8, 181–187. [Google Scholar] [CrossRef]
- Zhu, M.; Liu, F.; Zhou, C.; Lin, L.; Zhang, Y.; Chai, G.; Xie, L.; Qi, F.; Li, Q. Does intraoperative navigation improve the accuracy of mandibular angle osteotomy: Comparison between augmented reality navigation, individualised templates and free-hand techniques. J. Plast. Reconstr. Aesthetic Surg. 2018, 71, 1188–1195. [Google Scholar] [CrossRef]
- Cushen, S.E.; Turkyilmaz, I. Impact of operator experience on the accuracy of implant placement with stereolithographic surgical templates: An in vitro study. J. Prosthet. Dent. 2013, 109, 248–254. [Google Scholar] [CrossRef]
- Rizzo, S.; Lupi, S.M.; Zampetti, P. Nerve damage resulting from oral surgery and medical legal implications. BioCensus 2009, 1, 86–94. [Google Scholar]
- Nejad, M.F.; Proussaefs, P.; Lozada, J. Combining guided alveolar ridge reduction and guided implant placement for all-on-4 surgery: A clinical report. J. Prosthet. Dent. 2016, 115, 662–667. [Google Scholar] [CrossRef]
- Li, J.; Chen, Z.; Dong, B.; Wang, H.; Joda, T.; Yu, H. Registering Maxillomandibular Relation to Create a Virtual Patient Integrated with a Virtual Articulator for Complex Implant Rehabilitation: A Clinical Report. J. Prosthodont. 2020, 29, 553–557. [Google Scholar] [CrossRef]
- Tian, Y.; Chen, C.; Xu, X.; Wang, J.; Hou, X.; Li, K.; Lu, X.; Shi, H.; Lee, E.-S.; Jiang, H.B. A Review of 3D Printing in Dentistry: Technologies, Affecting Factors, and Applications. Scanning 2021, 2021, 9950131. [Google Scholar] [CrossRef]
- Dawood, A.; Marti, B.M.; Sauret-Jackson, V. 3D printing in dentistry. Br. Dent. J. 2015, 219, 521–529. [Google Scholar] [CrossRef]
- Khorsandi, D.; Fahimipour, A.; Abasian, P.; Saber, S.S.; Seyedi, M.; Ghanavati, S.; Ahmad, A.; De Stephanis, A.A.; Taghavinezhaddilami, F.; Leonova, A.; et al. 3D and 4D printing in dentistry and maxillofacial surgery: Printing techniques, materials, and applications. Acta Biomater. 2021, 122, 26–49. [Google Scholar] [CrossRef]
- Ku, J.-K.; Lee, J.; Lee, H.-J.; Yun, P.-Y.; Kim, Y.-K. Accuracy of dental implant placement with computer-guided surgery: A retrospective cohort study. BMC Oral Heal. 2022, 22, 8. [Google Scholar] [CrossRef]
- Kim, M.-J.; Jeong, J.Y.; Ryu, J.; Jung, S.; Park, H.-J.; Oh, H.-K.; Kook, M.-S. Accuracy of digital surgical guides for dental implants. Maxillofac. Plast. Reconstr. Surg. 2022, 44, 35. [Google Scholar] [CrossRef]
- Flügge, T.; Kramer, J.; Nelson, K.; Nahles, S.; Kernen, F. Digital implantology—A review of virtual planning software for guided implant surgery. Part II: Prosthetic set-up and virtual implant planning. BMC Oral Health 2022, 22, 23. [Google Scholar] [CrossRef]
- Kernen, F.; Kramer, J.; Wanner, L.; Wismeijer, D.; Nelson, K.; Flügge, T. A review of virtual planning software for guided implant surgery-data import and visualization, drill guide design and manufacturing. BMC Oral Health 2020, 20, 251. [Google Scholar] [CrossRef]
- Kalaivani, G.; Balaji, V.R.; Manikandan, D.; Rohini, G. Expectation and reality of guided implant surgery protocol using computer-assisted static and dynamic navigation system at present scenario: Evidence-based literature review. J. Indian Soc. Periodontol. 2020, 24, 398–408. [Google Scholar] [CrossRef]
- Ma, B.; Park, T.; Chun, I.; Yun, K. The accuracy of a 3D printing surgical guide determined by CBCT and model analysis. J. Adv. Prosthodont. 2018, 10, 279–285. [Google Scholar] [CrossRef]
- Todaro, C.; Torchia, M.; Benazzo, M.; Baena, R.R.Y.; Canzi, P.; Lupi, S.M. Overview and Future Perspectives on Bone 3D Bioprinting. J. Pharm. Res. Int. 2022, 34, 32–48. [Google Scholar] [CrossRef]
- Suganna, M.; Kausher, H.; Ali, A.B.M.R.; Abed, M.M.; Albishi, W.S.; Al Hajji, F.A.; Sultan, N.A. Knowledge on Applications of 3D Design and Printing in Dentistry Among Dental Practitioners in Saudi Arabia: A Questionnaire-Based Survey. Cureus 2022, 14, e28379. [Google Scholar] [CrossRef] [PubMed]
- Testori, T.; Weinstein, T.; Scutellà, F.; Wang, H.-L.; Zucchelli, G. Implant placement in the esthetic area: Criteria for positioning single and multiple implants. Periodontology 2000 2018, 77, 176–196. [Google Scholar] [CrossRef] [PubMed]
- Pascual, D.; Vaysse, J. Chirurgie implantaire et prothèse guidées et assistées par ordinateur: Le flux numérique continu. Rev. Stomatol. Chir. Maxillo-Faciale Chir. Orale 2016, 117, 28–35. [Google Scholar] [CrossRef]
- Carpentieri, J.; Greenstein, G.; Cavallaro, J. Hierarchy of restorative space required for different types of dental implant prostheses. J. Am. Dent. Assoc. 2019, 150, 695–706. [Google Scholar] [CrossRef]
- Jones, G.G.; Jaere, M.; Clarke, S.; Cobb, J. 3D printing and high tibial osteotomy. EFORT Open Rev. 2018, 3, 254–259. [Google Scholar] [CrossRef]
- Shelton, T.J.; Monazzam, S.; Calafi, A.; Leshikar, H.B.; Haus, B.M. Preoperative 3D Modeling and Printing for Guiding Periacetabular Osteotomy. J. Pediatr. Orthop. 2021, 41, 149–158. [Google Scholar] [CrossRef]
- Hegedus, T.; Kreuter, P.; Kismarczi-Antalffy, A.A.; Demeter, T.; Banyai, D.; Vegh, A.; Geczi, Z.; Hermann, P.; Payer, M.; Zsembery, A.; et al. User Experience and Sustainability of 3D Printing in Dentistry. Int. J. Environ. Res. Public Health 2022, 19, 1921. [Google Scholar] [CrossRef]
- Joda, T.; Zarone, F.; Ferrari, M. The complete digital workflow in fixed prosthodontics: A systematic review. BMC Oral Health 2017, 17, 124. [Google Scholar] [CrossRef]
- Srinivasan, M.; Kamnoedboon, P.; McKenna, G.; Angst, L.; Schimmel, M.; Özcan, M.; Müller, F. CAD-CAM removable complete dentures: A systematic review and meta-analysis of trueness of fit, biocompatibility, mechanical properties, surface characteristics, color stability, time-cost analysis, clinical and patient-reported outcomes. J. Dent. 2021, 113, 103777. [Google Scholar] [CrossRef]
- HLerner, H.; Hauschild, U.; Sader, R.; Ghanaati, S. Complete-arch fixed reconstruction by means of guided surgery and immediate loading: A retrospective clinical study on 12 patients with 1 year of follow-up. BMC Oral Health 2020, 20, 15. [Google Scholar] [CrossRef]
- Bover-Ramos, F.; Viña-Almunia, J.; Cervera-Ballester, J.; Peñarrocha-Diago, M.; García-Mira, B. Accuracy of Implant Placement with Computer-Guided Surgery: A Systematic Review and Meta-Analysis Comparing Cadaver, Clinical, and In Vitro Studies. Int. J. Oral Maxillofac. Implant. 2018, 33, 101–115. [Google Scholar] [CrossRef]
- Smitkarn, P.; Subbalekha, K.; Mattheos, N.; Pimkhaokham, A. The accuracy of single-tooth implants placed using fully digital-guided surgery and freehand implant surgery. J. Clin. Periodontol. 2019, 46, 949–957. [Google Scholar] [CrossRef]
- De Stavola, L.; Fincato, A.; Bressan, E.; Gobbato, L. Results of Computer-Guided Bone Block Harvesting from the Mandible: A Case Series. Int. J. Periodontics Restor. Dent. 2017, 37, e111–e119. [Google Scholar] [CrossRef]
- Cristoforetti, A.; De Stavola, L.; Fincato, A.; Masè, M.; Ravelli, F.; Nollo, G.; Tessarolo, F. Assessing the accuracy of computer-planned osteotomy guided by stereolithographic template: A methodological framework applied to the mandibular bone harvesting. Comput. Biol. Med. 2019, 114, 103435. [Google Scholar] [CrossRef]
- Arnal-Burró, J.; Pérez-Mañanes, R.; Gallo-Del-Valle, E.; Igualada-Blazquez, C.; Cuervas-Mons, M.; Vaquero-Martín, J. Three dimensional-printed patient-specific cutting guides for femoral varization osteotomy: Do it yourself. Knee 2017, 24, 1359–1368. [Google Scholar] [CrossRef]
- Pérez-Mañanes, R.; Manaute, J.R.; Rodriguez, F.C.; Martín, J.V.; Burró, J.A. 3D Surgical Printing Cutting Guides for Open-Wedge High Tibial Osteotomy: Do It Yourself. J. Knee Surg. 2016, 29, 690–695. [Google Scholar] [CrossRef]
- Shi, J.; Lv, W.; Wang, Y.; Ma, B.; Cui, W.; Liu, Z.; Han, K. Three dimensional patient-specific printed cutting guides for closing-wedge distal femoral osteotomy. Int. Orthop. 2019, 43, 619–624. [Google Scholar] [CrossRef]
- Wang, F.; Zhu, J.; Peng, X.; Su, J. The application of 3D printed surgical guides in resection and reconstruction of malignant bone tumor. Oncol. Lett. 2017, 14, 4581–4584. [Google Scholar] [CrossRef]
- Park, J.W.; Kang, H.G.; Kim, J.H.; Kim, H.-S. The application of 3D-printing technology in pelvic bone tumor surgery. J. Orthop. Sci. 2021, 26, 276–283. [Google Scholar] [CrossRef]
- El Kholy, K.; Lazarin, R.; Janner, S.F.M.; Faerber, K.; Buser, R.; Buser, D. Influence of surgical guide support and implant site location on accuracy of static Computer-Assisted Implant Surgery. Clin. Oral Implant. Res. 2019, 30, 1067–1075. [Google Scholar] [CrossRef] [PubMed]
- Venezia, P.; Torsello, F.; Santomauro, V.; Dibello, V.; Cavalcanti, R. Full Digital Workflow for the Treatment of an Edentulous Patient with Guided Surgery, Immediate Loading and 3D-Printed Hybrid Prosthesis: The BARI Technique 2.0. A Case Report. Int. J. Environ. Res. Public Health 2019, 16, 5160. [Google Scholar] [CrossRef] [PubMed]
- Derksen, W.; Wismeijer, D.; Flügge, T.; Hassan, B.; Tahmaseb, A. The accuracy of computer-guided implant surgery with tooth-supported, digitally designed drill guides based on CBCT and intraoral scanning. A prospective cohort study. Clin. Oral Implant. Res. 2019, 30, 1005–1015. [Google Scholar] [CrossRef] [PubMed]
- Cunha, R.M.; Souza, F.; Hadad, H.; Poli, P.P.; Maiorana, C.; Carvalho, P.S.P. Accuracy evaluation of computer-guided implant surgery associated with prototyped surgical guides. J. Prosthet. Dent. 2021, 125, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Tallarico, M.; Czajkowska, M.; Cicciù, M.; Giardina, F.; Minciarelli, A.; Zadrożny, Ł.; Park, C.-J.; Meloni, S.M. Accuracy of surgical templates with and without metallic sleeves in case of partial arch restorations: A systematic review. J. Dent. 2021, 115, 103852. [Google Scholar] [CrossRef]
- Al-Moraissi, E.; Elmansi, Y.; Al-Sharaee, Y.; Alrmali, A.; Alkhutari, A. Does the piezoelectric surgical technique produce fewer postoperative sequelae after lower third molar surgery than conventional rotary instruments? A systematic review and meta analysis. Int. J. Oral Maxillofac. Surg. 2016, 45, 383–391. [Google Scholar] [CrossRef]
- Cicciù, M.; Stacchi, C.; Fiorillo, L.; Cervino, G.; Troiano, G.; Vercellotti, T.; Herford, A.; Galindo-Moreno, P.; Di Lenarda, R. Piezoelectric bone surgery for impacted lower third molar extraction compared with conventional rotary instruments: A systematic review, meta-analysis, and trial sequential analysis. Int. J. Oral Maxillofac. Surg. 2021, 50, 121–131. [Google Scholar] [CrossRef]
- Gulnahar, Y.; Alpan, A. Comparison of postoperative morbidity between piezoelectric surgery and conventional rotary instruments in mandibular third molar surgery: A split-mouth clinical study. Med. Oral. Patol. Oral. Cir. Bucal. 2021, 26, e269–e275. [Google Scholar] [CrossRef]
- Hassan, B.; Gonzalez, B.G.; Tahmaseb, A.; Greven, M.; Wismeijer, D. A digital approach integrating facial scanning in a CAD-CAM workflow for complete-mouth implant-supported rehabilitation of patients with edentulism: A pilot clinical study. J. Prosthet. Dent. 2017, 117, 486–492. [Google Scholar] [CrossRef]
- Asutay, H.C.; Turkyilmaz, I.; Benli, M.; Martinez, J.L. Transforming smiles using an intraoral scanner and face scan application on smartphone. J. Dent. Sci. 2022, 17, 1413–1414. [Google Scholar] [CrossRef]
- Zhivago, P.; Turkyilmaz, I. A comprehensive digital approach to enhance smiles using an intraoral optical scanner and advanced 3-D sculpting software. J. Dent. Sci. 2021, 16, 784–785. [Google Scholar] [CrossRef]
- Amezua, X.; Iturrate, M.; Garikano, X.; Solaberrieta, E. Analysis of the influence of the facial scanning method on the transfer accuracy of a maxillary digital scan to a 3D face scan for a virtual facebow technique: An in vitro study. J. Prosthet. Dent. 2022, 128, 1024–1031. [Google Scholar] [CrossRef]
- Pérez-Giugovaz, M.G.; Mosier, M.; Revilla-León, M. An additively manufactured intraoral scan body for aiding complete-arch intraoral implant digital scans with guided integration of 3D virtual representation. J. Prosthet. Dent. 2022, 127, 38–43. [Google Scholar] [CrossRef]
- Nuytens, P.; D’Haese, R.; Vandeweghe, S. Reliability and Time Efficiency of Digital vs Analog Bite Registration Technique for the Manufacture of Full-Arch Fixed Implant Prostheses. J. Clin. Med. 2022, 11, 2882. [Google Scholar] [CrossRef]
- Moura, G.F.; Siqueira, R.; Meirelles, L.; Maska, B.; Wang, H.-L.; Mendonça, G. Denture scanning technique for computer-guided implant-supported restoration treatment of edentulous patients. J. Prosthet. Dent. 2021, 125, 726–731. [Google Scholar] [CrossRef]
- Rizzo, S.; Zampetti, P.; Baena, R.R.Y.; Svanosio, D.; Lupi, S.M. Retrospective analysis of 521 endosseous implants placed under antibiotic prophylaxis and review of literature. Minerva Dent. Oral Sci. 2010, 59, 75–88. [Google Scholar] [PubMed]




















Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Todaro, C.; Cerri, M.; Isola, G.; Manazza, A.; Storelli, S.; Rodriguez y Baena, R.; Lupi, S.M. Computer-Guided Osteotomy with Simultaneous Implant Placement and Immediately Loaded Full-Arch Fixed Restoration: A Case Report. Prosthesis 2023, 5, 221-233. https://doi.org/10.3390/prosthesis5010017
Todaro C, Cerri M, Isola G, Manazza A, Storelli S, Rodriguez y Baena R, Lupi SM. Computer-Guided Osteotomy with Simultaneous Implant Placement and Immediately Loaded Full-Arch Fixed Restoration: A Case Report. Prosthesis. 2023; 5(1):221-233. https://doi.org/10.3390/prosthesis5010017
Chicago/Turabian StyleTodaro, Claudia, Michael Cerri, Gaetano Isola, Andrea Manazza, Stefano Storelli, Ruggero Rodriguez y Baena, and Saturnino Marco Lupi. 2023. "Computer-Guided Osteotomy with Simultaneous Implant Placement and Immediately Loaded Full-Arch Fixed Restoration: A Case Report" Prosthesis 5, no. 1: 221-233. https://doi.org/10.3390/prosthesis5010017
APA StyleTodaro, C., Cerri, M., Isola, G., Manazza, A., Storelli, S., Rodriguez y Baena, R., & Lupi, S. M. (2023). Computer-Guided Osteotomy with Simultaneous Implant Placement and Immediately Loaded Full-Arch Fixed Restoration: A Case Report. Prosthesis, 5(1), 221-233. https://doi.org/10.3390/prosthesis5010017