
Using Active Seat Belt Retractions to Mitigate Motion Sickness in Automated Driving


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Motion Sickness in Automated Driving
1.2. Postural Instability and Head Movements during Automated Driving
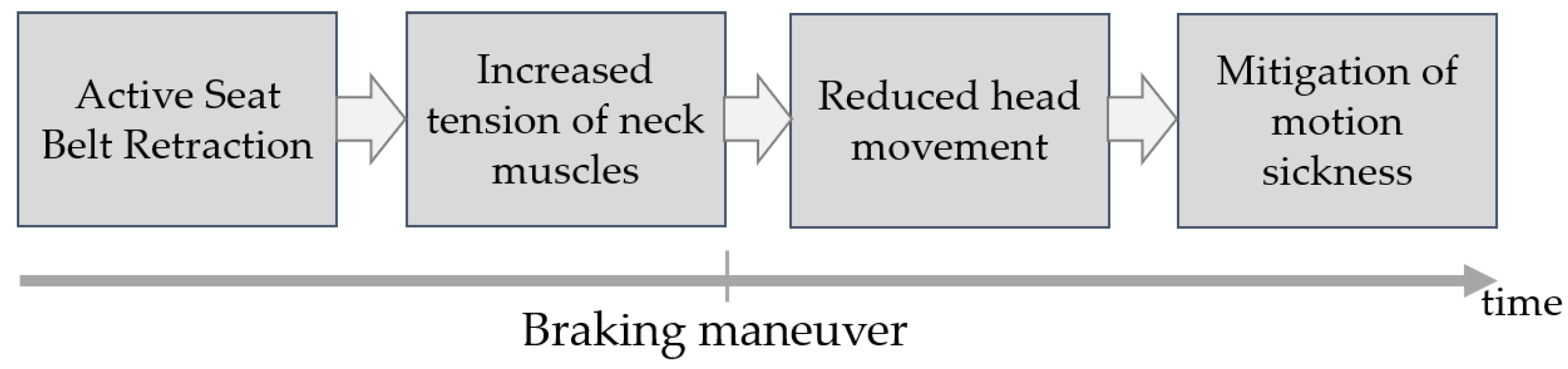
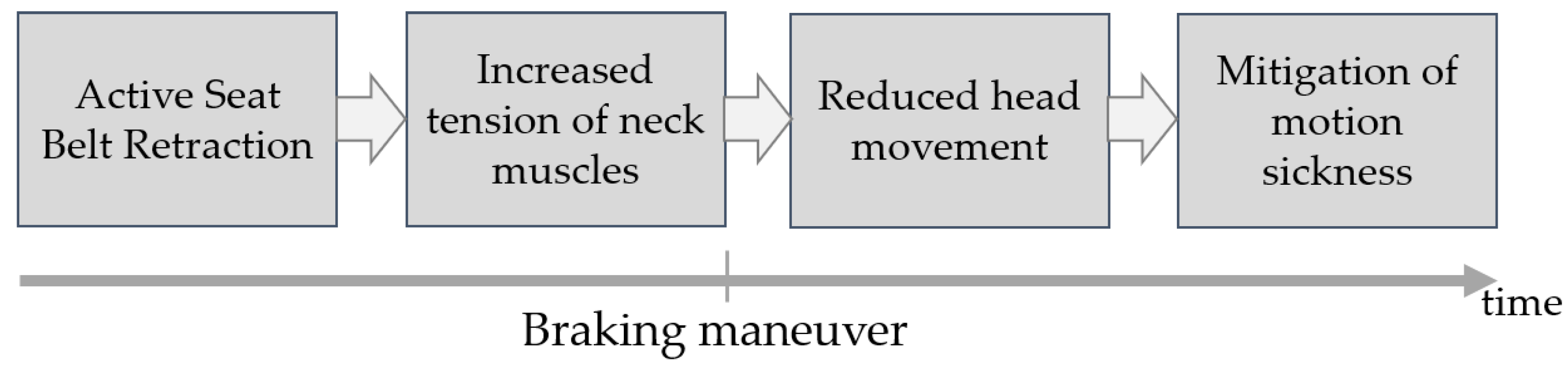
1.3. Active Seat Bealt Retractions as Potential Countermeasure
2. Methods
2.1. Participants
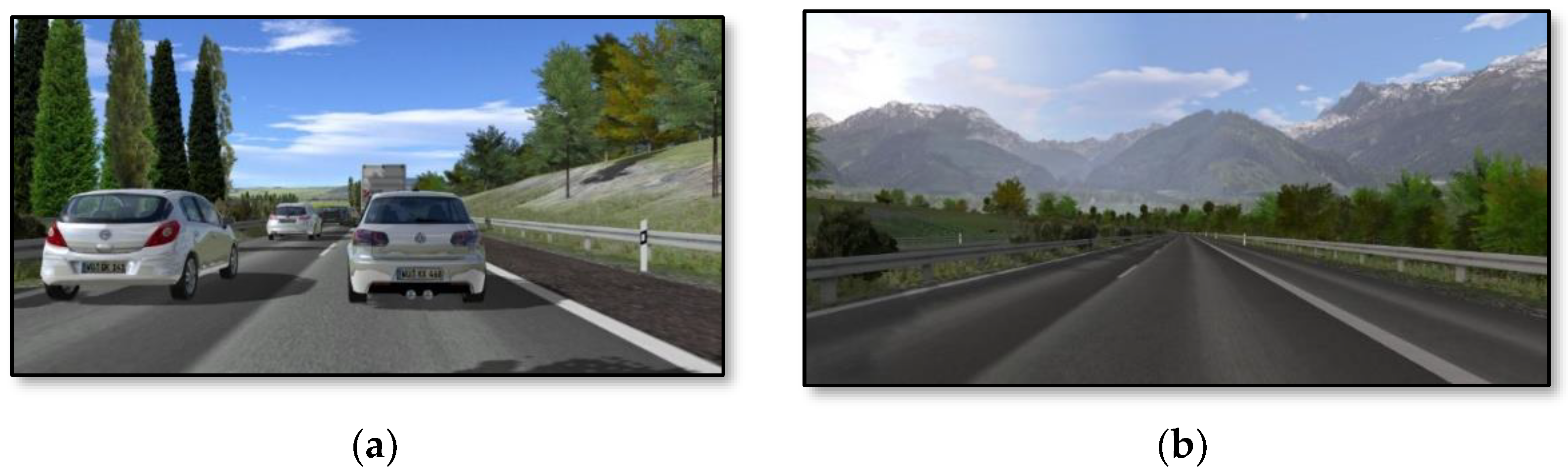
2.2. Driving Simulator and Active Seat Belt Retraction System
2.3. Experimental Design
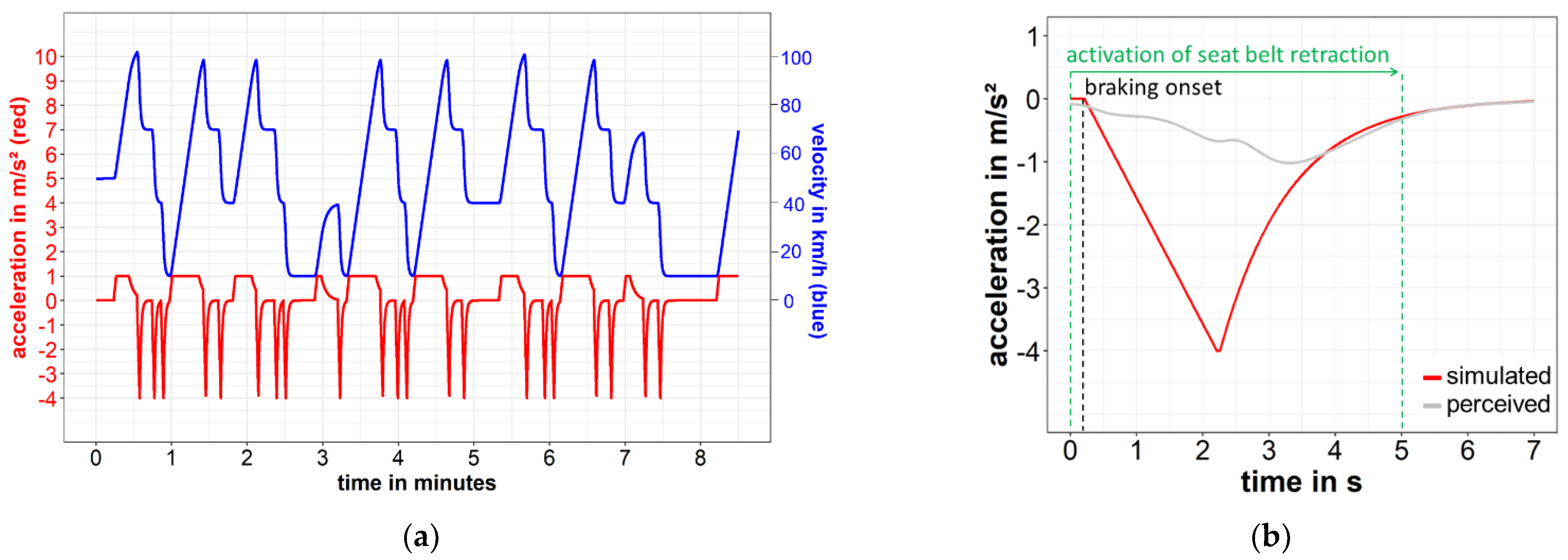
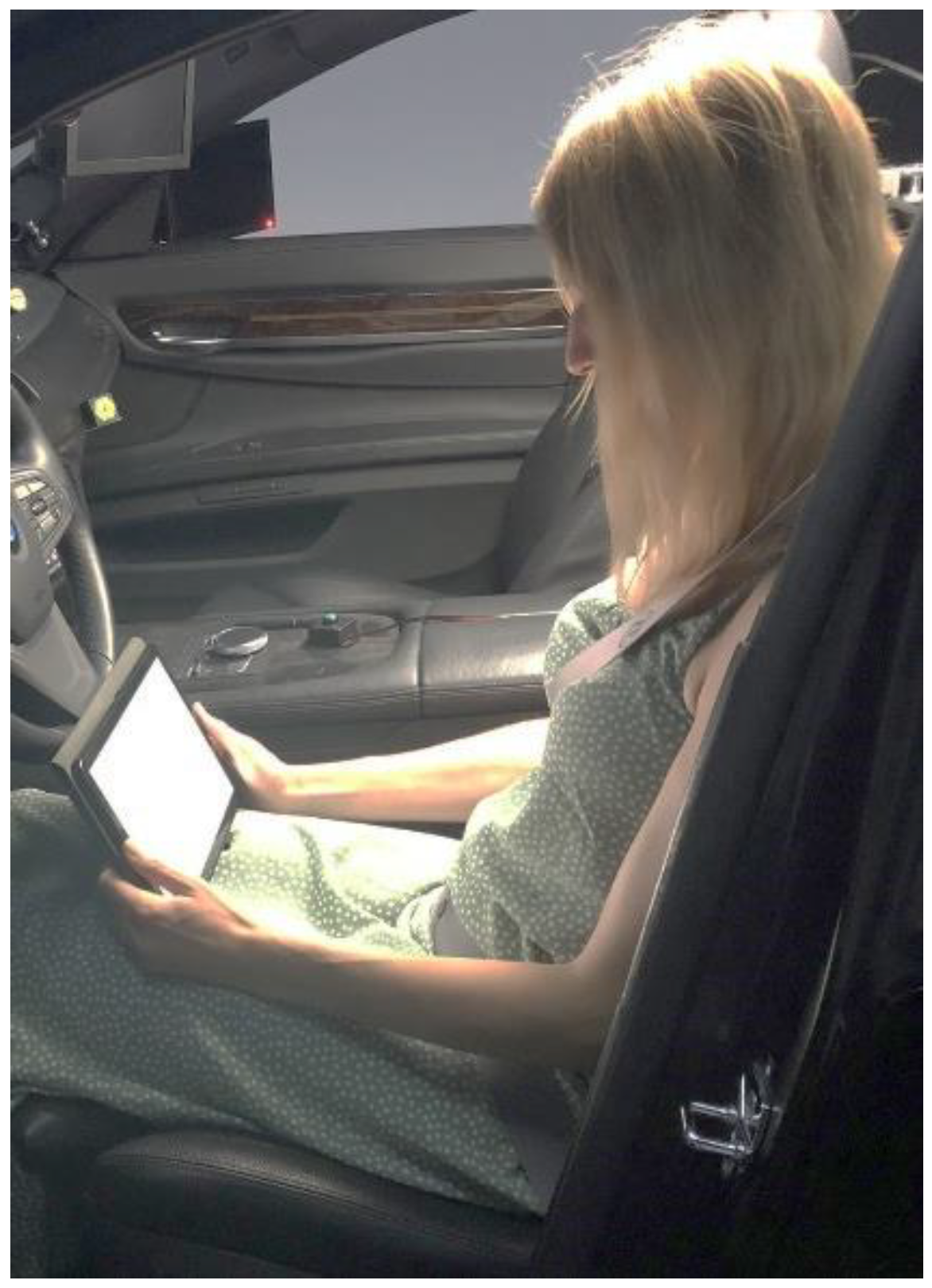
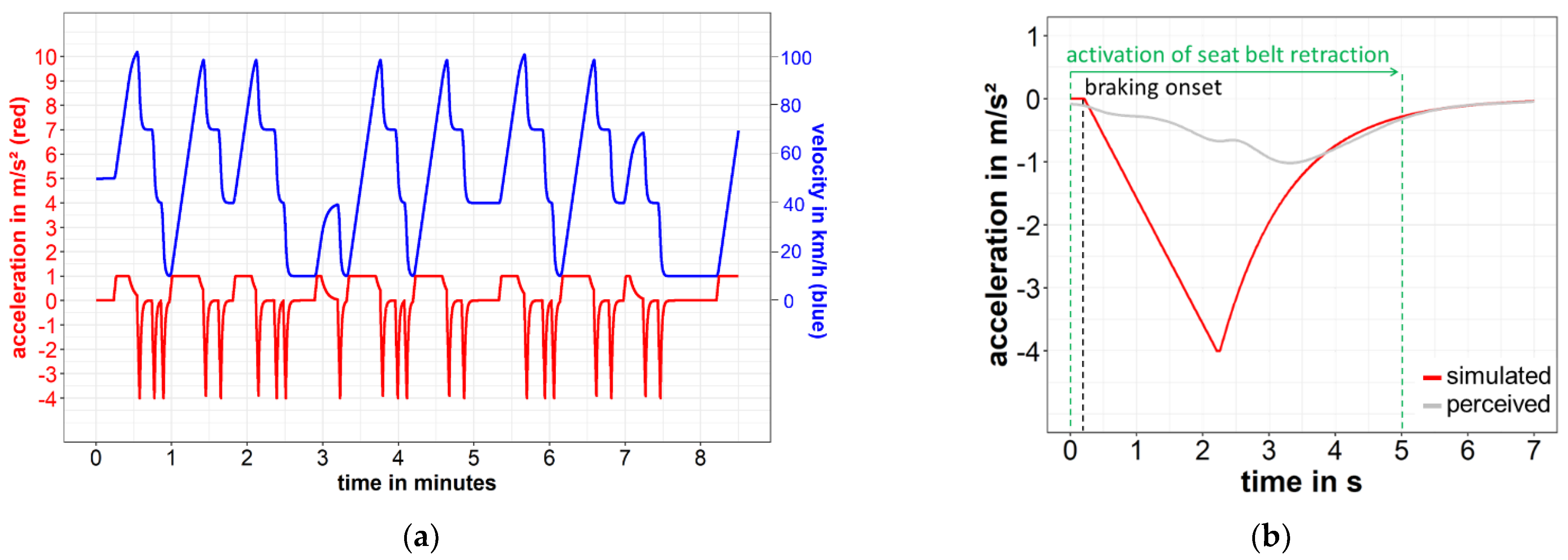
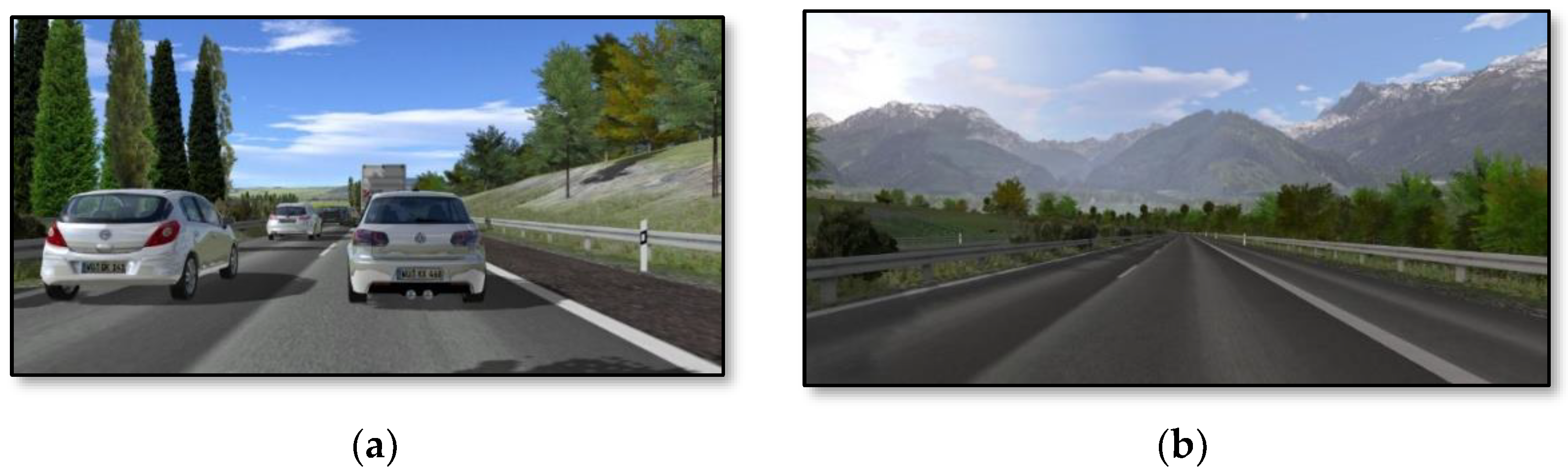
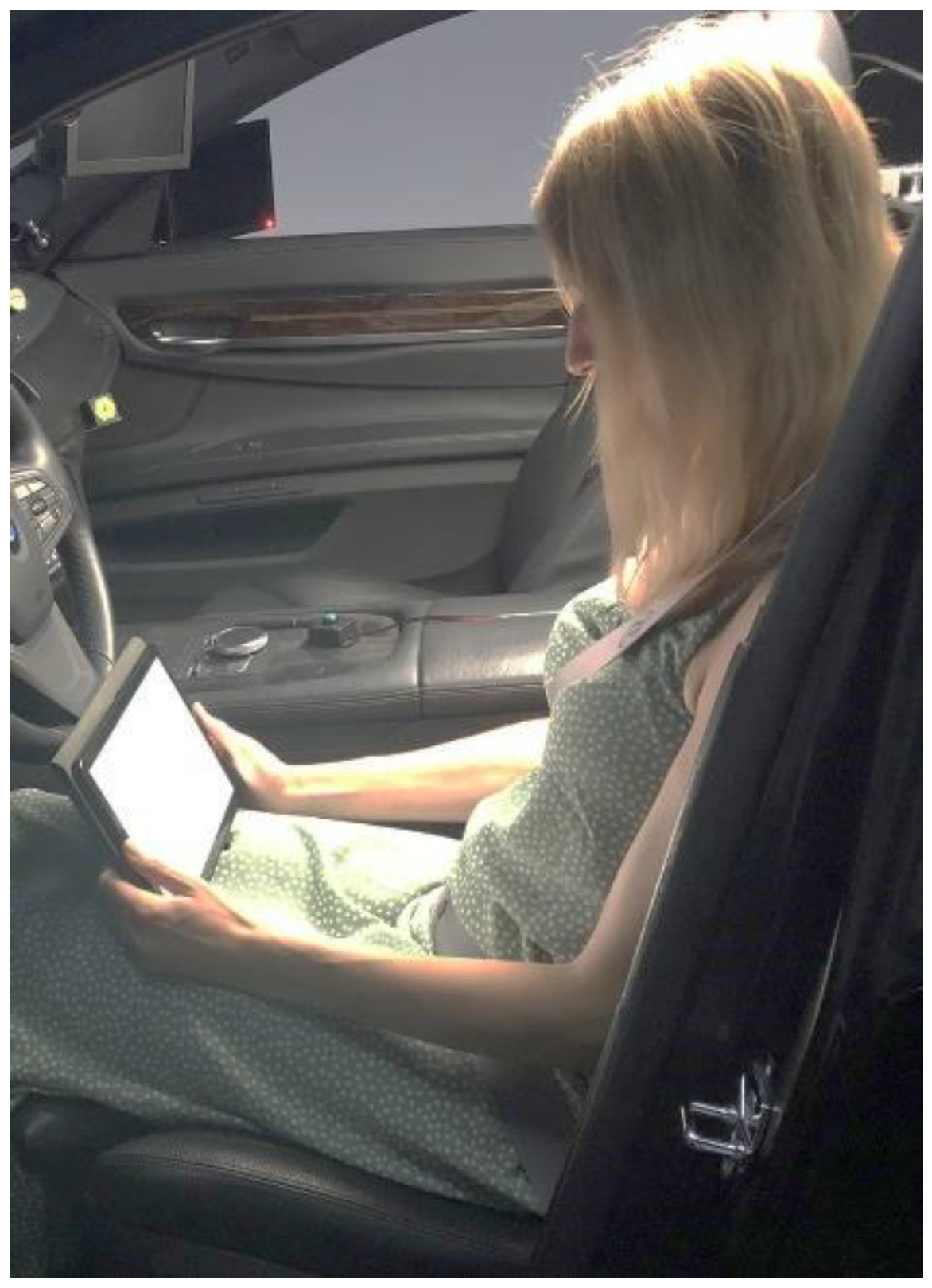
2.4. Driving Profile and NDRT
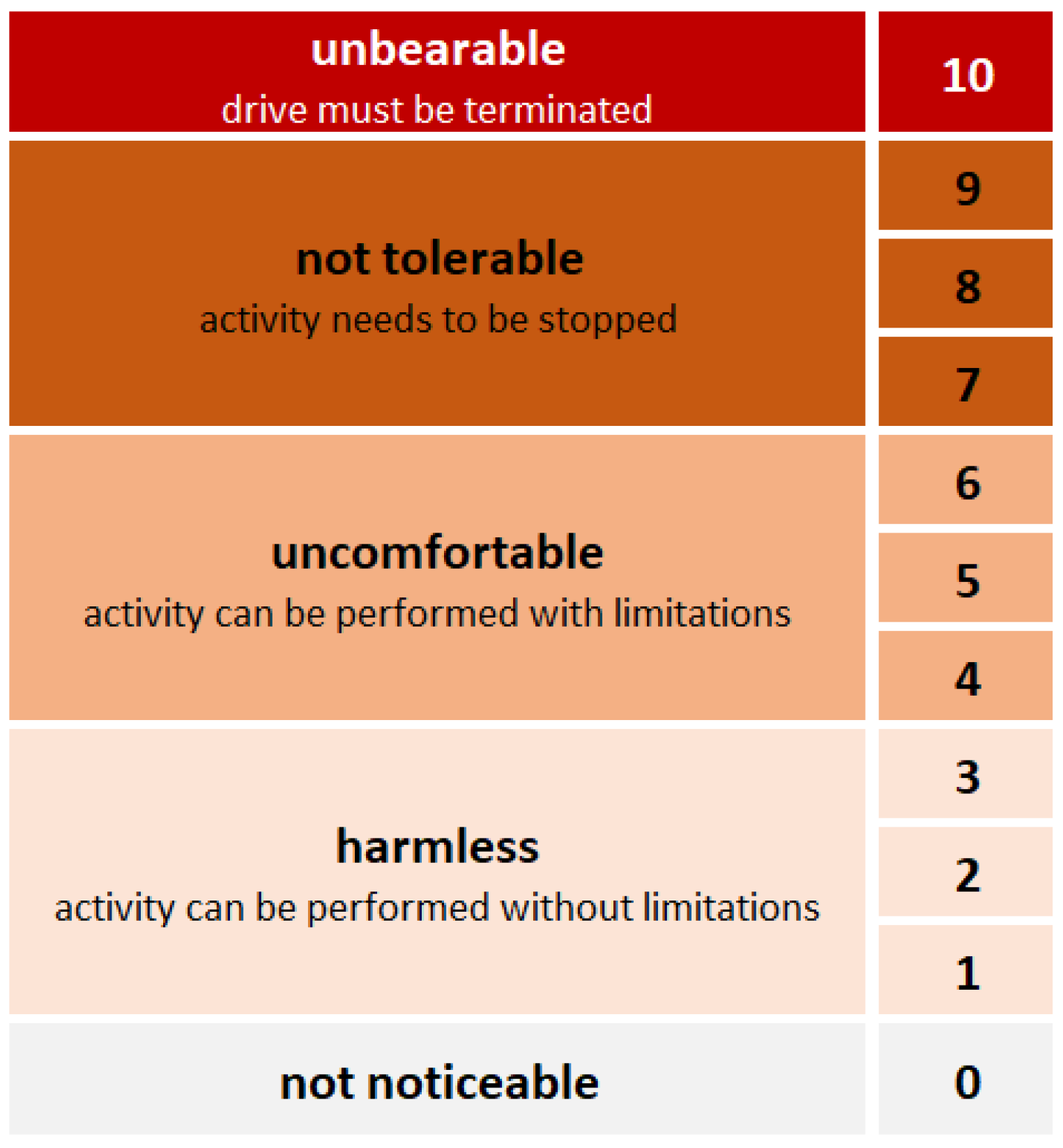
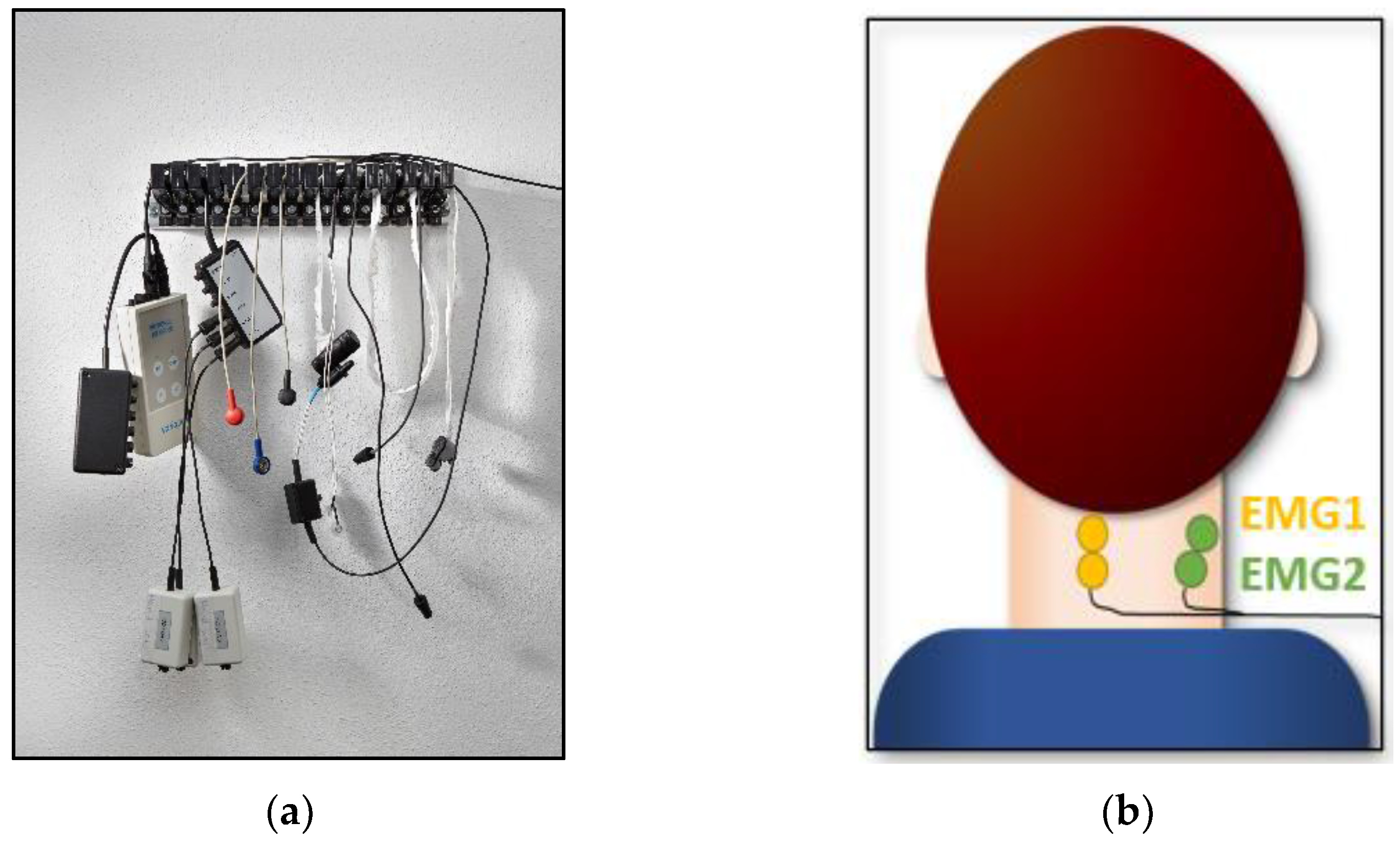
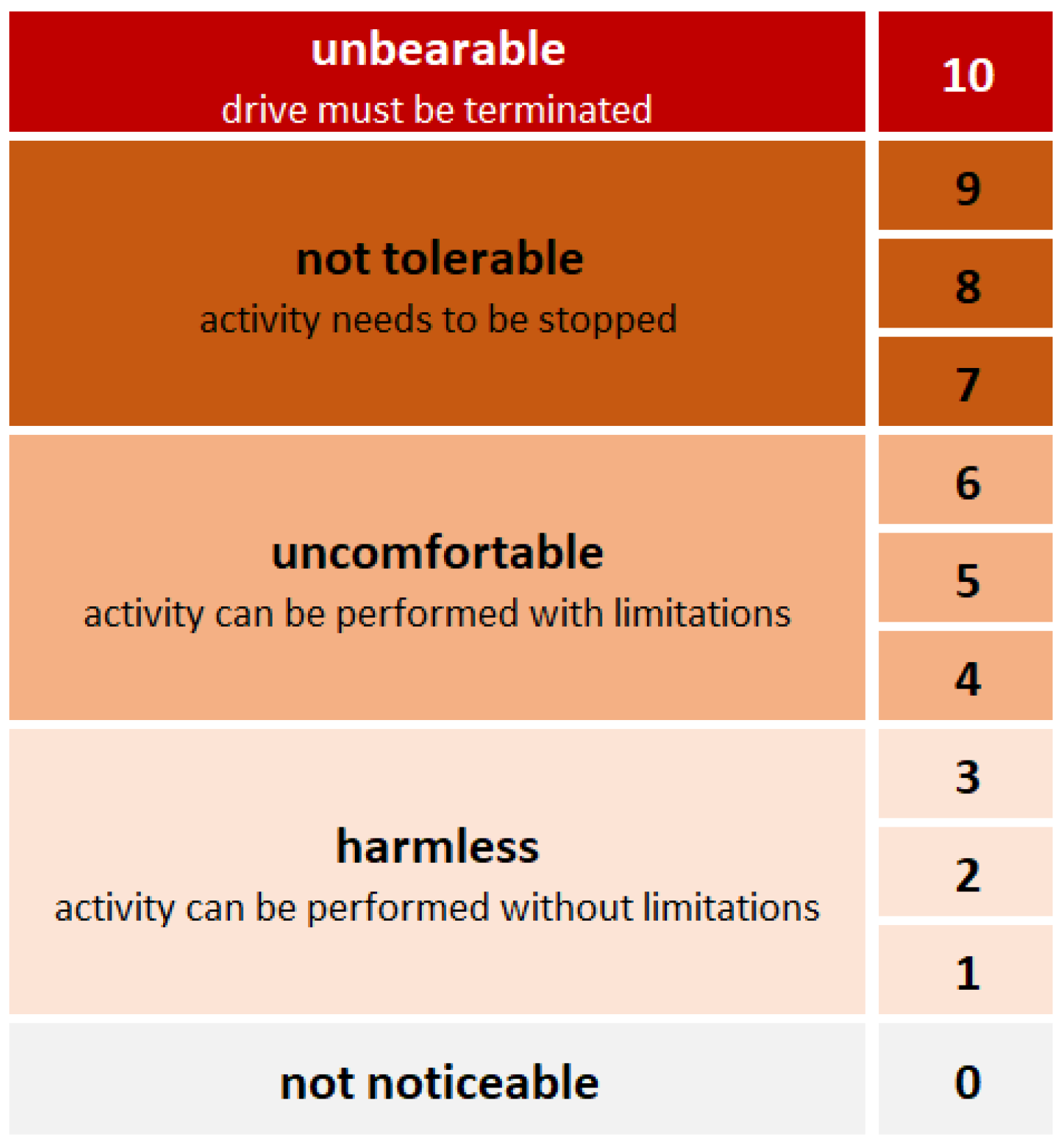
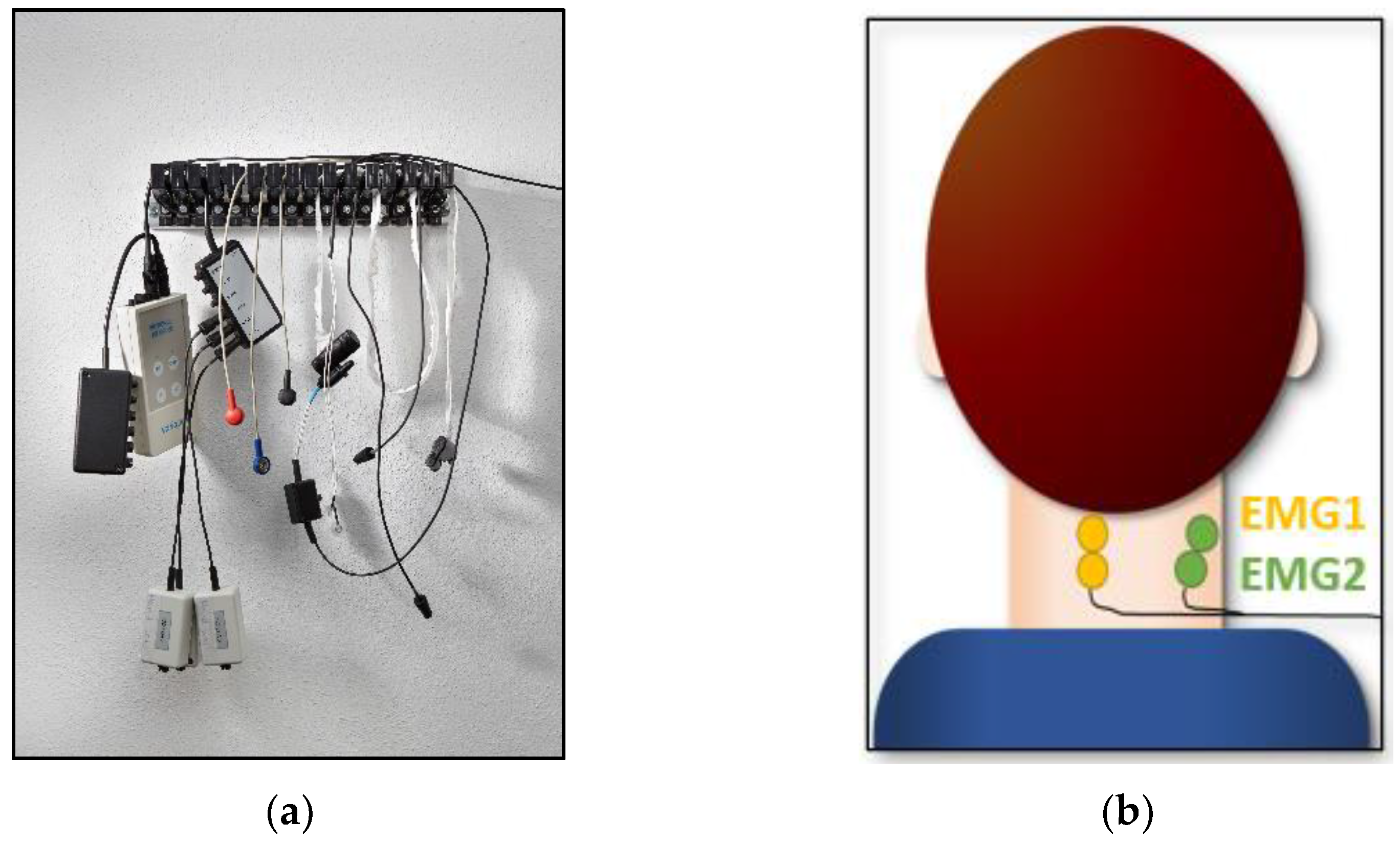
2.5. Dependent Measures and Measuring Instruments
2.6. Procedure
2.7. Data Analysis
3. Results
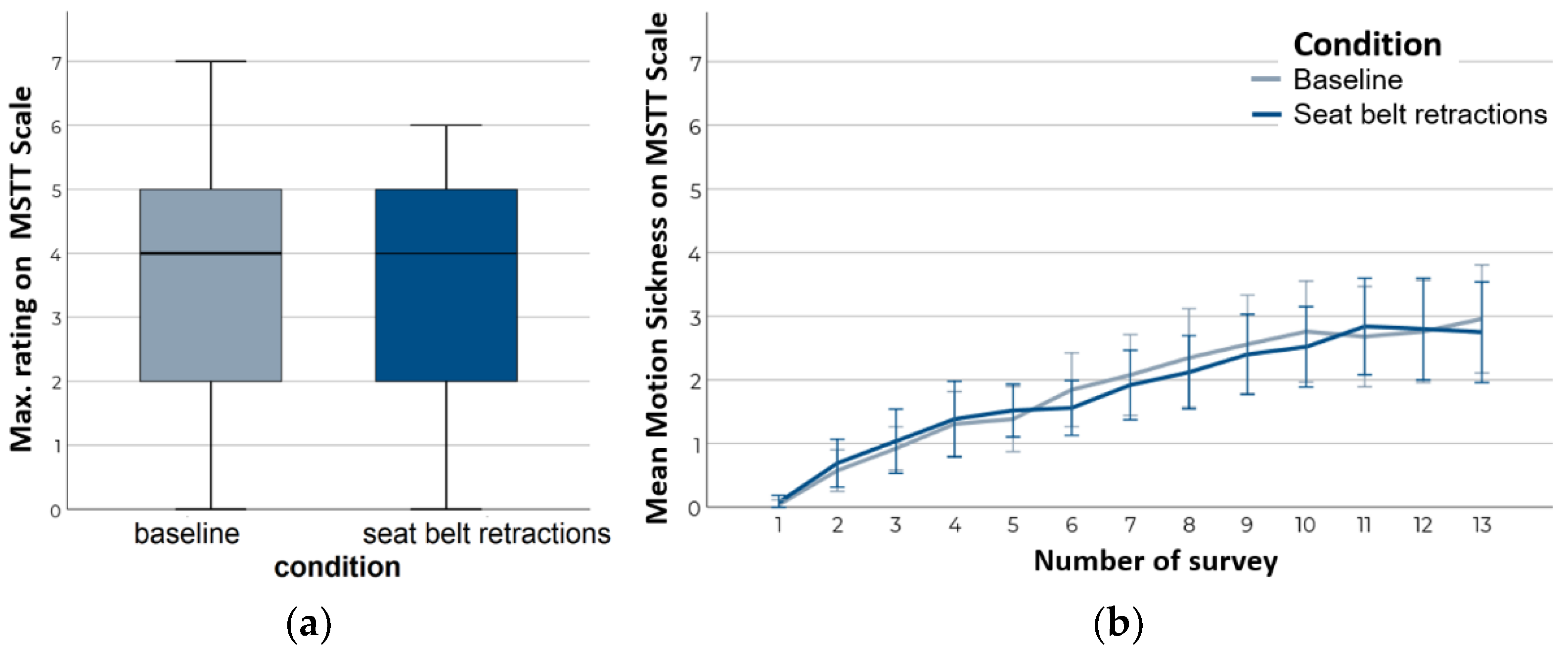
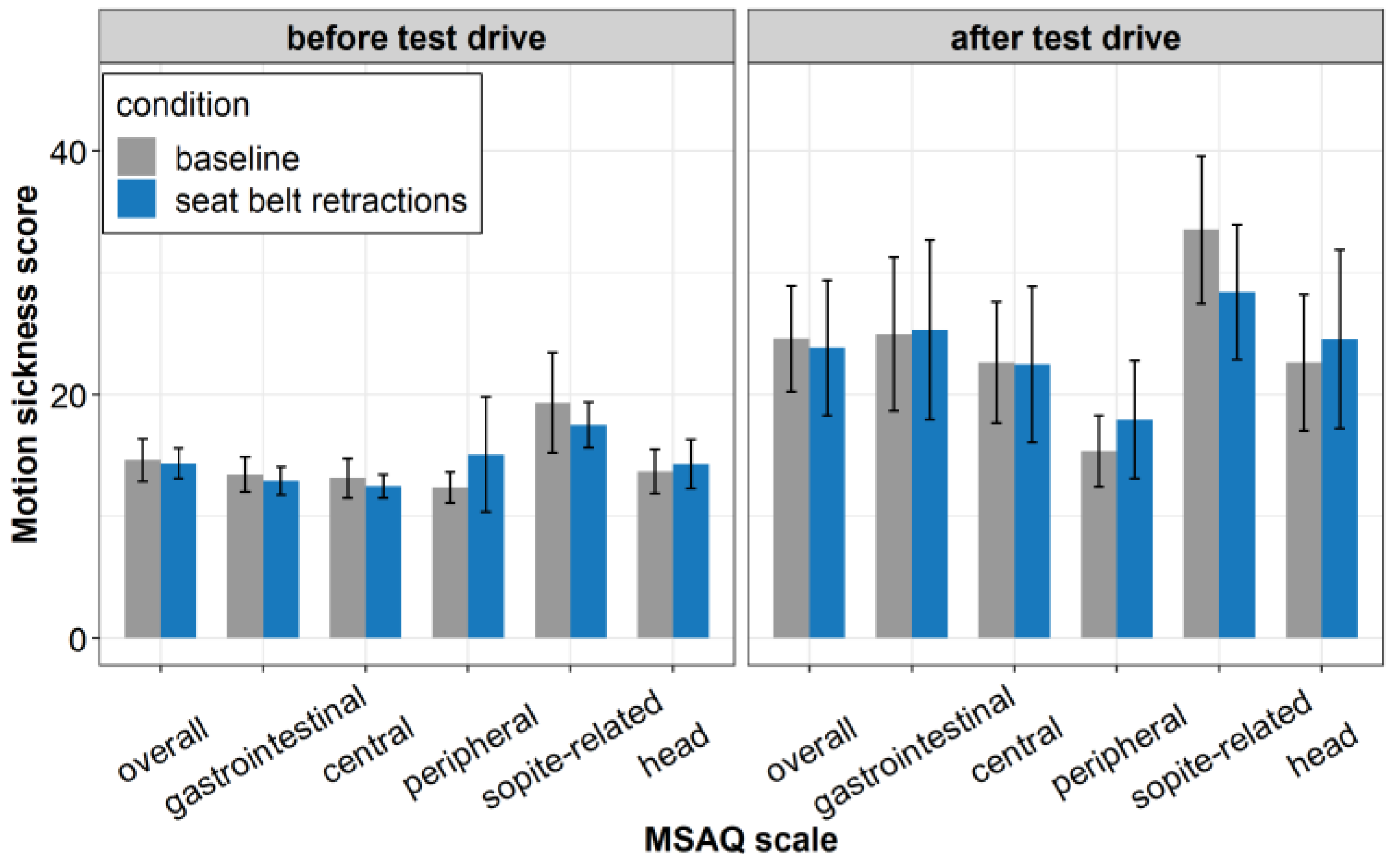
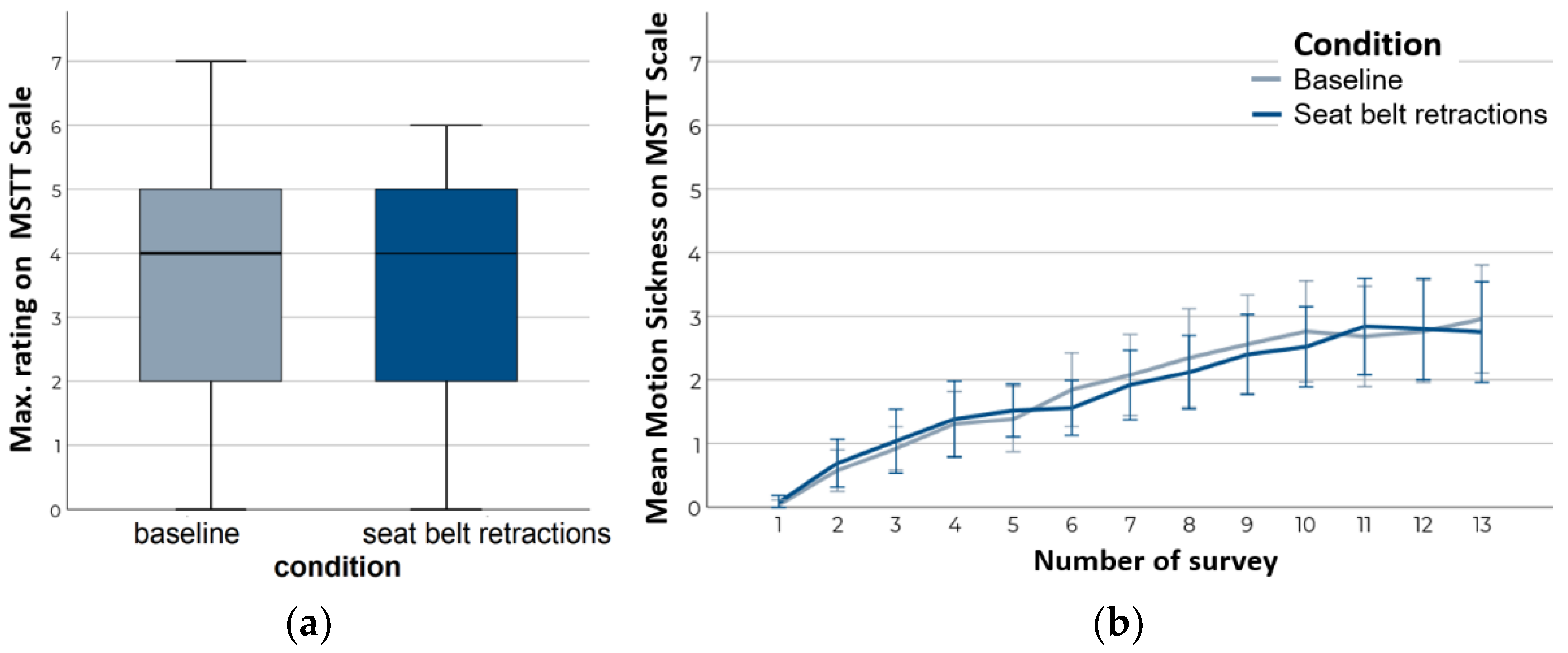
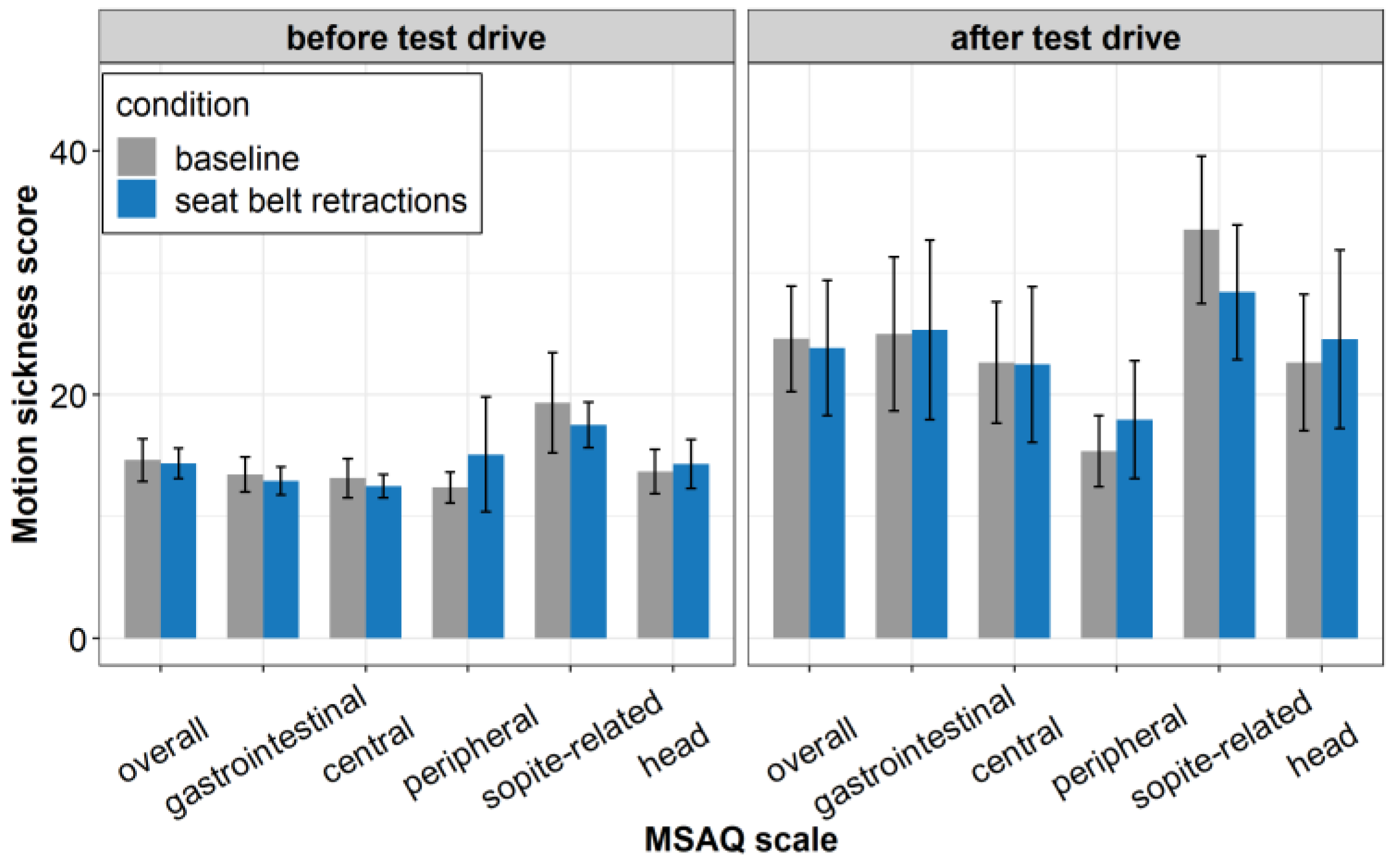
3.1. Motion Sickness
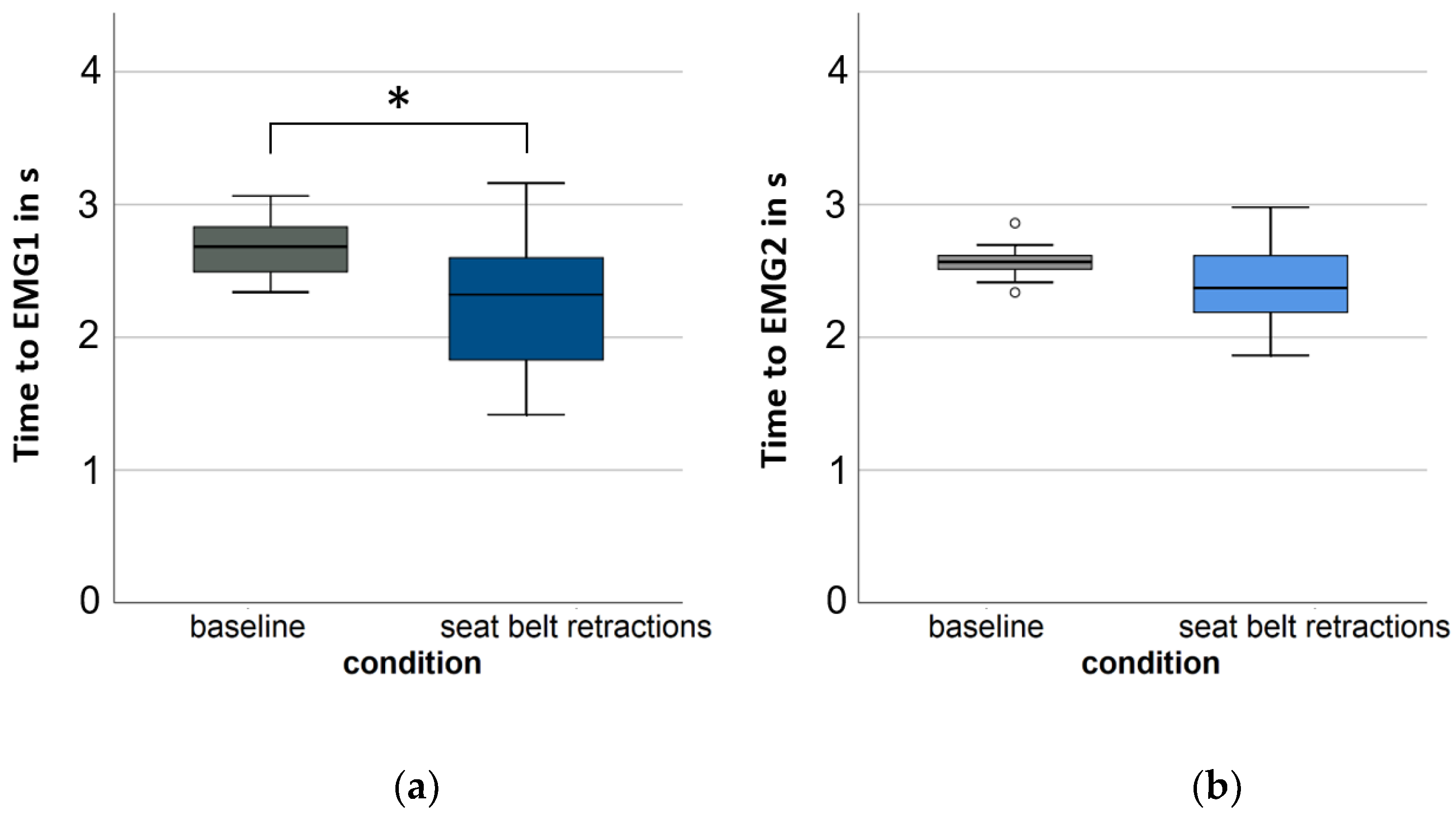
3.2. Anticipatory Effect
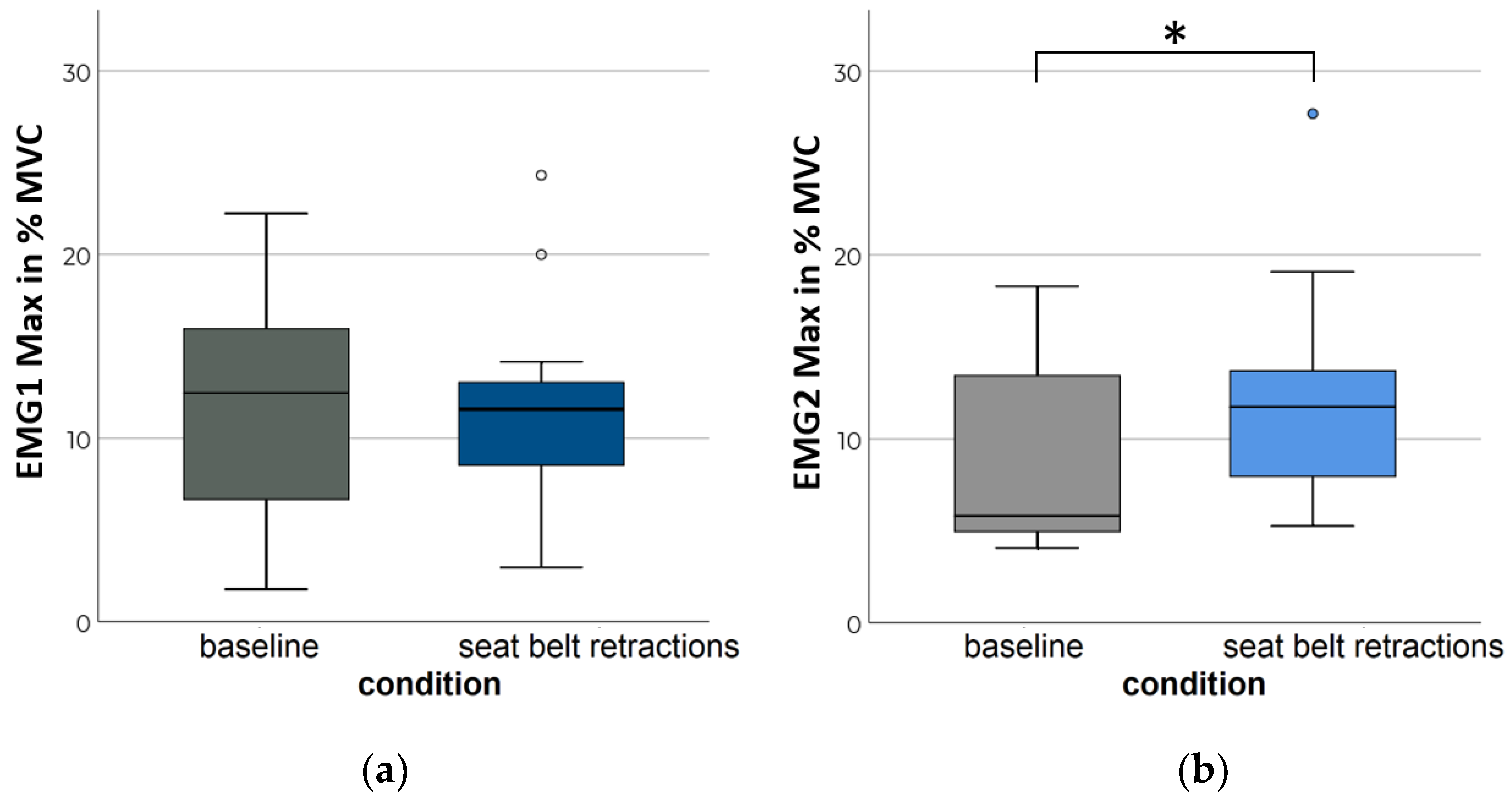
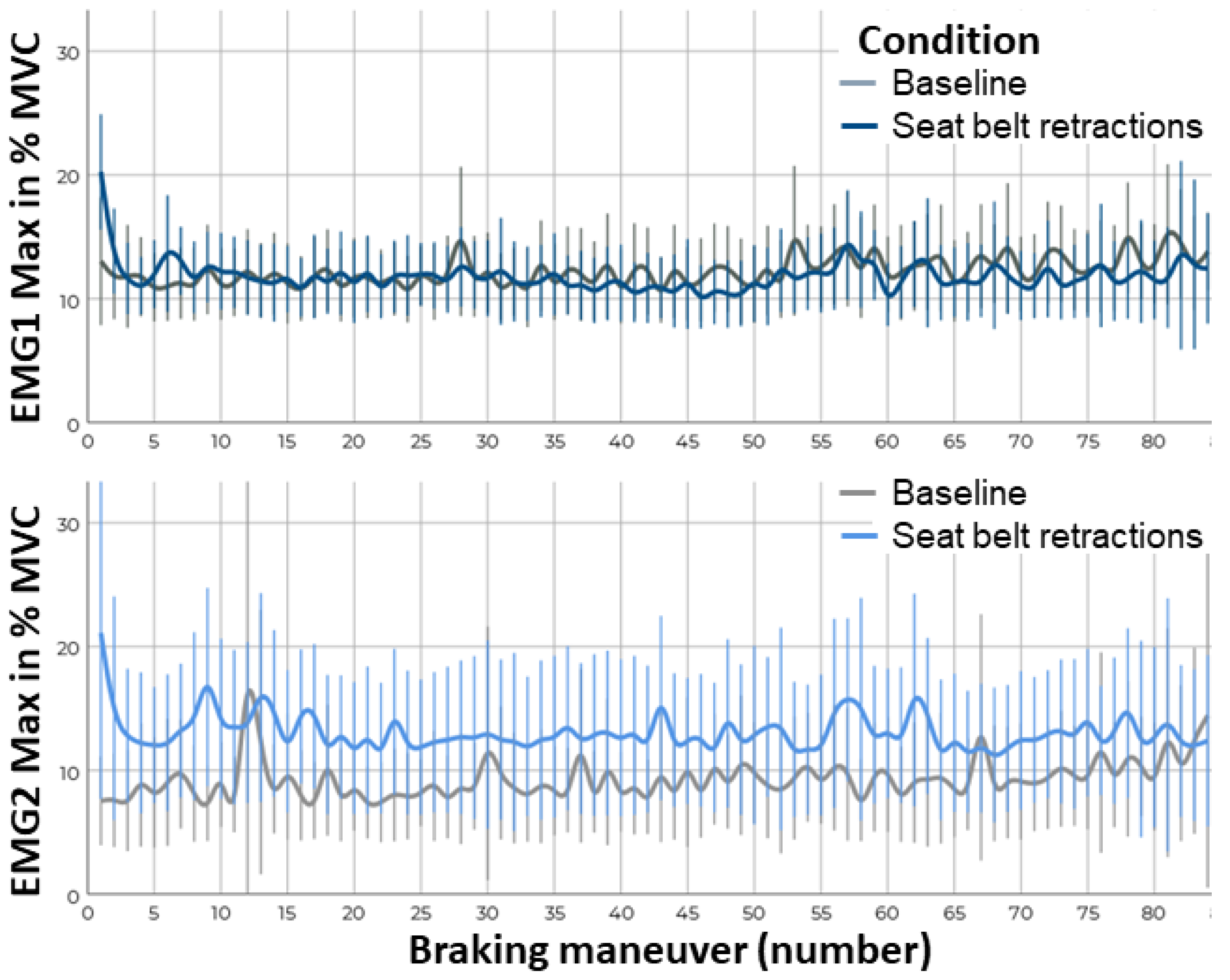
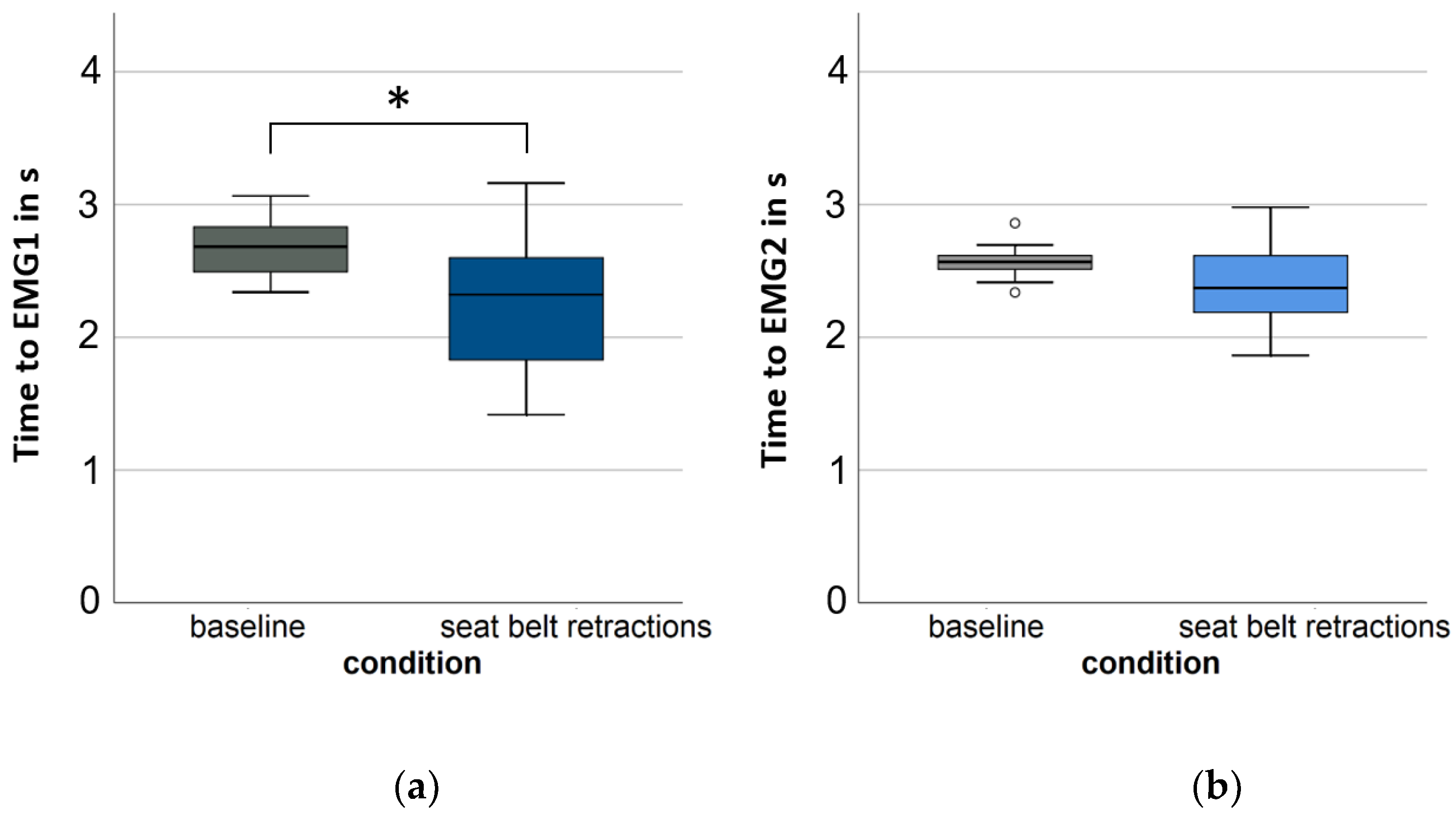
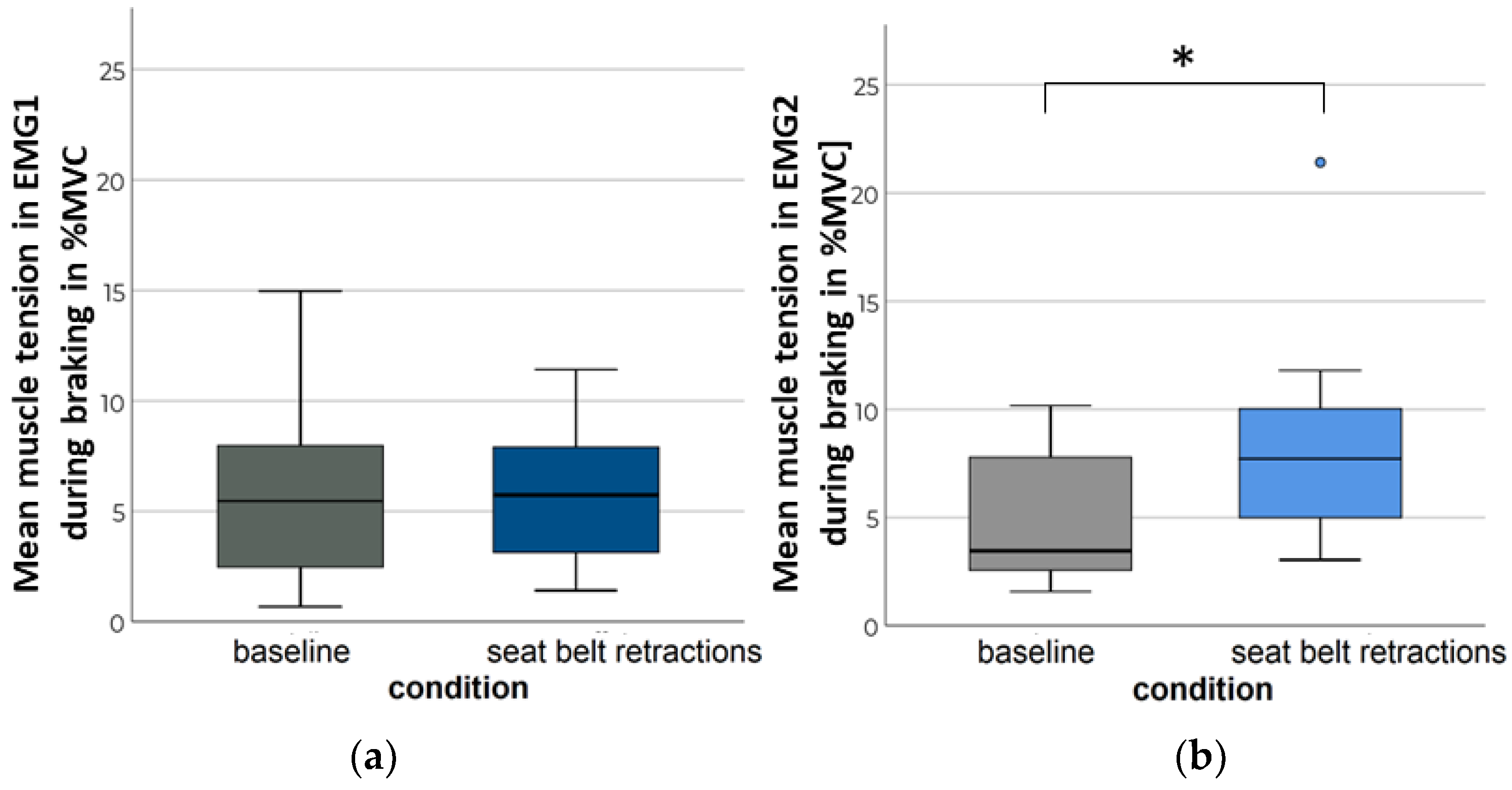
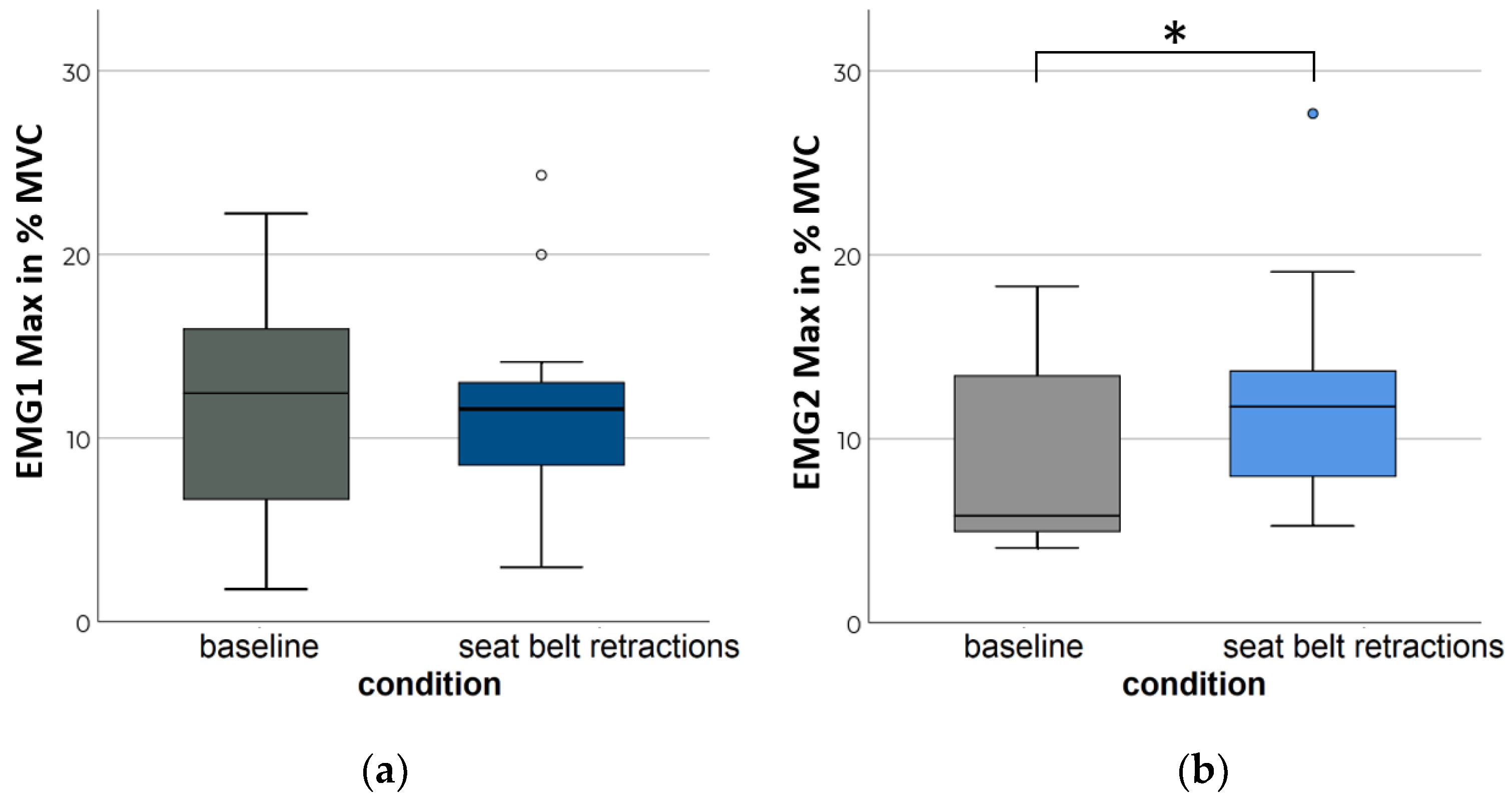
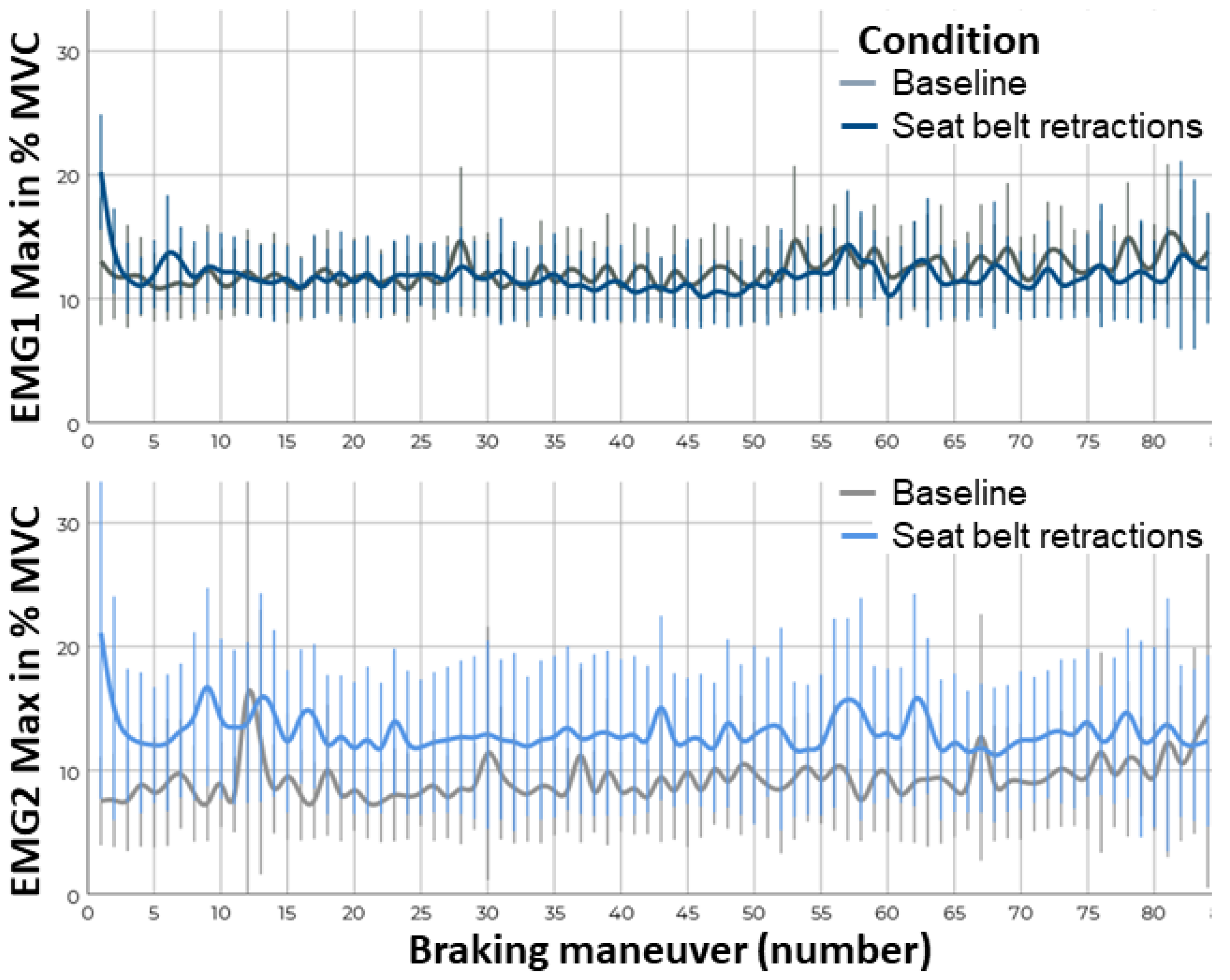
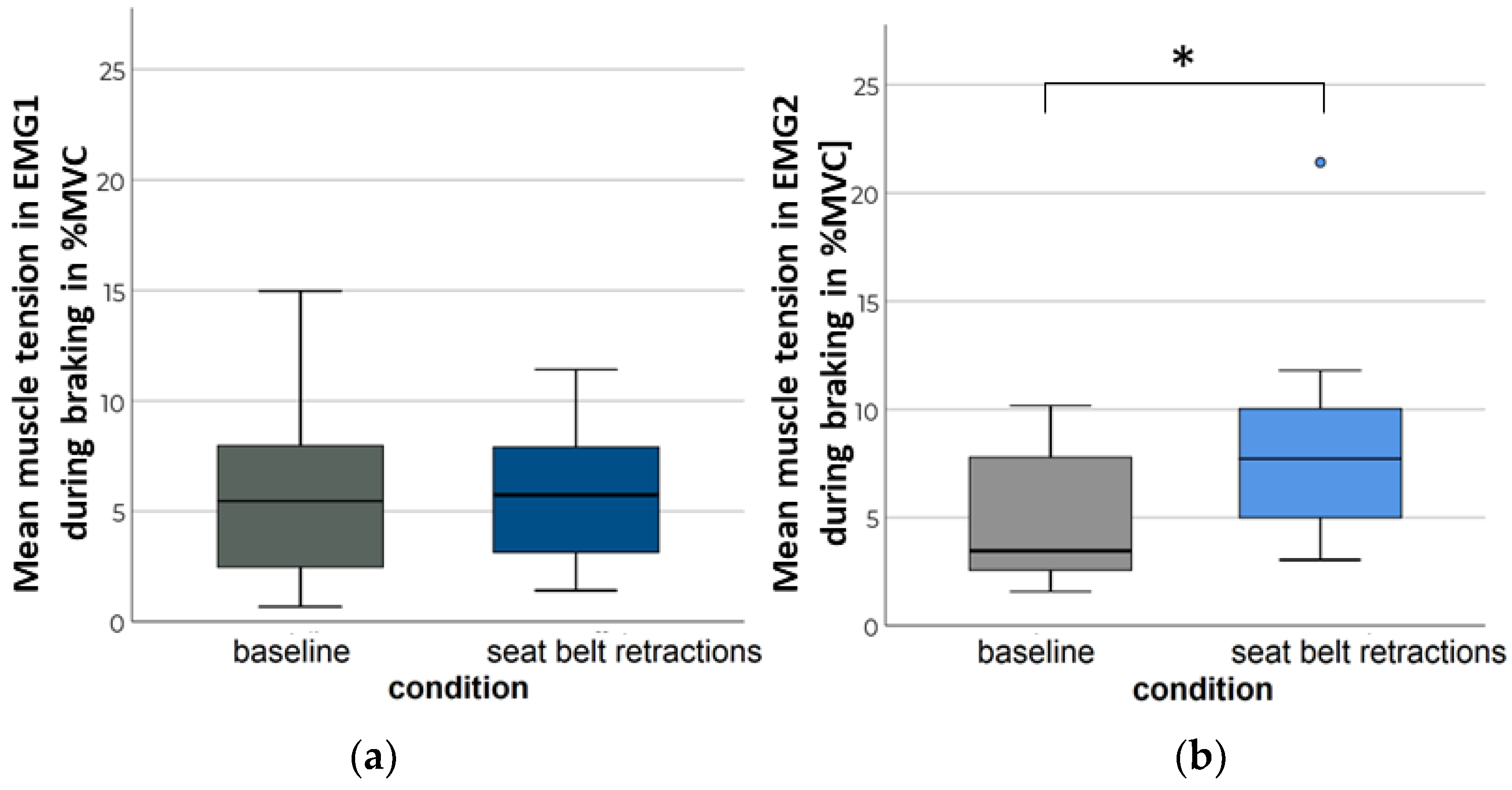
3.3. Neck Muscle Tension
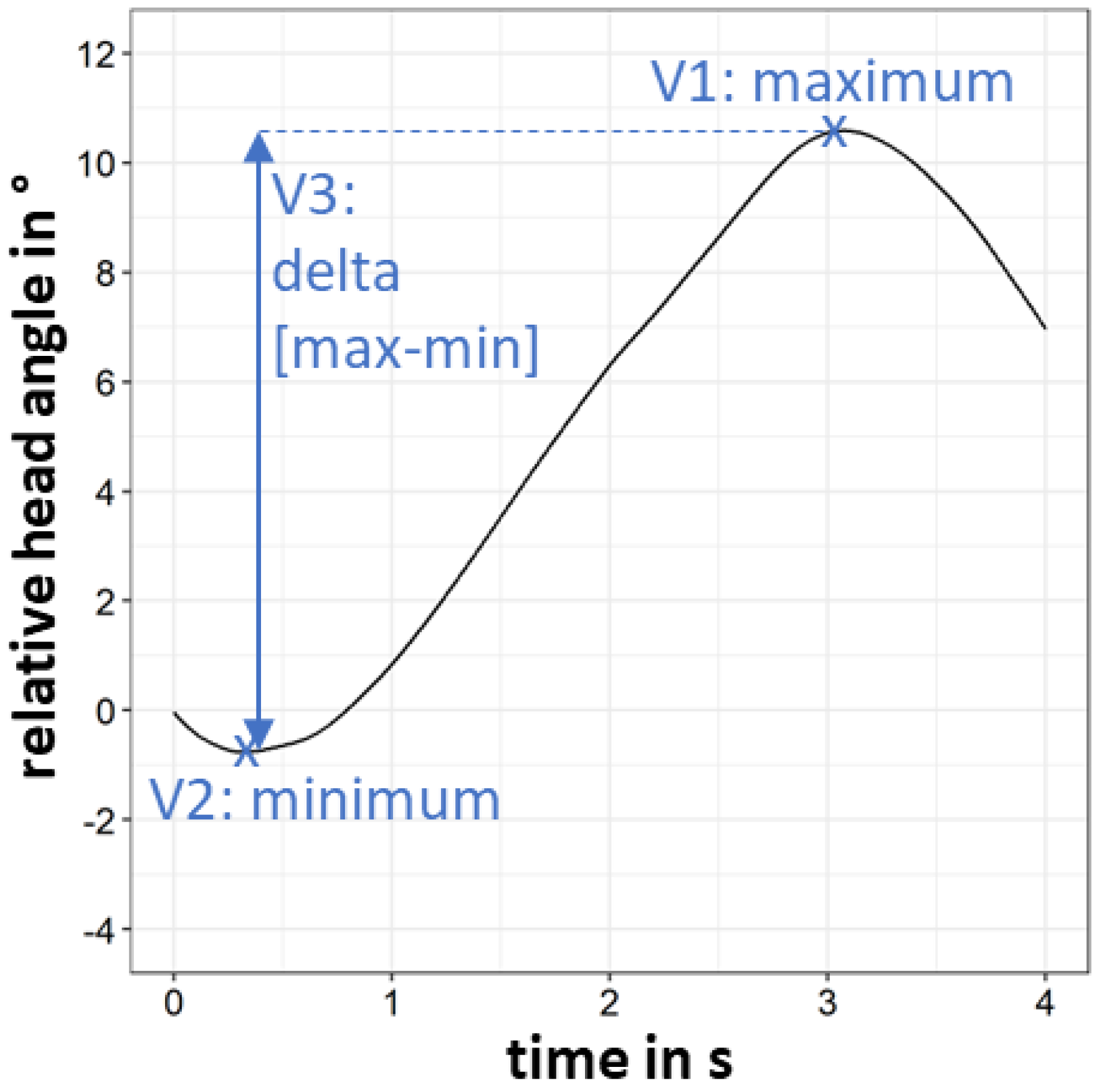
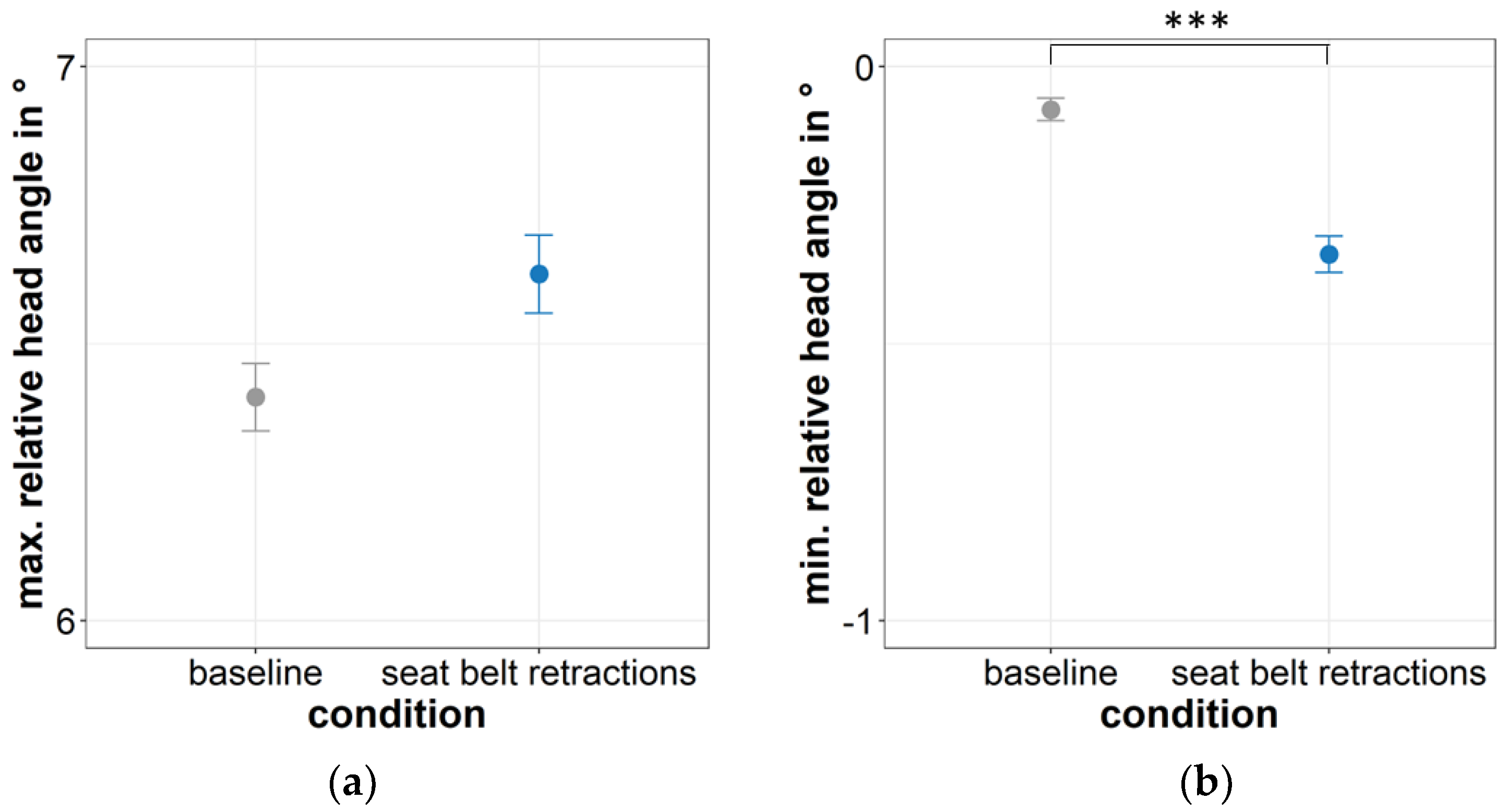
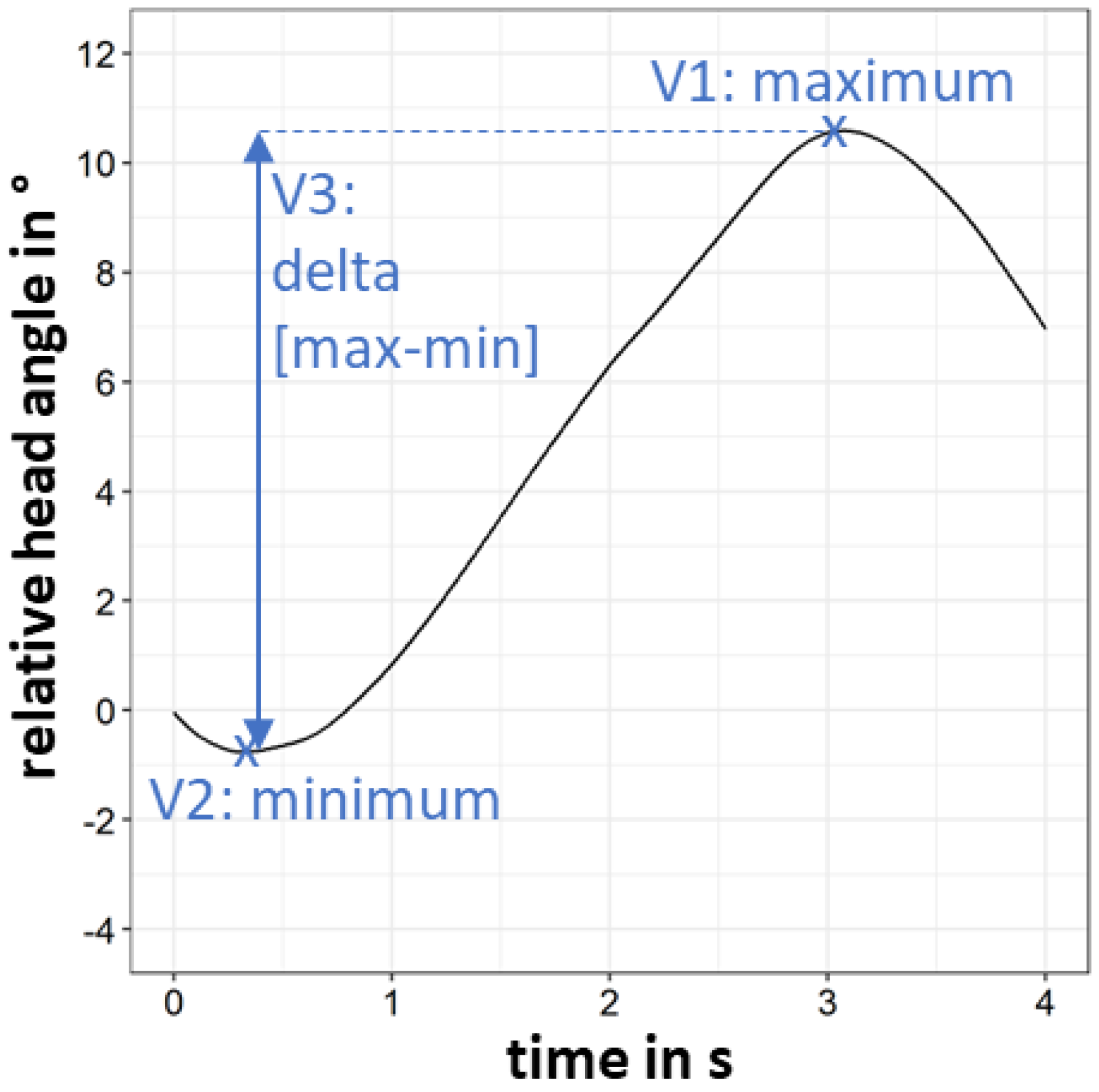
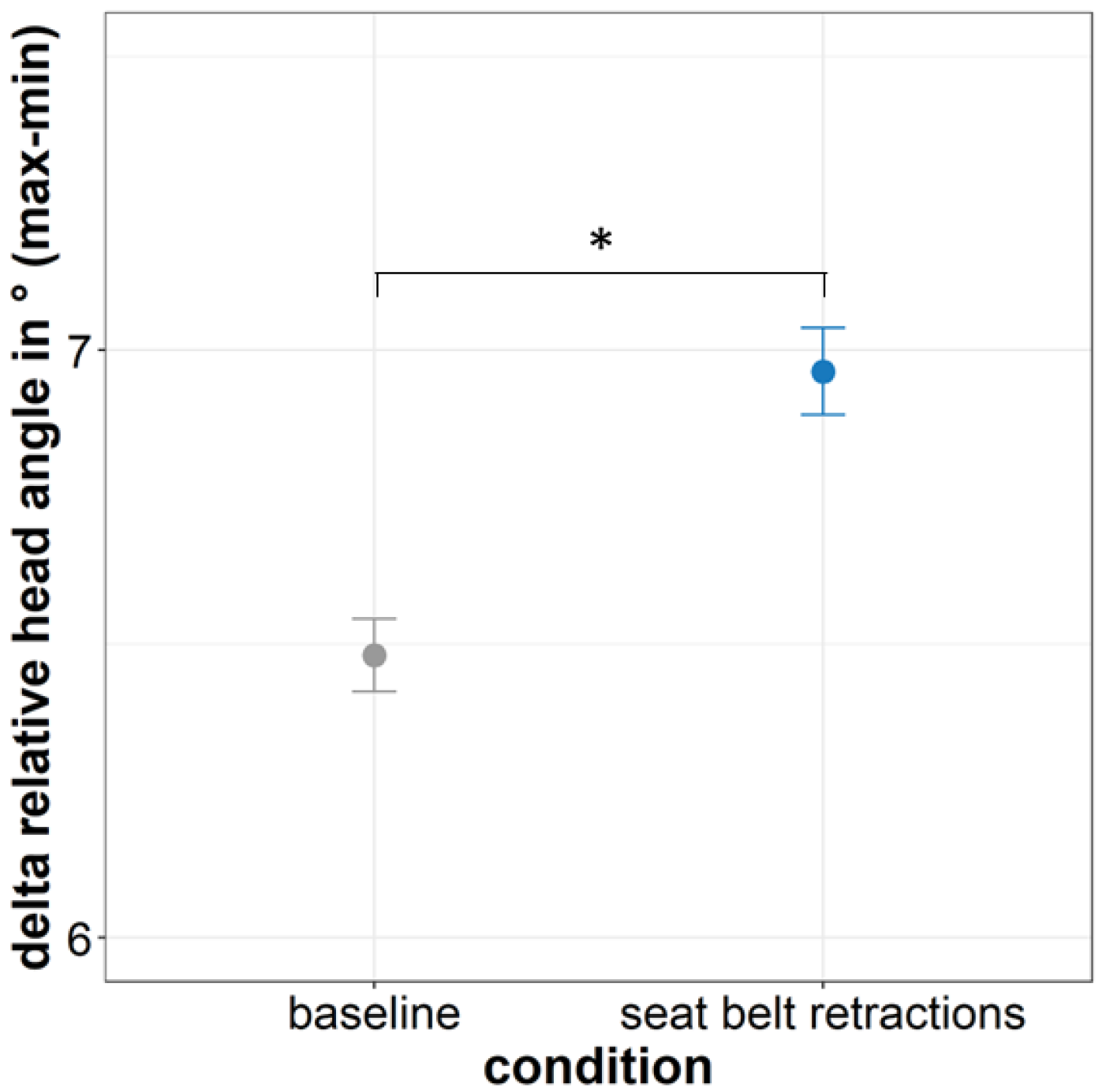
3.4. Head Movements
4. Discussion
Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Diels, C.; Bos, J.E. Self-driving carsickness. Appl. Ergon. 2016, 53 Pt B, 374–382. [Google Scholar] [CrossRef]
- Kato, K.; Kitazaki, S. Improvement of Ease of Viewing Images on An In-Vehicle Display and Reduction of Carsickness; SAE Technical Paper; SAE International: Warrendale, PA, USA, 2008. [Google Scholar] [CrossRef]
- Kuiper, O.X.; Bos, J.E.; Diels, C. Looking forward: In-vehicle auxiliary display positioning affects carsickness. Appl. Ergon. 2018, 68, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Sivak, M.; Schoettle, B. Motion Sickness in Self Driving Vehicles; UMTRI-2015-12; University of Michigang: Ann Arbor, MI, USA, 2015. [Google Scholar]
- Golding, J.F. Motion sickness. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2016; Volume 137, pp. 371–390. [Google Scholar] [CrossRef]
- Graybiel, A.; Wood, C.D.; Miller, E.F.; Cramer, D.B. Diagnostic criteria for grading the severity of acute motion sickness. Aerosp. Med. 1968, 39, 453–455. [Google Scholar] [PubMed]
- Bos, J.E.; MacKinnon, S.N.; Patterson, A. Motion sickness symptoms in a ship motion simulator: Effects of inside, outside, and no view. Aviat. Space Environ. Med. 2005, 76, 1111–1118. [Google Scholar] [PubMed]
- Diehls, C. Carsickness—Preventive Measures; Transport Research Laboratory: Crowthorne, UK, 2009. [Google Scholar]
- Reason, J.T. An Investigation of Some Factors Contributing to Individual Variation in Motion Sickness Susceptibility; Ministry of Defence (Air Force Department): London, UK, 1967.
- Wada, T. Motion sickness in automated vehicles. In Proceedings of the 13th International Symposium on Advanced Vehicle Control (AVEC’16), Munich, Germany, 13–16 September 2016; pp. 169–174. [Google Scholar]
- Smyth, J.; Birrell, S.; Mouzakitis, A.; Jennings, P. Motion Sickness and Human Performance—Exploring the Impact of Driving Simulator User Trials. In Proceedings of the 9th International Conference on Applied Human Factors and Ergonomics, Orlando, FL, USA, 22–26 July 2018; pp. 445–457. [Google Scholar]
- Smyth, J.; Jennings, P.; Mouzakitis, A.; Birrell, S. Too sick to drive: How Motion Sickness Severity Impacts Human Performance. In Proceedings of the 21st International Conference on Intelligent Transportation Systems (ITSC), Maui, HI, USA, 4–7 November 2018; pp. 1787–1793. [Google Scholar]
- Mercedes-Benz Group. The Front Number in Automated Driving and Safety Technologies. Available online: https://group.mercedes-benz.com/innovation/case/autonomous/drive-pilot-2.html (accessed on 17 June 2022).
- Vanholme, B.; Gruyer, D.; Lusetti, B.; Glaser, S.; Mammar, S. Highly automated driving on highways based on legal safety. IEEE Trans. Intell. Transp. Syst. 2012, 14, 333–347. [Google Scholar] [CrossRef]
- Schmidt, E.A.; Kuiper, O.X.; Wolter, S.; Diels, C.; Bos, J.E. An international survey on the incidence and modulating factors of carsickness. Transp. Res. Part F Traffic Psychol. Behav. 2020, 71, 76–87. [Google Scholar] [CrossRef]
- Brandt, T.; Dieterich, M.; Strupp, M. Vertigo: Leitsymptom Schwindel; Springer: Berlin/Heidelberg, Germany, 2004. [Google Scholar]
- Reason, J.T.; Brand, J.J. Motion Sickness; Academic Press: London, UK, 1975. [Google Scholar]
- Feenstra, P.J.; Bos, J.E.; van Gent, R.N.H.W. A visual display enhancing comfort by counteracting airsickness. Displays 2011, 32, 194–200. [Google Scholar] [CrossRef]
- Hainich, R.; Drewitz, U.; Ihme, K.; Lauermann, J.; Niedling, M.; Oehl, M. Evaluation of a Human–Machine Interface for Motion Sickness Mitigation Utilizing Anticipatory Ambient Light Cues in a Realistic Automated Driving Setting. Information 2021, 12, 176. [Google Scholar] [CrossRef]
- Karjanto, J.; Yusof, N.M.; Wang, C.; Terken, J.; Delbressine, F.; Rauterberg, M. The effect of peripheral visual feedforward system in enhancing situation awareness and mitigating motion sickness in fully automated driving. Transp. Res. Part F 2018, 58, 678–692. [Google Scholar] [CrossRef]
- Kuiper, O.X.; Bos, J.E.; Diels, C.; Schmidt, E.A. Knowing what’s coming: Anticipatory audio cues can mitigate motion sickness. Appl. Ergon. 2020, 85, 103068. [Google Scholar] [CrossRef]
- Kuiper, O.X.; Bos, J.E.; Schmidt, E.A.; Diels, C.; Wolter, S. Knowing What’s Coming: Unpredictable Motion Causes More Motion Sickness. Hum. Factors 2019, 62, 1339–1348. [Google Scholar] [CrossRef] [PubMed]
- Karjanto, J.; Yusof, N.M.; Hassan, M.Z.; Terken, J.; Delbressine, F.; Rauterberg, M. An on-road study in mitigating motion sickness when reading in automated driving. J. Hunan Univ. Nat. Sci. 2021, 48, 95–109. [Google Scholar]
- Riccio, G.E.; Stoffregen, T.A. An ecological theory of motion sickness und postural instability. Ecol. Psychol. 1991, 3, 195–240. [Google Scholar] [CrossRef]
- Konno, H.; Fujisawa, S.; Imaizumi, K.; Wada, T.; Kamiji, N.; Doi, S.i. Analysis of Driver’s Head Movement by Motion Sickness Model. In Proceedings of the 12th Korea and Japan Joint Ergonomics Symposium, Daejeon, Korea, 14 May 2010; pp. 290–293. [Google Scholar]
- Wada, T.; Fujisawa, S.; Doi, S. Analysis of driver’s head tilt using a mathematical model of motion sickness. Int. J. Ind. Ergon. 2018, 63, 89–97. [Google Scholar] [CrossRef]
- Zikovitz, D.C.; Harris, L.R. Head tilt during driving. Ergonomics 1999, 42, 740–746. [Google Scholar] [CrossRef]
- Brietzke, A.; Pham Xuan, R.; Dettmann, A.; Bullinger-Hoffmann, A. Head Motion as Indicator for Visual Anticipation in the Context of car Sickness. 2020; preprint. [Google Scholar]
- Wada, T.; Konno, H.; Fujisawa, S.; Doi, S. Can passengers’ active head tilt decrease the severity of carsickness?: Effect of head tilt on severity of motion sickness in a lateral acceleration environment. Hum. Factors 2012, 54, 226–234. [Google Scholar] [CrossRef]
- Wada, T.; Kamij, N.; Doi, S. A Mathematical Model of Motion Sickness in 6DOF Motion and Its Application to Vehicle Passengers. arXiv 2015, arXiv:1504.05261. [Google Scholar]
- Wada, T.; Yoshida, K. Effect of passengers’ active head tilt and opening/closure of eyes on motion sickness in lateral acceleration environment of cars. Ergonomics 2016, 59, 1050–1059. [Google Scholar] [CrossRef]
- Brietzke, A.; Pham Xuan, R.; Dettmann, A.; Bullinger-Hoffmann, A. Influence of dynamic stimulation, visual perception and individual susceptibility to car sickness during controlled stop-and-go driving. Forsch. Im Ing. 2021, 85, 517–526. [Google Scholar] [CrossRef]
- Golding, J.F.; Bles, W.; Bos, J.E.; Haynes, T.; Gresty, M.A. Motion sickness and tilts of the inertial force environment: Active suspension systems vs. active passengers. Aviat. Space Environ. Med. 2003, 74, 220–227. [Google Scholar] [PubMed]
- Johnsson, J.; Nobeling, N. Improving Braking and Cornering Sensation in A Driving Simulator by Developing An Active Seat Belt Tensioner. Master’s Thesis, Chalmers University of Technology, Gothenburg, Sweden, 2021. [Google Scholar]
- ZF. ZF Releases New Active Control Retractor Seat Belt System; ZF Friedrichshafen AG: Friedrichshafen, Germany, 2018; pp. 1–3. [Google Scholar]
- Östh, J.; Ólafsdóttir, J.M.; Davidsson, J.; Brolin, K. Driver Kinematic and Muscle Responses in Braking Events with Standard and Reversible Pre-Tensioned Restraints: Validation Data for Human Models; SAE Technical Paper; SAE International: Warrendale, PA, USA, 2013. [Google Scholar]
- Olafsdottir, J.M.; Östh, J.; Davidsson, J.; Brolin, K. Passenger Kinematics and Muscle Responses in Autonomous Braking Events with Standard and Reversible Pre-Tensioned Restraints. In Proceedings of the Ircobi Conference, Gothenburg, Sweden, 11–13 September 2013; pp. 602–617. [Google Scholar]
- Ghaffari, G.; Brolin, K.; Bråse, D.; Pipkorn, B.; Svanberg, B.; Jakobsson, L.; Davidsson, J. Passenger Kinematics in Lane Change and Lane Change with Braking Manoeuvres Using Two Belt Configurations: Standard and Reversible Pre-Pretensioner. In Proceedings of the 2018 IRCOBI Conference, Athens, Greece, 12–14 September 2018; pp. 12–14. [Google Scholar]
- Hoffmann, S.; Krüger, H.-P.; Buld, S. Avoidance of Simulator Sickness by Training the Adaptation to the Driving Simulation. In Simulation und Simulatoren—Mobilität Virtuell Gestalten; VDI-Berichte, Ed.; VDI-Verlag: Düsseldorf, Germany, 2003; Volume 1745, pp. 385–404. [Google Scholar]
- Johnson, D.M. Introduction to and Review of Simulator Sickness Research; Research Report 1832; U.S. Army Research Institute for the Behavioral and Social Sciences: Arlington, TX, USA, 2005. [Google Scholar]
- Hoffmann, S.; Buld, S. Darstellung und Evaluation Eines Trainings Zum Fahren in der Fahrsimulation. In Integrierte Sicherheit und Fahrerassistenzsysteme; VDI-Berichte, Ed.; VDI-Verlag: Düsseldorf, Germany, 2006; Volume 1960, pp. 113–132. [Google Scholar]
- Golding, J.F. Predicting individual differences in motion sickness susceptibility by questionnaire. Personal. Individ. Differ. 2006, 41, 237–248. [Google Scholar] [CrossRef]
- ISO 2631-1; Mechanical Vibration and shock—Evaluation of Human Exposure to Whole-Body Vibration—Part 1: General Requirements. International Organisation for Standardization: Geneva, Switzerland, 1997.
- Gianaros, P.J.; Muth, E.R.; Mordkoff, J.T.; Levine, M.E.; Stern, R.M. A questionnaire for the assessment of the multiple dimensions of motion sickness. Aviat. Space Environ. Med. 2001, 72, 115–119. [Google Scholar] [PubMed]
- Kaß, C.; Tomzig, M.; Marberger, C.; Schulz, M.; Alt, P.; Horn, S.; Teicht, M.; Engeln, A. Short Assessment Scale to Assess Motion Sickness in Automated Driving: Motion Sickness Task Tolerance (MSTT) Scale. Available online: https://projekt-rumba.de/wp-content/uploads/2022/07/MotionSickness_homepage_website_en.pdf (accessed on 14 July 2022).
- Keshavarz, B.; Hecht, H. Validating An Efficient Method to Quantify Motion Sickness. Hum. Factors 2011, 53, 415–426. [Google Scholar] [CrossRef]
- Neukum, A.; Lübbeke, T.; Krüger, H.-P.; Mayser, C.; Steinle, J. ACC-Stop&Go: Fahrerverhalten An Funktionalen Systemgrenzen. In Proceedings of the 5. Workshop Fahrerassistenzsysteme-FAS, Walting, Germany, 2–4 April 2008; pp. 141–150. [Google Scholar]
- Pupil Labs. Pupil Invisible: The Future of Eye Tracking. Available online: https://pupil-labs.com/products/invisible/ (accessed on 17 June 2022).
- Field, A. Discovering Statistics Using IBM SPSS Statistics; University of Sussex: Brighton, UK, 2013. [Google Scholar]
- Yokota, Y.; Aoki, M.; Mizuta, K.; Ito, Y.; Isu, N. Motion sickness susceptibility associated with visually induced postural instability and cardiac autonomic responses in healthy subjects. Acta Oto-Laryngol. 2005, 125, 280–285. [Google Scholar] [CrossRef]
- Owen, N.; Leadbetter, A.G.; Yardley, L. Relationship between postural control and motion sickness in healthy subjects. Brain Res. Bull. 1998, 47, 471–474. [Google Scholar] [CrossRef]
- Gordon, C.R.; Spitzer, O.; Doweck, I.; Shupak, A.; Gadoth, N. The vestibulo-ocular reflex and seasickness susceptibility. J. Vestib. Res. Equilib. Orientat. 1996, 6, 229–233. [Google Scholar] [CrossRef]
- Nachum, Z.; Gordon, C.R.; Shahal, B.; Spitzer, O.; Shupak, A. Active high-frequency vestibulo-ocular reflex and seasickness susceptibility. Laryngoscope 2002, 112, 179–182. [Google Scholar] [CrossRef]
- Mühlbacher, D.; Tomzig, M.; Reinmüller, K.; Rittger, L. Methodological Considerations Concerning Motion Sickness Investigations during Automated Driving. Information 2020, 11, 265. [Google Scholar] [CrossRef]
- Blaauw, G.J. Driving experience and task demands in simulator and instrumented car: A validation study. Hum. Factors 1982, 24, 473–486. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kremer, C.; Tomzig, M.; Merkel, N.; Neukum, A. Using Active Seat Belt Retractions to Mitigate Motion Sickness in Automated Driving. Vehicles 2022, 4, 825-842. https://doi.org/10.3390/vehicles4030046
Kremer C, Tomzig M, Merkel N, Neukum A. Using Active Seat Belt Retractions to Mitigate Motion Sickness in Automated Driving. Vehicles. 2022; 4(3):825-842. https://doi.org/10.3390/vehicles4030046
Chicago/Turabian StyleKremer, Christina, Markus Tomzig, Nora Merkel, and Alexandra Neukum. 2022. "Using Active Seat Belt Retractions to Mitigate Motion Sickness in Automated Driving" Vehicles 4, no. 3: 825-842. https://doi.org/10.3390/vehicles4030046
APA StyleKremer, C., Tomzig, M., Merkel, N., & Neukum, A. (2022). Using Active Seat Belt Retractions to Mitigate Motion Sickness in Automated Driving. Vehicles, 4(3), 825-842. https://doi.org/10.3390/vehicles4030046